
Abstract
Alzheimer’s disease (AD) is often associated with feeding difficulties and changes in eating behavior with may lead to malnutrition. In French nursing homes, AD patients may live in special care units that better meet dementia residents’ needs. However, meals are often delivered to AD patients by using meal trays coming from central kitchens. This led to the disappearance of cues that could help residents to foresee mealtime, such as the smell of food odors. The aim of the present study was to assess the impact of odorizing the dining room of AD Units with a meat odor before lunch on subsequent food intake and eating behavior. Thirty-two residents (>75 years old) from three AD Units were included in the study. They participated in two control lunches and two primed lunches, for which a meat odor was diffused in the dining room 15 minutes before the arrival of the meal tray (olfactory priming). Results of the first replication showed a significant effect of olfactory priming, with a 25% increase in meat and vegetable consumption compared to the control condition. Behavioral measurements also showed a significant increase of resident’s interest toward the meal in the primed lunch. However, this effect was no longer observed when the priming session was replicated two weeks later with the same priming odor and the same menu. Although further research is needed to understand why this priming effect cannot be replicated, our experiment is one of the very first to investigate the effect of food odor priming on subsequent food intake in AD patients in a real-life setting.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is often associated with feeding difficulties and changes in eating behavior with may cause a decrease in food intake [1–5]. Ikeda et al. [3] observed that 58% of AD patients showed at least one symptom among the following: swallowing difficulty (e.g., coughs or chokes when swallowing, takes a long time to swallow food or liquids), change in appetite (e.g., loss or increase of appetite), change in food preference (e.g., prefers sweet foods more than before), disorders of oral behavior (e.g., tends to overfill mouth, eats non-edible foodstuffs), feeding difficulties (e.g., eats with hands, takes a long time to eat). Distraction from eating, frequent table-leaving events, and refusal to eat because of inability to recognize an object as food were other eating disorders frequently reported in AD patients living in long-term care facilities [6–8]. Finally, AD is often associated with polymedication which may contribute to decrease appetite (iatrogenic anorexia) [9, 10]. As a result, it is estimated that 30–40% of AD patients are malnourished [11, 12]. Malnutrition corresponds to a deficiency in nutritional intake, in terms of calories and/or nutrients and micronutrients. The many consequences include muscle wasting and impaired immune defenses. An elderly person with malnutrition is at risk of entering a vicious spiral: without prevention and without care, malnutrition leads to decreased mobility, an increased risk of falls or fractures, and an increased vulnerability to systemic infections, which in turn contribute to loss of appetite and exacerbated malnutrition [13–15]. For AD patients, malnutrition increases the burden of cognitive and functional decline and worsen the patient’s quality of life [11, 17].
It has been previously demonstrated that exposing healthy adults to food odors may 1) increase appetite [18, 19], 2) influence food choice [20–22], and 3) increase food intake [23, 24]. Regarding appetite, Ramaekers et al. [18] observed that exposure to food odors for 20 minutes increased appetite while exposure to non-food odors decreased appetite. Similarly, Zoon et al. [19] found that exposure to an odor signaling a specific taste (e.g., a beef odor) increase appetite for taste-congruent food (e.g., beef croquette, cheese cubes, and crisps). Regarding food choice, recent studies demonstrated that a non-attentively perceived pear odors increased the proportion of choices of a fruity dessert (e.g., apple sauce) in adults, whereas a chocolate-croissant odor increased the proportion of choices of a fatty-sweet dessert (e.g., a waffle) [20, 22]. Regarding food intake, Fedoroff et al. [23] observed that food intake for pizza increase after exposure to the smell of pizza. However, all these studies were completed with middle-aged adult participants. To the best of knowledge, the impact of food odor on appetite and food intake in the elderly population, including elderly people with cognitive impairment, has not been yet studied.
In French nursing homes, AD patients may live in special care units (‘Unités de Vie Protégées’) that better meet dementia residents’ needs, offering them a safe space adapted to their disabilities and preserved capacities. However, meals are seldom prepared within these units but rather delivered to AD patients by using meal trays coming from ‘central kitchens’. This led to the disappearance of cues that could help residents to foresee mealtime, such as the sight of foods, the presence of a cooker or the smell of food odor. In fact, special care units are often overwhelmed by a disinfectant smell, even in the minutes before meals. In such a context, the present study aimed at assessing the impact of a food olfactory cue before lunch on subsequent eating behavior. AD can affect some forms of memory while leaving others relatively intact. One form of memory, explicit memory, is the ability to consciously and directly recall or recognize recently processed information. This type of memory is highly impaired in AD patients [25]. On the contrary, implicit memory recalls past experiences without thinking about them (unconscious recollection), which can affect thoughts and behaviors. Implicit memory is involved with the unconscious recognition of an object (i.e., priming) and the correct completion of the steps in a task (i.e., procedural memory). This kind of memory is assessed indirectly by measuring facilitation in performance (i.e., decreased processing time or increased accuracy) due to previous exposure to identical or related information. It has been consistently shown that procedural memory remains relatively preserved throughout the course of AD [26–28]. In other words, although AD patients have severe failures to consciously retrieve information from the past, these patients are usually able to access previous experiences through non-conscious memory processes.
