
Abstract
Background:
Affective symptoms are considered a risk factor or prodromal symptom for dementia. Recent reviews indicate that depressive symptoms predict progression from mild cognitive impairment (MCI) to dementia, but results need to be further explored.
Objective:
To investigate the effect of depressive symptoms on the development of dementia in people with MCI, and explore potential sources of between-study variability, including study setting by a systematic review and meta-analysis.
Methods:
Databases were searched for prospective studies defining people with MCI at baseline, investigating dementia at follow-up and giving information about depressive symptoms. Two authors independently extracted data from the studies and rated the methodological quality. Meta-analyses were conducted using random-effect models to yield pooled risk ratios (RR). Meta-regression analyses tested differences between clinical and community-based studies and other sources of heterogeneity.
Results:
Thirty-five studies, representing 14,158 individuals with MCI, were included in the meta-analysis. Depressive symptoms in MCI predicted dementia in 15 community-based studies (RR = 1.69, 95% CI 1.49–1.93, I2 = 0.0%), but not in 20 clinical studies (RR = 1.02, 95% CI 0.92–1.14, I2 = 73.0%). Further investigation of this effect showed that the mean age of community-based studies was significantly higher than of clinical studies but neither this nor other study characteristics explained variability in study outcomes.
Conclusions:
Depressive symptoms are associated with an increased risk of conversion from MCI to dementia in community-based studies. In contrast, evidence in clinical populations was insufficient with high heterogeneity.
Keywords
INTRODUCTION
Mild cognitive impairment (MCI) is a well-known risk state for developing dementia, but the heterogeneity in underlying etiologies leading to cognitive impairment causes diversity in outcome. Importantly, not all individuals with MCI will develop dementia; a longitudinal study found that less than half of the individuals with amnestic MCI will develop dementia within ten years [1]. It is important to gain insight into easily-accessible factors that predict who will develop dementia and who will not. This might indicate potential for secondary prevention or, alternatively, lead to an earlier and more accurate diagnosis, give opportunities to start care and treatment timely, and to enable patients and their families to better anticipate their future.
Affective symptoms are considered a major risk factor or prodromal symptom for dementia in the general population [2–4]. However, their predictive value in persons with MCI is unknown as current results are conflicting. A recent review and meta-analysis of a broad range of potentially modifiable predictors of dementia in MCI found that there is evidence that depressive symptoms predict progression from MCI to dementia in community-based studies, but not in clinical studies [5]. However, the study was not specified for depressive symptoms, and hence only 13 studies were included and the associations were not further explored. Additionally, another recent review and meta-analysis found evidence that depressive symptoms increase the risk of progression from MCI to dementia, but heterogeneity was very high and not further explored [6].
The aim of this study is to systematically review the current evidence and perform a meta-analysis to investigate the effect of depressive symptoms on the development of dementia in persons with MCI. In addition, we investigate study characteristics that may explain the variability in study outcomes, especially differences between community-based and clinical studies.
METHODS
This study adhered to the PRISMA statement: Preferred Reporting Items for Systematic Reviews and Meta-Analyses [7].
Search strategy
We searched the PubMed, PsycINFO, EMBASE, and CINAHL databases for relevant studies published until March 31, 2018. The following search terms were used: ‘human’ and ‘depression’, ‘anxiety’, ‘apathy’, ‘aggression’, ‘irritability’, ‘affective’, ‘mood’, ‘behavioral’, ‘neuropsychiatric’, or ‘behavioral and psychological symptoms of dementia’ and ‘mild cognitive impairment’, ‘MCI’, ‘amnestic’, ‘amnestic syndrome’, ‘memory impairment’, ‘mild cognitive decline’, ‘age-associated cognitive decline’, ‘AACD’, ‘age-associated memory impairment’, ‘AAMI’, ‘cognitive impairment no dementia’, ‘CIND’, ‘memory clinic’, ‘memory disorders clinic’, ‘dementia clinic’ or ‘memory disorder clinic’ and ‘follow-up studies’, ‘follow up studies’, ‘follow-up study’, ‘follow up study’, ‘follow up’, or ‘follow-up’. Neuropsychiatric symptoms such as anxiety and apathy were included in the search because of possible overlap with depressive symptoms and potential that associations were reported in sub-analyses. No search limits were applied.
