
Abstract
Early-onset Alzheimer’s disease (EOAD) accounts for 1–5% of Alzheimer’s disease cases and is associated with specific ethnicities. It has been our impression that non-Ashkenazi Jews have a higher rate of EOAD and we therefore explored this hypothesis. We performed a retrospective case control study of EOAD cases referred to our cognitive neurology clinic between January 1999 and December 2016. Patients (n = 129) were compared to age- and geographically-matched controls generated from the Second Israeli National Health Survey (n = 1,811). Data on country of origin, education, dementia family history, depression, and vascular risk factors were compared between the groups. The association of non-Ashkenazi Jewish heritage and country of origin with EOAD was calculated using a logistic multivariate regression model. The EOAD group’s mean age was 59.6±4.1 years, with a female predominance (64.3%). The EOAD group had a higher percentage of individuals of non-Ashkenazi Jewish origin (64.3% versus 51.4%, p = 0.003) and of Yemenite descent in particular (16.28% versus 6.24%, p < 0.001). On multiple logistic regression analysis, Yemenite Jewish origin was an independently associated with EOAD (OR 2.54, 95% CI 1.4–4.8). There were no significant differences in parameters between non-Ashkenazi and Ashkenazi Jews. Only 4.6% of EOAD cases had a positive EOAD family history. In conclusion, EOAD is over-represented among non-Ashkenazi Jews. Yemenite origin is independently associated with EOAD and the majority of patients with EOAD have no family history of Alzheimer’s disease. Further evaluation with genetic studies is warranted.
Keywords
Introduction
Early-onset Alzheimer’s disease (EOAD) is defined as the development of dementia before the age of 65 years. It affects approximately 1–5% of all patients with Alzheimer’s disease (AD) [1, 2]. The estimated prevalence is 40–100 per 100,000 in the 40–64-year age group [1]. Some cases of EOAD are due to autosomal dominant mutations in genes coding for the amyloid precursor protein, presenilin 1 or presenilin 2. In cases without a clear family history, the disease is presumed to be due to a combination of genetic and environmental factors. These cases are referred to as sporadic EOAD as opposed to familial EOAD.
Late-onset Alzheimer’s disease (LOAD) is considered to be a sporadic disease. Studies of LOAD have implicated many risk factors, including possession of an APOE4 allele [3], cerebrovascular disease, dyslipidemia [3], hypertension [3], diabetes, head trauma [4], physical inactivity [5], and other factors. It is unclear if these risk factors apply to EOAD and if they affect the age of onset or clinical progression of EOAD.
Previous studies have also pointed to a role of ethnicity/race factors in the prevalence and incidence of LOAD and EOAD [6–15]. Higher rates of LOAD have been reported in African-Americans, Hispanics, Native Americans, Aboriginal communities of Canada, and Arabs from Northern Israel, as well as other ethnicities [6, 16–22]. Higher rates of EOAD have been reported in Native Americans, Native Alaskans, and African-Americans [17].
Selective ethnic populations have been shown to harbor genes which confer a risk for the development of LOAD with variable prevalence. The effect of these mutations may also be subject to complex gene-environmental interactions. For example, the APOE4 allele poses a lower risk of LOAD in African-Americans than in Caucasians [23], and its carrier rate is relatively low in Asians and almost negligible in Northern Israeli Arabs [24, 25]. A study of American Hispanics with mild cognitive impairment found no significant association of the disease with APOE4 carrier status, educational attainment, gender, and the Hachinski ischemic scale score [26]. A study of an Israeli Jewish cohort without dementia reported that the estimated prevalence of the APOE4 allele was 0.1 in the non-Ashkenazi Jewish population and 0.095 in the Ashkenazi Jewish population [27]. These rates are similar to those previously reported in the Caucasian populations [28].
Selective populations may harbor specific mutations that alter the susceptibility for LOAD. The A673T variant of the amyloid precursor protein has been shown to confer protection from LOAD in an Icelandic population [29]. It apparently recurs in populations from Nordic countries but is extremely rare in non-Nordic populations [30].
The population of Israel is a unique composite of individuals of diverse ethnic and cultural origins due to mass immigrations from dozens of communities worldwide [31, 32]. According to the Israel Bureau of Statistics, in 2016, there were 646,100 Ashkenazi Jews and 689,350 non-Ashkenazi Jews between the ages of 40 and 64 years residing in the country.
