
Abstract
Background:
Many psychosocial and behavioral interventions have been developed for informal dementia caregivers. Because existing meta-analyses only focused on a limited number of interventions and outcomes, how effective these interventions are overall and which interventions components are associated with larger effects has yet to be explored.
Objective:
To provide a comprehensive meta-analysis of the effectiveness of psychosocial and behavioral interventions on burden, depression, anxiety, quality of life, stress, and sense of competence in informal dementia caregivers. In addition, we examined if interventions which utilized more sessions and/or were delivered personally (face-to-face) had larger effect sizes. In exploratory meta-regressions, we examined seven additional moderators.
Methods:
The protocol was registered with PROSPERO, number CRD42017062555. We systematically searched the literature to identify controlled trials assessing the effect of psychosocial and behavioral interventions on the six outcome measures, for informal dementia caregivers. We performed six random effects meta-analyses, to assess the pooled effect sizes of the interventions. In addition, we performed separate meta-regressions, for each outcome, for each moderator.
Results:
The sample consisted of 60 studies. For all outcomes except anxiety, the pooled effects were small and in favor of the intervention group. No moderator was found to systematically predict these effects. There were no indications for publication bias or selection bias based on significance.
Conclusion:
Overall, the interventions yield significant (small) effects, independent of intervention characteristics. Future research should explore options to enhance the effectiveness of interventions aimed at assisting informal caregivers.
Keywords
INTRODUCTION
Worldwide, more than 47 million people suffer from dementia, with 9.9 million new cases diagnosed every year, predominantly in Asia, Europe, and America [1]. Most patients are community-residing and cared for by at least one informal caregiver (hereafter: caregiver), typically an (unpaid) spouse, relative, or friend of the person with dementia [2].
Although caregiving is satisfying for some caregivers [3–6], it can also be very burdensome [7, 8], with depression [9] and caregiver burden [10] being the most prevalent problems. Caregivers also often experience relatively high rates of anxiety, and general distress [11], and their quality of life and sense of competence can be negatively affected by their caregiving responsibilities [12, 13].
Many psychosocial or behavioral interventions to support these caregivers have been developed. These include training and education programs, support groups, counseling, and so-called ‘multi-component interventions’ that combine two or more of the previous types (e.g., education and support). Existing meta-analyses in this area mostly limited their focus to specific subgroups of informal caregivers (e.g., only co-residing caregivers [14]); or to one specific ‘type’ of intervention, such as meditative interventions [15], service coordinating interventions [16], or educational interventions [17]. While classifying interventions may seem useful, substantial inconsistencies exist in how they have been categorized across systematic reviews [18], which in turn hinders interpretation of the findings and comparability of the results. In addition, due to focusing on only one of these categories or on one specific subgroup, the overall and relative effectiveness of these interventions remain unclear. Meta-analyses which have examined all psychosocial interventions for caregivers of people with dementia, are no longer up to date [19].
Some previous meta-analyses tried to identify intervention characteristics which contributed to larger effects; Backhouse et al. [16] found that, among four service coordinating interventions, those delivered by case managers with a nursing background showed greater positive effects on caregiver quality of life compared to those that were delivered by professionals with other backgrounds (standardized mean difference (SMD) = 0.94 versus SMD = 0.03, respectively). However, this characteristic was not associated with larger effects on the other outcomes (burden, mood, and person with dementia related outcomes). Jensen et al. [17] also employed subgroup analyses (with k = 5 educational intervention studies) and found that shorter interventions yielded larger effects on caregiver burden than longer interventions. However, the authors noticed that the same analysis also separated trials into settings in low versus high income countries with greater effects seen in low income countries, and they found no significant differences in effect sizes for individual versus group interventions. Brodaty et al. [19] examined five predictors: whether the intervention involved support/help from extended family, counseling, involvement of both the caregiver and the person with dementia, support groups, and stress management. They only found that involvement of both the person with dementia and caregiver in the intervention was associated with larger effect sizes on caregiver psychological morbidity. No significant effects were found for the other characteristics evaluated. Overall, the results have been mixed, probably due to the inclusion of small subsets of studies, and because the focus has typically been on one specific intervention type. Thus, the overall and relative effectiveness of these interventions and the intervention characteristics that predict better outcomes remain unclear. The current study aims to answer these questions.
Schulz et al. [20] developed an intervention taxonomy in an attempt to systematically describe features of psychosocial and behavioral interventions. This taxonomy focused on two broad categories: delivery characteristics and intervention content. In addition, the taxonomy considered adaptability, that is, whether or not the intervention is (or can be) tailored to the participant. Gaugler et al. [18] examined the differences in the labeling of informal dementia caregiver interventions across various systematic reviews. They found substantial inconsistencies and discovered, using a qualitative content analysis, seven themes by which dementia caregiver interventions were categorized. These themes overlapped with the intervention taxonomy by Schulz et al. [20] and included: content or type (e.g., education, psychosocial support, skill-building), delivery modality, intended audience (e.g., dyadic, individual), whether or not the intervention was standardized or tailored to the participant, the number of sessions, and the source of delivery (professional- or peer-led). Both Schulz et al. [20] and Gaugler et al. [18] argued that accurate reporting of intervention components, and using these in a meta-analysis, would lead to a better determination as to which characteristics contribute to larger effects. This knowledge could in turn be used to develop the most effective interventions for both informal dementia caregivers and the people with dementia they care for. However, no meta-analysis to date has attempted to analyze all types of psychosocial and behavioral interventions, irrespective of certain types, and tried to identify which of these intervention characteristics contribute to larger effects.
To fill this gap, we aimed to evaluate the effectiveness of interventions for informal dementia caregivers in reducing caregiver burden, depression, anxiety, and general (dis)stress, and in heightening quality of life, and sense of competence. Caregiver burden and depression were the primary outcome measures in our meta-analyses, while the other variables were secondary outcomes. We hypothesized that the interventions would show small to moderate average effect sizes, with a considerable amount of heterogeneity due to differences in the intervention characteristics, and heterogeneity across the included participants. Meta-regressions were carried out in order to identify which intervention characteristics, as proposed by Schulz et al. [20] and Gaugler et al. [18], were associated with larger intervention effects. We hypothesized that interventions which utilized more sessions and/or those which were delivered personally (face-to-face) instead of indirectly (via the internet or telephone), would show larger effects.
METHODS
This review is registered with PROSPERO (number: CRD42017062555).
