
Abstract
Background:
Alzheimer-associated neuronal thread protein (AD7c-NTP) has been found to be a biomarker for Alzheimer’s disease (AD).
Objective:
The aim of the present study was to investigate the distribution of Alzheimer-associated neuronal thread protein and its relationship to common chronic diseases in the general population.
Methods:
Urine samples of 1,805 participants were collected from four districts (Xi Cheng, Fang Shan, Tong Zhou, and Yan Qing) in Beijing. The assessment in this study included a questionnaire that captured participants’ demographic information, use of medication and histories of disease, neurological examinations, psychometric evaluations, physical and clinical examinations, and laboratory tests.
Results:
Urine AD7c-NTP level was increased among the population over 60 years old and females exhibited higher levels than males. These results controlled for other demographic factors such as education levels, employment status, body mass index and current residence. The urine AD7c-NTP levels exhibited no association with non-neurological diseases (0.3346±0.4482 ng/ml), such as hypertension (0.3445±0.4187), stroke (0.3652±0.4010), diabetes (0.3319±0.4371), dyslipidemia (0.3440±0.4314), renal insufficiency (0.3223±0.3909), cancer (0.5055±1.0006), chronic lung disease (0.2911±0.2852), chronic liver disease (0.5579±0.6726), severe depression symptoms (0.5186±0.7040), and mild depression symptoms (0.3669±0.3811).
Conclusions:
Cut-off values for urine AD7c-NTP levels for different age groups and genders should be established. AD7c-NTP levels proved relatively stable in the body and were not impacted by demographic factors or common chronic diseases.
INTRODUCTION
Alzheimer’s disease (AD) is a progressive and fatal neurodegenerative disorder manifested by cognitive and memory deterioration, progressive impairment of daily activities, and a variety of neuropsychiatric symptoms and behavioral disturbances [1]. Currently there are more than 26.6 million AD patients worldwide. As the world population ages, the number of AD patients is expected to reach more than 106.2 million by 2050; one of every 85 persons will live with AD [2]. The onset of AD is often hidden and the disease seems to be irreversible. To date, no effective treatments to prevent, halt, or reverse it are available. What therapies exist only alleviate or postpone clinical symptoms [3]. Diagnostic tests have moved the field closer to the development of effective AD biomarkers to facilitate early diagnosis and to improve clinical care [4, 5]. Therefore, simple and non-invasive biomarker tests for early detection of AD would prove invaluable, especially those that could be performed during a routine clinical screening for the elderly.
Alzheimer-associated urine neuronal thread protein (AD7c-NTP) is a member of the neuronal thread protein family with a molecular weight of approximately 41 kD. As a potential biomarker of AD, it is closely related to the pathophysiology of the disease. Previous studies demonstrated that AD7c-NTP immunoreactivity co-localized with tau-immunoreactive neurofibrillary tangles and dystrophic neurites, and abnormal AD7c-NTP gene expression precedes the formation of neurofibrillary tangles [6, 7]. Elevated levels of AD7c-NTP are detectable in cortical neurons, brain tissue extracts, cerebrospinal fluid (CSF), and urine in the early course of AD [8–10]. From 1996 when AD7c-NTP was first discovered and reported by de la Monte et al. [6], to the present, a number of studies have confirmed and further developed understandings about the association between the protein and AD; these studies have focused on the improvement of detection methodologies [10–14], the validation of clinical multi-facility measurements [15–17], and the combination of the protein with other biomarkers [18–20].
Due to a lack of large-scale epidemiological data for urine AD7c-NTP and a dearth of studies on the physiological variations of urine, some important questions remain. First, the distribution of urinary AD7c-NTP in the general population is unclear. Second, whether or not the levels of urinary AD7c-NTP are associated with non-neurological diseases is unknown. Thus, we measured the urinary concentrations of AD7c-NTP in 1,805 human urine samples obtained via a community-based survey. The focus on the general population permitted a deep examination of a spectrum of the disease as well as of confounding factors that could potentially impact AD7c-NTP levels. The purpose of the survey was to investigate the level of urine AD7c-NTP in relation to demographic factors and common diseases among the Chinese population.