In an epidemiological study conducted in Israel of all-cause dementia that incorporated data on ethnicity, Khana et al. [12] evaluated a cohort of 1,501 individuals aged 75 years or more from the medium-sized southern city of Ashkelon. They found that the prevalence of dementia was significantly higher in non-Ashkenazi than Ashkenazi Jews (p = 0.016) and suggested that the significantly fewer years of education of the non-Ashkenazi group could at least partly account for this difference. However, another study of 998 elderly individuals from Jerusalem reported that after controlling for education, non-Ashkenazi ethnicity remained a risk factor for LOAD [13]. Treves et al. [23] evaluated the incidence of EOAD in Israel and noted a higher rate in Ashkenazi than non-Ashkenazi Jews.
In recent years, it has been our impression that most cases of EOAD diagnosed in our clinic are sporadic, and most of the Jewish patients with EOAD are of non-Ashkenazi origin. These observations prompted the present study of ethnic-racial differences among patients with EOAD attending our clinic in the last 17 years. We compared the origin, demographic and medical data of our EOAD group to a non-demented control group (age and geographically matched). The comparison revealed a higher prevalence of EOAD in non-Ashkenazi Jews, especially in the Yemen origin subgroup.
METHODS
A retrospective comparative cohort study design was used. The electronic database of the Cognitive Neurology Clinic of Rabin Medical Center, a tertiary university-affiliated hospital, was screened for all patients diagnosed with AD from 1999 to 2016. The diagnosis (probable or possible) was ascertained using the 2011 guidelines of the National Institute on Aging-Alzheimer’s Association Workgroups [33]. Patients diagnosed before 65 years of age and of Jewish origin (both maternally and paternally) were identified, and their medical records were reviewed by two independent cognitive neurology specialists. Those with trisomy 21, traumatic brain injury, HIV infection, previous encephalitis or s/p brain surgery were excluded, as were patients found to have another type of dementia on follow-up (vascular, frontotemporal, Lewy body, or Parkinson’s disease). The remaining subjects were included in the EOAD study group by consensus of the two independent reviewers.
The control group was derived from the Second Israeli National Health Interview Survey [34] carried out in 2007–2010 as part of the EUROHIS project of the World Health Organization. A total of 10,331 Israelis age 21 years or more were interviewed by phone in Hebrew, Arabic, or Russian, as required. The survey collected data on demographics, years of formal education, ethnic origin, morbidity, smoking status, and chronic medical conditions (diabetes, hypertension, dementia, and depression). For the present study, the survey database was screened for cognitively healthy Jewish subjects aged 40 to 64 years, residing in the same central Israel and Tel Aviv districts as the EOAD group.
The following data were recorded for the EOAD and control groups from the medical records and the survey database: age at diagnosis/initial interview, country of origin, years of formal education, presence of vascular risk factors (smoking status, diabetes, and hypertension), and previous diagnosis of a depressive disorder. For subjects born in Israel, we used the parental country of origin. If the country of origin could not be elicited from the records, the subject was excluded from the analysis. Data regarding family history of dementia (parents and siblings) and age at onset (reported by subject or spouse) were documented as well.
Subjects were categorized as non-Ashkenazi if they or their parents originated from Yemen, Morocco, Iran, Iraq, India, Italy, Brazil, Greece, Libya, Turkey, Kazakhstan, Tunis, Egypt, Dagestan, Bulgaria, Syria, Lebanon, Uzbekistan, Spain, Serbia, Bosnia and Herzegovina, Bolivia, Georgia, France, Cyprus, Afghanistan, or Azerbaijan. Subjects were categorized as Ashkenazi if they or their parents originated from Poland, Russia, Estonia, Austria, Moldova, Netherlands, Canada, Latvia, Lithuania, Czech Republic, Belgium, Croatia, Ukraine, Belarus, Romania, Slovakia, Germany, Argentina, Chile, Uruguay, Hungary, South Africa, United Kingdom, or United States (Fig. 1).
