
Abstract
Incidental memory can be defined as the ability to acquire information unintentionally. The present study investigated incidental memory performance in amnestic mild cognitive impairment (aMCI) and mild Alzheimer’s disease (AD) patients; additionally, hippocampal atrophy between groupswas examined. Twenty-nine aMCI patients (14 with hippocampal atrophy, measured by the Medial Temporal Lobe Atrophy scale), 15 mild AD patients, and 20 cognitively intact individuals underwent a detailed medical and neuropsychological assessment examining intentional memory, using the Hopkins Verbal Learning Test-Revised and the Brief Visuospatial Memory Test. Participants first took part in a driving simulator experiment, followed by an unexpected incidental memory questionnaire referring to elements related to the driving simulation. The mild AD group performed worse than the aMCI group and the control group both in incidental and intentional memory tasks, whereas the aMCI group differed significantly from the control group only in the intentional memory tasks. The incidental recognition memory task was the only measure that differed between aMCI patients with and without hippocampal atrophy. Moreover, incidental memory tasks were the only measures that correlated significantly with both left and right hippocampal atrophy. The current findings indicate that incidental memory testing may provide potentially useful information for detecting aMCI patients with greater hippocampal atrophy, who may be considered at higher risk of developing dementia due to AD.
Keywords
INTRODUCTION
Mild cognitive impairment (MCI) is considered to be the intermediate stage between normal aging and mild dementia [1]. Amnestic MCI (aMCI), which often progresses to Alzheimer’s disease (AD) dementia, involves memory impairments usually corroborated by an informant, objective episodic memory impairment; however, dementia is absent, and daily functioning as well as general cognitive functions are preserved [2–4].
Encoding and consolidation of information in episodic memory can be achieved, either intentionally, when the participants have the intention to learn and retain information, or incidentally, when information is acquired more automatically, without clear intention. Episodic memory impairment through intentional memory evaluation has been investigated extensively in MCI and AD, as it is a fundamental component of a typical neuropsychological assessment [5–12]. On the other hand, few studies have investigated incidental memory in patients with aMCI and mild AD.
In a recent study, Grönholm-Nyman, Rinne & Laine [13], investigated whether patients with aMCI and AD could incidentally retain definitions of unfamiliar objects. Their results showed that aMCI patients did not differ significantly from the control group in number of objects correctly identified or in the quality of the definitions retrieved. AD patients were poor in recalling object definition, and also recalled definitions less precisely than both aMCI patients and the control group. Moreover, Parra et al. [14] used an incidental memory paradigm to assess emotional memory in positive and neutral scenes. The incidental recognition task did not differ between aMCI patients and the control group. In contrast, AD patients performed significantly worse in the incidental recognition task compared to both the aMCI and control group. In conclusion, with regards to the aforementioned studies, incidental memory appears preserved in aMCI patients, and impaired in AD patients.
An fMRI study conducted by Mandzia and colleagues [15] examined incidental memory in aMCI patients using a levels-of-processing paradigm. In their experiment, pictures were presented to the participants while they were asked to make deep (natural versus man-made) and shallow (color versus black and white) decisions. In contrast to previous research, the results indicated that aMCI patients had an impaired ability to detect the correct pictures that had been encoded incidentally. In another study [16], incidental and intentional memory were investigated using a recognition task, assessing incidental superficial encoding and a free recall task, assessing intentional deep encoding. Their findings showed that the aMCI group performed significantly worse than the control group in both tasks.
There is agreement within the field, that AD patients have impaired incidental memory [17, 18]. On the other hand, results with regards to aMCI patients are mixed; some studies suggest incidental memory impairments [15, 16] whereas other studies indicate intact performance [13, 14]. A reason that could explain this discrepancy is the use of different methodological procedures for the assessment of incidental memory such as deep versus shallow encoding on the one hand [15, 16] and retrieval of information without previous warning [13, 14]. Furthermore, most studies focus only on the recognition process, not on free recall, the more demanding process [13–16]. Finally, the comparison between incidental and intentional memory has only been partially explored in one previous study, which, compared incidental recognition and intentional free recall, without comparing similar tasks regarding the nature of retrieval namely free-recall, cue-recall and recognition.