Titles and abstracts of the retrieved studies were reviewed using the criteria specified below. Additionally, references of relevant publications were searched to identify additional studies.
Study selection
Studies were selected for further analysis if they fulfilled the following inclusion criteria: 1) prospective study; 2) defining individuals with MCI at baseline; 3) a diagnosis of dementia at follow-up according to any of the following criteria: Diagnostic and Statistical Manual of Mental Disorders 4th edition (DSM-IV) (American Psychiatric Association, 1994), DSM 3rd Revised Edition (DSM-III-R) (American Psychiatric Association, 1987), the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) (World Health Organization, 1993), National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA); 4) Available information on depressive symptoms or depression at baseline; and 5) A study cohort of 50 or more individuals.
We included all studies that defined MCI as subjective and/or objective cognitive impairment, without fulfilling dementia criteria. We included all subtypes of MCI, except for studies focusing on MCI in Parkinson’s disease.
Data extraction
Two authors independently extracted the data from the studies. When available, we extracted both the number of individuals with and without baseline depression or depressive symptoms (dichotomous variable) of converters and non-converters to dementia. We also extracted the reported risk measure including the 95% confidence interval. In addition, the following study characteristics were extracted: setting (clinical studies versus community-based studies), inclusion and exclusion criteria (specifically exclusion of a baseline major depressive disorder), MCI definition, measurement of depression, subject characteristics (e.g., gender, age, Mini-Mental State Examination (MMSE), education) and number of converters to dementia. Concerning the characteristic ‘setting’ the studies were divided into two types of studies: 1) Clinical studies: studies performed in a clinical setting (e.g., memory clinic); and 2) Community-based studies: studies performed in the general population.
In case the two authors disagreed, a third author reviewed the paper and consensus was reached. In case of incomplete data, authors were contacted and asked to complete or specify the data.
Assessment of methodological quality
To assess methodological quality, two reviewers rated each study according to a 19 items scale derived from a published method [8]. For the specific items, see Supplementary Table 1. In case of discrepancies between the reviewers, a third reviewer was asked to review and score to reach consensus. A median split and a split into tertiles of the total quality score classified studies into those with low, medium or high risk of bias.
Statistical analysis
Analyses were performed using STATA/MP version 12.1 for Mac OSX (StataCorp, Texas). Statistical significance was set at p < 0.05 in two-sided tests. The main outcome measure was the pooled risk ratio (RR) from random-effect models.
Unadjusted RR and standard errors (SE) were calculated directly from raw tables. For four studies raw data were not available and the reported risk measure was used. These risk measures were log-transformed and standard errors were calculated from the 95% confidence interval (CI). For two of these studies, only a hazard ratio (HR) was reported, but it was considered equivalent to the RR.
The amount of heterogeneity was calculated with the DerSimonian and Laird method, which is a method to estimate the variance between studies. I2 denotes the proportion of the observed variance between studies that reflects real differences rather than chance and was used next to the Q-statistic to assess heterogeneity. We performed meta-regression analyses to investigate possible sources of heterogeneity, i.e., sampling method (clinical versus community-based setting), baseline mean age of the cohort, baseline MMSE score, conversion rate, publication year, depression versus depressive symptoms, and whether studies used major depression as an exclusion criterion. Analyses were performed 1-by-1 for all variables, analyses were first performed on all studies and then for community and clinical studies separately. Publication bias was investigated using Egger’s regression test and a visual inspection of the funnel plot.
RESULTS
Search results
A total of 5,470 publications were reviewed on title and abstract, of which 208 publications were selected for further scrutiny (Fig. 1). Additionally, 20 publications were retrieved through references. Of these 228 papers, 98 were excluded due to overlap in used literature databases. Additionally, from the remaining 130 papers, 8 were posters or correspondence letters, 18 gave no or unclear information about baseline depressive symptoms, 20 referred to the same cohort as another publication, 23 were excluded because of other reasons, and 26 publications were not included because not enough data were available. Concerning the publications reporting on the same cohort, the publication with the largest sample size was selected, if the sample size was the same then the study with the longest follow-up was selected. There was one exception, concerning the data of the Alzheimer’s Disease Neuroimaging Initiative (ADNI); a recent study was selected fitting our research question most properly. Finally, 35 studies were included in the meta-analysis.