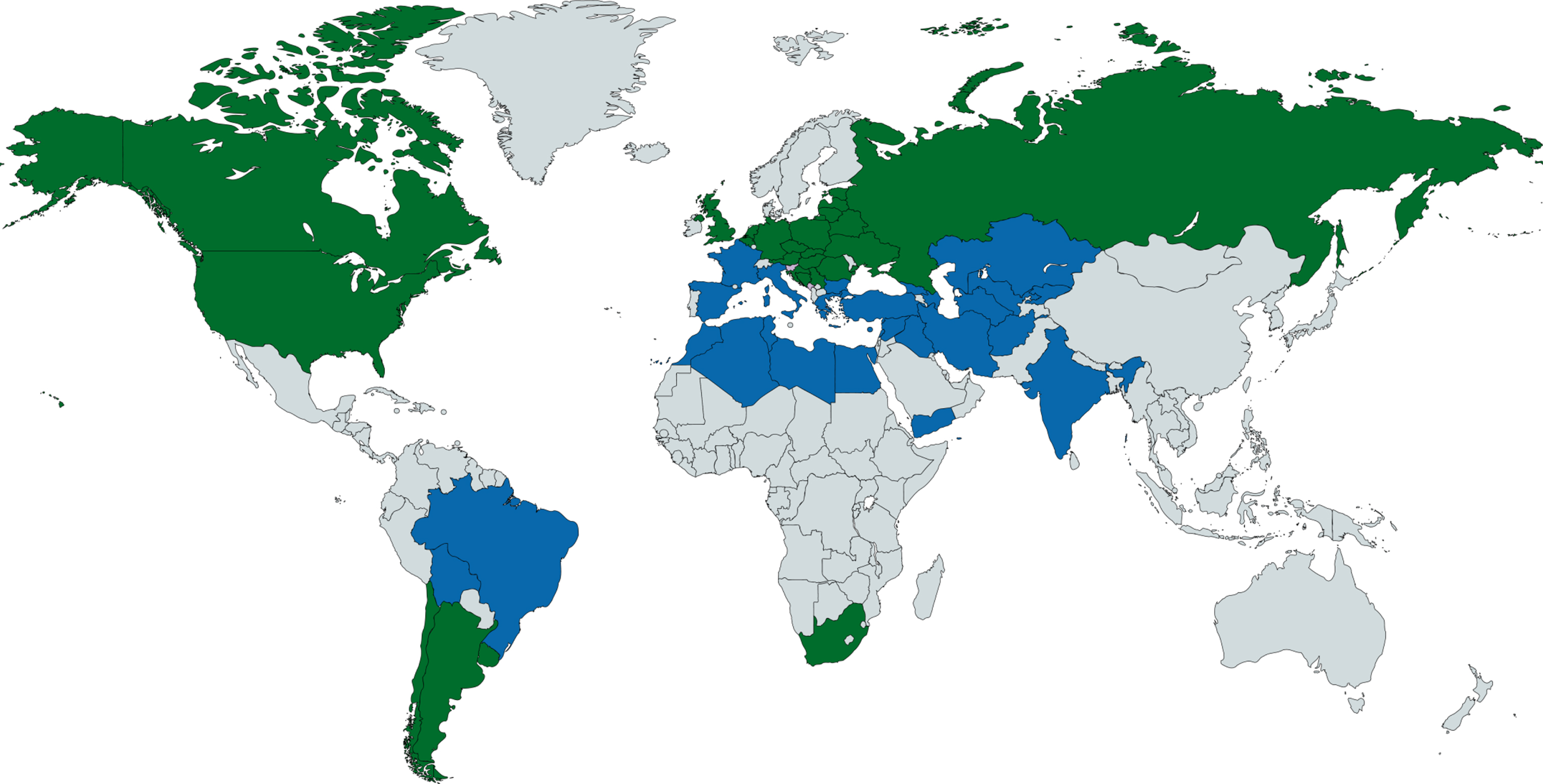
World map (made via mapchart.net). Countries of origin of Ashkenzi Jews (labeled in black) and Non-Ashkenazi Jews (labeled in dark grey). Countries not denoted in this study are shown in light gray.
The data collection and analysis protocols were approved by the local Institutional Review Board. All subjects were included anonymously. The need for informed consent was waived because of the retrospective study design.
Statistical methods
Categorical variables [ethnicity, gender, vascular risk factors, and years of education (<8 or ≥8)] were summarized as number and percent deviation, and continuous variables (age, years of education) as mean and standard deviation. A chi-square test was used to analyze differences in categorical variables between the EOAD and control groups, and a t-test was used for continuous variables. The data were fitted to a multiple logistic regression model to examine the combined relationship of demographic and vascular risk factors with the risk of EOAD. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated as estimates of relative risk. A p-value less than 0.05 was considered significant. Statistical Analysis Software (SAS V. 9.4; SAS Institute Inc., Cary, NC, USA) was used for all statistical analyses.
