
Abstract
Background:
Neurological features are often overlooked in systemic sclerosis (SSc) patients and little is known about the link between dementia and SSc.
Objectives:
We sought to investigate whether an association exists between Alzheimer’s disease (AD) and SSc, as well as assess the impact of a dual diagnosis on mortality rates, by performing an extensive data analysis on a large subject sample.
Methods:
We utilized the medical database of the Clalit-Health-Services in a case-control study. Patients with SSc were compared with age- and sex-matched controls with regard to the prevalence of AD and its impact on their mortality.
Results:
Our study included 2,431 SSc patients and 12,377 age- and sex-matched controls. The mean age of the study population was 63.32±18.06 years and the female to male ratio was 4.5:1. 134 (5.5%) cases had AD as a co-morbidity in comparison with 749 (5.9%) of the controls. The mortality rate was 12.5% among controls and 26.2% among SSc cases. On the Cox multivariate survival analysis, diagnosis of SSc and AD demonstrated significant HRs (2.35 (95% CI 2.05–2.69, p < 0.0001) and 2.19 (95% CI 1.94–2.48, p < 0.0001), respectively). SSc patients with AD had a relative risk of death of 2.35 (95% CI: 1.44–3.83) in comparison with SSc patients without AD.
Conclusion:
AD is a predictor of death in SSc and therefore preemptive screening may be warranted. Further studies are needed to evaluate whether improvements in the medical regimen for SSc may lead to a reduction in AD development and possibly to increased survival as well.
INTRODUCTION
Systemic sclerosis (SSc) is a connective-tissue disorder characterized by micro-vascular damage and tissue fibrosis. Its prevalence varies greatly according to geographic location, ranging between 30–340 cases per million people [1]. The pathogenesis of SSc is a complex interplay between innate and adaptive immune system dysregulation and small vessel endothelial fibroproliferative vasculopathy, resulting in an extensive accumulation of collagen and other matrix components in various organs [2].
In the last decades, SSc survival has improved significantly due to advances in SSc therapy, with an emphasis on breakthroughs in the management and treatment of renal crisis [3]. However, recent studies still report decreased survival rates with a standardized mortality ratio of 1.46 [95% confidence interval (CI) 1.28–1.69] [4]. The significant morbidity and mortality of patients with SSc is mainly attributed to severe involvement of the cardio-respiratory system, and pulmonary fibrosis and pulmonary arterial hypertension are considered the leading causes of SSc-related deaths [1, 5].
Although the pathology of SSc is marked by diffuse small vessel vasculopathy and extensive tissue fibrosis of various organs, primary central nervous system involvement in SSc is believed to be rare, perhaps due to the fact that the brain parenchyma itself is largely collagen-free [6]. Thus, vascular cognitive impairment is rarely attributed to SSc and neurological symptoms are considered uncommon and unusual features in the disease’s clinical presentation [6, 7]. Nevertheless, recent imaging studies have demonstrated focal and diffuse cerebral hypoperfusion in more than half of neurologically asymptomatic SSc patients [8, 9]. Furthermore, according to a recent systematic review of the literature, 8.47% of SSc patients present with cognitive impairment [10]. Other reported manifestations of central nervoussystem involvement were headache and seizures.
Among other neuropsychiatric disorders, Alzheimer’s disease (AD) has rarely been investigated in context with SSc and only several case reports have raised the possibility of an association between the two diseases [11, 12]. Therefore, the present study was conducted on a large-scale population-based database with the goal of shedding light on the potential link between these two disorders.
MATERIAL AND METHODS
Design, sample, and procedures
This study represents the first of a series of explorative and analytic studies aimed at investigating the impact of co-morbidities on the diagnosis of SSc. These studies are based on the chronic diseases registry of the Clalit Health Services (CHS), the largest healthcare maintenance organization in Israel which provides services for approximately half of the Israeli population. The CHS chronic diseases registry receives input data from a variety of sources, namely, pharmaceutical, medical and administrative computerized operating systems.
With the use of massive data-mining techniques, an array of patient data can be automatically extracted from the database, allowing scholars to perform a wide-scale epidemiological study on a real-time heterogeneous population in an effective and accurate manner. Using the CHS’s computerized database, we extracted a cohort consisting of SSc patients and compared them with age- and sex-matched controls. The data drawn from the database were recorded continuously since the beginning of the utilization of computerized systems in the CHS, approximately from the year 2000 until the year 2017.
