
Abstract
Background:
Alzheimer’s disease (AD) is one of the most costly conditions, both economically and regarding patient disability and dependency. The huge costs coupled with the predicted increase in prevalence worldwide are likely to challenge healthcare systems in the future. The classic version of the Alzheimer’s Disease Assessment Scale-Cognition subscale (ADAS-Cog) is generally seen as the current gold standard primary outcome measure of cognitive symptom progression in dementia clinical trials.
Objective:
This study evaluated the relationship between ADAS-Cog scores as a measure of clinical progression and the healthcare resource utilization (HCRU)-measured burden of cognitive impairment in patients with mild cognitive impairment, AD, or suspected AD in the real world.
Methods:
A retrospective observational survey of physicians and their consulting patients with multiple ADAS-Cog scores. Regression models were constructed for HCRU variables (e.g., consultations, hospitalizations, caregiving requirements) with ADAS-Cog rate of change, baseline ADAS-Cog, and their interaction included as exposure variables.
Results:
651 patient records were completed by 154 physicians. Approximately 70% of patients had mild to moderate dementia. In 56.7% of patients, clinical progression was maintained/stable from baseline. Mean change in ADAS-Cog (adjusted to 12 months) was 2.8 points and change scores increased with increasing dementia severity. Most HCRU variables increased significantly (p < 0.05; joint test) with increasing ADAS-Cog scores (indexing clinical deterioration).
Conclusion:
The results suggest that further understanding the relationship between HCRU and ADAS-Cog changes in real-world clinical practice could potentially provide a baseline upon which the success of disease-modifying, as well as newer symptomatic, dementia therapies can be judged.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the most common cause of dementia, contributing to 60–70% of cases, and is characterized by deterioration in higher cognitive functions such as memory, learning, and judgement [1]. The end stage of the disease, AD, is thought to affect approximately 46 million people worldwide (aged mainly >65 years) and people present with symptoms including forgetfulness, losing track of time, and becoming lost in familiar places [1–4]. The cause of AD is poorly understood and there are currently no treatments that stop or alter its progression, although some drug treatments can temporarily improve symptoms, e.g., cholinesterase inhibitors [4–6]. The substantial economic burden of AD is well-documented [1, 7–10]. It is one of the most costly conditions, both economically and also regarding disability, dependency, and burden on families and caregivers [1]. Informal care (i.e., unpaid care provided by family members or other non-professional caregivers) and formal social care have been shown to be the largest cost components of AD, while direct medical costs are lower [1, 10]. Costs also increase as disease severity worsens. The huge costs of AD coupled with the predicted increase in prevalence are likely to challenge healthcare systems in the future [1].
The classic version of the Alzheimer’s Disease Assessment Scale-Cognition subscale (ADAS-Cog) was designed to evaluate the severity of cognitive symptoms characteristic of AD [11]. It is generally seen as the current gold standard primary cognitive outcome measure used in dementia clinical trials as it is sensitive to change and can therefore determine improvements or declines in cognitive function [12, 13]. Its 11 tasks measure several cognitive domains including disturbances of memory, learning, attention, and other core symptoms of AD. Total scores range from 0–70 (no impairment to severe impairment) and higher scores (≥18) indicate greater cognitive impairment. In dementia drug trials, a four-point change in the ADAS-Cog after 6 months is generally seen as a clinically important difference [14]. The ADAS-Cog is commonly considered more comprehensive and sensitive than other measures of global cognitive function such as the Mini-Mental State Examination, especially in the moderate stages of AD [15, 16]. However, the ADAS-Cog has more items and takes longer to complete. The ADAS-Cog is the most widely used instrument for assessing cognitive symptom progression in AD, i.e., it shows a longitudinal response relating to the progression rate of cognitive decline [17–20]. Understanding the use of this cognitive symptom progression measure in real-world clinical practice, as opposed to clinical trials, and its relationship with healthcare resource utilization (HCRU) could potentially provide a baseline upon which the success of disease modifying, as well as newer symptomatic, therapies can be judged.