Search strategy
The following databases were systematically searched: MEDLINE in PubMed, Psycarticles; Psychology and Behavioral Sciences Collection; and PsycINFO via EBSCO Host, the Cochrane Library, and EMBASE.
The search was conducted using the following keywords: Caregivers [MeSH]/Caregiver/Care givers/Care giver/Carers/Carer, Informal/Family, Dementia [MeSH]/Alzheimer/Alzheimers, Intervention/Training/Support. Terms were searched in titles and abstracts. The customized strategies for each database can be found in Supplementary Table 1. The reference lists of the selected studies and published reviews were manually scanned for supplementary relevant publications.
Eligibility criteria
For studies to be included in this review, they had to meet the following inclusion criteria:
Participants
A sample (n > 5) of adults (≥18 years) providing informal care to a relative, spouse, or friend with dementia. If a combined sample (of for instance professional and informal caregivers) was used, the study was only considered when data for informal caregivers were reported separately.
Intervention
Non-pharmacological, psychosocial, psycho-behavioral, or psychoeducational interventions for informal caregivers were included. Dyadic interventions were excluded. Dyadic studies include both the caregiver and the person with dementia, and partly depend on participation of the people with dementia. This can bias inclusion because then only the caregivers who care for the more active or willing persons with dementia are included. In addition, respite interventions, case management/nursing interventions (which are generally considered usual care), cost-effectiveness studies, usability studies, protocols, and drug trials (for either caregivers or person with dementia) were also excluded.
Intervention and control group
The design included both an intervention and an untreated control condition. Comparisons of several treatments (without an untreated control group) were not included because 1) the goal of this meta-analysis was to test whether greater improvements were found in caregivers who received treatment compared with caregivers who received no specific intervention(s); 2) if interventions were compared, there would be no theoretical reason to label one as the experimental group and the other as the control condition; and 3) comparing the change of an experimental condition to the change of a control condition who also received help, underestimates intervention effects when both interventions show desired effects. Single group pre-posttest studies were excluded because of this design’s inherent weakness in reaching valid conclusions. These studies often do not permit reasonable causal inferences, because observed changes can be due to other aspects than the intervention, including regression to the mean, maturation, and test effects [21, 22]. This weakness justifies their omission from meta-analyses [23].
Outcomes
At least one outcome measure experienced by the caregiver was included as an effectivity measure, which could be clustered into one of the following domains: burden, depression, anxiety, distress, quality of life, or sense of competence.
Other
The publication was an original empirical article published in English between 01-01-2002 and 01-27-2017. Protocols, implementation studies, letters to the editor, and comments were excluded. Reviews were excluded, but their references were hand searched for additional articles. When studies reported identical results using the same participant sample with the same intervention, we only used the most recent publication. When studies evaluated the same intervention, but with different samples, we included both (independent) studies. Experimental and quasi-experimental studies were both included in order to analyze all possible data ensuring that no valuable insights were lost by including only experimental studies. We only included quantitative (not qualitative) studies.
Study selection
Two reviewers (LJ and RM) independently screened the titles and abstracts of studies retrieved using the search strategy in order to identify studies that met our inclusion criteria. If they met the criteria, full-texts were obtained and again independently assessed (by the same two reviewers) for eligibility. Disagreements were resolved by consensus. If consensus could not be reached, a third reviewer was consulted.
Data collection process
Data regarding study design, participants and intervention characteristics, outcome measures (data from the first follow-up assessment after completion of the intervention) and moderators were extracted by one reviewer (LJ) using a self-developed, pre-piloted, data extraction form. If studies reported statistics for subscales of questionnaires which measured the same construct (for example, if multiple subscales of one questionnaires measured burden), the accompanying effect sizes were pooled [24]. If studies used multiple questionnaires measuring one outcome measure (e.g., both CES-D and HADS-D were used to measure depression), only the first described questionnaire was included in the analyses. If studies reported two or more interventions (and an untreated control condition), only the most complete was used. In case of equal relevance, we only used the first intervention.
The reviewer extracting the data completed three rounds: one initial assessment and two additional checks for inconsistencies/errors. In case of difficulties, the second and/or third reviewer was asked for his/her judgment. All problems were resolved through discussion. In case of incomplete data, we contacted the original authors. The authors were given three weeks to reply, after which two follow-up e-mails were sent. If there was still no reply, we used published data. In the case of no published data, the study was omitted. Adjusted data from Bourgeois et al. [25], Joling et al. [26], Gonzalez et al. [27], and Hepburn et al. [28] were used because unadjusted data were unavailable upon request.
Statistical analyses and data synthesis
The results of studies measuring the same outcome variables (burden, depression, anxiety, (di)stress, quality of life, sense of competence), were pooled using random-effects meta-analyses based on standardized mean differences (Hedges’ g). Burden and depression were the primary outcome measures while the others were secondary outcome measures. Effect sizes were recalculated so that higher scores indicated more burden, more depression symptoms, more anxiety symptoms, more stress, higher quality of life, and greater sense of competence. 95% Confidence Intervals were used and two-sided p-values were employed for each outcome variable. Six separate meta-analyses were conducted in total (one for each outcome variable). Heterogeneity between the studies in effect sizes was assessed using both the Q test and the I2 statistic. An I2 value greater than 50% was considered indicative of substantial heterogeneity. To check for publication bias, Sterne and Egger’s test [29] for funnel plot asymmetry was used (with alpha set at 0.10), followed up by another sensitivity test using p-uniform for sufficiently homogenous subsets of studies [30, 31].
To identify which intervention characteristics were associated with greater effects on each of the six outcome measures, we ran six mixed effects meta-regressions. The following moderators were tested in a confirmatory manner: the type of delivery (dummy coded, face-to-face/other), and the number of sessions (continuous) (against Alpha = 0.05 based on the Q test for that moderator). Both the individual contribution of the moderators and their interaction were tested in separate regression analyses. In addition, the following moderators were added in explorative analyses: intervention type (categorical variable: psycho-educational, support, psychotherapy), content (the inclusion of knowledge transfer, skill training, support, feedback, and/or cognitive counseling (all dummy coded, included/not included)), materials used (written information, assistive devices, and/or homework (all dummy coded, included/not included)), whether or not the interventions were adaptable/tailored to the participant (dummy coded, yes/no), whether or not it was a group intervention (dummy coded, yes/no), and the location where the intervention took place (dummy coded, at home/other). Ideally, for each outcome six exploratory meta-regressions were executed; one for each moderator. However, a meta-regression was only executed if there were >10 studies included in the meta-analysis to ensure statistical power.