The primary objective of the present study was to investigate incidental memory performance in patients with aMCI and mild AD in comparison to healthy individuals. Incidental memory performance and intentional memory performance were also compared in order to evaluate the difficulties within the patient groups. Moreover, due to the important role of the hippocampus in episodic memory function [19–23], we sought to examine the relationship between the degree of hippocampal atrophy and incidental and intentional memory performance.
MATERIALS AND METHODS
Participants
The present study included 29 patients with aMCI, 15 patients with mild AD, and 20 cognitively intact individuals. The diagnosis of aMCI was made by an experienced behavioral neurologist (SGP) following the established criteria for aMCI [4], whereas the diagnosis of AD was made by the same authors following the McKhann et al. [24] diagnostic criteria. Participants were all right-handed and had to meet specific inclusion and exclusion criteria related to the methodology used: 1) a score equal to 0.5 (for aMCI patients) on the Clinical Dementia Rating scale (CDR) [25], 2) a CDR score equal to 1 (for mild AD patients), 3) a valid driving license, 4) regular driving, 5) no history of car accidents (within the last 2 years), 6) negative psychiatric history for psychosis, 7) absence of dizziness or nausea while driving, 8) absence of alcohol or any other drug addiction, 9) absence of any significant visual or movement disorder.
Ethical considerations
This study was completed in accordance with the Helsinki Declaration. The participants were informed that they will participate in the study voluntarily and that they had the right to withdraw any time they wished. All the participants were asked to sign an informed consent form that explained the nature of the study and their engagement. Moreover, participants were informed of the study procedure and were ensured of the anonymity and confidentiality of the experimental process
Procedure
The patients’ assessments were divided into two parts:
(A) Neurological/Neuropsychological Assessment: The participants went through a complete medical/neurological, neuropsychological, and ophthalmological assessment. During the neurological evaluation, a detailed medical history was provided and the participants and their relatives were asked to complete questionnaires about: 1) neuropsychiatric-behavioral symptoms: Neuropsychiatric Inventory [26], Frontal Behavioral Inventory [27], Geriatric Depression Scale [28]; 2) sleep quality: Epworth sleepiness scale [29], Athens Insomnia Inventory [30]; 3) motor disorders; and 4) functionality of everyday life: Functional Activities Questionnaire [31].
The neuropsychological assessment was extensive and detailed as it included measures from a range of cognitive functions in order to facilitate the clinical diagnosis [4, 24] as well as to obtain a deeper insight of the cognitive profile of the participants. Specifically, the following tests were administrated: Mini-Mental State Examination (MMSE) [32], Letter Number Sequencing (LNS) [33], Spatial Span Task [34], Trail Making Test (TMT) [35, 36], Useful Field of View (UFOV) [37], Judgment of Line Orientation Test [38], and the Psychomotor Vigilance Test (PVT). Because of their central role in the present study, the two intentional memory tests, Hopkins Verbal Learning Test-Revised [39] and Brief Visuospatial Memory Test-Revised [40], are subsequently described in-detail.
(B) Driving Simulator Testing: The driving simulator involved a motion base quarter-cab made by the FOERST Company, a 3 LCD wide screens 40” (full HD: 1920×1080 pixels), a driving position and a support motion base. The dimensions are 230×180 cm, while the base width is 78 cm, and, the total field of view is 170 degrees. The assessment of driving ability included driving for roughly 20 minutes in two different environments, rural and urban, in different driving conditions such as moderate or high traffic volume, and with or without the presence of an exogenous distraction. Incidental memory was evaluated through the driving simulator experiment, as recent studies suggest that virtual reality experiments, such as driving simulators, appear to be an ecologically valid way of assessing cognitive abilities [41–44].
Throughout the driving experiment, different elements were presented to the participants. Speed limit signs, in both rural and urban environments, were always presented twice, once at the beginning and once in the middle of the driving route. A warning sign for wild animal crossing was presented only in the rural environment, once at the beginning of each driving route. Furthermore, in the rural environment an 800-meter pond appeared in the background with a small floating boat. Moreover, during the experiment two unexpected incidents occurred. In the rural environment, an animal (donkey) suddenly appeared in the middle of the road, whereas in the urban setting a child suddenly appeared, chasing a red/orange ball. Finally, the driving in the rural environment occurred on a single carriageway, while in the urban environment it was on a dual carriageway, separated by guardrails.