The aim of the present experiment was to assess the impact of odorizing the dining room of Alzheimer Units with a meat odor before lunch on subsequent food intake and eating behavior of the residents. We hypothesized that a non-attentional perceived food odor may trigger food-related mental representations, which in turn may stimulate appetite, willingness to eat, and food intake through implicit processes (priming effect).
MATERIAL AND METHOD
AD patients (either diagnosed AD or displaying AD symptoms) living in a special care unit participated in a ‘control’ lunch and a ‘primed’ lunch, for which a meat odor was diffused in the dining room 15 minutes before the arrival of the meal tray (olfactory priming). Two measures were carried out for each participant: food intake measurement and behavioral assessment (e.g., willingness to eat, staying sitting at table). This procedure was replicated: participants completed a second control and primed lunch.
Participants
Three special care units (A, B, C) took part in our study. Altogether, 32 AD patients were recruited, 17 in establishment A, 9 in establishment B, and 6 in establishment C (7 men and 25 women; mean age: 86.8 years; age range: 75 to 98 years). Residents on a prescribed diet were not included, neither were residents with psychiatric disorders and those with an acute episode of disease at the time of the study. All the participants scored below 20 on the Mini-Mental State Examination (MMSE mean = 7.7; range: 0 to 18) [29]. Four participants were at risk of malnutrition (35 > albumin≥40 g/l) and 28 were malnourished (albumin≤35 g/l). In accordance with current legislation, the protocol of the study was submitted to and approved by the ethics committee Comité de Protection des Personnes Est I (ANSM #2012-A01431-42). Residents were explained the study in simple terms, fitting with their level of understanding. If the elderly person did not manifest a refusal to participate in the study, the study was explained to his/her tutor who countersigned the consent form.
Food products
A menu composed of a starter (grated carrots), a main course (roast pork and green beans), a dairy product (cottage cheese), and a dessert (apple purée) was chosen by the dietician of the establishments to be neither disliked nor well-liked by the residents. The menu was strictly the same in the four lunches. Residents with dysphagia (n = 7) were served with texture modified foods (grated carrots and pork were mixed to a pureed consistency; green beans were replaced by mashed potatoes).
Olfactory priming
The aroma “sauté de boeuf” (Scentys Fragrance©) was encapsulated and diffused in the dining room of the special care units using a large scent diffuser (Scentys4 #PSIA-J-000018 v.1.00, Scentys Fragrance©) and two small diffusers (Scentys Pocket, Scentys Fragrance©). An odorization procedure was designed in order to: 1) obtain a homogeneous distribution of the odorant in the dining rooms; 2) obtain an intensity of the odor relatively stable during the priming phase; 3) obtain an odor intensity so that young adults would clearly notice the odor. The procedure adopted consisted in distributing in the room 90-s puffs every 30-s for the large diffuser and 30-s puffs every 30-s for the small diffusers. Odorization started 15 min before the lunch (11h45) and ended just before serving the main course (around 12h15). Diffusers were also turned on in the control condition with blank capsule to have the same background noise throughout all the lunches (diffusers make a slight purr).
Procedure
The residents took part in four lunches—two control and two primed lunches—at a rhythm of one lunch every two weeks. These meals took place at the same time, in the same room, using the same crockery and were served by the same service staff as the usual meals served in the establishments. Before the lunches, participants were free to come to the dining room and sit at their table when they want until 11:55. At this time, the service staff fetched residents who had not yet arrived. Lunches always started at noon. For the first helping, portion weights fitted to the weights recommended by the GEMRCN (2007) for meals served in French elderly institutions: 100 g for the grated carrots, 100 g for the meat, 150 g for the vegetables, 100 g for the cottage cheese, and 100 g for the apple purée. A second helping was systematically proposed to participants who finished their plate (the weight of the second helping corresponded to one half of the weight of the first helping). Control and primed lunches were alternate; establishment A started with a control lunch; establishments B and C started with a primed lunch.
Outcome measurements
Food intake
Food intake was measured by weighing the plates before and after consumption (SOEHNLE scales, precision: ±1 g). This was done for each participant and for each meal course.