All analyses were executed using the R package Metafor (version 2.0 [32]) using Restricted Maximum Likelihood (REML).
RESULTS
The literature searches identified 5,133 potentially relevant studies, and 9 were added by manually scanning reference lists (of existing reviews). After removing the duplicates, 3,782 studies remained, of which 3,416 were discarded after reading the title/abstract. 366 full texts were retrieved, of which 297 were excluded for a variety of reasons; 23 studies did not evaluate a psychosocial or behavioral intervention; 44 studies did not include one of the pre-specified outcomes; 59 studies did not have at least 1 intervention and 1 control group; 44 studies included no(t) (only) informal caregivers; 104 studies were not original empirical effectivity studies, but protocols or implementation studies; 9 were in another language than English; and 14 studies used only qualitative analyses. 7 papers could not be included because we did not receive the required data on request, and 1 paper was excluded due to the reporting of incoherent data. The final, included, sample consisted of 60 studies, published between 2002 and 2017. Figure 1 shows the PRISMA [33] flow diagram and Table 1 shows an overview of the included studies.
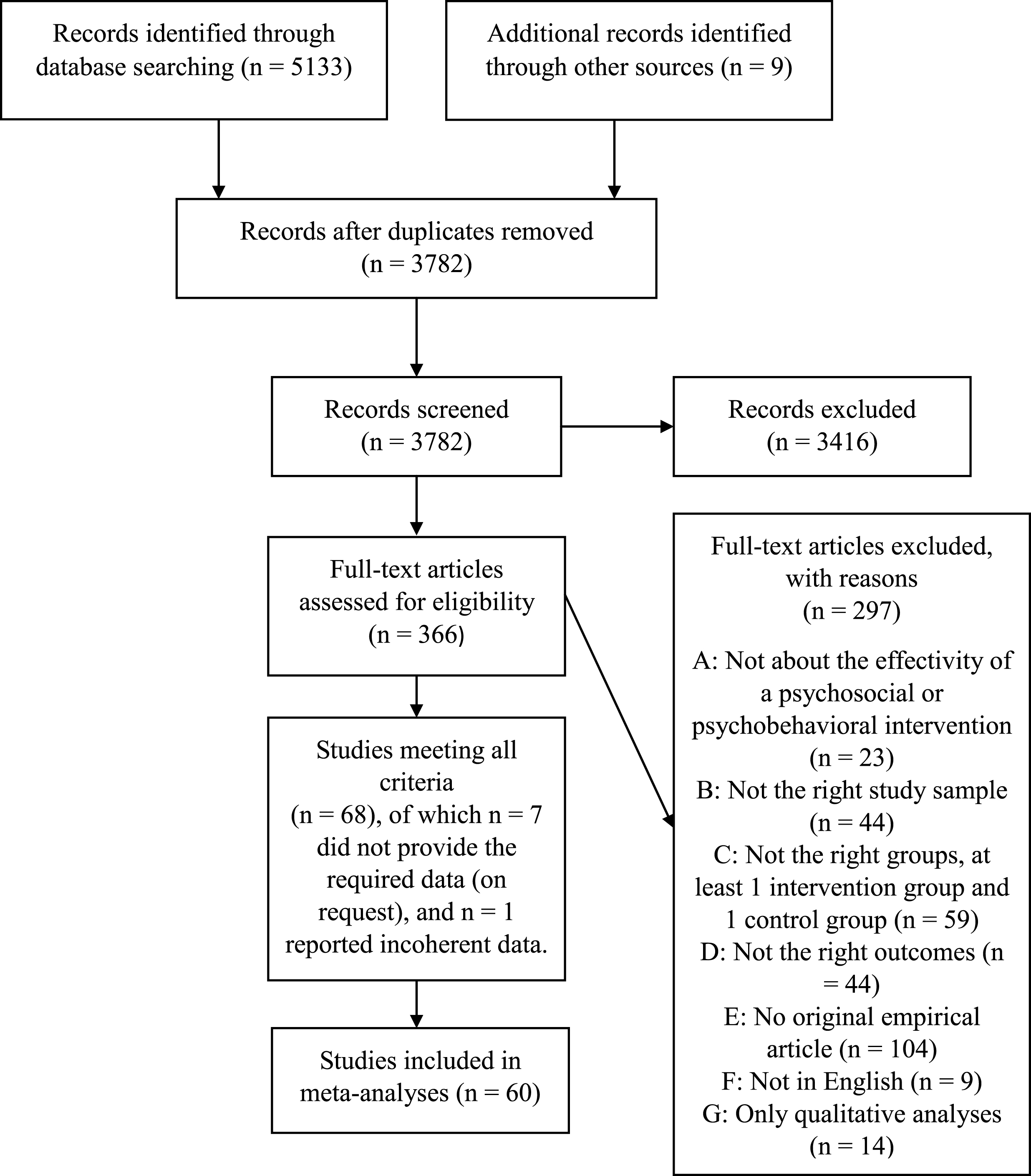
Flow diagram.
Overview of the included studies
Note. NA, not applicable; ND, not described; CSS, Caregiver Satisfaction Scale; CES-D, Center for Epidemiological Studies Depression Scale; STAI, State-Trait Anxiety Inventory; PSS, Perceived Stress Scale; CSE, Caregiver Self-efficacy Scale; RMBPC, The Revised Memory and Behavior Problems Checklist; MAACL-D, Multiple Affect Adjective Checklist – Depression; RSCSE, Revised Scale for Caregiving Self-Efficacy; CMI, Caregiver Mastery Index; ISSB-PES, Inventory of Socially Supportive Behavior – Personal Efficacy Scale; AMSS, Agitation Management Self-efficacy Scale; BAI, Beck Anxiety Inventory; NPI, Neuropsychiatric Inventory; ZBS, Zarit Burden Scale; PMS, Personal Mastery Scale; PDS, Patient Distress Scale; RSS, Relatives Stress Scale; HADS – A/D, Hospital Anxiety and Depression Scale – Anxiety/Depression; EQ-5D, Euroqol – 5 Dimensions; WHOQOL (bref), World Health Organization Quality of Life (abbreviated); CBS, Caregiver Burden Scale; ZBI, Zarit Burden Inventory; GDS, Geriatric Depression Scale; QOL-AD, Quality of life in Alzheimer’s Disease; SSCQ, Short Sense of Competence Questionnaire; GSE, General Self-efficacy scale; CBI, Caregiver Burden Inventory; PDI, Psychological Distress Inventory; SF-12 = Short-Form 12 Items; CCS, Caregiver Competence Scale; SF-36, Short Form-36 items; CRS, Caregiver Role Strain; BDI-II, Beck Depression Inventory-II; Webneuro-Depression/Anxiety, Webneuro test battery-Depression/Anxiety; AQoL-8D, Assessment of Quality of life 8-dimensions.
