
Abstract
Background:
Neuropsychiatric symptoms and cognitive impairment are independent contributors of functional impairment in activities of daily living (ADL) in Alzheimer’s disease (AD) patients. ADL could be divided according to its complexity in three subdomains: basic (BADL), instrumental (IADL), and advanced (a-ADL).
Objective:
Studying the cognitive and neuropsychiatric determinants of BADL, IADL, and a-ADL in normal cognitive elders and AD patients.
Methods:
144 subjects were graduated using the clinical dementia rating (CDR) in CDR = 0, n = 52 (control group) and 92 AD patients CDR = 0.5, n = 34 and CDR = 1&2, n = 58. They were assessed with measures of cognitive performance and neuropsychiatric symptoms that were included in regression models to measure the best predictors for each ADL subdomain at every CDR status.
Results:
AD patients were significantly older, and had significantly more severe functional impairment, neuropsychiatric symptoms, and cognitive decline than controls. The best predictors of functional impairment in controls and CDR = 0.5 AD patients were neuropsychiatric symptoms; in the CDR 0.5 patients, apathy severity was the most important determinant of IADL and a-ADL impairment. While in the CDR 1&2 AD patients, cognitive impairment was the principal determinant of functional impairment, being memory the best determinant of IADL and a-ADL impairment, while global cognition was of BADL impairment.
Conclusions:
The contribution of cognitive impairment and neuropsychiatric symptoms varied according to the subdomain of ADL, and the CDR. In very mild AD and controls the neuropsychiatric symptoms are the best predictors of more complex ADL impairment, while cognitive impairment is more important at mild to moderate states of AD.
Keywords
INTRODUCTION
The number of elderly people is set to increase dramatically worldwide, demographic changes are likely to result in the rise of age-related chronic diseases which largely contribute to years lived with disability [1]. In low and middle-income countries dementia has been found as the leader cause of disability [2] and dependency in elderly people [3].
Dementia definition requires the presence of cognitive impairment (CI) associated with acquired functional impairment (functional impairment) in activities of daily living (ADL) [4, 5]. However, the notion that functional impairment starts only at the stage of dementia has been challenged with several studies showing that minor impairment in complex ADL precede dementia in many years [6, 7] and are already present at the stage of mild cognitive impairment (MCI) [8, 9].
Thus, ADL includes activities of different levels of complexity, been traditionally divided in Basic ADL (BADLs) and Instrumental ADL (IADLs). BADL are defined as the daily activities directly related to basic physiological and self-regulated needs, including tasks like eating, toileting, or getting dressed, while IADL, involve activities for maintaining life in community, such as managing finances, shopping, handle medications, or using the public transportation [10]. However, an additional and important category of IADL could be separately evaluated: the advanced ADL (a-ADL) that are more complex activities related with social functioning [11]. Some of these activities are going on holidays, doing sports, practice hobbies, use technology, and employment [12, 13].
In patients with Alzheimer’s disease (AD), functional impairment in ADL have been usually accepted to be the consequence of cognitive decline, but other non-cognitive symptoms, like behavioral and psychological symptoms, or frequently called neuropsychiatric symptoms (NPS) had emerged as mayor contributors to functional impairment [14–16]. Indeed, NPS and CI seems to be independent contributors of everyday function’s limitations in older adults with and without cognitive impairment [17]. Identifying specific risk factors for functional impairment in elderly population and AD patients is particularly important for planning targeted interventions for preventing this decline [18].
Importantly, to our knowledge, no studies have addressed the determinants of functional impairment in activities of different level of complexity (i.e., BADL, IADL, and a-ADL)
This study aims to establish the cognitive and neuropsychiatric variables associated with functional impairment at different ADL subdomains in cognitively normal elders, very mild AD, and mild to moderate AD dementia.
METHODS
Subjects
A convenience sample made up of 52 cognitively normal elders or “control group” and 92 AD patients were considered in this study. They were recruited from two memory clinics: The Clinic of Memory and Neuropsychiatry (CMYN) of the Neurology Department at Hospital del Salvador, and the Neuropsychology Unit of the Neurology and Neurosurgery Department at Hospital Clínico Universidad de Chile (HCUCH), which are both located in Santiago, Chile. Inclusion and exclusion criteria are detailed in a previous study [19]. Broadly, they were Spanish-speaking participants older than 60 years of age with a proper capacity to provide consent for research, without underlying neurological or psychiatric illness that could affect cognition (except AD). Ethical approval for this study was obtained from the Ethical and Scientific Committee of the East Metropolitan Health Service and HCUCH. All participants, or their legal guardian, provided informed consent in accordance with the Declaration of Helsinki.