MATERIALS AND METHODS
To investigate the distribution of AD7c-NTP and its relationship to common chronic diseases in the general population, the urine AD7c-NTP levels of 1,805 participants were detected, and the assessment in this study included a questionnaire that captured participants’ demographic information, use of medication and histories of disease, neurological examinations, Mini Mental State Examinations (MMSE), Montreal Cognitive Assessments (MoCA), Activities of Daily Living (ADL), psychometric evaluations, physical and clinical examinations, and laboratory tests.
Participants
Participants, aged 35–93 years (n = 1,805), were recruited and evaluated from the general population residing in four Beijing districts (Xi Cheng, Fang Shan, Tong Zhou, and Yan Qing) from August 2014 to December 2015. The study encompassed 16 administrative districts in Beijing: 14 urban and 2 rural. The definitions of urban and rural areas were adopted from government administrative data that categorized settings according to their levels of urbanization and economic development. To ensure adequate representation of the population, the survey populations were selected using a 4-stage stratified random procedure, details of the process were previously described [21, 22]. Exclusion criteria were participants with cognitive impairment (mild cognitive impairment (MCI), AD, vascular dementia, or other types of dementia). A consensus expert panel of 2 neurologists (Fang Li and Jing-Hong Ma) reviewed all of the data collected and determined diagnoses. All participants were informed of the purpose of the study at the time of recruitment and signed an informed consent form to participate in the survey. The study was conducted in accordance with relevant clinical research regulations and was approved by the Ethics Committee of Xuanwu Hospital, Capital Medical University.
Questionnaire
All of the enrolled participants were asked to complete a questionnaire conducted by well-trained medical students using standardized methods. The questionnaire covered a wide range of topics, including demographic characteristics (gender, age, education level, employment status, and current residence), and history of hypertension, stroke, diabetes, dyslipidemia, renal insufficiency, cancer, chronic lung disease, chronic liver disease, and the use of medication. Depression symptoms were assessed using the Geriatric Depression Scale (GDS) [23].
Physical examination and laboratory measurements
Physical examination
Before the examination, each participant was asked to rest for at least 20 min. Sitting blood pressure (BP) was measured twice on the right arm at 2- to 5-min intervals, and the mean of the two measurements was calculated for analysis. Blood pressure was measured using a standard mercury sphygmomanometer. Height was measured without shoes using a standard right-angle device and a fixed measurement tape (to the nearest 0.5 cm). Body weight without heavy clothing was measured using a weight measurement device (V-body HBF-371, Kyoto, Japan).
Blood samples laboratory measurement
All blood samples were obtained from participants in the morning following an overnight fast, centrifuged to serum, stored in a refrigerator at 2°C to 8°C, and transferred to a central laboratory (IPE Center for Clinical Laboratory, Beijing, China), which performed all analyses within 24 h. Total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and fasting blood glucose (FBG) levels were determined by a Hitachi 7600 automatic analyzer (Hitachi High-Technologies Corporation, Tokyo, Japan). Serum creatinine level was measured by enzymatic assay, which was calibrated to the isotope dilution mass spectrometry-traceable creatinine assays.
Urine AD7c-NTP laboratory measurement
The midstream urine samples were collected in an EP tube with boric acid (2 g/L) as a preservative, refrigerated immediately, and maintained at 4°C. An enzyme-linked immunosorbent assay (ELISA) kit (Anqun Biological Technology Co. Ltd., Shenzhen, China) was used to detect the level of urinary AD7c-NTP. The method used for detection reflected standard procedures for ELISA kits [13]. According to the introduction, 100μl of standard or urine specimen was added to the AD7c-NTP antibody pre-coated plate and incubated at 37°C for 1 h. Following five consecutive wash steps with PBS, 100μl of biotinylated rabbit anti-AD7c-NTP antibody was added and incubated at 37°C for another 1 h. Next, 100μl of horseradish peroxidase labeled avidin was added after five times of washing with PBS and incubated at 37°C for 30 min. Finally, 50μl of chromogenic reagent A and B was added in turn after five times of washing with PBS, and then incubated at 37°C for 15 min. The reaction was stopped by adding 50μl of sulfuric acid as stop buffer. The OD value of each sample was measured at 450 nm with a microplate reader (Multiskan Spectrum, Thermo Fisher Scientific, Waltham, MA, USA). The AD7c-NTP concentration in a urine specimen was positively correlated with the absorbance value and calculated according to the standard curve of recombinant human AD7c-NTP peptides with measured taken simultaneously.