Results
Of the 982 patients diagnosed with AD at our clinic during the study years (Fig. 2), 772 had LOAD and 65 were further diagnosed with non-Alzheimer’s dementia upon follow-up. An additional 16 were excluded for medical reasons (Down syndrome, 3 patients; schizophrenia/schizoaffective disorder, 2 patients; and HIV positivity, traumatic brain injury, cerebral malignancy, and s/p encephalitis, 1 patient each) or background factors (unknown country of origin, 3; non-Jewish origin, 4). The remaining 129 patients with EOAD (125 probable, 4 possible) formed the study group. There were 83 women and 46 men of a mean age of 59.6±4.1 years with 63% of subjects at or above the age of 60 at their initial interview and 13% at or below the age of 54.
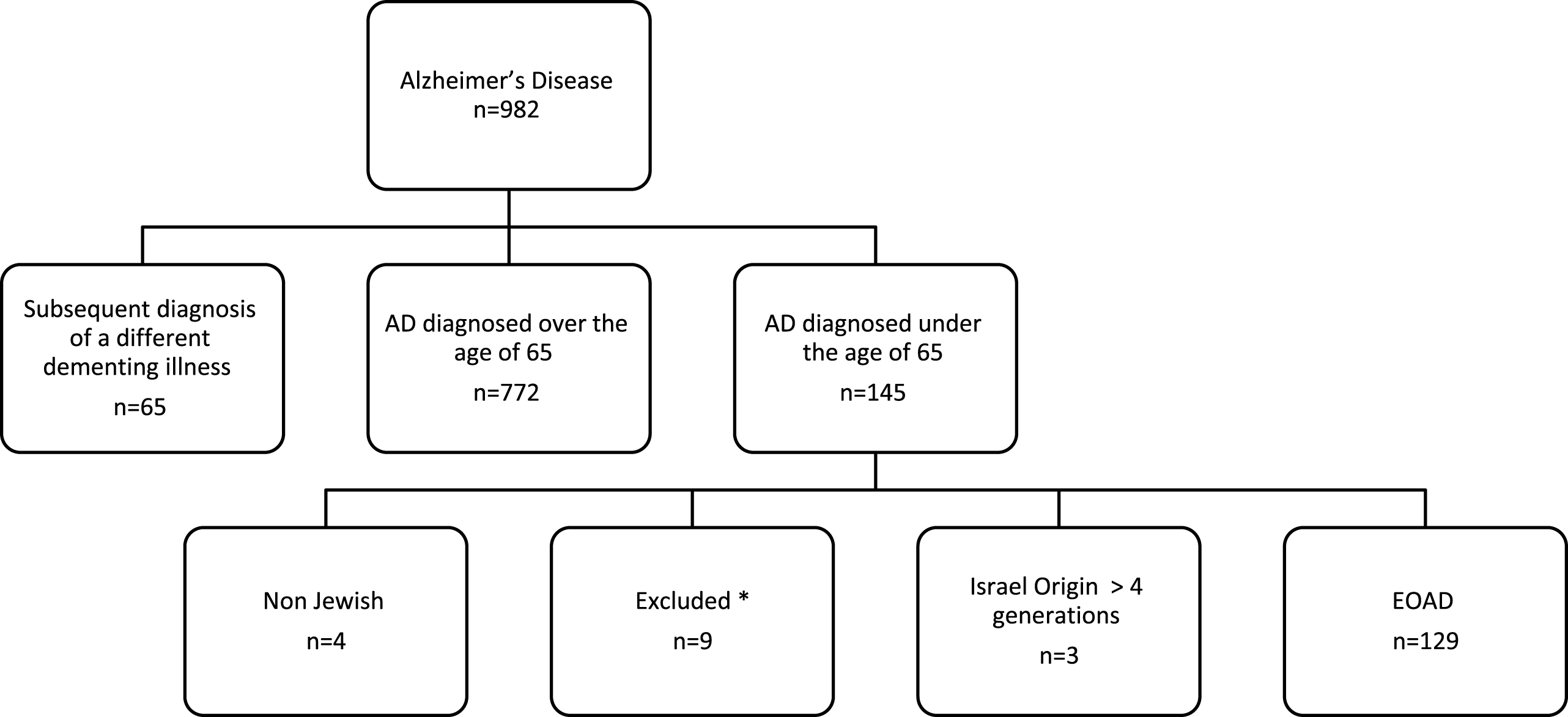
Patient inclusion and exclusion algorithm. All cases were reviewed by two cognitive neurology specialists. *Excluded due to the following comorbidities: Down syndrome (3 patients), HIV positive status (1 patient), schizophrenia/ schizoaffective disorder (2 patients), traumatic brain injury (1 patient), cerebral malignancy (1 patient), status post severe encephalitis (1 patient).