Measures
Incidental memory
Incidental memory was evaluated using a questionnaire, designed by our research group that was presented immediately after the driving simulation. The first part of the questionnaire included a free recall task, in which, participants were asked to recall 8 elements from the driving simulation (Free Recall Score) presented in Fig. 1. The recognition task (Fig. 2) followed the free recall task, where participants were asked to select the correct answer among three alternatives (Recognition Score).

Incidental Memory Questionnaire – Free Recall task.
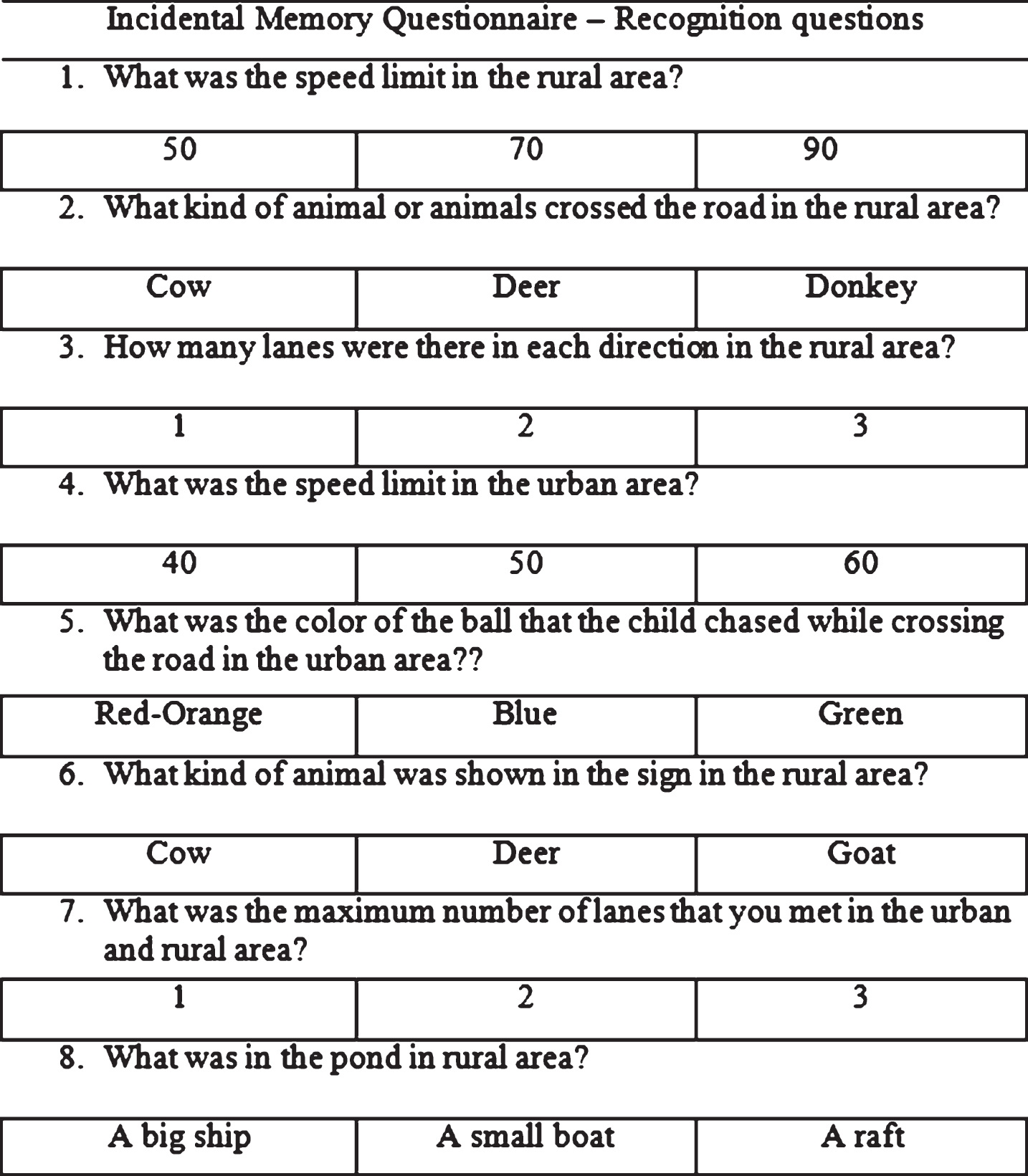
Incidental Memory Questionnaire – Recognition Task.