Behavior
Six staff members of the hosting establishments rated participants’ behavior during lunch by using an evaluation grid (Fig. 1). In order to design this grid, a lunch (different from the lunches of the present study) was videotaped in a special care unit. Movies were analyzed by three experimenters (co-authors CSR, MG, SC) to design the scales. A training session gathering experimenters and staff members ensured consensual interpretation of the scales and homogeneous ratings. During the study, the staff members remained unaware of the presentation order of the conditions. They wore nose-clips before entering the special care unit until the end of the lunch to ensure blind evaluation. Each staff member rated the behavior of 3 to 4 residents, the same throughout the study.
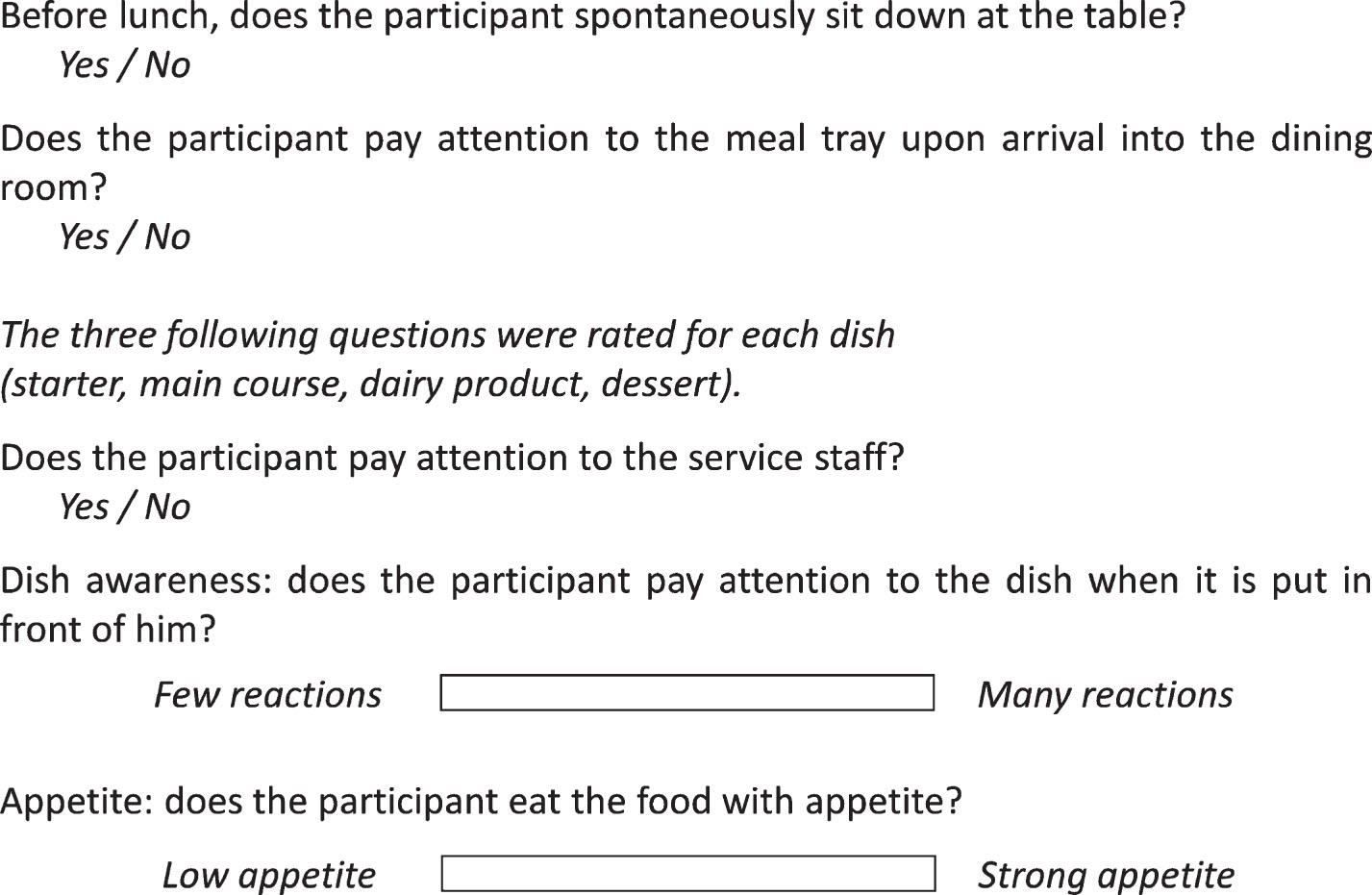
Evaluation grid to assess participants behavior during lunch.