A feasibility study (to determine whether the ADAS-Cog is being used by physicians who manage people with AD in their clinical practices) suggested that there are physicians who use the ADAS-Cog in the real-world and identified an initial target pool of 261 physicians that may be contactable for further survey purposes. These results gave the research group confidence that they would be able to find in their dataset people with cognitive impairment where the ADAS-Cog has been applied and therefore would enable them to further investigate its use in a real-world setting. Following on from this, the objectives of the current study were: 1) to evaluate the associations between ADAS-Cog scores and HCRU in people with AD and mild cognitive impairment (MCI) in the real-world, and 2) to evaluate the impact of a change in ADAS-Cog scores and the rate of these changes on the HCRU-measured burden of AD and MCI.
MATERIALS AND METHODS
Design
A multicenter, retrospective observational survey of physicians who were responsible for people with a diagnosis of AD or MCI was conducted in five European countries (France, Germany, Italy, Spain, and the United Kingdom [UK]) and in the United States (US). Recruited physicians were required to complete a minimum of three patient record forms (PRFs) for previous consulting patients with AD (or suspected AD) or MCI, and where the ADAS-Cog rating scale had been applied (Fig. 1). Data were extracted from medical records and recorded on the PRFs.

Study design. Note: This figure shows the basic study design of the current real-world, multinational, retrospective observational survey. AD, Alzheimer’s disease; ADAS-Cog, Alzheimer’s Disease Assessment Scale-Cognition; HCRU, healthcare resource utilization; PRF, patient record form; RCT, randomized controlled trial.
Population
The study used a convenience sample of physicians and patients who had used the ADAS-Cog identified via the feasibility study. Physicians were invited to participate and screened to ensure they met eligibility criteria. To be considered, the physicians’ specialism was required to be neurologist, geriatrician, or psychiatrist (or psycho-geriatrician in the UK). Participating physicians were required to be personally responsible for the management of at least 10 people with AD/MCI and to have completed the ADAS-Cog for at least three of their managed patients, and at multiple time points, in the last 12 months. Patients were required to be cognitively impaired patients diagnosed with MCI, AD, or suspected AD and with a history of ADAS-Cog usage, i.e., an ADAS-Cog assessment in the previous 6 months and another no more than 18 months prior to that (i.e., in the previous 24 months). Patients who were taking part in randomized controlled clinical trials were excluded from the study.
Outcomes
The data collected pertained to patient and physician baseline demographics; ADAS-Cog scores (the most recent ADAS-Cog test had to be no more than 6 months ago and the baseline ADAS-Cog was taken as the nearest measurement to 12 months from the most recent score and had to be between 6 and 18 months prior to the most recent score; total scores range from 0 [no impairment] to 70 [severe impairment]); and details relating to HCRU which included: consultations with primary care physicians (PCPs), specialists, and other healthcare professionals (HCPs) in the last 12 months; all-cause and cognitive impairment-related hospitalizations in the last 12 months; institutionalized status (i.e., whether the patient was living in a nursing home owing to dementia); and the requirement and hours of professional and non-professional caregiving. HCRU data was collected from patient’s medical records that the physician refers to when completing their PRFs. The patients’ current degree of cognitive impairment was physician-defined as MCI, or mild, moderate, or severe dementia.
Statistical methods
The primary outcomes of interest were: ADAS-Cog levels and change scores (rate of change/clinical progression), HCRU variables, and HCRU associated with ADAS-Cog levels and changes. Over the time course of the study, ADAS-Cog change scores ≤–4 were equated with improvement and ≥4 were equated with worsening; scores between <4 and > –4 were considered maintained/stable [14]. Patients were also categorized into quartiles by most recent ADAS-Cog score. Standard descriptive statistics were used to describe outcomes. Numerical variables were described in terms of mean, median, standard deviation (SD), minimum and maximum; categorical variables were described by frequency and percentage of patients falling into each category. Basic statistical tests (e.g., Kruskal-Wallis; Pearson’s Chi-Square) were used to assess differences in outcomes between groups, e.g., the degree of baseline cognitive impairment and ADAS-Cog rate of change (improved, maintained/stable, or worsened).