Hippocampal atrophy (HA)
The Medial Temporal Lobe Atrophy scale (MTA) [45] was used to assess HA. MTA is a five-point visual rating scale of HA where a score of 0 means normal and a score of 4 is equivalent to severe atrophy. The MTA is a widely used scale, which distinguishes AD patients from cognitively intact individuals with a sensitivity of 70–100% and a specificity of 67–96% [46–50]. In addition, it has good predictive value for the progression of MCI to AD [51–53].
In order to evaluate HA, all the participants had an MRI scan, which was obtained on a 1.5 Tesla MRI machine and MTA was rated on a coronal view of the brain. Based on the MTA scores, the aMCI group was separated into aMCI patients with HA and aMCI patients without HA. As a score of 1 is considered normal in patients above the age of 75 years old [52, 54], the group of aMCI patients without HA included patients below 75 years old who had a MTA score = 0, and patients above 75 years old who had a MTA score≤1while the group of aMCI patients with HA included patients below 75 years old who had a MTA score≥1 as well as patients above 75 years old with score in MTA scale≥2.
The MTA scores of the current sample of patients with aMCI and AD were evaluated by two expert behavioral neurologists, a rater (NA) and a reviewer (SGP). To test the reliability of the MTA scores between the rater (NA) and the reviewer (SGP), the unweighted κ for 2 raters was used. When the atrophy of the left hippocampus was considered, there were 4 discordances (κ= 0.761, p < 0.0001); when the atrophy of the right hippocampus was considered, there were 2 discordances (κ= 0.854, p < 0.0001). In the case that discordances were present, the reviewer’s MTA score was selected as the final measure.
RESULTS
Demographic characteristics
The demographic characteristics such as age and education of patients with aMCI, mild AD, and healthy individuals are presented in Table 1. Additionally, Table 1 includes measures that contributed to the diagnosis of the patients such as the general cognitive level measured by the MMSE [32], the depressive symptoms assessed by the Geriatric Depression Scale (GDS) [28], and the level of functionality measured by the Functional Activities Questionnaire (FAQ) [31].
Descriptive statistics of aMCI, mild AD and healthy controls
MMSE, Mini-Mental State Examination; GDS, Geriatric Depression Scale; FAQ, Functional Activities Questionnaire.
*p < 0.05,
**p < 0.001.
Age, MMSE total score and FAQ were significantly different between mild AD patients and control participants. More specifically, participants in the control group were significantly younger than the mild AD patients, had a higher score in MMSE, and a lower score in FAQ indicating a good functionality. In comparison to the aMCI group, mild AD patients had a significant lower score in the MMSE, as well as, a significantly higher score in FAQ representative of functionality disorders. No other significant differences were observed between the groups of the aMCI and the mild AD patients. Furthermore, no significant differences were observed between the aMCI patients and the control group.
Selecting the intentional and incidental memory task: Equivalent level of difficulty
The present study focused on the application of equal levels of difficulty between the incidental and the intentional memory tasks. Consequently, paired sample t-test analyses were performed on the control group to investigate the levels of difficulty between incidental and intentional memory (verbal and visuospatial) performances. The common scale, which compares tests, used the raw scores of incidental and intentional memory tasks which were converted into percentages, and is presented in Table 2.
Paired-Samples t-tests of incidental and intentional memory performances
HVLT Tr1, the first learning trial of the Hopkins Verbal Learning Test; HVLT Tr2, the second learning trial of the Hopkins Verbal Learning Test; HVLT Tr3, the third learning trial of the Hopkins Verbal Learning Test; BVMT Tr1, the first learning trial of the Brief Visuospatial Memory Test; BVMT Tr2, the second learning trial of the Brief Visuospatial Memory Test; BVMT Tr3, the third learning trial of the Brief Visuospatial Memory Test.
*p < 0.05,
**p < 0.001.
The results indicated that healthy individuals have a similar performance (non-significant difference) in the following tasks: 1) incidental memory task with the second learning trial of HVLT–R (intentional verbal memory), and 2) incidental memory task with the second learning trial of BVMT-R (intentional visuospatial memory). Regarding the other learning trials of HVLT–R and BVMT-R, the applied analysis revealed significant differences between the incidental and intentional performance.
Differences in incidental and intentional memory among aMCI, AD, and healthy participants
In order to investigate the differences in incidental and intentional memory performance, age needed to be controlled for, as it was found to be significantly different between AD patients and the control group. Therefore, an analysis of covariance (ANCOVA) was carried out with the variable of age as a covariate. The data from the free recall tasks as well as from the recognition tasks were analyzed accordingly. The results of the ANCOVA analysis are presented in Table 3. Post hoc comparisons with Bonferroni correction as well as d values of the effect size were also calculated.