Clinical diagnosis of cognitive status was made by consensus between neurologists based on the interviews with the subjects and reliable proxies, neuropsychological assessment, and a complementary study. Neurologists rated all participants according to the clinical dementia rating scale (CDR) [20]; in those without cognitive decline or controls (CDR = 0), and with very mild (CDR = 0.5) or mild to moderate cognitive decline (CDR = 1&2). Since we did not measure any biomarker to support AD diagnosis, and because of the great variability in the evolution of patients with MCI [9], we only included patients that fulfill the criteria for AD dementia (ADD) [4]. ADD patients displayed a history of progressive and significant episodic memory loss, confirmed the proxy and poor performance on an episodic memory test (free recall <20 in the Word Free and Cued Selective Reminding Test (FCSRT) [21] and loss of independence in daily life [22]. Also, they had a complementary study including structural neuroimaging and serological exams that excludes other causes of cognitive impairment.
Activities of daily living were measured by the informant using the Technology-Activities of daily living questionnaire (T-ADLQ) [23]. The T-ADLQ, is composed of 33 items that measure different ADL, gathered in 7 subscales. Each item is rated on a 4-point scale from 0 (no problem) to 3 (no longer capable of performing the activity). Higher percentage scores indicate major deterioration. For each item, a rating is provided for instances in which the patient may never have performed that activity in the past, stopped the activity prior to the onset of dementia, or for which the proxy did not has information [24]. An expert panel (2 neurologists, 3 psychologists, 1 occupational therapist) gathered the activities of the T-ADLQ in three subdomains (BADL, IADL, and a-ADL). The consensus of the classification is presented in Table 1.
Division of the three domains of the Technology – Activities of daily living questionnaire: Basic (B), Instrumental (I), and Advanced (A)
Cognitive performance
Experienced clinical neuropsychologists administered an extensive battery of tests described in detail elsewhere [19]. It included among others the Chilean’s versions of the MMSE [25] and the ACE-R [26] to assess global cognitive functioning; the “Word” Chilean Spanish-version of the FCSRT [21] to measure episodic memory, the Frontal Assessment Battery (FAB) [27] and the Modified Version of the Wisconsin Card Sorting Test (MCST) [28] to measure executive function. The MCST has two main scores, the number of categories achieved and the number of perseverative errors, a proper measure of cognitive flexibility.
Behavioral and psychological symptoms
The NPS were measured using different questionnaires: for global measurement we used the Chilean version of the Neuropsychiatric Inventory Questionnaire (NPI-Q) [29]. The NPI-Q is rated by the proxy and evaluates 12 neuropsychiatric disturbances common in dementia [30]. The presence and severity of each symptom was rated from 0 to 3 on the basis of scripted questions administered to the proxy. In addition, we calculated the total NPI severity score ranking from 0 to 36.
Apathy was measured using the apathy evaluation scale informant version (AESi). It consists in a18 item questionnaire which is rated on a 4-point Likert scale from 1 (not at all characteristic) to 4 (very characteristic). Higher scores indicate higher levels of apathy [31]. Significant levels of apathy were considered 2 standard deviations over the control’s group mean score. We used the informant version, because it is more reliable than the patient version in subjects with cognitive decline [32].
Depression was self-rated by the participants using the Geriatric Depression Scale (GDS) that consist in 15 YES/NO answer questions. Higher scores indicate higher levels of depression, scores over five indicate significant depressive symptoms [33].
Statistical analyses
The Statistical Package for the Social Sciences (SPSS) version 20 for Windows (IBM Corp., Armonk, NY, USA) and R Project (R project Core Team) were used for statistical analysis. Comparisons between subjects at different CDR category were conducted using Chi-squared tests (contingency table) for the categorical variables, and ANCOVA for the continuous variables, using age and years of education as covariates. Differences with a p < 0.05 were considered significant.
Effect size was reported using Partial Eta Squared (η _ p2) or Cohen’s d, according to Cohen, effect sizes between 0.2 and 0.49 are considered small; those between 0.5 and 0.79, moderate; and those >0.8, large [34]. Finally, in order to predict the best determinants of ADL impairment at different CDR categories, multiple linear regression models were done including demographic, cognitive and NPS data. All variables used in regression models were standardized to Z scores, allowing comparison among them. For reducing the number of variables included in the model we developed two “cognitive” composite scores including those most important dimensions previously related with functional impairment [17, 35]: Episodic memory (FCSRT total recall score plus ACE-R memory score) and Executive functions (FAB total score, plus scores in perseverative errors and categories found of the WCST). In the same direction, because many subjects had >1 NPS, and some symptoms appear to co-occur more often than others, we reduced the dimensionality of NPI-Q. We first transform the test scores (in NPI-Q for each subscale) in to Z-score using controls’ mean and standard deviation, we further did a factor analysis; Principal Axis extraction method was used [36]. We determine the number of factors to extract using eigen value >1, assessing a fine grain solution [37]. Once factor analysis supported composite scores and NPI reduction, we evaluate internal consistency using Cronbach’s Alpha.