Measures
SSc patients were defined as such if they had at least one documented diagnosis of SSc in their medical records as an outpatient, either by a primary care physician or a specialist, or if they were diagnosed with SSc in their hospital discharge papers. All SSc patients detected in the CHS database were considered eligible and, as such, enrolled in this study. Controls were randomly selected from the CHS database, with the exclusion of SSc patients. Approximately five controls were matched by age and gender for each SSc patient. Data available from the CHS database included age, sex, socioeconomic status (SES), body mass index (BMI), and diagnoses of chronic diseases. More in detail, SES was defined according to the poverty index of the member’s residence area as defined during the 2008 National Census. More specifically, the poverty index was computed based on an array of several parameters, including household income, education, crowding, material conditions, and car ownership, among others. This composite index can range from 1 to 20, based on cluster analysis, with 1 as the lowest SES and 20 as the highest. We divided the population into three categories according to their SES. Concerning BMI, in order to reflect a nonlinear relation between BMI and dependent variables, BMI was classified into 4 categories: <20, 20–25, 25–30, and >30 kg/m2.
The definition of AD, similar to that of SSc, was based on a documented diagnosis of AD inmedical records, as registered in the CHS database. The validity and reliability of the diagnoses in the registry were found to be high, as shown in ourpreviously published studies [13 –16].
Statistical analyses
Rates of AD were compared between SSc patients and controls in the study sample group. The Chi-square test was used to assess the distribution of categorical socio-demographic and clinical parameters, such as SES and gender, between SSc patients and controls. The student’s t-test and one-way analysis of variance (ANOVA) or their non-parametric versions, were applied for continuous parameters, such as age at study commencement or age at diagnosis/beginning of the follow-up (between two and more groups, respectively), based on the normality of data distribution.
The association between SSc and AD was evaluated by a multivariate logistic regression model, adjusting for possible confounders. Dates of registration in the medical records of SSc (or alternatively, start of follow-up for controls), AD and death, as well as anthropometric information and medical co-morbidities, were extracted from the database when available.
Survival analysis using Kaplan-Meier curves, log-rank test and multivariate Cox proportional hazards method was performed to detect variables associated with an increased risk of all-cause mortality, adjusting for possible risk factors.
All statistical analyses were carried out with the commercial software “Statistical Package for Social Sciences” for Windows (SPSS version 24.0, IBM, USA). Figures with a p-value of less than 0.05 were considered statistically significant.
RESULTS
The overall population of the present study was comprised of 15,141 subjects, of which 2,431 were SSc patients and 12,377 were age- and sex-matched controls (case-control match - 1:5.2). The mean age of the study population was 63.32±18.06 years (median 66 years) and the female to male ratio was 4.5:1. No statistically significant differences could be found in terms of age at study commencement, age at diagnosis/beginning of follow-up, gender, and smoking habits. The SSc group had significantly lower proportions of overweight and obese subjects than the controls (p < 0.0001), as well as subjects from medium and high SES categories(p < 0.0001).
Concerning AD as co-morbidity, 883 cases were diagnosed: 749 (5.9%) among controls and 134 (5.5%) among cases. The mortality rate of the study population was 14.7%, with altogether 2,226 deaths; 12.5% among controls (1,589 deaths) and 26.2% among SSc cases (637 deaths, p < 0.0001). For further details, the reader is referred to Table 1.
Overall population, systemic sclerosis (SSc) patients (cases) and age-and-sex matched controls – basic characteristics
aAvailable for 91.8% of data; bAvailable for 94.1% of data. SSc, systemic sclerosis; AD, Alzheimer’s disease; BMI, body mass index; SES, socioeconomic status SD; NS, not significant.
On multivariate logistic regression which assessed covariates, age (1-year increment, OR 1.14 [95% CI 1.13–1.15], p < 0.0001), BMI (20–25 kg/m2, OR 0.59 [95% CI 0.45–0.79], p = 0.0003; 25–30 kg/m2, OR 0.47 [95% CI 0.36–0.63], p < 0.0001; >30 kg/m2, OR 0.48 [0.36–0.64], p < 0.0001), SES (high, OR 0.64 [0.51–0.80], p = 0.0001) and a smoking habit (OR 0.70 [0.57–0.86], p = 0.0008) were all independently associated with AD in a statistically significant way. Further details are shown in Table 2.
Multivariate logistic regression assessing covariates associated with Alzheimer’s disease
SSc, systemic sclerosis; BMI, body mass index; SES, socioeconomic status.