Definitions
Classification of population demographic characteristics
The 1,805 participants were divided into four groups according to age (Table 1); less than 60 years of age, 60–69 years of age, 70–79 years of age, and 80–89 years of age, respectively. Education levels were categorized as follows: less than a high school diploma (<high school), high school diploma, and college or higher (>college). Employment status were categorized as employed, retired and unemployed. Current residence was classified as either urban or rural. Body mass index (BMI) was calculated as body weight in kilograms divided by the square of height in meters and divided into categories of underweight (BMI <18.5), normal weight (18.5 ≤ BMI <23.9), overweight (24.0 ≤ BMI <27.9), and obese (BMI ≥ 28) as defined by the National Health and Family Planning Commission for Chinese adult weight standards.
Baseline characteristics of study participants
Notes: “+” represents the disease; for depression symptoms, “+” represents severe depression, “– /+” represents mild depression; “#” represents that the health history with regard to these diseases were only obtained from participants (n = 1,141) over 65 years old; age is expressed as a mean±standard deviation.
Definitions of the diseases
Hypertension was defined following the Joint National Committee guideline VII36 to include participants with systolic blood pressure ≥140 mm Hg or/and diastolic blood pressure ≥90 mm Hg or who had a history of hypertension or had taken antihypertension medication [24]. The diagnosis of diabetes was based on the American Diabetes Association criteria for people with high FBG (≥7.0 mmol/L [126 mg/dL]), a history of diabetes, or who had taken hypoglycemic medication [25]. Participants who had high TC (serum level of TC ≥6.21 mmol/L [240 mg/dL]), high TG (serum level of TG ≥2.26 mmol/L [200 mg/dL]), high LDL-C (serum level ≥4.14 mmol/L [160 mg/dL]), low HDL-C (serum level <1.03 mmol/L [40 mg/dL]) or had taken lipid-lowering medication were diagnosed with dyslipidemia according to the Adult Treatment Panel III guidelines [26]. Renal function was assessed using the estimated glomerular filtration rate, which was calculated by the Modification of Diet in Renal Disease formula as follows: 186×(serum creatinine–1.154)×(age–0.203)×(0.742, if female), with the serum creatinine concentration expressed in milligram per deciliter (mg/dL) [27]. Stroke, cancer, chronic lung disease and chronic liver disease were self-reported and the disease history was verified with medical or hospital records. Depression symptoms were evaluated using the 30-item GDS Scale [23]. Scores ranged from 0 to 30. Scores of ten or lower were identified as normal, 11 to 20 as mild depression, and 21 to 30 as severe depression.
Statistical analysis
Analysis of the data was performed using the Statistical Package for the Social Sciences version 20.0 software (SPSS Inc., Chicago, IL, USA). Data are expressed as mean±standard deviation (SD). The urine level of AD7c-NTP between two groups were compared by two independent sample t-test and three groups or more were analyzed with one-way ANOVA followed by a LSD’s post hoc test. Multivariate analysis of variance was used for confounders analysis. A p value of <0.05 was considered statistically significant.
RESULTS
Baseline characteristics of study participants
The 1,805 participants had an average age of 65.7±10.1 years and 41.9% (n = 756) were male. The participants’ baseline characteristics and prevalence of disease are shown in Table 1. The history of cancer, chronic lung disease, chronic liver disease, and depression symptoms were obtained from participants over 65 years of age. Those participants (n = 1,141) completed an additional questionnaire relevant to the community management of chronic disease in the presence of geriatric syndrome. All questions and examinations yielded a response rate of 93.3% to 100%.
Urine AD7c-NTP levels by gender
As shown in Table 2, compared to males, the urine AD7c-NTP level in female subjects was significantly higher (0.3790±0.4873 and 0.2739±0.3815 ng/ml, respectively (p < 0.05)).
Urine Alzheimer-associated neuronal thread protein (AD7c-NTP) levels according to demographic characteristics and some non-neurological diseases
Notes: p (a) represents the value of one-way ANOVA; p (b) represents the value of multivariate analysis; Data are expressed as mean±SD.