Olfactory capacities
A non-verbal olfactory test was designed to assess participants’ olfactory capacities. Participants completed 5 trials. Each trial comprised 3 vials, with only one vial containing an odorous compound among the three. Five different odorants were used, one per trial. The presentation order of the 5 trials and the presentation order of the 3 vials within each trial were randomized across participants. Odorants were chosen to be very unpleasant (Table 1). Concentrations were adjusted to achieve rather high odor intensities, in order to ensure that above-threshold levels were reached. During the afternoon following the last lunch, face-to-face sessions were carried out between each participant and one experimenter. Experimenter wore nose-clips and was blind regarding the position of the odorous vials (vials were prepared and coded by another experimenter, who did not carry out the face-to-face sessions). For each trial, the experimenter was instructed to open the first vial, to put the vial under participant’s nose for 5 seconds while asking him to smell it, to remove the vial, and to do so for the two other vials. Afterwards, the experimenter indicated in which of the three vials he thought the participant had perceived a smell. He based his answer by considering both non-verbal reactions (e.g., facial mimics, breathing rhythm) and verbal reactions if any (e.g., onomatopoeia reflecting disgust).
Odorous compound used for the olfactory test
Data analysis
The quantities consumed were converted into caloric intake according to the CIQUAL database, which gives the nutritional composition of nearly 3,000 foods available on the French market (version from 2012; https://ciqual.anses.fr/). Scale responses (“How does the participant react when the dish is put in front of him?” and “How does the participant react when eating the food?”) were converted into scores ranging from 0 (left anchor) to 6 (right anchor).
Categorical variables (e.g., frequencies) were submitted to chi-square analysis by using the FREQ procedure of SAS software (SAS Institute INC., Cary, NC, USA). After checking for data normality, continuous variables (e.g., caloric intake, scale score) were submitted to a three-way Analysis of Variance (ANOVA), with condition, repetition, participant as factors, and the interaction condition*repetition. ANOVAs were performed using the General Linear Model (GLM) procedure of SAS software. Post-hoc analyses were computed for each significant factor using the LSMEANS option of the GLM procedure. Means (M) are associated with their standard errors computing in the LSMEANS analyses (SE). The threshold for significance was set at 5%.
Regarding the olfactory test, a score was computed for each participant by counting the number of odorous vials that were correctly found over the 5 trials (i.e., the number of correct answers). For a 1-out-of-3 test, the probability of having a correct answer at random is 1/3 and the probability of having a wrong answer at random is 2/3. When the test is replicated 5 times, the probability of observing k correct answers at random over the 5 trials is equal to P = (1/3) k × (2/3)5 - k. The probability of observing 1, 2, 3, 4, and 5 correct answers at random is respectively equal to 0.26, 0.27, 0.14, 0.037, and 0.004. Consequently, the probability of observing 4 to 5 correct answers at random is lower than 0.05 (the hypothesis H0—all the answers were given at random—could be rejected for a type I error risk of 5%). In other words, for an error risk of 5% we can conclude that participants who obtain a score equal to or higher than 4 have perceived at least one odor among the five trials.
RESULTS
Food intake
Table 2 depicts ANOVA results for the whole meal and for each dish (starter, meat, vegetable, dairy product, dessert). A significant repetition effect was observed for the starter, the meat, and the vegetable, as well as a significant condition*repetition interaction for the meat and an almost significant for vegetable. According to post-hoc analyses, participants consumed more meat and more vegetable in the primed session than in the control session during the first replication, but no significant difference was observed between the primed and the control session during the second replication (Fig. 2). No significant interaction was observed on intake for the starter, the dairy product, and the dessert (Table 2).