Differences in memory performance among aMCI, AD & healthy participants
*p < 0.05,
**p < 0.001.
After applying the Bonferroni correction, the results of post hoc comparisons revealed that in comparison to the control group, aMCI patients performed worse in the intentional verbal memory task, in the free recall (d = 1.23), and the recognition tasks (d = 0.87). Patients with mild AD performed significantly worse than the healthy individuals in incidental recall (d = 1.33), and recognition (d = 1.67), intentional verbal recall (d = 2.39), and recognition (d = 1.43), and intentional visuospatial recall (d = 2.35). Compared to aMCI patients, mild AD patients performed significantly worse in incidental recognition (d = 1.22) and intentional visuospatial recall (d = 1.47).
Differences in incidental and intentional memory between aMCI patients with and without HA
Subsequently, incidental and intentional memory performance was examined in aMCI patients: 1) aMCI patients with HA and 2) aMCI patients without HA. The demographic characteristics of these groups are presented in Table 4. Independent samples t-tests were carried out in order to identify differences in incidental and intentional memory between aMCI subgroups. The results are presented in Table 5.
Demographic characteristics of aMCI patients with and without HA
MMSE, Mini-Mental State Examination; GDS, Geriatric Depression Scale; FAQ, Functional Activities Questionnaire.
Differences in memory performance among MCI with and without HA
*p < 0.05,
**p < 0.001.
In comparison to aMCI patients without HA, aMCI patients with HA performed significantly worse only in the incidental recognition task (d = 1.03). No significant differences were observed between subgroups in the intentional memory tasks.
Association of incidental and intentional memory tasks with HA
Spearman’s correlation analyses were carried out in order to demonstrate the association between incidental and intentional performance in aMCI patients with HA and AD patients. Table 6 sets out the results from this correlation analyses.
Spearman’s correlations between memory variables and HA
*p < 0.05,
**p < 0.001.
The results from the correlation analyses demonstrated that only incidental recall (r = –0.56, p = 0.000, r = –0.65, p = 0.000) and recognition (r = –0.64, p = 0.000, r = –0.72, p = 0.000) tasks were significantly associated with the right as well as the left hippocampi. Moreover, the high correlation coefficient values indicated a strong effect size. On the contrary, none of the intentional verbal (r = –0.18, p = 0.264, r = –0.09, p = 0.542) and visuospatial (r = –0.18, p = 0.244, r = –0.16, p = 0.298) memory tasks correlated significantly with the left or the right hippocampi.
DISCUSSION
The aim of the present study was to investigate incidental versus intentional memory performance of patients with aMCI and mild AD compared to cognitively intact individuals. Considering the fact that incidental memory has an important role in everyday life and is difficult to assess during typical neuropsychological assessment, we decided to examine incidental memory through a virtual-reality driving experiment that resembles a condition of everyday life [55–59]. The results of this study indicated that mild AD patients performed worse than aMCI patients and the control group in incidental and intentional visuospatial memory tasks, but not in verbal memory tasks. In comparison to the control group, aMCI patients had a significant attenuation of performance only in intentional memory. When we separated the aMCI group to aMCI patients with or without HA, the only memory measure that appeared to differentiate between the two subgroups was the incidental recognition task, in which aMCI patients with HA performed significantly worse than aMCI patients without HA. In addition, the incidental memory tasks were the only memory measures that strongly correlated with both right and left HA scores in patients with aMCI and mild AD.
Our findings are in accordance with two previous studies [13, 14] that indicated that aMCI patients manifest impaired memory performance only when additional effort to memorize is demanded as is the case for intentional memory tests; whereas their ability to remember information that has been incidentally encoded appears to be similar to cognitively intact individuals. However, the aforementioned studies have not compared incidental versus intentional memory performance in the same groups.
In contrast to our findings, previous studies have detected impairments in incidental memory in patients with aMCI [15, 16]. Both studies [15, 16] evaluated incidental memory through an experimental design based on the level-of-processing theoretical framework and in those experiments the ability to retain information incidentally was associated with the level of processing during the encoding of information (deep or shallow). The methodological approach followed guides the participants to focus on the information tested by making judgments that are considered to reflect deep or shallow encoding. As the participant’s attention is guided, the incidental nature of encoding can be questioned. Moreover, a condition of shallow encoding does not necessarily exclude that some aspects of information are processed under deep encoding as well [60].