Urine AD7c-NTP levels by age
According to one-way ANOVA, the greatest differences (p = 0.002) of urine AD7c-NTP levels among the four age groups were between the groups <60 years of age and 80–89 years old. The urine AD7c-NTP levels in groups <60, 60–69, 70–79, and 80–89 years old appear in Table 2. The urine AD7c-NTP level in group <60 years old was significantly lower (p = 0.046, p = 0.084, p = 0.000) and the group 80–89 was significantly higher (p = 0.000, p = 0.005, p = 0.004) than other groups. There was no significant differences of urine AD7c-NTP levels between the group 60–69 and the group 70–79 (p = 0.839). Additionally, the multivariate analysis of variance between different age groups showed no differences (p > 0.05).
Urine AD7c-NTP levels by some other demographic characteristics
The urine AD7c-NTP levels among participants with different education levels, employment statuses, BMI levels, current place of residence all showed no significant differences (p > 0.05, Table 2).
The association between urine AD7c-NTP level and nine common diseases
Urine AD7c-NTP levels did not show any differences (p > 0.05, Table 2) in people with the depression symptoms or any of the following diseases: hypertension, stroke, diabetes, dyslipidemia, renal insufficiency, cancer, chronic lung disease, and chronic liver disease.
DISCUSSION
In this population-based cross-sectional study, we measured the concentrations of AD7c-NTP in 1,805 human urine samples and obtained demographic data and comorbidity information from participants. Our results demonstrated that urine AD7c-NTP had a tendency to increase with age to some extent, and females exhibited higher levels than males. However, urine AD7c-NTP levels were not affected by other demographic factors such as education levels, employment status, BMI, or current place of residence. Moreover, there was no association between AD7c-NTP levels and non-neurological diseases, such as hypertension, stroke, diabetes, dyslipidemia, renal insufficiency, cancer, chronic lung disease, chronic liver disease, and depression symptoms. This study represents the first one to examine urine AD7c-NTP levels together with possible confounding factors in a large sample of the elderly. The results provide a compelling case for the use of urinary AD7c-NTP as a biomarker for AD.
The key neuropathological hallmarks of the AD brain are diffuse and neuritic extracellular amyloid plaques— often surrounded by dystrophic neurites— and intracellular neurofibrillary tangles [28]. The expression of AD7c-NTP and related genes are modulated with neuritic sprouting; an overexpression of AD7c-NTP in neuronal cells causes neuritic growth and cell death [6, 9]. In AD patients, the elevated levels of AD7c-NTP in the CSF and urine may reflect the neurodegenerative processes. The correlation between AD7c-NTP levels and the severity of the dementia makes it a potential biomarker for AD diagnosis [8, 15–18]. The urine AD7c-NTP ELISA test is recognized as sensitive, economical, and non-invasive. Moreover, urine does not form part of the body’s homeostatic mechanisms, yet reflects changes such as pregnancy, daily rhythms, and kidney diseases [29]. Because the brain and urine seem so anatomically distant and distinct, a direct relationship between the two has proven difficult to establish [30]. Additionally, physiological variations in urine have not been studied extensively [29]. Moreover, very little is known about confounding factors of AD7c-NTP, as very few studies with large samples have been conducted.
The findings indicated that AD7c-NTP levels did not increase with age among participants between the ages of 60 and 79. However, in a previous study, we have reported that AD7c-NTP levels did increase with age in a healthy Chinese population [31]. The discrepancy could be explained by the fact that the number of samples in the previous study was small (n = 294) and treated all subjects >60 years old together in one group. For the population as a whole, the incidence of AD/MCI increases exponentially with age, with the most pronounced increase occurring during the seventh and eighth decades of life [28, 32]. This may be consistent with the age-relatedness of urine AD7c-NTP levels. However, multivariate analysis of variance suggested that urinary AD7c-NTP levels are not related to age, so further study needs to be done. Female urine AD7c-NTP levels were higher than those of males, consistent with findings from the earlier study [31]. The higher AD7c-NTP levels in females also prove consistent with the higher incidence of AD among females [33]. This result suggests the need to establish different AD7c-NTP cutoff values for males and females.
Some epidemiological studies have suggested that low education is a risk factor for AD. A Chinese population-based cross-sectional survey also reported that the higher incidence of dementia and AD in rural areas compared to urban ones might be due to differences in educational levels [34]. However, other studies have demonstrated that more highly educated people may have a greater cognitive reserve that possibly delays the clinical manifestation of dementia [35]. Our results demonstrated that urinary AD7c-NTP concentrations were not related to educational attainment, place of residence, environment, or employment status. The comparison of urinary AD7c-NTP levels between different BMI groups also failed to show any differences. This finding counters an understanding that an association exists between BMI and dementia/AD. Whereas some epidemiological studies have shown that people with high BMI in midlife demonstrated an increased risk of dementia/AD in old age, no clear relationship between obesity in old age and AD has been proven [36–38].