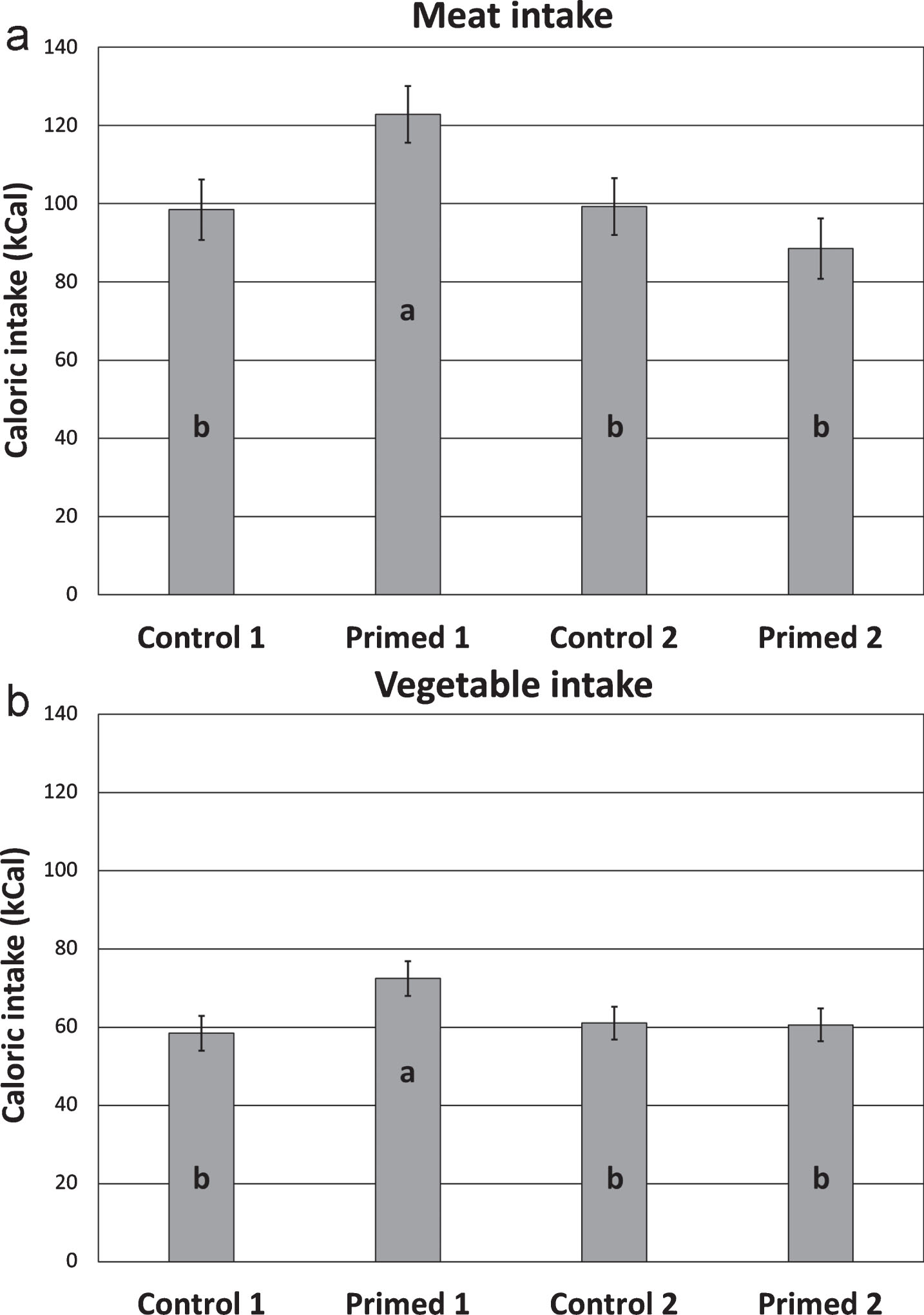
Mean caloric intake (±SE) of meat (A) and vegetable (B) for each meal. Means with different letters (a, b) stand for significant differences (p < 0.05; the p-values were obtained from post-hoc analyses). For each replication, the order of the control and primed meals were counterbalanced across the participants.
Results of the ANOVA performed on caloric intake (ns: non significant)
Eating behavior
Most of the participants sat themselves down at the table before the lunch and no significant difference was observed between the meals (control 1: 81% of the participants sat themselves; primed 1: 71%; control 2: 65%, primed 2: 85%; χ 2 = 3.46; p > 0.05). Regarding the percentage of participants paying attention to the meal tray before lunch, no significant difference was observed between the control and the primed meals during the first replication (χ 2 = 0.35; p > 0.05), neither during the second replication (χ 2 = 0.16; p > 0.05). However, more participants paid attention to the meal tray during the first primed lunch than during the two subsequent meals (primed 1 versus control 2: χ 2 = 5.38; p < 0.01; primed 1 versus primed 2: χ2 = 4.26; p < 0.05) (Fig. 3).

Percentage of participants paying attention to the meal tray for each meal. The different letters (a, b) stand for significant differences (p < 0.05; the p-values were obtained from chi-square analyses). For each replication, the order of the control and primed meals were counterbalanced across the participants.
Regarding dish awareness, a significant condition*repetition interaction was observed for the main dish (F = 5.94; p < 0.01). Participants paid more attention to the main dish during the first primed lunch (M = 3.88; SE = 0.29) than during the first control lunch (M = 2.88; SE = 0.29); no such difference was observed during the second replication. No significant effect was observed on the appetite score. Similarly, no difference was observed between the meals regarding the attention devoted by the participant to the service staff, whatever the dish.