Regression models were constructed for each HCRU variable; negative binomial regressions for numeric outcomes and logistic regressions for binary outcomes. Standard errors were adjusted to allow for possible intragroup correlation within reporting physicians. For primary analyses, ADAS-Cog rate of change, baseline ADAS-Cog, and the interaction between ADAS-Cog change and baseline were included as the exposure variables. For secondary analyses, most recent ADAS-Cog score was included as the exposure variable. All models were adjusted for the following potentially confounding covariates: patients’ age, sex, body mass index (BMI), and Charlson Comorbidity Index (CCI). Statistical results were interpreted at the 5% significance level and the models were constructed globally. Data management and statistical analyses were conducted using Stata Version 15 [21].
The analysis described in this manuscript includes all patients with MCI/AD, but excludes outliers; i.e., patients who showed rapid changes in ADAS-Cog scores (change rate >10 or < –10). The decision to exclude outliers using explicit criteria was based on initial statistical investigation and clinical knowledge, and was made because these results were clinically unrealistic and not considered consistent with the population overall. Variance may be driven by changes in the test environment or comorbidities and therefore not reflective of underlying changes in clinical progression, which may have impacted the results and masked real effects. Specifically, the concomitant profile of these patients, regarding central nervous system conditions (such as depression, Parkinson’s disease, bipolar disorder, and insomnia/sleep disorders), was higher in the rapid change group. When reviewed in consultation with a physician, it was considered that this trend could impact the variation seen in the ADAS-Cog.
Ethical conduct
Data collection was undertaken in line with European Pharmaceutical Marketing Research Association guidelines and as such it does not require ethics committee approval. Each survey was performed in full accordance with relevant legislation at the time of data collection, including the US Health Insurance Portability and Accountability Act 1996 and Health Information Technology for Economic and Clinical Health Act legislation.
RESULTS
Population
A total of 651 PRFs were completed by 154 physicians. Briefly, the analysis started with 1,086 patients; 1,006 patients had an ADAS-Cog assessment in the previous 6 months and 758 had a matching test in the preceding 6–18 months. 107 patients were excluded as outliers (93 had an ADAS-Cog rate of change >10 and 14< –10), and therefore 651 patients had a rate of change between –10 and 10 and were included in the analyses.
Most of the included physicians were neurologists (90.3% with 3.9% psycho-geriatricians in the UK only) and male (66.9%) who managed an average (SD) of 48.8 (98.1) patients for whom they had completed the ADAS-Cog. Patient demographic characteristics are given in Table 1. Overall, there were slightly more female than male patients in the study population and the mean (SD) age was 72.7 (8.8) years. 40.2% of patients had mild dementia as their current diagnosis label, followed by 28.4% with moderate dementia and 13.6% with severe dementia; 17.9% of patients were diagnosed with MCI. The mean (SD) ADAS-Cog score at baseline was 24.6 (15.9) and scores ranged from 0.0 to 69.0 (total scores could be up to 70, indicating severe impairment).
Patient demographics and clinical characteristics and HCRU, overall and by ADAS-Cog response group
Note: *Improved = ADAS-Cog change scores ≤–4, Maintained/stable = ADAS-Cog change scores between 3 and –3, Worsened = ADAS-Cog change scores ≥4; †p < 0.0001 (Pearson’s Chi-squared or Kruskal-Wallis); ‡p = 0.0279 (specialist visits in last 12 months; Kruskal-Wallis), p = 0.0086 (number of hospitalizations for cognitive impairment in last 12 months, Kruskal-Wallis), p = 0.0102 (professional caregiver required, Pearson’s Chi-squared), p = 0.0098 (total professional caregiver hours; Kruskal-Wallis); Physician-estimated time per week in hours. AD, Alzheimer’s disease; ADAS-Cog, Alzheimer’s Disease Assessment Scale-Cognition; HCP, healthcare professional; HCRU, healthcare resource utilization; MCI, mild cognitive impairment; N/n, number; PCP, primary care physician; SD, standard deviation.