When stratifying according to presence of SSc and AD, 11,961 controls had neither diagnosis and 749 were diagnosed with AD. In the SSc group, 134 had an additional diagnosis of AD and 2,297 did not. The four groups differed in terms of age at study commencement, age at diagnosis/beginning of follow-up, BMI, SES, smoking habits, and all-cause mortality rate (p < 0.0001 for all variables), however the gender ratio was relatively consistent between the groups. Additional details are reported in Table 3.
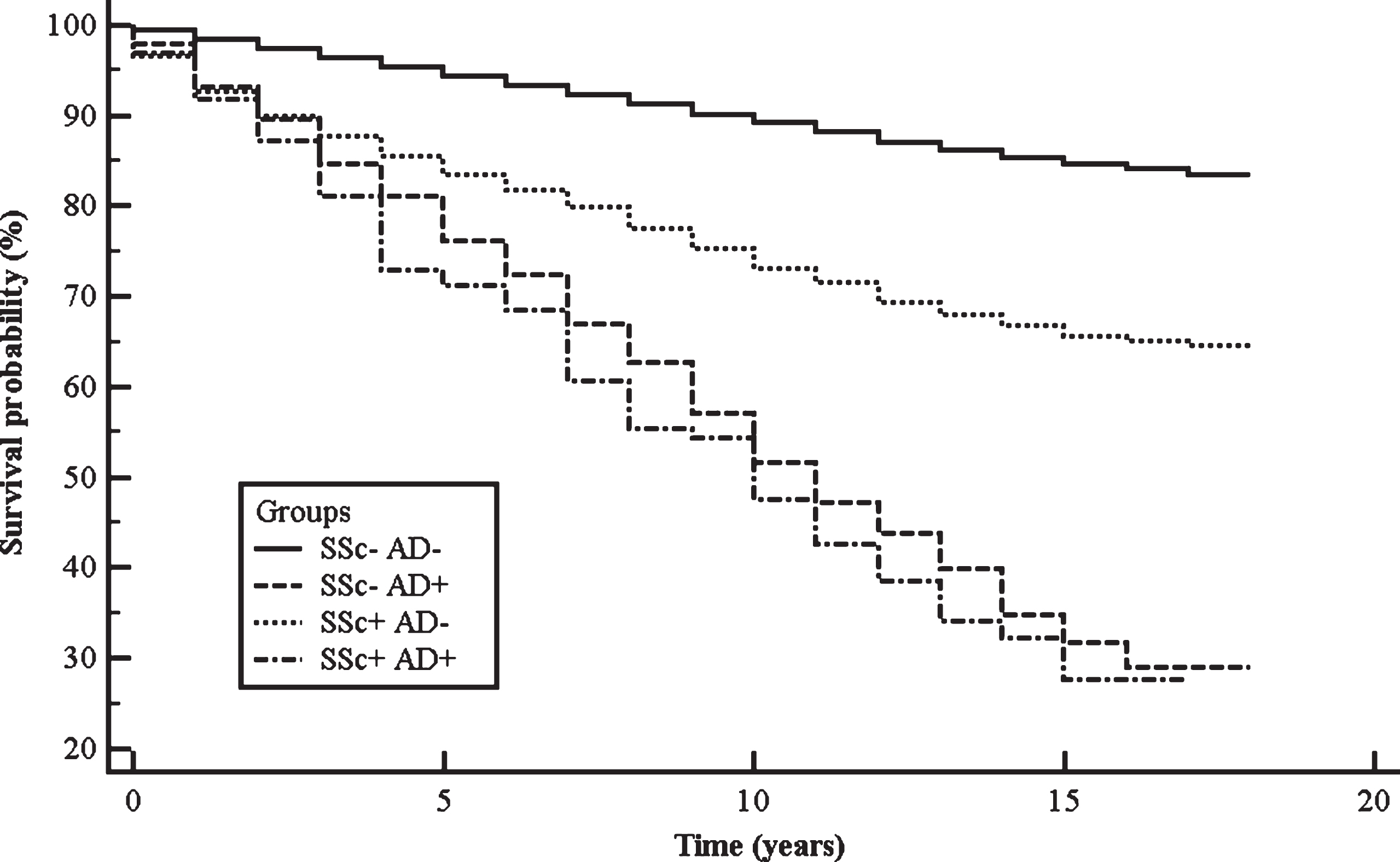
Kaplan-Meier survival plot of study cohorts (namely, SSc cases with and without AD, and controls with and without AD). SSc, systemic sclerosis; AD, Alzheimer’s disease.