It is noteworthy that urinary AD7c-NTP was associated with age and gender, but not with education levels, place of residence, and BMI. These findings support an understanding that urinary AD7c-NTP represents a reliable and feasible biomarker for AD. Additionally, AD7c-NTP in human urine also could be affected by other factors, such as some diseases common among the elderly. For biomarker studies, the most important purpose is to identify a specific and stable biomarker for a particular disease. The expression of neuronal thread protein in the brains of people with AD has proven to be distinct from those with other neurodegenerative diseases (Down’s syndrome, Parkinson’s disease, Parkinson’s disease dementia, Huntington’s disease, multi-infract dementia, and schizophrenia) [8]. The concentration of urine AD7c-NTP also has been proven to be higher than an MCI group, a non-AD dementia control group, and a non-dementia group [15–17, 39].
Nevertheless, it remains unclear whether or not the level of AD7c-NTP in urine could be affected by other diseases. AD7c-NTP shows up in urine from blood by filtration and the kidneys/urinary tracts by secretion. Even though the brain and urine seem to be completely separate, we cannot rule out the possibility that changes present in the brain could somehow be reflected in urine [30]. Therefore, it would be necessary to co-analyze urine AD7c-NTP with other diseases, especially the risk factors of AD with large-scale population data. Previous studies have shown that depression symptoms and all of the diseases included in this study were associated with the incidence of AD [28, 40–45]. However, whether those diseases in other parts of the body could influence the vitro excretion or detection of urinary AD7c-NTP remained unclear.
Our results suggested that the urinary AD7c-NTP levels were no different between subjects who have or do not have symptoms of depression or non-neurological diseases, such as hypertension, stroke, diabetes, dyslipidemia, renal insufficiency, cancer, chronic lung disease, and chronic liver disease. These results demonstrated that AD7c-NTP was relatively stable in the body and not affected by confounding factors.
An overview of the previous research conducted on AD7c-NTP is shown in Fig. 1. The sample type selection, detection technology, and clinical verification have been confirmed by several laboratories. This study improved upon existing work on AD7c-NTP through the information obtained from a large-scale population since the metabolic process of AD7c-NTP in humans has been unclear. The search for brain disease biomarkers in urine poses challenges that derive from the possibility that a variety of factors could temporarily affect urine. Additionally, the pathological changes of human AD cannot be completely replicated in experimental animals, which limits the possibilities for research on the mechanism of AD7C-NTP and AD development. Therefore, large-scale population data research represents the most compelling approach to be able to achieve an objective understanding of AD7c-NTP. Our laboratory has been devoted to the development of the urinary AD7c-NTP diagnostic kit in recent years and it has been developed for the diagnosis of AD. The detection linear range was 0–10 ng/ml and the normal reference value was ≤1.5 ng/ml. The sensitivity was 89.3% and specificity was 84.7% [13]. In this study, we demonstrated that AD7c-NTP levels were higher for the population over the age of 60 and for females. Therefore, greater attention could be devoted to the identification of different diagnostic thresholds based on age and gender. The urine AD7c-NTP levels exhibited no association with non-neurological diseases. Therefore AD7c-NTP proved to represent a biomarker with good specificity; other diseases did not interfere with the suspected presence of AD. These findings suggest the merits of a test like the AD7c-NTP ELISA kit for use in clinical practice.