Mean Mini-Mental State Examination (MMSE) score at presentation was 22.43±4.08 with 29 patients having moderate to severe dementia (MMSE < 20) at the initial visit. The control group consisted of 1,811 age- and geographically-matched cognitively healthy subjects: 1,033 women and 778 men.
Comparison of the two groups for sociodemographic variables and vascular risk factors (Table 1) revealed that the EOAD group was characterized by a significantly higher prevalence of diabetes (21.7% versus 5.0%, p < 0.001), hypertension (34.1% versus 21.1%, p < 0.001), and depression (12.4% versus 2.7%, p < 0.001). The EOAD group also had significantly less education (mean school years 11.4±3.5 versus 14.0±3.1, p < 0.001) and a greater likelihood to have only an elementary level education (0–8 school years) or no formal education (20.1% versus 5.6%, p < 0.001). There was no between-group difference in the rate of smokers (17.8% versus 25.6%, p = 0.58).
EOAD by sociodemographic variables and vascular risk factors
Data are presented as mean±SD or percentage. EOAD, early onset Alzheimer’s disease.
Twenty-nine patients in the EOAD group had a positive family history of dementia in a first-degree relative: parental late onset dementia in 20 (15.5% of the study group), early-onset dementia in 6 (4.6%), and dementia of unknown age of onset in 3 (2.3%). One patient had a history of dementia in more than one first-degree relative. Family history of dementia in the oldest (ages 60–64), middle (ages 55–59), and youngest EOAD groups (ages below 54) was present at a rate of 15%, 25%, and 25% in each group, respectively. A family history of early onset dementia was present in 12.5% of the youngest EOAD group and scarce in the older patients (2.4%).
Non-Ashkenazi Jews accounted for 64.3% of the EOAD group compared to 51.4% of the control group (p = 0.003). On evaluation of the relationship between demographic and vascular risk factors with EOAD using a multiple logistic regression model, no significant association was found of non-Ashkenazi Jewish origin with EOAD (OR 1.3 95% CI 0.8–2.0, p = 0.17). However, subanalysis of the non-Ashkenazi subjects by specific country of origin revealed that the largest subgroup diagnosed with EOAD were those of Yemenite descent (n = 21). Yemenite Jewish ancestry proved to be a significant independent association with EOAD after controlling for risk factors (OR 2.43, 95% CI 1.4–4.2) (Table 2). A family history of dementia was documented in six Yemenite patients with EOAD (27%): five had a family history of late-onset dementia, and one had a family history of early-onset dementia (4.8%). None of the other ethnic subgroups within the non-Ashkenazi or Ashkenazi groups had a significantly higher risk for EOAD.
Logistic regression model of factors affecting EOAD
CI, confidence interval; EOAD, early onset Alzheimer’s disease.
Comparison of the risk factors between the Ashkenazi and non-Ashkenazi patients with EOAD revealed a significantly lower mean number of years of education in the non-Ashkenazi patients (12.8±2.75 versus 10.8±3.5, p < 0.001). There was no significant difference between the groups in any of the other parameters investigated.
DISCUSSION
This study compared the prevalence and risk factors of EOAD between Ashkenazi and non-Ashkenazi Jews in an Israeli population. The results demonstrated that EOAD was significantly over-represented in the non-Ashkenazi patients. Further analysis using a regression model adjusted for age, gender, education (in years), diabetes, hypertension, smoking status, and depression yielded a non-significant association of non-Ashkenazi Jewish origin with EOAD.
Vascular risk factors, age, and education have been suggested as risk factors for LOAD (Table 1) and may contribute to the higher prevalence of EOAD in non-Ashkenazi Jews. However, we found no significant difference in vascular risk factors between the Ashkenazi and non-Ashkenazi patients with EOAD, and it remains unclear if vascular risk factors are as important in EOAD as they are in LOAD [35–37]. Few studies have investigated the role of vascular risk factors and patient education levels in EOAD [9, 38], or in any type of early-onset dementia [39], and our study is not sufficiently powered to significantly assess this interaction. It is possible that our observation was a consequence of a complex gene-environment interaction affecting non-Ashkenazi Jews, similar to findings in other ethnicities [23–26, 40].