Meta-analyses
Primary outcome variables
Figures 2 and 3 show the forest plots containing all the effect sizes for each study and the pooled effect sizes for the outcome variables burden and depression respectively.
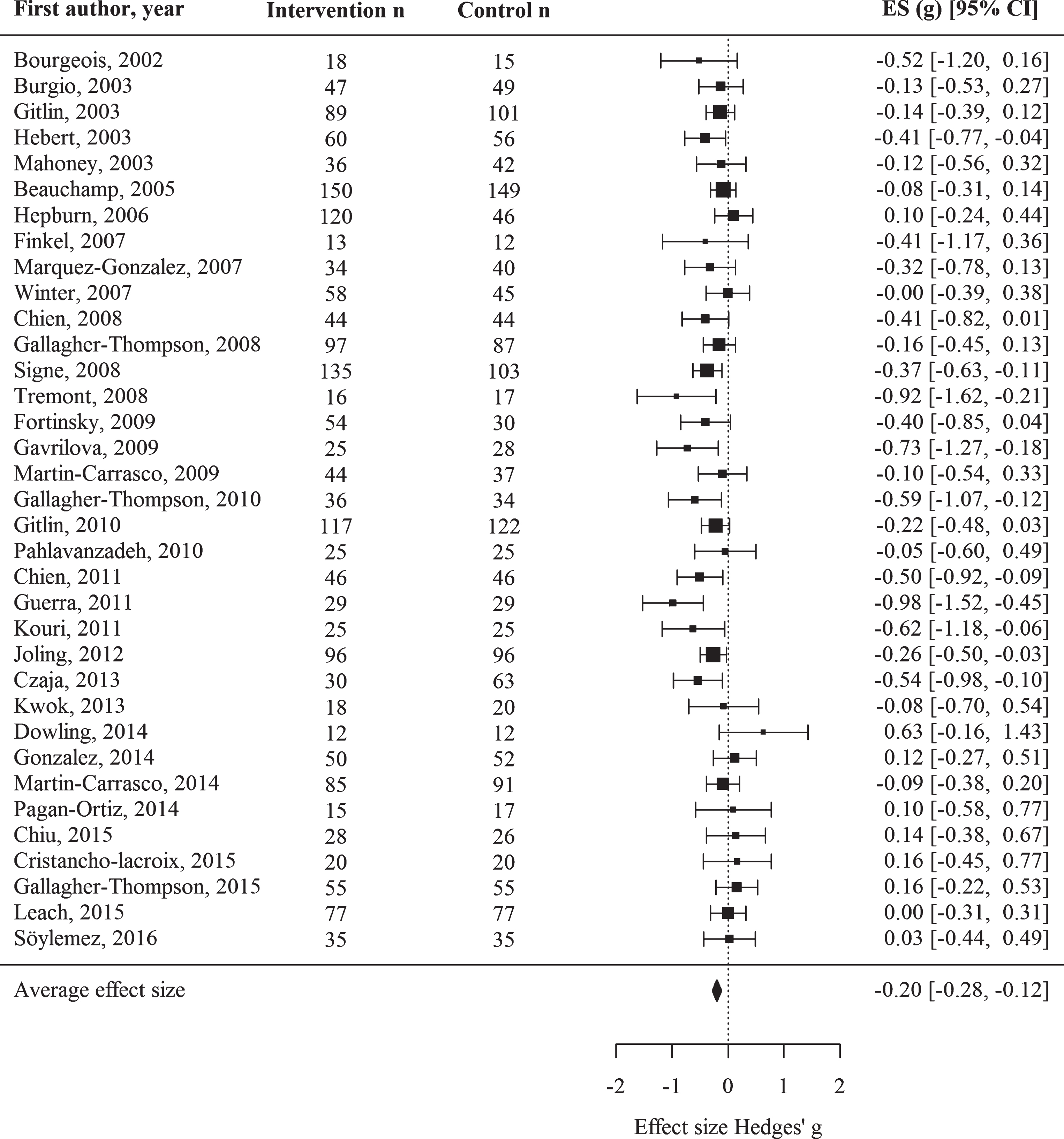
Intervention effects on caregiver burden.

Intervention effects on depression.
Caregiver burden
The random-effects analysis (k = 35, total n = 3,682) on the intervention effects on caregiver burden, yielded an estimated average effect of g = –0.20, p < 0.001, 95% CI [–0.28, –0.12]. This is a small effect size and indicates that the participants who were exposed to an intervention, scored lower on burden questionnaires than the control groups, after the intervention. There was a significant amount of heterogeneity, Q (34) = 54.49, p = 0.014, I2 = 28.62%, estimated at τ2 = 0.02, SE = 0.01), which indicates that there is variability among the underlying population of effect sizes. Sensitivity tests identified no outliers.
Depression
The random effects analysis on depression (k = 35, total n = 3773) yielded an estimated average (small) effect of g = –0.19, p < 0.001, 95% CI [–0.27, –0.10], in favor of the intervention group. There was a significant amount of heterogeneity, Q (34) = 55.19, p = 0.012, I2 = 37.54%, estimated at τ2 = 0.02, SE = 0.02.
Sensitivity tests (Q test and the I2 statistic) identified one outlier [34], with an effect size of g = –0.95. One of the differences between this study and the other studies is that Losada et al. [34] only included participants with high depressive symptomatology at baseline, whereas other studies included all participants, regardless of their baseline depressive symptoms. As such, the participants in the study by Losada et al. [34] may have had more room for growth and are more likely to show change after an intervention. Removing this outlier reduced the residual heterogeneity, Q (33) = 46.48, p = 0.060, I2 = 28.43%, estimated at τ2 = 0.02, SE = 0.01. This analysis yielded an estimated average (small) effect of g = –0.17, 95% CI [–0.25, –0.09], p < 0.001.