Olfactory capacities
Figure 4 display the score distribution observed for the olfactory test. Eleven participants over 32 (34%) obtained a score equal or higher to 4 (i.e., number of correct answers≥4). When setting the threshold for significance at 5%, we can conclude that at least one answer was not given at random for these participants, in other words that they actually perceived at least one odor among the 5 trials. A significant correlation was observed between the olfactory score and the MMSE score (R2 = 0.36; p < 0.05). For the meat, the correlation between the olfactory score and the “priming” effect, namely the difference between the caloric intake of the first primed lunch versus the one of the first control lunch just failed to be significant (meat: R2 = –0.30; p = 0.10). No correlation was observed for the other dishes.
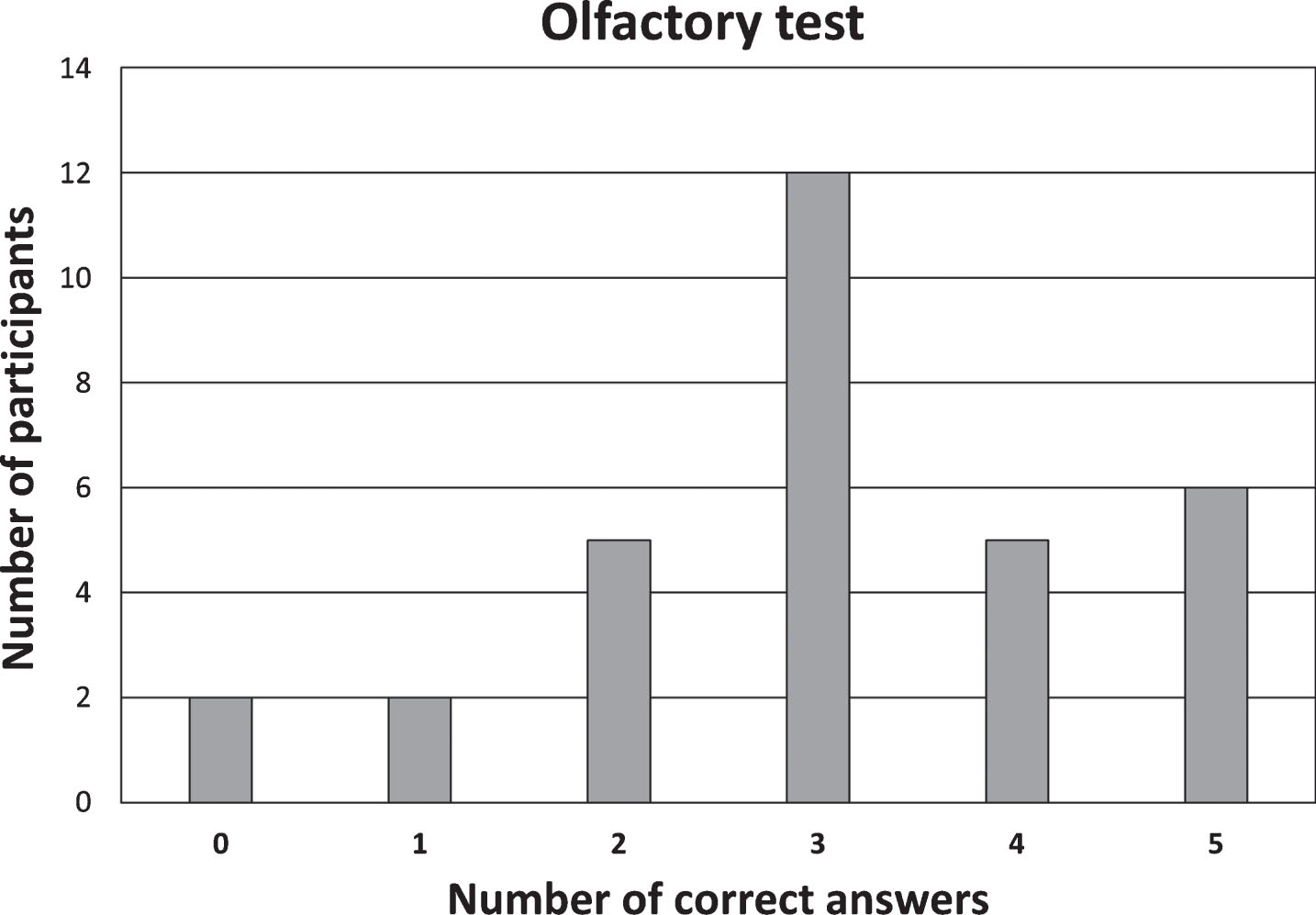
Distribution of the scores obtained at the olfactory non-verbal test.