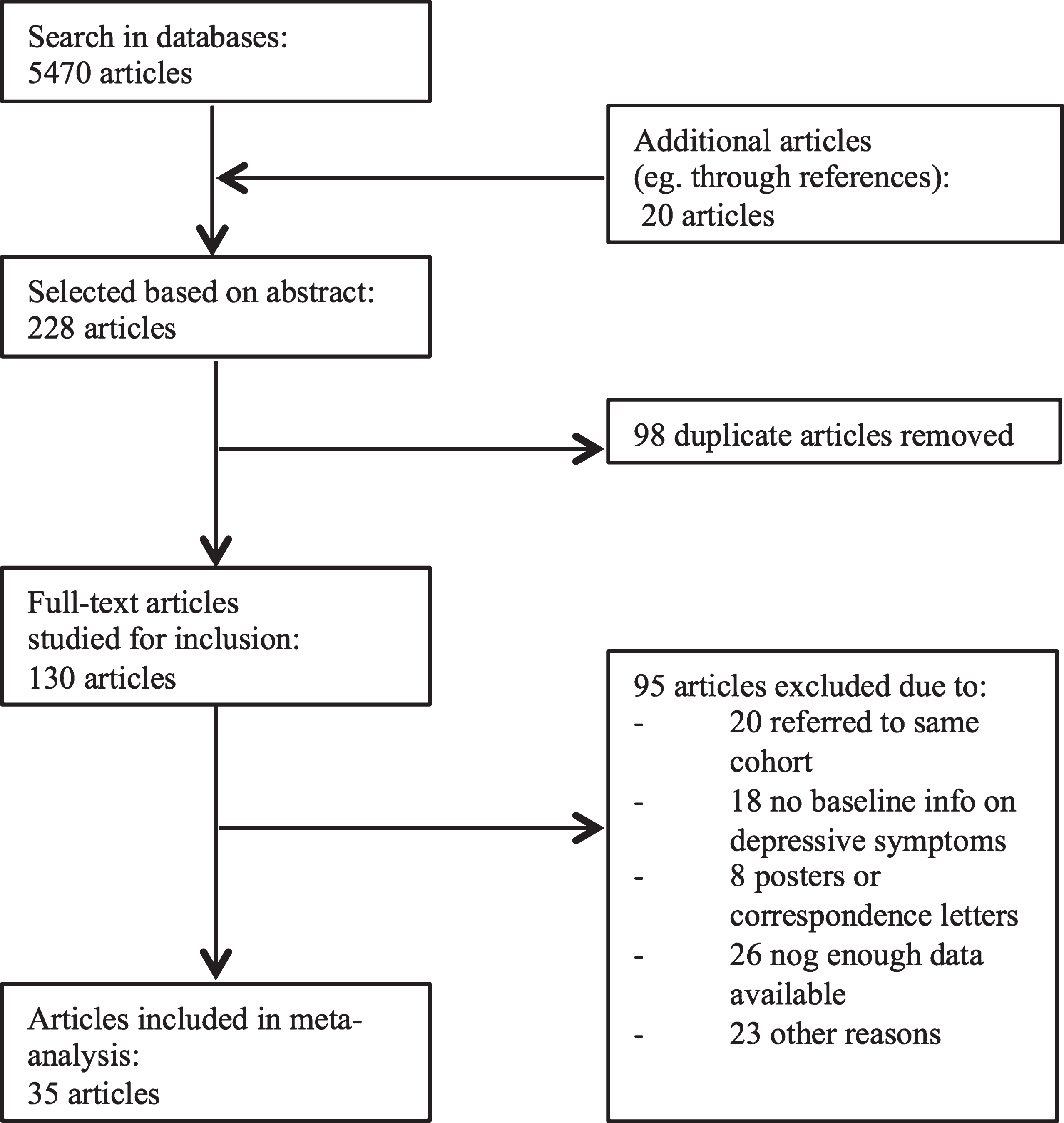
Selection of studies.
Study characteristics
In total, the 35 studies (Table 1) [9–43] included 14,158 individuals with MCI, of whom 7,855 (57.2%) were female (data missing for 1 study [41], n = 429). Of the 35 studies, fifteen were community-based studies (n = 6,803) and twenty (n = 7,355) were based on clinical samples. In 23 studies, MCI was defined according to the Petersen criteria [44] or minor variants thereof. The mean baseline age was 73.7 years (SD 4.2), mean MMSE score was 26.3 (SD 2.0) and mean education was 10.9 years (SD 3.8). In total, 3,509 (27.6%) MCI individuals showed depression or relevant depressive symptoms at baseline (not specified for 4 studies [11, 47], n = 1,427), 25.1% in community-based studies, and 32.5% in clinical studies.