Primary outcomes
Rate of clinical progression
In 56.7% of patients, clinical progression was maintained/stable from baseline (ADAS-Cog change score between <4 and > –4); followed by worsening (≥4) in 38.9% and improvement (≤–4) in 4.5% of patients. The mean (SD) change in the ADAS-Cog (adjusted to 12 months) was 2.8 (3.6) points. Mean change scores increased with increasing dementia severity: 1.4 points (MCI), 2.9 points (mild dementia), 3.2 points (moderate dementia), and 3.8 points (severe dementia) with statistically significant differences between the groups (p < 0.0001, Kruskal-Wallis test).
Patients whose clinical progression was maintained/stable from baseline were more likely to have had a diagnosis of MCI or mild to moderate dementia, whereas patients who worsened were more likely to have had moderate to severe dementia. Statistically significant differences were found between the clinical progression groups (i.e., improvement, maintained/stable, worsening in ADAS-Cog) for baseline ADAS-Cog score, most recent ADAS-Cog score, and worst of the two ADAS-Cog scores being assessed (p < 0.0001, Kruskal-Wallis test), and also for the patients’ current diagnosis label (i.e., MCI or mild, moderate, or severe dementia; p < 0.0001, Pearson’s Chi-Squared test).
HCRU
HCRU overall and by clinical progression (ADAS-Cog rate of change) is described in Table 1. Patients had an average of 2.8 PCP, 3.6 specialist and 1.6 other HCP visits in the previous 12 months. The mean number of hospitalizations for cognitive impairment was 0.08 and 10.2% of patients were institutionalized. Moreover, 29.6% and 69.0% of patients required professional and non-professional caregiving, respectively. Statistically significant differences were found between the three clinical progression groups (i.e., improvement, maintained/stable, or worsening in ADAS-Cog) for specialist visits and number of hospitalizations for cognitive impairment in the last 12 months, and professional caregiving requirements and hours. Similar results were found when excluding the ADAS-Cog improvement change group (i.e., only in patients with an ADAS-Cog rate of change > –4).
The association between clinical progression and HCRU was confirmed for individual HCRU variables by the regression analysis (adjusted for covariates). For all variables (except PCP consultations in the last 12 months) there was an association with statistically significantly higher levels of resource utilization with increasing clinical progression (p < 0.05 with a joint test for the three main predictors; Table 2). For each unit increase in ADAS-Cog rate of change, the percentage resource use increases ranged from 1.05% for PCP consultations to 3.34% for number of professional caregiver hours. The contour plots suggest that the way clinical progression affects HCRU outcomes depends heavily on the baseline ADAS-Cog score (Fig. 2).
Regression analysis of HCRU by ADAS-Cog rate of change in the last 12 months
ADAS-Cog, Alzheimer’s Disease Assessment Scale-Cognition; CI, confidence interval; HCP, healthcare professional; HCRU, healthcare resource utilization; IRR, incidence rate ratio; OR, odds ratio; PCP, primary care physician.