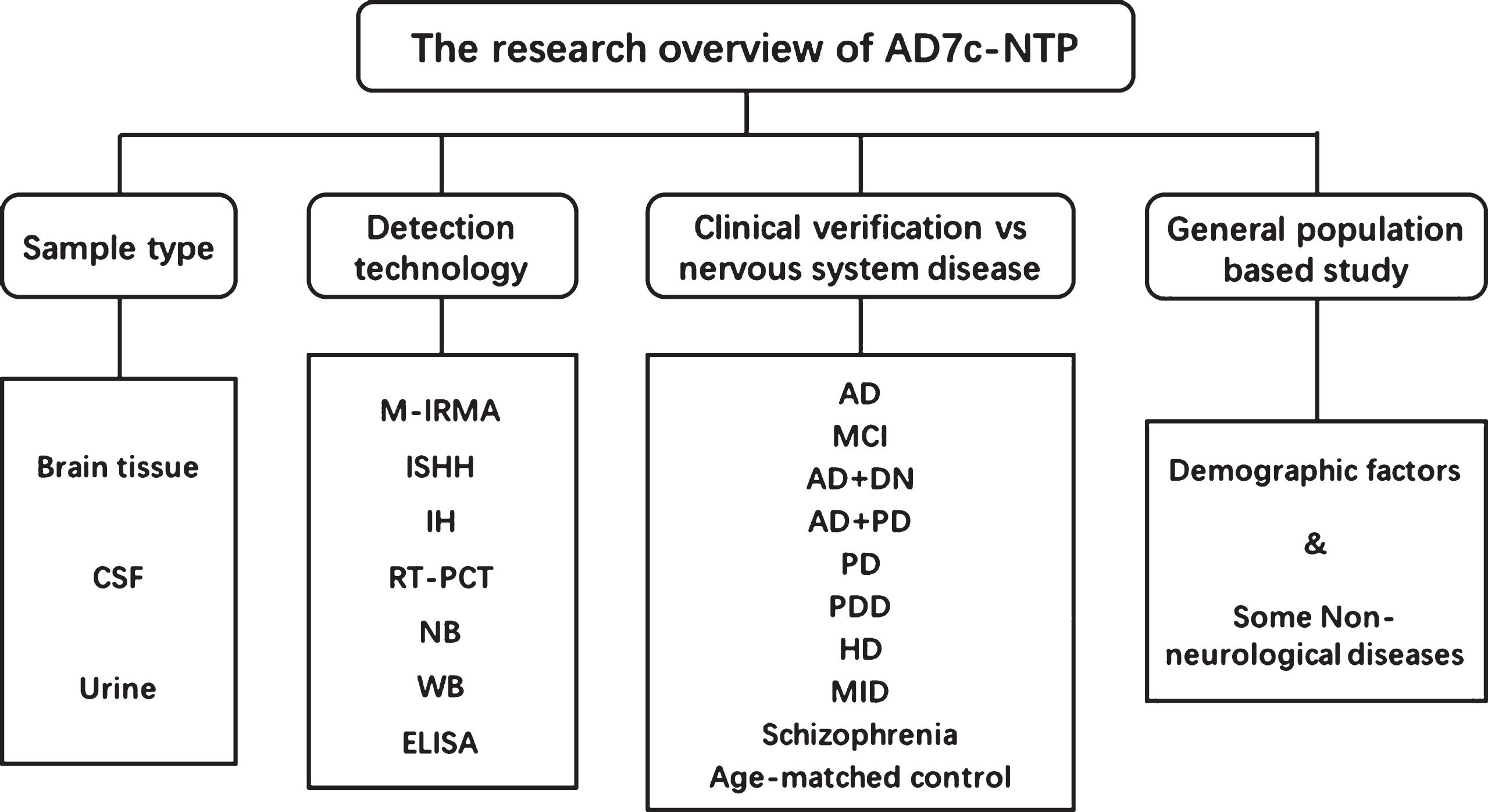
Research related to AD7c-NTP. CSF, cerebrospinal fluid; M-IRMA, immunoradiometric assay; ISHH, in situ hybridization histochemistry; IH, immunohistochemical; RT-PCR, reverse transcriptase; NB, Northern blot; WB, Western blot; ELISA, enzyme-linked immunosorbent assay; DN, Down’s syndrome; PD, Parkinson’s disease; PDD, PD dementia; HD, Huntington’s disease; MID, Multi-infarct dementia.
Further research could build upon this work through the inclusion of factors that potentially impact AD7c-NTP levels that have not been examined here, such as drinking, smoking, coffee consumption, heart disease, and/or orthopedic diseases. And for a biomarker research, the coefficient of variation in this study was in a relative high level; future research would also be needed to track and analyze this issue.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the funding from the National Key R&D Program of China (grant no.2016YFC1306300) and the Capital Health Research and Development of Special (grant no.2014-1-1031). The authors wish to thank the participants who took part in the study, and acknowledge State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Disease, Peking Union Medical College and Chinese Academy of Medical Science: Drs. Zengwu Wang; Ming Guo; Ying Li.