Secondary outcome variables
Figures 4–7 show the forest plots for the outcome variables anxiety, quality of life, stress, and sense of competence respectively.

Intervention effects on anxiety.
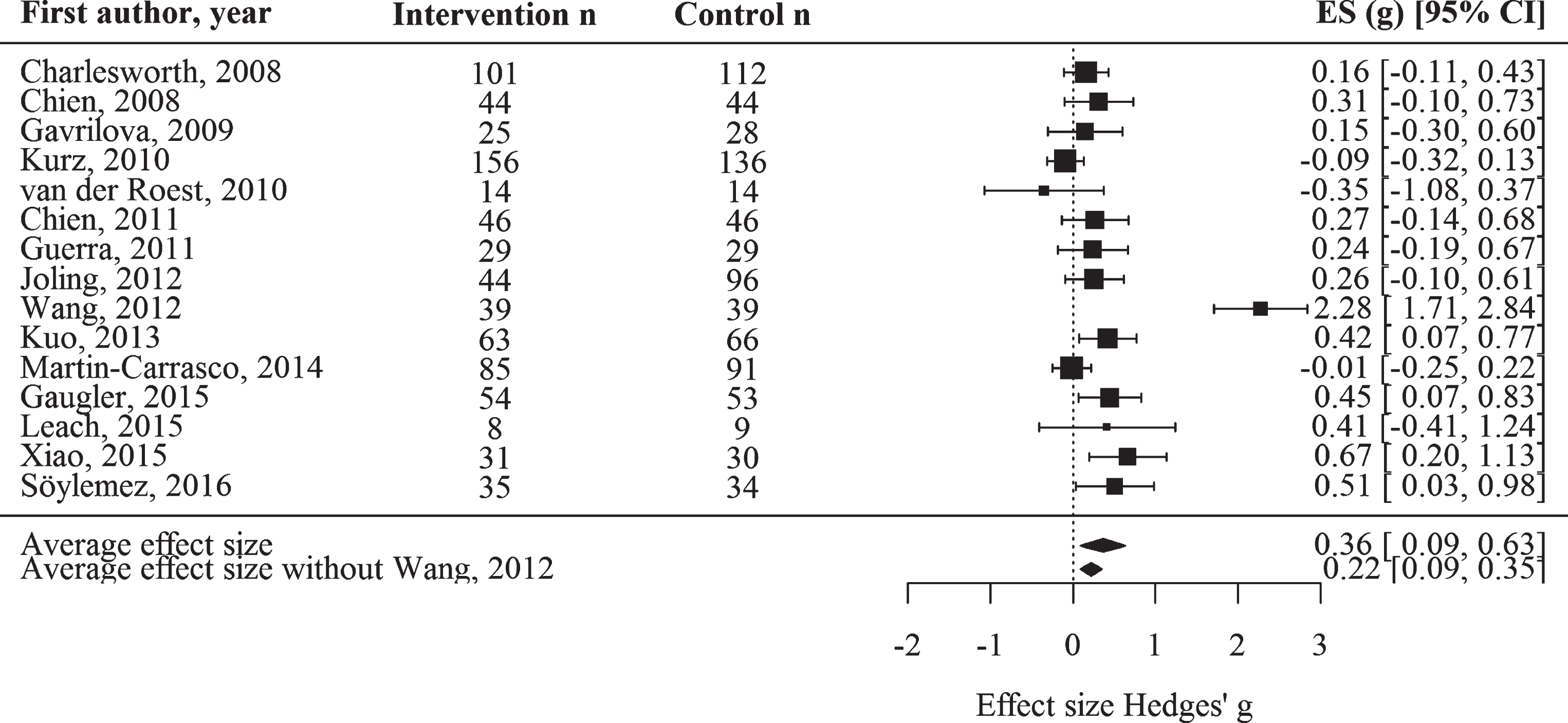
Intervention effects on quality of life.
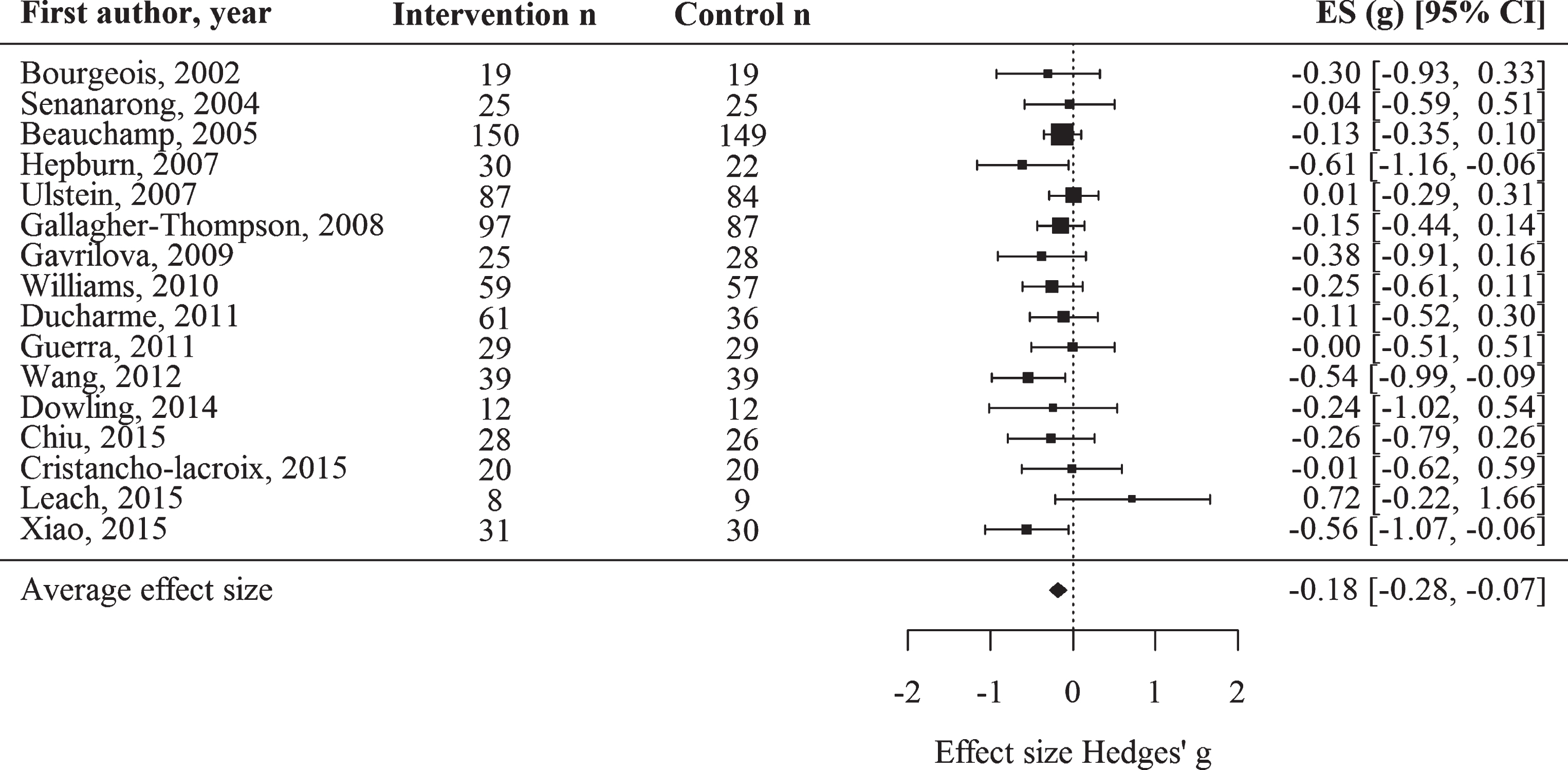
Intervention effects on stress.