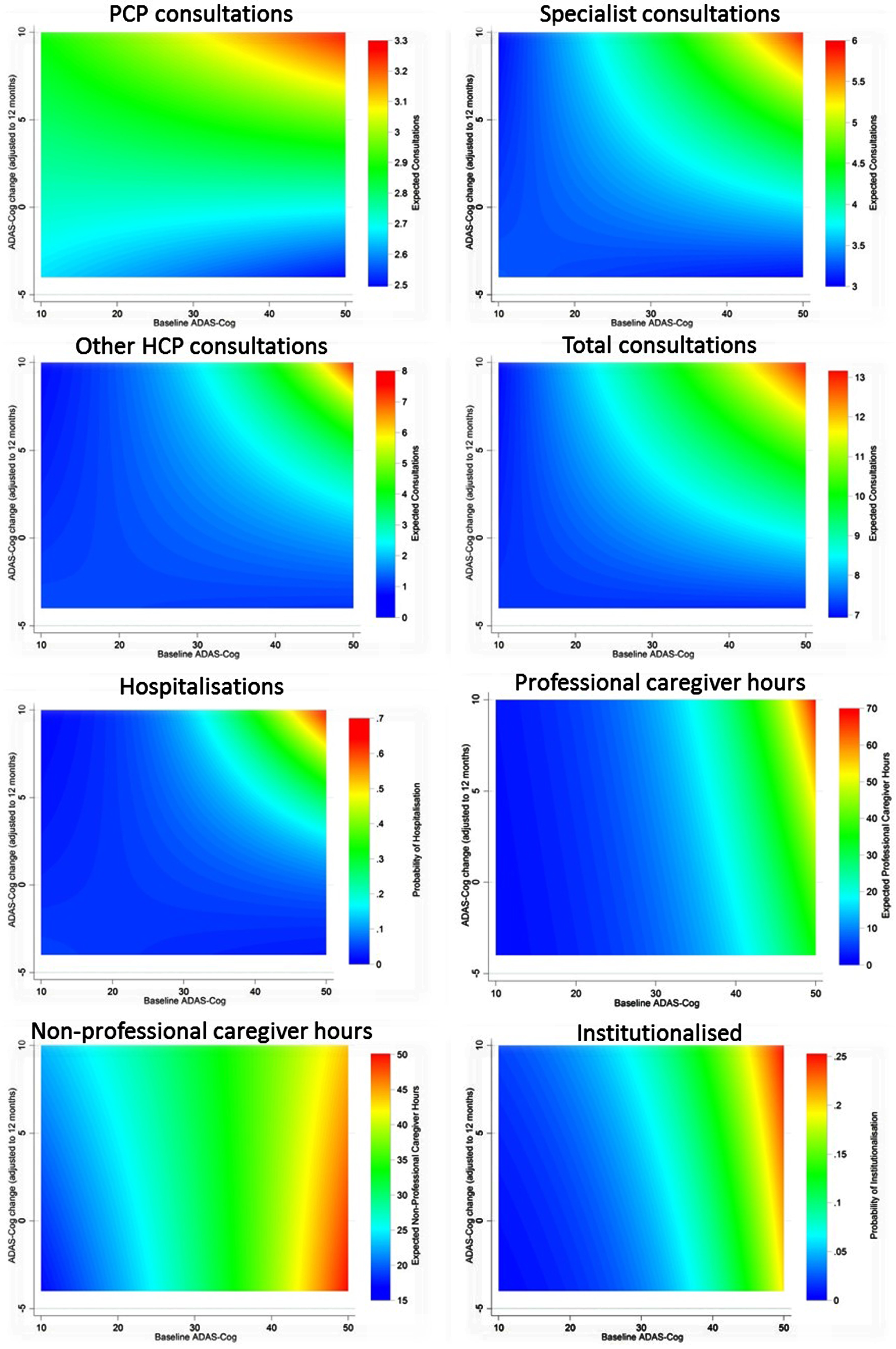
HCRU by ADAS-Cog rate of change in the last 12 months. This figure shows contour plots of the association between clinical progression (using ADAS-Cog score changes) and the individual HCRU variables. ADAS-Cog, Alzheimer’s Disease Assessment Scale-Cognition; HCP, healthcare professional; HCRU, healthcare resource utilization; PCP, primary care physician.
Secondary outcomes: Most recent ADAS-Cog
The mean (SD) most recent ADAS-Cog score was 27.4 (16.0) points (range, 2.0–69.0 points). Dividing the most recent ADAS-Cog results into quartiles, 27.5% of patients had scores of 2–15 points, 26.0% had scores of 16–26, 22.7% had scores of 27–39, and 23.8% had scores of 40–69. There were significant differences between the quartile groups for all HCRU variables except PCP visits in the last 12 months (p < 0.01, Kruskal-Wallis and Pearson’s Chi-Squared tests). Mean values were generally higher in the highest quartile range group (i.e., 40–69 points).