With regards to incidental memory in patients with AD, our results corroborate previous studies [13, 18] demonstrating that incidental memory tasks can discriminate patients with AD from healthy individuals. Nonetheless, to the best of our knowledge, our study is the first to investigate both incidental and intentional memory and to examine the difference between AD groups when compared to cognitively healthy individuals. According to our results, the effect sizes that were observed indicate more pronounced differences between the mild AD and the control group in the case of intentional verbal and visuospatial recall in comparison to the recall condition of the incidental memory task. The above findings are along the same trajectory with those observed in the aMCI group indicating that intentional memory tasks are more demanding than incidental memory tasks for the specific clinical group. However, regarding mild AD patients, impairments in incidental memory were also apparent. Therefore, our results suggest that the progression from MCI to mild AD may be related more to the deterioration of incidental memory function. Nonetheless, future research is warranted in order to increase our insight regarding this issue.
The only memory task that differed between aMCI patients with and without HA was incidental recognition. This difference suggests that the underlying memory deficit of aMCI patients with HA are linked to the consolidation process of incidentally encoded information. Previous studies [61] have demonstrated that the concurrent use of both recall and recognition tasks is the most appropriate testing method for elucidating retrieval from retention deficits. Our results are in line with the prominent view that even under incidental encoding of information, storage and consolidation of new information is associated with the hippocampus and the adjacent cortical areas [62–65].
We have found that in aMCI and mild AD patients the atrophy of both right and left hippocampi was significantly associated with the incidental memory tasks. The findings from the correlation analysis combined with previous results from the ANCOVA analysis provide strong evidence of the relationship between the hippocampus and incidental memory. This is in accordance with previous brain imaging studies in cognitively intact individuals, which have revealed that the hippocampus plays a central role during incidental memory tasks [66–68]. To the best of our knowledge, this is the first study to investigate the relationship between incidental memory tasks with hippocampal damage, especially in patients with aMCI and HA. Our findings regarding the absence of association between HA and intentional memory performance could be explained by the findings of previous studies in cognitively intact individuals [66, 69–71] that have shown that additional brain regions including the prefrontal lobe, parietal cortex, and the cingulate gyrus are also heavily involved in the process of intentional memorization of information.
Overall, our results in aMCI patients demonstrate that while intentional memory impairment is present, incidental memory remains intact in those patients without HA. As the present study indicated a strong association of incidental memory performance with HA, it may be suggested that the addition of incidental memory testing could provide useful information that can help distinguish aMCI patients, who are at greater risk of developing dementia due to AD.
A limitation of the study that should be taken under consideration is the presence of adequate statistical power only in the case of large effect sizes because of the relatively small sample size. The extensive and multimodal assessment in combination with the strict exclusion and inclusion criteria that the participants had to meet regarding their clinical and driving status restricted the recruitment of more patients with aMCI and mild AD. Nonetheless, this constraint does not appear to influence the direction of the findings that were observed in the current study. Another restriction of the present study that needs to be recognized is the use of a visual rating scale instead of a more modern brain imaging approach. Nonetheless, the MTA scale is used often use as a measure of hippocampal atrophy and is strongly related to volumetric measures [47, 72]. In addition, the level of agreement between the rater and the reviewer was at least satisfactory regarding the MTA measures of the current study. Nonetheless, the application of modern brain imaging techniques has the capacity to expand the findings of the present study and appears to be a reasonable target for future work in the field. Finally, an additional goal of prospective research could be the design of longitudinal studies with patients with MCI in order to explore the relative risk of progressing to AD according to their performance on incidental memory tasks.
Footnotes
ACKNOWLEDGMENTS
This research was carried out within the framework of the Operational Program “Education and Lifelong Learning” of the National Strategic Reference Framework (NSRF), namely the Research Funding Program: THALES Investing in knowledge society through the European Social Fund (Grant agreement No: 10969/09-07-2012), and the Action: ARISTEIA (Action’s Beneficiary: General Secretariat for Research and Technology) (Grant agreement No: 15765/30-11-2012), co-financed by the European Union (European Social Fund - ESF) and Greek national funds. The authors received no other funding for this study.