Characteristics of studies included in the meta-analysis
CAMDEX-R, Cambridge Examination for Mental Disorders of the Elderly – revised; CES-D, Center for Epidemiological Studies Depression scale; CDR, clinical dementia rating scale; EADC, European AD Consortium; GDS, Global Deterioration Scale; GDS-15/GDS-30, Geriatric Depression Scale; CSDD, Cornell Scale for Depression in Dementia; HAM-D, Hamilton Depression Rating Scale; MADRS, Montgomery–Åsberg Depression Rating Scale; NACC, National Alzheimer’s Coordinating Centre; NIA-AA, National Institute of Aging and Alzheimer’s Association; NPI, Neuropsychiatric Inventory; SMC, subjective memory complaints. aWinblad et al., 2004 [57]. Extra information about depression as an exclusion criterion in some of the studies: 1MADRS >20; 2Yesavage Geriatric depression scale >16 (major depression); 3MADRS >20; 4‘Current major affective disorder’; 5‘Patients with major depressive disorder if meaningful clinical improvement in cognition accompanying improvement in depression was observed within 6 months of antidepressants treatment initiation’; 6GDS-30 >17; 7CSDD ≥22 or GDS-30 ≥21; 8GDS-15 ≥6.
In total, 3,208 (22.7%) individuals progressed from MCI to dementia during a mean follow-up period of 3.0 (SD 1.3) years. In 27 studies, it was specified whether the dementia was due to Alzheimer’s disease, which was the case in 2,367 of 11,315 (20.9%) individuals.
Meta-analysis
Dementia developed in 1,043 (29.6%) individuals with MCI with depressive symptoms at baseline, compared to 1,833 (21.1%) MCI individuals without depressive symptoms at baseline (raw data missing for 4 studies [10, 40]). The accompanying pooled RR based on data from all 35 studies was 1.19 (95% CI = 1.07–1.32). When the two studies reporting HRs were excluded, the pooled RR was 1.22 (95% CI 1.06–1.41). When the four studies that reported ratios instead of raw data were excluded, the pooled RR was 1.22 (95% CI = 1.06–1.40).
There was significant heterogeneity across studies (I2 = 73.6%, p < 0.001). Since we expected sampling method (clinical versus community-based) to partly explain differences between studies, we conducted meta-analysis stratified by sampling method. In community-based samples, the pooled risk ratio was 1.69 (95% CI = 1.49–1.93), compared to 1.02 (95% CI = 0.92–1.14) in clinical samples (Fig. 2). Additionally, heterogeneity was high in clinical studies (I2 = 73.0%) but marginal in community-based studies (I2 = 0.0%).

Pooled Risk Ratios for studies grouped by setting.
Exploratory analysis of additional variability in study outcomes
Studies were divided in two age groups: studies with a mean age ≥75 years (8 studies, n = 1927) and studies with a mean age <75 years (25 studies, n = 11087). The pooled risk ratio for studies with a mean age ≥75 years was 1.41 (95% CI = 1.12–1.77) and for studies with a mean age <75 years 1.16 (95% CI = 0.99–1.37). However, there was a large overlap between the community-based studies and the studies with a mean age ≥75 years, with a higher mean age in community-based studies than in clinical studies (76.4 versus 71.8, p < 0.001). To understand this effect further, we divided the community-based studies into those with a mean age ≥75 years or below. This showed slightly stronger associations in the younger cohorts (RR = 1.71, 95% CI = 1.38–2.14) versus the older cohorts (RR = 1.60, 95% CI = 1.32–1.93). The same analysis could not be performed in the clinical studies because only one of them had a mean age ≥75 years.
Multivariable meta-regression of all 35 studies suggested that only setting (clinical, community) significantly explained heterogeneity between studies (residual I2 = 60.0%). In this model, community-based studies reported on average a 1.61-fold higher risk (95% CI = 1.24–2.09) as a function of depression compared with clinical studies. Adding mean age to this model did not substantially change results (RR = 1.58, 95% CI = 1.13–2.22, residual I2 = 60.0%). Studies with a higher mean age did not convey a higher risk in this model (RR for age = 1.01, 95% CI = 0.97–1.05).