Similar to the primary results, the regression analysis of the most recent ADAS-Cog result found statistically significant increases for all HCRU variables, except PCP consultations in the last 12 months, with increasing ADAS-Cog score (Table 3; Fig. 3). The incidence rate ratios ranged from 1.003 for PCP consultations to 1.083 for patients institutionalized.
Regression analysis of HCRU by most recent ADAS-Cog
ADAS-Cog, Alzheimer’s Disease Assessment Scale-Cognition; CI, confidence interval; HCP, healthcare professional; HCRU, healthcare resource utilization; IRR, incidence rate ratio; OR, odds ratio; PCP, primary care physician.
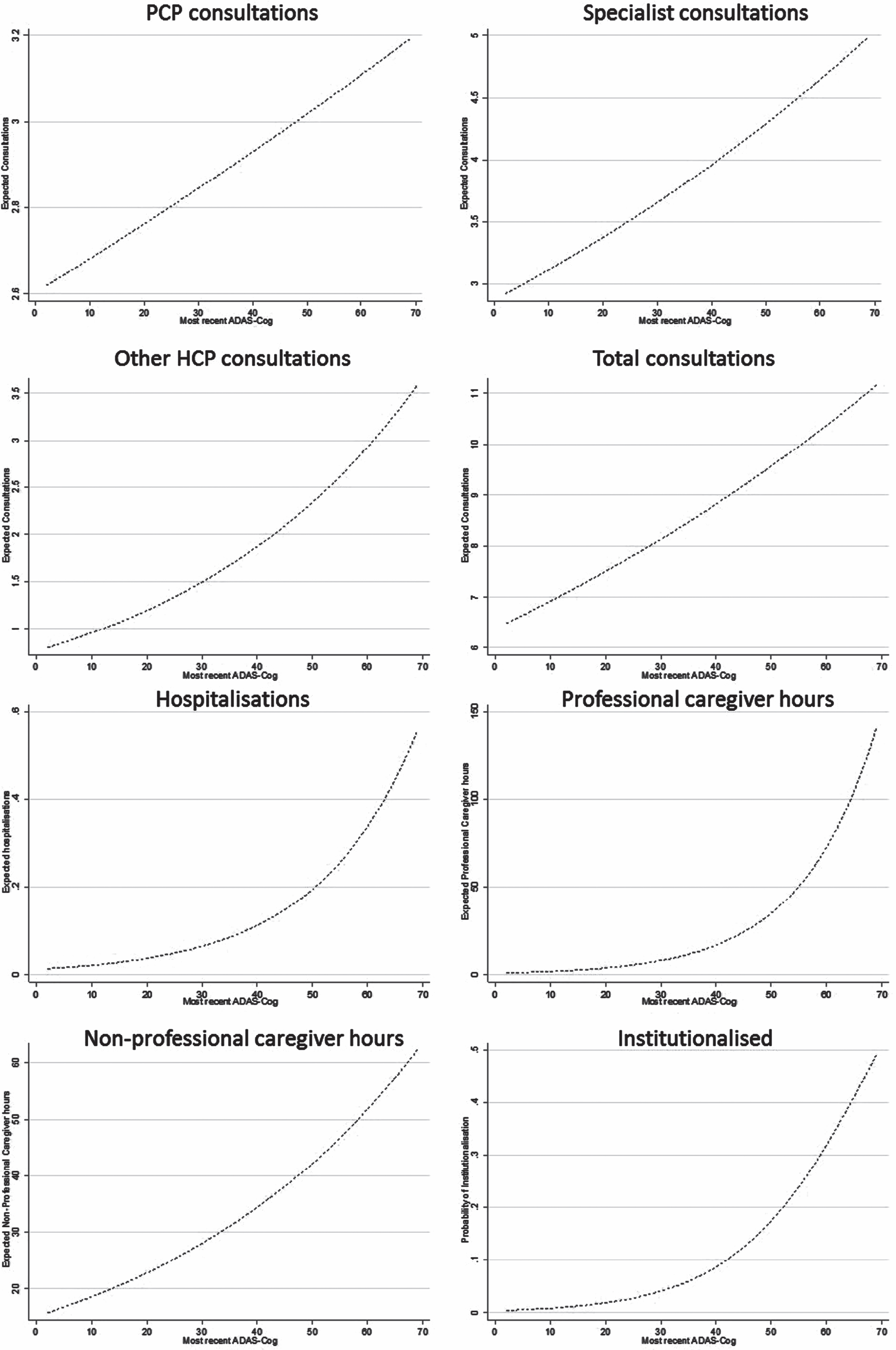
HCRU by most recent ADAS-Cog. This figure shows graphs of the association between clinical progression (using the most recent ADAS-Cog score) and the individual HCRU variables. ADAS-Cog, Alzheimer’s Disease Assessment Scale-Cognition; HCP, healthcare professional; HCRU, healthcare resource utilization; PCP, primary care physician.