DISCUSSION
The aim of this present study was to assess the impact of an olfactory priming in AD patients before a lunch on their subsequent food intake, in special care units (‘Unité de Vie Protégée’). A specificity of AD is that, in this pathology, explicit memory is altered whereas implicit memory is relatively preserved [30]. Our main hypothesis was that a non-attentional perceived food odor will impact the implicit memory by activating food-related mental representations, which will stimulate appetite, willingness to eat, and food intake. In fact, our results highlighted that when the “sauté de boeuf” odor was diffused, participants pay more attention to the meal and increase their intake for the main dish compared to the control condition (non-odorized). Our results are in line with those of Guéguen and Petr [31] in a younger adult population. They have found that when a lavender aroma was diffused in a restaurant, this odor seemed to relax people which stay longer in the odorized area. However, this effect was no longer observed when the priming session was replicated two weeks later with the same priming odor and the same menu. Several hypotheses were considered to explain this intriguing result.
It could be argued that the priming effect may depend on the ability of AD participants to perceive the meat odor. To get rid of this possible limit as far as possible, the odorization procedure was designed in order to obtain a quite strong odor intensity and a quite long exposure duration. Furthermore, an olfactory test was carried out afterwards to assess participants’ olfactory capacities. Odor intensity was set up by the authors of the papers to range between medium and strong intensity, according to their expertise on odorization procedure. Unfortunately, it was not possible to have a panel of healthy assessors coming into the dining room of the special care unit to assess odor intensity. The length of exposure duration (i.e., 30 minutes, between 11:45 and 12:15) was chosen because it may reflect an ecological situation—in France, it is quite common to smell cooking odor in a kitchen during the half-hour before a meal. On average, participants sat down at their table around 12:00, for both conditions (primed: 11:99; control: 11:96; F = 0.38; p > 0.05) and both repetition (first: 11:97; second: 11:98; F = 0.00; p > 0.05). However, from 11:30 to 12:00, almost all the residents were either sat down somewhere in the dining room or wandering in the large hallway that go through the dining room. Giving these conditions, it was not possible to have an exact measurement of odor exposure duration for each participant. Finally, the results of the olfactory test highlighted large inter-individual variability regarding the olfactory score, but no correlation was observed between olfactory performance and the priming effect. However, as discussed further on, the olfactory test allowed to infer that ‘a participant was able to perceive odors’ when he obtained a score of 4 or 5 for an error risk of 5%, but it did not allow to infer that ‘a participant was not able to perceive odors’ when he obtained a score lower than 4 (e.g., for participants who obtained 3 correct answers, the present test did not allow to decipher if the 3 correct answers were given at random or if the participant actually perceived an odor). As the odorization procedure was strictly the same between the two priming sessions and as it is unlikely that participants’ olfactory capacities drastically changed between the two priming sessions, it is hardly plausible that changes in these parameters may explain the inconsistency between the results of the first and second priming repetition. However, future research should definitively better control and assess these parameters. In particular, future experiments should better track the duration of odor exposure at an individual level. Furthermore, future research should also consider individual factors such as dysphagia or severe malnutrition that often goes along with a severe decline in appetite, and thus may affect this impact of a priming odor on subsequent food intake.
Köster et al. [32] recently argued that in humans, the role of implicit olfactory memory is to react immediately to unexpected odors rather than to notice well-known odors or in our everyday surroundings, olfaction being the guardian of vital functions such as breathing and food ingestion (“Misfit” Theory). Köster and Mojet [33] proposed that olfaction follows the rules “perception by exception”: odors stay in the “background” unless they are new or unexpected. In line with this theory, we can hypothesize that the perception of an unexpected meat odor activated related mental representations leading to an increase of meat intake during the first priming condition, but that the recurrence of the same odor in the same context failed to arouse olfactory memory during the second priming condition because of a habituation process. While the interval of two weeks seems to be long enough to prevent habituation, future research should consider expanding this duration and assessing the impact of various odors over several priming sessions. Finally, it should be noted that to our knowledge, no other olfactory priming experiment had used a procedure involving multiple repetitions of priming. In cognitive psychology, priming is generally a “one shot” paradigm [34–37]. Beyond the specific paradigm used in the present study, futures studies in cognitive psychology should investigate if a repeatable priming effect would be obtained or not from one session to another by considering various stimulus (and not only odor) and various population (and not only AD patients). This may lead to the development of a theoretical framework liable to account for the effect of learning and habituation effect through repeated priming events.