It is assumed that Non-Ashkenazi Jews migrated from ancient Israel to locations in the Middle East and North Africa following conquests by the Babylonians (586 BCE) and Romans (70 CE). The non-Ashkenazi Jewish diaspora communities were usually isolated from the surrounding non-Jewish population. They married among themselves and maintained a unique way of life and tradition. Despite their geographic variability, they share similar religious rituals and practices. The vast majority immigrated to Israel soon after its foundation in 1948. Even today, Ashkenazi and non-Ashkenazi Jews in Israel attend separate synagogues, have different chief rabbis, and practice diverse religious rituals. Genetically, non-Ashkenazi Jews are more strongly related to other members of their community and other non-Ashkenazi Jewish communities in different geographic regions (e.g., Mediterranean and Middle Eastern countries) than to any non-Jewish or Ashkenazi Jewish populations [31].
In the present study, Jews of Yemenite origin were significantly over- represented in the EOAD group, and Yemenite Jewish origin continued to be a significantly associated with EOAD after controlling for other known AD risk factors. Yemenites are a small discrete ethnic subgroup of non-Ashkenazi Jews. They are believed to have migrated to the southern end of the Arabian Peninsula at around the time of the destruction of the first Hebrew temple (∼2500 years ago).They remained geographically isolated from other Jewish populations of the diaspora and established closed community structures [32]. From 1948 to 1951, more than 47,000 Yemenite Jews immigrated to Israel. They were found to harbor several distinct genetic diseases, including spinocerebellar ataxia type 3 (Machado-Joseph syndrome) and metachromatic leukodystrophy [41, 42]. They also have a significantly higher prevalence of diabetes than the general Israeli population [43]. The clinical phenotype of several neurodegenerative diseases such as Parkinson’s disease differs between Yemenite and Ashkenazi Jews. Parkinson’s disease onset is earlier in the Yemenite Jews, and the course is more severe and rapidly progressive. Furthermore, the cognitive decline associated with Parkinson’s disease is more prevalent in Yemenite Jews than in Ashkenazi Jews [44].
The prevalence of family history of dementia in our EOAD subjects varied according to subject’s age and was between 16% to 25%. A surprising observation in our study was the low rate of a family history of early onset dementia in our cohort (4.2%) compared to reported rates in earlier studies (17.5–60%) [37, 45–47]. The low rate of early onset dementia family history persisted in our younger EOAD patients (ages below 54). A possible explanation for the absence of a clear familial history of AD is that some of our subjects possess APOE4 alleles. Possession of APOE4 alleles has been shown to increase the risk of AD and reduce its age of onset [48, 49]. Only one previous study evaluated the prevalence of the APOE4 in non-Ashkenazi Jews [27] and reported carriage rates between 0.07–0.1 depending on country of origin. This rate was similar to previously reported rates in Ashkenazi Jews [28]. The rate of APOE2 allele was previously compared and found 8 fold higher in Ashkenazi than Yemenite Jews [50], but it does not imply a higher APOE4 rate in this group. Thus the effect of APOE4 could be modulated by several gene-environmental interactions in Non Ashkenazi Jews, as seen in African-Americans [23, 40].
We postulate that cases of EOAD in our cohort were sporadic and not due to a known autosomal dominant familial AD mutation. Nearly all cases of familial EOAD are transmitted in an autosomal dominant inheritance pattern with full penetrance, which is scarce in our EOAD group. Whether APOE4 plays a role has not been substantiated and the evaluation of APOE allele in our subjects is beyond the scope of our study. Since we did not perform genetic analyses, the nature of the genetic risk factors in our cohort is incomplete.
The present study is limited by the retrospective design which prevented verification of a causal relationship between ethnic origin and EOAD. Furthermore, the study group was restricted to patients attending our tertiary medical center. However, the likelihood of this setting leading to an under-representation of EOAD cases is low given that the alarming phenotype of early-onset dementia usually warrants prompt evaluation in a dedicated cognitive clinic or tertiary care center. By contrast, patients with LOAD are far more likely to be managed in the community by primary care physicians. Therefore, to avoid bias, we did not perform a similar comparison of individuals with LOAD.
In conclusion, we observed a higher prevalence of EOAD in non-Ashkenazi Jews, specifically those of Yemenite origin, in our cohort. The results should be confirmed in prospective cohorts and further evaluated with genetic studies.