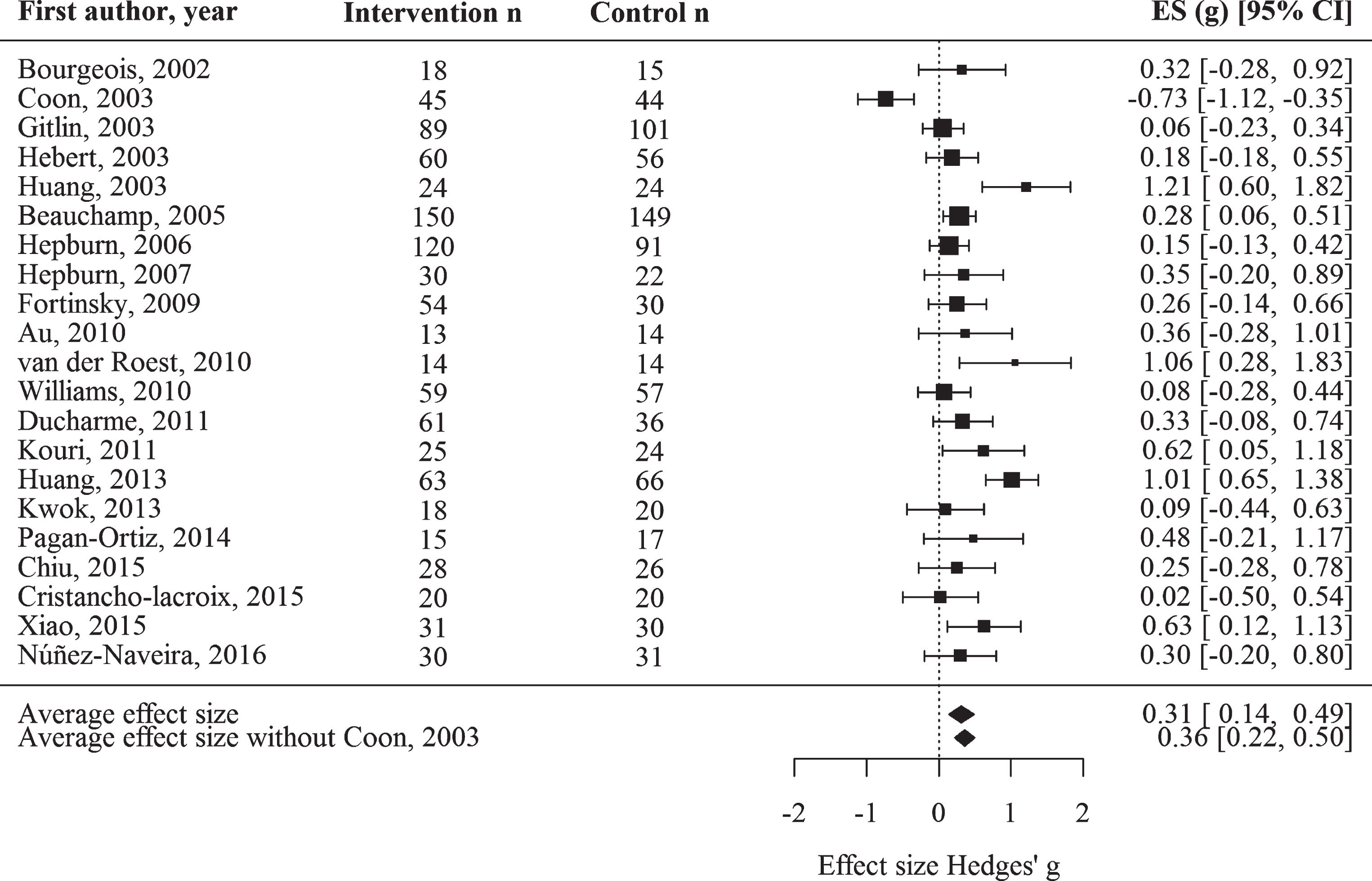
Intervention effects on sense of competence.
Anxiety
The random-effects analysis on the outcome anxiety (k = 14, total n = 1753), yielded an estimated non-significant (small) effect of g = –0.13, p = 0.058, 95% CI [–0.26, 0.00]. There was a significant amount of heterogeneity, Q (13) = 23.65, p = 0.035, I2 = 43.35%, estimated at τ2 = 0.03, SE = 0.02. Sensitivity tests identified no significant outliers.
Quality of life
Regarding the outcome quality of life (k = 15, total n = 1601), the analysis yielded an estimated significant (small to medium) effect of g = 0.36, p = 0.008, 95% CI [0.09, 0.63], in favor of the intervention group. There was a significant amount of heterogeneity, Q (14) = 71.90, p < 0.001, I2 = 86.50%, estimated at τ2 = 0.23, SE = 0.11.