In the present experiment, the choice of a meat odor was done because it is often the odor of the main dish that predominates among the cooking odors in a real-life kitchen, but also because sustaining protein intake (and thus meat intake) is at key to prevent malnutrition. For young people, the selected odorant proved to be well-known and rather pleasant, but one could not rule out that this odor may have induced disgust among people who are disliking meat, and thus decrease meat consumption rather than increase it. Consequently, before providing clinical recommendations on the use of odor to promote food intake in a nursing home, future studies should carefully consider the impact of olfactory priming while taking into account individual food preference to avoid adverse effect.
Finally, the present experiment also provided interesting features regarding the ability of AD patients to perceive odors. As described in the literature, olfactory dysfunction is a widely admitted feature of AD with patients showing overt deficits in odor identification [38–40]. Smell loss can even precede cognitive symptoms by years [41, 42] and some authors have suggested the use of olfactory identification tests for screening and follow-up [43–45]. However, identifying an odor, that is to say find its name, is a reputedly difficult task (even for young people) and often requires the use of explicit memory that is known to be altered in AD [46, 47]. The use of explicit identification tests may have led to an over-estimation of the olfactory decline in AD patients. In fact, odor identification performances does not only rely on the ability of the AD patient to detect an odor, but also on the ability of the AD patient to associate an odorous sensation with a verbal label [48]. Furthermore, using an identification task assumes that the name of the odor is known by the participant, namely that it was learnt during life course, which is far from being the case [46]. Finally, odor identification tasks are hardy utilizable with aphasic or almost aphasic patients, which was the case of several of our participants. If an identification task may be an interesting tool for screening AD at an early stage of the disease, it is not a suitable test for assessing the ability of AD patients to perceive odor at an advanced stage of the disease, which was the case of all our participants.
The two advantages of the olfactory test used in the present study were that it did not request any verbal answer from the AD patients and it did not represent any cognitive cost for the AD patients. Even a very simple 1-out-of-3 detection test is based on explicit memory capacities by requiring the participant to remember the smell of the 3 vials in order to decide in which one there was an odor. However, in the present test, the AD patients were just presented the 3 vials one after the other and no explicit memory capacities was solicited. The results showed that 34% of the participants were able to perceive unpleasant odors. For the remaining participants (and in particular for the 37% participants for who 3 correct answers were observed), the present test did not allow to conclude if the correct answers were given at random or if the participant actually perceived an odor. The present test was a very first attempt to assess olfactory capacities in AD patients without requiring verbal answer or cognitive load from these patients, but it could of course be improved for future studies. Statistical power could be improved by increasing the number of trials. Reliability could be improved by videotaping the AD participants during the test and asking two independent observers to code the answers (instead of one in a face-to-face session in the present study). However, it may be difficult to standardize the expected verbal and non-verbal reactions given the large inter-individual variability observed in the present test. For instance, one participant did not say a word during the test, but he systematically “sniffed” when he was presented an odorous vial. Another participant always said “It smell good” for all the vials (blank and odorous), but frowned when he was presented an odorous vial. Some reactions were much more subtle (and even sometimes difficult to verbalize by the experimenter).
To conclude on the olfactory capacities, it can be assumed that AD is accompanied by an increase in odor threshold. In fact, in a meta-analysis conducted by Mesholam et al. [38] over 8 studies revealed significant higher odor threshold for AD patients compared to healthy control. However, AD patients may be still able to detect odors providing that their intensity is strong enough [49, 50]. In the present experiment, the use of a non-verbal olfactory test and quite intense odors showed that 34% of the AD participants perceived at least one odor among the 5 trials. Finally, the fact that an odor diffused in the dining room had a significant impact on food intake and behavior during the first priming session also suggests that AD patients remained somehow able to perceive the meat odor.
Conclusion
The present study revealed that diffusing a food odor just before a meal positively impact food intake and behavior in AD patients. However, when the experiment was replicated two weeks later in the same conditions, the effect faded away. Although further research is needed to understand why the priming effect cannot be replicated, this experiment is one of the very first to investigate the effect of food odor priming on subsequent food intake in AD patients in a real life setting.
Footnotes
ACKNOWLEDGMENTS
This study is part of AUPALESENS—Improving the pleasure of elderly people for better ageing and to fight against malnutrition—funded by the French National Research Agency (ANR-09-ALIA-011-02). This work was also supported by grants from the Regional Council of Burgundy France and the European Funding for Regional Economical Development (FEDER). The authors thank Jeanne Dufour, Amandine Layer, Sandrine Plissonneau from the nursing homes as well as the M1 students Valentin Constant and Christelle Welty, for their help during the experiment.