In an attempt to explain the variability in outcome in clinical studies, several meta-regression analyses were conducted (see Supplementary Table 2). Although all articles gave information on depression or depressive symptoms at baseline, in some clinical studies major depressive disorder was an exclusion criterion. There was no significant difference in the risk of progression to dementia in clinical studies with and without major depressive disorder as an exclusion criterion (Coef. 0.12, p = 0.627). Studies also differed in the way depression was defined, with some studies investigating depression according to clinical criteria and others as scoring above the cut-off on continuous symptom scales. Meta-regression analysis did not reveal any significant difference in outcome according to exposure definition (Coef. 0.20, p = 0.373). The Geriatric Depression Scale (GDS-15 or GDS-30) was the most commonly used scale (n = 9 out of 20 clinical studies) to measure depressive symptoms, but usage of the GDS versus other instruments did not result in a significantly different outcome (Coef. 0.02, p = 0.927). We further found no significant effect of other study characteristics: Peterson criteria for MCI (yes, no), clinical diagnosis of depression (yes, no), study quality (tertiles), mean MMSE score, mean follow-up duration, publication year, and conversion rate for explaining heterogeneity in clinical studies. Meta-regression analysis with the characteristic mean education was not possible, due to insufficient and possibly not comparable data.
Small sample effect
Visual inspection of the stratified funnel plots for community and clinical studies, as well as Egger’s regression tests for community studies (bias coef. –0.860, SE 0.542, p = 0.137) and clinical studies (bias coef. –0.675, SE 0.783, p = 0.824), showed little evidence for small study effects.
Methodological quality
Meta-regression showed that studies with high or low risk of bias did not explain heterogeneity in study outcome. Dividing methodological quality scores into tertiles did not change this.
DISCUSSION
In a meta-analysis of 35 studies, representing almost 15,000 individuals with MCI, we found strong and consistent evidence that depressive symptoms predict a higher dementia risk in community-dwelling persons with MCI. The pooled risk ratio suggests a 1.69 times higher risk in depressed people with MCI for conversion to dementia with very low between-study heterogeneity. In contrast, the pooled risk was not increased in clinical cohorts with MCI, and heterogeneity in these studies was high. Other study characteristics did not explain the difference between clinical and community-based studies.
These findings give important insight into the robustness of the association between depression in MCI and risk of dementia conversion. A recent meta-analysis with a smaller total population [6] found depression to be associated with an increase in the risk but reported high variability in study outcomes. In the current study, an association with depression was only found in the community-based studies, which has also been shown in an earlier study by Cooper et al. [5]. The latter was, however, a smaller study (13 studies on depression compared to 35 in the present one), not focusing on depressive symptoms in particular. Importantly, our meta-regression analyses show that the difference between study settings is not explained by other study characteristics such as mean age, follow-up-duration, definition of MCI, or how depression was assessed.
The results of our study and these two studies also amplify two meta-analyses in cognitively healthy persons: a meta-analysis [2] studying the risk of dementia in cognitively healthy older adults with late-life depression in community-based prospective cohort studies found that late-life depression is associated with a 1.8-fold increased risk of incident all-cause dementia, and a meta-analysis [3] that found that cognitively-healthy persons with a history of major depression are more likely to be diagnosed with Alzheimer’s disease later in life than persons without a history of major depression.
In clinical studies we could not find an association between depressive symptoms and the progression from MCI to dementia. A possible explanation is that heterogeneity in clinical studies was very high (I2 = 73.0%). An exploratory analysis indicated that age partly explains this heterogeneity. Another possible explanation for the heterogeneity might be that there are many different types of memory clinics in and outside hospitals with different populations (e.g., neurology, psychiatry, internal medicine). A study in a clinical population on neurobiological correlates of depressive symptoms in individuals with MCI and subjective memory impairment found that depressive symptoms are common, but not associated with pathological Alzheimer’s disease biomarkers [47]. The authors suggest that in their clinical population depressive symptoms may drive the cognitive symptoms rather than being a mere correlate of neurodegenerative changes. This finding could also explain why some of the clinical studies in this meta-analysis found a negative relation between depressive symptoms and progression from MCI to dementia. Also, in clinical studies of individuals seeking help, one could expect the symptoms, whether being depressive symptoms or cognitive problems, to be more severe. This could lead to hypothetical subgroups of individuals with MCI with different subsets of symptoms and a different course and outcome. A recent study by Hanfelt el al. [48] on latent classes of MCI, in a clinical population, indeed found that seven latent classes of MCI differed significantly in clinical outcome. It could be that the heterogeneity in the clinical studies is a reflection of different classes with different outcomes, while in the community studies the homogeneity may indicate fewer classes or a different distribution.