Systemic sclerosis patients and controls with and without Alzheimer’s disease– basic characteristics
SSc, systemic sclerosis; AD, Alzheimer’s disease; BMI, body mass index; SD, standard deviation; NS, not significant. aAvailable for 91.8% of data; bAvailable for 94.1% of data.
The Kaplan-Meier analysis (Fig. 1) resulted as statistically significant at the log-rank test (Chi-squared = 1,416.62, degrees of freedom = 3, p < 0.0001), showing the impact of AD diagnosis. HRs with their computed 95% CIs, obtained from the Kaplan-Meier survival analysis, are shown in Table 4. As expected, the diagnosis of SSc dramatically impacted mortality rate, as can be seen when comparing SSc patients without AD to controls without AD (HR 2.73 [95% CI 2.42–3.08]). AD as a co-morbidity worsened the prognosis of SSc (HR 2.35 [1.44 –3.83]). Interestingly, it can be observed that the diagnosis of AD (either in cases or controls) has a significant effect with respect to controls without AD (HR 5.68 [95% CI 4.65–6.92] and HR 6.42 [95% CI 3.99–10.35], respectively). On the other hand, the HR of SSc patients with AD in comparison with controls with AD was not considered statistically significant (HR 1.13 [95% CI 0.68–1.89]). Controls with AD had a statistically significant HR with respect to cases without AD (HR 2.08 [95% CI 1.66–2.59]). In other words, on the Kaplan-Meier survival analysis, without correcting for potential confounders, the diagnosis of AD seems to dramatically impact mortality rate, irrespectively of a SSc diagnosis.
Hazard ratios (HRs) computed with their 95% Confidence Interval (CI) obtained from the Kaplan-Meier survival analysis
SSc, systemic sclerosis; AD, Alzheimer’s disease.
On the Cox multivariate survival analysis, age (1-year increment, HR 1.05 [1.05–1.06], p < 0.0001), BMI (20–25 kg/m2, HR 0.79 [95% CI 0.67–0.94], p = 0.0058; 25–30 kg/m2, HR 0.65 [95% CI 0.55–0.76], p < 0.0001; >30 kg/m2, HR 0.76 [95% CI 0.64–0.89], p = 0.0009), gender (female, HR 0.72 [95% CI 0.64–0.81], p < 0.0001), SES (high, HR 0.73 [95% CI 0.64–0.84], p < 0.0001), diagnosis of SSc (HR 2.35 [95% CI 2.05–2.69], p < 0.0001) and diagnosis of AD (HR 2.19 [95% CI 1.94–2.48], p < 0.0001) were associated with all-cause mortality (Table 5).
Cox multivariate survival analysis assessing covariates statistically associated with all-cause mortality
SSc, systemic sclerosis; AD, Alzheimer’s disease; BMI, body mass index; SES, socioeconomic status.
DISCUSSION
In the present study, we demonstrated the significantly adverse impact of AD on the mortality rates of SSc patients. SSc patients with AD had an estimated relative risk (RR) of death of 2.35 (95% CI: 1.44–3.83) in comparison to SSc patients without AD. However, the prevalence of AD was found to be similar between SSc patients and controls (5.5% versus 5.9%, respectively).
Various reports in the literature have revealed the tendency of patients with autoimmune disorders towards development of dementia and AD. A recent study which compared 34,660 middle-aged autoimmune disease patients with 138,640 controls detected an increased risk of 1.18 for developing dementia amongst the patient group, after adjustment for confounders [17]. A significant association between systemic lupus erythematosus, a prototypal disease of autoimmune dysregulation, and dementia, was reported in a cross-sectional study by Gendelman et al. [18] (odds ratio = 1.51, 95% confidence interval, 1.11-2.04).
When the potential link between SSc and dementia was examined more closely, Robinson and coworkers reported RRs of 1.6 and 2.3 for the MarketScan and IMS Health databases, respectively (95% CI: 0.8–3.2 and 0.7–7.8, respectively) [19]. A systematic review conducted by Amaral et al. [10] which described the neurologic involvement in SSc, as well as in localized scleroderma, demonstrated that central nervous system involvement in SSc, which is considered to be relatively rare, was characterized by headache, seizures, and cognitive impairment in significant percentages (23.73%, 13.56%, 8.47%, respectively), although the nature of the cognitive impairment was not specified.