Sensitivity tests (Q test and the I2 statistic) identified one outlier [35], with an effect size of g = 2.27. The model without this outlier reduced the amount of heterogeneity, Q (13) = 21.11, p = 0.071, I2 = 39.35%, estimated at τ2 = 0.02, SE = 0.02. The effect size for this model was small; g = 0.22, p = 0.001, 95% CI [0.09, 0.35].
Stress
The random-effects analysis on stress (k = 16, total n = 1392), yielded an estimated average effect of g = –0.18, p < 0.001, 95% CI [–0.28, –0.07], favoring the intervention group. There was no significant amount of heterogeneity, Q (15) = 14.40, p = 0.495, I2 = 0.00%, estimated at τ2 = 0.00, SE = 0.01). Sensitivity tests identified no outliers.
Sense of competence
The random-effects analysis (k = 21, total n = 1854) on the intervention effects on sense of competence yielded an estimated average effect of g = 0.31, p < 0.001, 95% CI [0.14, 0.49], in favor of the intervention group. There was a significant amount of heterogeneity, Q (20) = 64.84, p < 0.001, I2 = 71.04%, estimated at τ2 = 0.11, SE = 0.05.
Sensitivity tests (Q test and the I2 statistic) identified one outlier [36], with an effect size of g = –0.73. This deviating effect size was likely to due to pre-intervention differences between the intervention and control group on this outcome. The model without this outlier still yielded a significant amount of heterogeneity, Q (19) = 37.74, p = 0.006, I2 = 50.85%, estimated at τ2 = 0.05, SE = 0.03. The effect size for this model was small to medium, g = 0.36, p < 0.001, 95% CI [0.21, 0.50].
Meta-regressions
Primary predictors
Table 2 shows the meta-regressions for the primary predictor variables (delivery modality and number of sessions), per predictor, per outcome. The only meta-regression yielding a significant result was the regression on the outcome sense of competence, with the (positive) predictor number of sessions; QM = 4.40, p = 0.036.
Results of the mixed-effects meta-regression analyses per moderator, per outcome
Note. No. sessions, the number of sessions the intervention utilized (continuous variable); QoL, quality of life; SoC, sense of competence. The moderator Delivery modality was dummy coded face-to-face = 1; other = 0. First, the predictors were examined in separate meta-regressions. To explore their interaction, the analyses were repeated including both moderators and the accompanying interaction. †For Anxiety, QoL, and Stress, the predictors could not be added simultaneously, because there was no variation in delivery modality in the remaining studies. For the outcome variables depression, QoL, and SoC, the significant outliers were excluded from the meta-regressions. *<0.05, **<0.01.
Exploratory predictors
Given the amount of heterogeneity, we conducted several additional exploratory meta-regressions. The predictors were: intervention type, the content of the intervention, the materials used, adaptability to the participant, intervention duration, whether it was a group or an individual intervention, and the location (participants’ home or other). No predictors were found to systematically predict the outcomes, see Supplementary Tables 2 through 7.
Publication bias
To check for publication bias, we ran a random effects version of Sterne and Egger’s test [29] for funnel plot asymmetry (at alpha = 0.10), for each outcome separately, and again for the models without outliers. The funnel plots can be found in the supplemental material (Supplementary Figures 1–6). For the models including the outliers, significant funnel plot asymmetry was found for the outcomes depression (Z = –2.06, p = 0.039) and sense of competence (Z = 1.85, p = 0.065). For the models without outliers, significant funnel plot asymmetry was found for the same two outcomes; depression (Z = –1.80, p = 0.070) and sense of competence (Z = 1.88, p = 0.060). These findings indicate that for these models, imprecise study samples (study samples with a larger standard error) averaged larger intervention effects than precise study samples. Although such a small study effect can be due to publication bias, there might be other (non-bias related) explanations for it [29]. We also used p-uniform to check for publication bias. No evidence for publication bias was found for either outcome variable. This aligns with the finding that the majority of the primary studies yielded non-significant outcomes. Altogether, we conclude that there are no indications for publication bias or selection bias based on significance.
DISCUSSION
During the past 15 years, many interventions for informal dementia caregivers have been developed. Previous meta-analysis however examined mostly subsets of these interventions, focusing on certain types or interventions with specific characteristics. Consequently, it remained unclear to what extent the interventions work overall and if there are intervention characteristics which contribute to larger effects. The current study focused on a broad range of psychosocial and behavioral interventions and examined how effective they were overall and also explored the influence of intervention characteris-tics on this effectiveness. Despite some heterogeneity, the results concerning the mean effects show consistency across intervention effects: the pooled effects on burden, depression, quality of life, stress, sense of competence were small and in favor of the intervention groups. The pooled effect size for the outcome anxiety was not significant. The meta-regressions showed that these small effects were (mostly) independent of the number of sessions the intervention utilized, whether or not the intervention was delivered face-to-face, type of intervention, content, materials, whether or not the interventions were adaptable/tailored to the participant, whether or not it was a group intervention, and the location where the intervention took place.
Overall, previous meta-analyses involving interventions for informal caregivers found (significant) small to moderate effect sizes: Dharmawardene et al. [15] found that meditative interventions were able to significantly (with small to moderate effects) reduce caregiver depression, anxiety, stress, and heighten self-efficacy, and quality of life, but they found no significant effects for caregiver burden. Backhouse et al. [16] found that care coordinating interventions were effective (small to moderate effects) in reducing caregiver burden, but not in improving mood, quality of life, or heightening social support. Jensen et al. [17] found that educational interventions were effective in reducing caregiver burden (moderate effect) and depression (small effect). Abrahams et al. [14] found that 15 multicomponent interventions for co-residing caregivers were able to lower depression and burden, and heighten health and social support (small to moderate effects). However, all of these meta-analyses included only one specific type of intervention, and included only three to 10 studies, leading to low statistical power. In addition, the 95% confidence intervals were wide, indicating relatively weak evidence of overall effectiveness. An older meta-analysis (Brodaty et al. [19]), with 30 original studies, did examine all interventions, irrespective of the type or a specific subgroup, and found overall significant small effects on all psychosocial outcome measures. Our findings (based on 60 studies) are largely in line with these previous meta-analyses and show that interventions, irrespective of the type, or intended outcome, yield small effects.