DISCUSSION
Real-world data on the relationship between progression of AD and HCRU are lacking and therefore this study reports on the impact of clinical progression, as measured by the ADAS-Cog in clinical practice, on resource utilization. Randomized controlled trials and other types of clinical study influence guidelines and treatment decisions; however, the data they provide may not reflect real-world clinical practice patterns because of the often narrow criteria applied for trial inclusion. Real-world studies can provide insights into decisions being made in clinical practice and patient outcomes and can support prioritization of resources.
The patient population observed in this real-world study was similar to the demographic characteristics of the GERAS study, an 18-month prospective observational study of resource use and costs associated with AD in France, Germany, and the UK; although the current study had a smaller overall population size (651 versus 1497 patients) and a slightly younger patient sample (mean age of 72.7 versus 77.6 years) [10].
In the current study, the mean change in ADAS-Cog scores was 2.8 points, which is equated with relatively stable disease [14]. Generally, a four-point change on the ADAS-Cog after 6 months is indicative of a clinically important difference; therefore, in this study the change (adjusted to 12 months) was smaller indicating that patient clinical progression was quite modest. However, mean change scores increased with increasing severity of the person’s diagnosed AD, which highlights different rates of deterioration over the varying stages of AD and has been shown in previous studies. In a systematic review and meta-analysis model of 52 studies (N = 19,972) by Ito et al. (2009), baseline ADAS-Cog was a significant covariate on clinical progression, i.e., greater impairment at baseline was associated with faster cognitive decline [22]. Clinical progression was estimated at 5.5 ADAS-Cog points per year, which is higher than in the current study, although baseline ADAS-Cog values were comparable (25 versus 24.6 in the Ito et al. and current studies, respectively) and the proportion of stable MCI patients in our sample may have reduced the mean ADAS-Cog.
HCRU increased with increasing clinical progression for the majority of the individual resource use variables measured (specialist, other, and total consultations in the last 12 months; hospitalizations in the last 12 months; professional and non-professional caregiver hours; and proportion of patients institutionalized). Regression analyses, adjusted for potentially confounding factors, confirmed statistically significant increases in resource utilization (joint test of three main predictors). For each unit increase in ADAS-Cog rate of change, the percentage resource use increases ranged from 1.05% to 3.34%. The largest increase was for number of professional caregiver hours which may reflect the transition from non-professional (i.e., informal care by family members and non-professional caregivers) to formal professional and community care requirements as the patient’s condition worsens and their needs increase. This has been discussed before [15]. The only apparent anomaly in the results was for the number of PCP consultations in the last 12 months, for which no associations were evident. This may be explained by the engagement of PCPs in the management of older people with multiple comorbidities where the progression of AD is not in its own right significant enough to change the ongoing rate of contact older people have with their family doctors. The results of the secondary analyses (using the most recent ADAS-Cog score), were largely supportive of primary results. Furthermore, an interpretation of the contour plots confirms that the link between clinical progression and HCRU depends heavily on baseline ADAS-Cog values. The importance of baseline ADAS-Cog scores in predicting outcomes has been shown previously [22–24].