The extremely pertinent subject of survival in patients with dementia has been assessed numerous times. A prospective population-based cohort study by Helmer et al. [20] determined that people with dementia had an increased risk of death in comparison to those without, yielding an RR of 1.82 (95% CI: 1.77, 2.68). Furthermore, several studies have found an interaction between dementia and various terminal diseases, such as end stage renal disease and Parkinson’s disease [21, 22]. However, our study is the first to demonstrate the detrimental effect of dementia on the prognosis and outcome of SSc. Moreover, in addition to the higher RR of death generated by the presence of SSc (2.73), we found that the RR of death for subjects with a dual diagnosis of both SSc and AD was 6.42, when they were compared to controls with neither disease.
Another one of the interesting findings in our study was the protective effect of smoking upon AD development. Previous studies have reported conflicting results regarding the link between smoking and AD. In a large meta-analysis, the label of ever smoking was associated with an increased risk of AD of 1.12 (95% CI 1.00–1.26), albeit the risk was of marginal significance [23]. Other studies have also described smoking as a risk factor for AD [24, 25]. However, it has also been reported that short-term nicotine administration may provide modest improvements in measures of mental functioning for AD patients, which supports the notion of a protective influence [26]. Moreover, nicotine has been found to have a possible effect on amyloid deposition due to inhibition of β-amyloidosis formation [27].
In our study, BMI was found to be inversely associated with AD. In a similar manner to the previously discussed link between smoking and AD, studies attempting to evaluate the association between BMI and dementia have produced contrasting results. In corroboration with our findings, a large cohort study which followed two million people over a study period of two decades, demonstrated that people who fell in the underweight category during middle and old age had an increased risk of dementia [28]. In contrast, a recent meta-analysis determined that mid-life obesity was a risk factor for dementia development [29], and an additional study has reported that the link between BMI and dementia is influenced by the length of the follow-up period; thus a higher BMI appears protective in the short term, yet a harmful effect emerges during a longer follow-up period [30]. BMI was also inversely associated with mortality: in epidemiology, this is known as the “obesity paradox”, “reverse epidemiology”, “reverse causation” or “BMI paradox”, a hypothesis initially put forth by Kamyar Kalantar-Zadeh in 2003 [31], which claims that obesity and high cholesterol levels, despite being major risk factor for cardiovascular disease may be protective and associated with better prognosis and greater survival rates in certain subjects, such as very elderly individuals or patients suffering from certain chronic-degenerative disorders, when compared to individuals with normal BMI.
When focusing on the link between SES and dementia, the findings of our study support previous reports in the literature that a lower SES can predict cognitive decline independently of biomedical factors. When using different indicators of SES, including education, income, and ownership of financial assets, ORs for cognitive decline ranging from 1.51 to 2.16 were found in the lowest socioeconomic groups [32]. Another study which followed 2,457 elderly individuals for 12 years, demonstrated that African-American participants, who typically have higher proportions of lower SES, were more likely to develop dementia in comparison with participants of Caucasian descent (20.7% versus 16.6%, respectively, p < 0.001) [33].
Our study has several strengths, mainly the novelty of its objectives and its population-based design, which avoids the potential referral bias that often afflicts center-based studies. Our approach relies on Big Data, which are extremely promising and are anticipated to drive innovation in the field of biomedicine. Specifically concerning AD, initiatives such as the AD Big Data DREAM Challenge or OMICS-based investigations, are aimed at identifying new biomarkers and dissecting the physio-pathological basis of AD from a molecular standpoint, potentially leading to the discovery of new druggable targets and therapeutic compounds [34, 35]. However, there are several drawbacks, which should be properly acknowledged. The major limitation was that due to the reliance on the CHS database, we were unable to distinguish between the various clinical variants of SSc (i.e., limited versus diffuse) and further explore their separate associations with AD. Additionally, information regarding the pharmacological treatment administered to patients and its potential impact on our results, was lacking.
In conclusion, we found that although SSc patients have a similar prevalence of AD in comparison with controls, the impact of AD on SSc outcomes is significant, and a concurrent diagnosis of AD may be considered a predictor of death for SSc patient. Therefore, the corroboration of this association has clinical implications and preemptive screening for AD development may be warranted. Further studies are needed to evaluate whether improvements in the medical regimen for SSc may lead to a reduction in AD development and possibly to increasedsurvival.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/18-0516r1).