The absence of large effects can be explained in different ways. Caregiving has a great impact on the caregiver’s life [37]. Some caregivers become homebound in this process, face difficulties maintaining or keeping employment, and feel that caregiving is a 24/7 job, without access to vacation days. While psychological interventions can help caregivers gain knowledge about dementia and to develop skills or learn how to treat people with dementia, the fact that providing care for someone with dementia can be a 24/7 job remains a major challenge. In addition, caregiving can be emotional challenging: some caregivers state that having a spouse or relative with dementia feels like a long mourning process, where they take leave from the person with dementia step by step. Researchers and clinicians may underestimate the enormous impact caregiving has on a caregiver, assuming that the problems caregivers face may be solved by (short) psychological interventions. As found in the current study, these interventions often produce small effects thereby raising some questions about their usefulness. Future research should explore other options to aid caregivers in their task, ideally together with the caregivers, because the caregivers can really point out what they need. It might be useful to start with a needs assessment to be able to tailor the interventions, and to develop person-centered interventions. In addition, these altered interventions may include respite care (which we did not review in the current study), since these interventions seem promising [38]. On the other hand, it may be useful to work towards a more continuous care plan, starting from the dementia diagnosis through all the dementia stages (which typically cause different problems), instead of only examining short, separate interventions. The current interventions, which yield small effects, can however provide guidelines or a basis for developing more effective interventions. These more effective interventions ideally sort larger effects on the (different aspects of) well-being of the caregiver, which in turn might lead to better care for the persons with dementia, so they can stay at home longer with better quality of life.
To pinpoint intervention characteristics associated with larger effects, we employed several meta-regressions, based on the intervention taxonomy by Schulz et al. [20] and the recommendations by Gaugler et al. [18]. However, we found no significant moderators. Some previous meta-analyses also investigated potential moderator variables, and these yielded mixed results: interventions delivered by a case manager with a nursing background were found to be more effective in heightening quality of life compared to those delivered by professionals with other backgrounds among four care-coordinating interventions [16]; shorter interventions were found to sort larger effects on caregiver burden than longer interventions (among five educational interventions [17]), and involvement of both the person with dementia and caregiver in the intervention may be associated with larger effect sizes on caregiver psychological morbidity [19]. However, these findings were based on small samples of studies, leading to low statistical power, and should therefore be interpreted with caution. In addition, these predictors may not be associated with larger effects on different outcome measures across other subtypes of interventions (that is, they may not be ‘consistent’ predictors). Furthermore, all of these meta-analyses examined many predictors, and only a few were found to be significant. A systematic review of systematic reviews [39] also aimed to determine which intervention aspects are most effective at maintaining the health of informal dementia caregivers. They concluded that the most effective interventions incorporated both an educational component, focused on enhancing carers’ knowledge of dementia and the caring role, and included a therapeutic component. They also concluded that the effectiveness of interventions can be further increased if delivered in a support group format rather than individually, and that multi-component interventions also benefit the person with dementia. However, Dickinson et al. [36] completed a narrative evaluation of (a subset of) existing systematic reviews and meta-analysis, instead of performing a meta-analysis on the original studies. Furthermore, the reviews included in Dickinson et al. [36] varied in their scope and inclusion criteria, and most of them did not examine predictors, but instead only included specific types of interventions. Dickinson et al. [36] did not take these limitations into consideration, which is why these results should be interpreted with caution. To summarize, the small intervention effects (found in both the current and previous studies) are likely to be independent of intervention characteristics as defined by Gaugler et al. [18] and Schulz et al. [20].
The current study had several limitations. First, not all included studies reported detailed information about the intervention used, and some authors failed to respond to e-mails asking for this information, causing us to rely on (our interpretation of) the published information. However, this may have led to us categorizing studies as being psychoeducational, or support interventions, while the original authors intended otherwise. In addition, we may have wrongly assumed that interventions did not include specific content (for instance knowledge transfer) because this was not specified, while the original authors may have thought this to be self-evident. For instance, some interventions were called ‘psycho-educational’ by the original authors, but transfer of knowledge was not included in the intervention description. In addition, if nothing was specified regarding a moderator, this was coded as a missing value, which led to lower statistical power in the meta-regressions. To overcome these problems, future research should specify detailed information about the investigated interventions. Second, we focused only on the first follow-up measurement reported by the studies. However, this measurement was not at the same moment for all studies; for some it was immediately after completion of the intervention, and for some 2 weeks after completion. A third limitation was that the original studies varied in the questionnaires used to measure all the outcome measures. For example, the outcome burden was measured (across different studies) using the Revised Memory and Behavior Checklist, the Zarit Burden Scale, the Caregiver Satisfaction Scale, and the Caregiver Reaction Assessment. The questionnaires may measure (slightly) other aspects of burden and may as such not be entirely comparable. Another limitation is that only articles written in English were included, so eligible studies in other languages were missed. However, we still had a relatively large sample of studies, leading to sufficient statistical power.
Implications for practice and research
While the current study supports findings of other meta-analyses of dementia caregiver interventions [14–17, 19], it adds to the literature because we included all types of psychobehavioral and psychoeducational interventions for informal caregivers, instead of relying on a specific subset. As a result, we have a complete overview of (the effectivity) of interventions, on a variety of outcomes, generalizable to all informal dementia caregivers. Our findings suggest that there are consistent small intervention effects across all interventions, irrespective of intervention characteristics.
The challenges informal dementia caregivers face might be underestimated and may therefore not be (entirely) solvable with psychobehavioral and educational interventions. Clinical practice with informal caregivers should be aware of these findings: the interventions may aid the caregivers to some extent, but they may need more in order to be really helped in their caregiving role. We found that several studies did not report details about the interventions, which makes comparison across studies difficult. Future research should report more details about the used interventions, to make it easier to compare the interventions and execute meta-regressions using these details. In addition, future research should explore the effectiveness of interventions complemented with other components, including for example respite care. Other ways to enhance interventions would be to personalize these, and to develop a continuous care plan, to be able to offer caregivers help through all dementia stages. This might in turn increase the effectivity of interventions and ultimately enhance the lives of informal dementia caregivers and the people with dementia they care for.
Footnotes
ACKNOWLEDGMENTS
We would like to thank all researchers who sent the data upon request and helped us collect the data we needed. This work was supported by the program Memorabel, of The Netherlands Organisation for Health Research and Development (ZonMw), part of The Netherlands Organisation for Scientific Research (NWO); and Alzheimer Nederland (project number: 733050608). However, solely the authors are responsible for the design and conduct of this study, study analyses, interpreting, drafting and editing of this article.