The main results are generally consistent with previous study findings. A longitudinal observational study of community-dwelling subjects with mild to moderate AD found that a one point change in ADAS-Cog was associated with a 1.74% increase in total care cost (repeated measures model) [25]. This is comparable to the percentage resource use increases for some of the HCRU variables in the current study, e.g., PCP (1.05% increase for each unit increase in ADAS-Cog rate of change), specialist (1.29%), and total (1.34%) consultations in the previous 12 months; and non-professional caregiver hours (1.07%). Furthermore, the GERAS study showed that all healthcare resources and cost components (excluding caregiver resource use) increased significantly as disease severity worsened [10]. The costs of AD are known to be substantial and studies have shown increased costs and resource utilization with increased disease severity, i.e., as cognitive function declines [15, 26–28]. However, this is the first study that we know of looking at the real-world burden of AD in relation to ADAS-Cog change as a measure of clinical progression.
The strengths of this study were that it included multiple sites and countries, the setting was reflective of real-world practice, and the target population included all consulting AD (or suspected AD) patients at all disease severity levels, from MCI to severe dementia. As an observational survey it avoided the narrow selection criteria intrinsic in clinical trials and should therefore have greater relevance to wider populations in clinical practice. However, this was a chart review using a convenience sample of physicians and patients who had used the ADAS-Cog which has a number of methodological limitations: the sample was not fully random owing to the specific inclusion criteria required for participation; the study relied on accurate and complete patient records and data collection; and owing to the cross-sectional nature of this study and because data were drawn from patient records retrospectively, there may have been incomplete overlap of HCRU and time between ADAS-Cog measurements. The accuracy of data such as HCRU is dependent on the availability of the data in patient records, meaning there is a possibility this data is underreported by physicians. It was decided to exclude outliers (with rapid ADAS-Cog score changes) from the final analyses as their results were considered inconsistent with the overall population and may have been influenced by external factors. This was based on statistical investigations, clinical knowledge, and previous research suggesting that the greatest expected change in ADAS-Cog scores over a year is likely to be around 10 points [29]. The main disadvantage of excluding patients is that the data are less likely to be representative of the population as a whole which may affect generalizability. Furthermore, although the ADAS-Cog is commonly used in clinical trials, its scoring methodology has been criticized for having low sensitivity and reliability for measuring meaningful clinical change, particularly in earlier stages of the disease [30–32]. Finally, the use of the ADAS-Cog in the real world is rare and thus physicians (and their patients) who have used it in clinical practice may be inherently different from other AD providers and patients.
The results of this study suggest that the ADAS-Cog may be a useful tool for predicting the burden of the disease; however, further work is needed. The results should be interpreted cautiously as this was an exploratory observational study; however, the findings help understand the usage of the ADAS-Cog in real-world settings across multiple countries and the usefulness of the ADAS-Cog as a tool to understand the burden of AD.
In conclusion, this study confirms a relationship between increased HCRU and increasing ADAS-Cog scores (clinical progression) in a real-world population across a range of countries. There is still a way to go; however, these results may be a starting point in understanding the effects of AD therapies on clinical progression by providing a baseline upon which the success of treatment can be judged. The results highlight the importance of early intervention. Countries that employ interventions and strategies, which prevent or delay deterioration during the earlier stages of AD before dementia develops, may result in cost savings and benefit from lower HCRU requirements at the later more severe stages of the disease. Further research is needed to see if the ADAS-Cog can be used as a guide for decision-making and also to investigate country-specific differences.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank Nancy Milligan of Nancy Milligan Medical Ltd for preparing the draft manuscript on behalf of Adelphi Real World in accordance with the European Medical Writers Association guidelines. Medical writing support was paid for by Adelphi Real World.
Merck & Co., Inc. funded the research and had input into the study design, analysis of data, the writing of the report, and in the decision to submit the article for publication. Adelphi Real World designed the study, collected the data, and did all analysis and interpretation of data. Dr. Ritchie is funded by Merck and contributed to the analysis and interpretation of data, in the writing of the report, and in the decision to submit the article for publication.