The direction of the relation between depression and dementia in the community-based studies remains unclear. Different hypothesis are plausible and described in the literature, suggesting a causal or corollary effect or favoring reversed-causality [49, 50]. For instance, depressive symptoms may interact with, or provoke, the pathophysiological mechanism(s) of dementia, for example due to a cortisol-hippocampal pathway [49], resulting in a faster progression from MCI to dementia. Another hypothesis is that the progression from MCI to dementia itself leads to depressive symptoms, for example as an early symptom [51]. A quite similar hypothesis could be that the awareness of the patient that his or her cognitive functions are failing results in depressive symptoms. A fourth, and often postulated, hypothesis is the vascular depression hypothesis in which depression is associated with an increase in vascular risk factors and therefore an increased incidence of cognitive dysfunction due to cerebral small vessel disease [52]. Indeed, some studies suggest that cerebrovascular factors are the link between depressive symptoms and the progression from MCI to (vascular) dementia [41, 53]. Moreover, the meta-analysis of Diniz et al. found that, in case of late-life depression, the risk of vascular dementia is significantly higher than for Alzheimer’s disease. Unfortunately, we were not able to perform a separate analysis focusing on vascular dementia due to insufficient data. Late-life dementia is often due to mixed brain pathologies (i.e., both vascular and Alzheimer’s disease factors) [54]. Since depression has been strongly related to cerebrovascular disease including cerebral small vessel disease [55], stroke [56], and vascular dementia [2], its predictive value for dementia should be higher in populations that comprise more (mixed) vascular pathologies. This might also explain the paralleling effect of age: since the mean age in community studies was higher than in the clinical studies, there may have been more vascular or mixed dementias in the community-studies. Of course, also a combination of these different hypotheses is possible in which different mechanisms operate in different (groups of) individuals (Fig. 3).

Different hypotheses concerning the direction of relation between depressive symptoms and progression from MCI to dementia. a) Depressive symptoms influence the pathophysiological mechanisms of dementia. b) 1. The progression from MCI to dementia itself leads to depressive symptoms as an early symptom, 2. The awareness of failing cognitive functions leads to depressive symptoms.c) Another factor (e.g., vascular risk factors) leads to progression to dementia and to depressive symptoms.
Although the direction of the association between depressive symptoms and dementia in the community studies is unclear, the present study does imply screening of depressive symptoms in MCI. The detection of depressive symptoms may lead to adequate treatment and a better quality of life, and may possibly modify the progression from MCI to dementia.
Strengths of this study are the comprehensive and broad search for the literature review, and the extensive analyses. However, the study has several limitations. First, useful studies may be missing because not all data were available in the published papers and not all authors of previous studies replied to our requests for additional data, for example because the authors were already retired. These studies were mainly studies with an earlier publication year. Furthermore, as noted before, we were able to include 35 studies, instead of the 13 and 18 studies included in earlier meta-analyses [5, 6]. Second, studies with different MCI definitions were included, although most studies used Petersen criteria [44] or criteria quite similar to Petersen criteria. Meta-regression findings showed that this did not affected our results. In addition, there was also heterogeneity in the depression scales, although meta-regression analysis indicated that this had no effect on the results. As stated earlier, heterogeneity in clinical studies was high and we could only partly explain this heterogeneity. Also, more information on the type, course and any received treatment of depression and depressive symptoms, e.g., history of depression and age of onset, would have given more insight into the kind of association, but was unfortunately not available in enough studies to perform meta-regression analysis. More information on the type, course and any received treatment of the depressive symptoms could also have been useful to further understand the heterogeneity in the clinical studies.
In conclusion, we found strong evidence that depressive symptoms predict higher dementia risk in community-dwelling persons with MCI. More research is needed to identify the underlying mechanisms of this higher risk, particularly vascular risk factors should be taken into account and studies should differentiate between types of dementias. We found no significant association in clinical studies, but heterogeneity in these studies was very high.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/18-0513r2).