RESULTS
Demographics
Patients with AD were graduated as CDR = 0.5 n: 34, CDR = 1 n: 47 and CDR = 2 n: 11. Patients with AD were significantly older 74±7 than controls 71±6 (t = –2.47, p = 0.014), without differences in education (13±5 and 13±4) or gender proportion (58 and 67% of females, respectively) (Table 2).
Comparison of demographic, functional, cognitive, and behavioral data between CDR groups
ES, effect size; †Significantly larger than controls; ‡Significantly larger than CDR 0.5; §Significantly larger than CDR 1&2.
Activities of daily living
As expected, either global and subdomain functional impairment deteriorate across CDR categories, from CDR 0 to 0.5 and from 0.5 to 1 and 2. There were significant differences between the three CDR groups in the global T-ADLQ score (F = 93, p < 0.001,
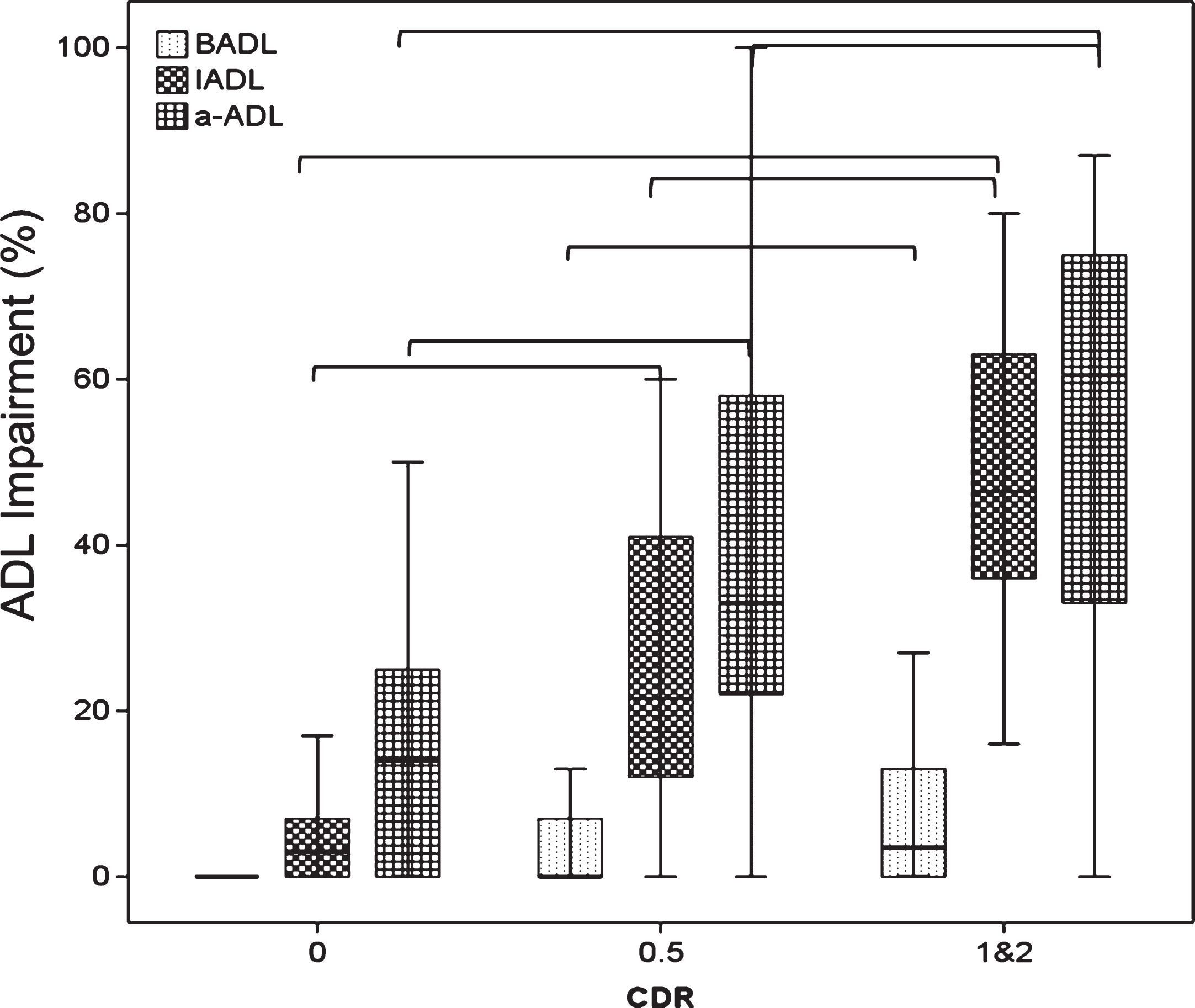
Comparison of impairment in each ADL subdomain between CDR groups. Brackets denotes significant differences between groups.
Cognitive performance
There were significant differences between the three cognitive groups in all cognitive evaluations (Table 2). The internal consistency of the cognitive composite scores was excellent for episodic memory (Cronbach’s Alpha = 0.92), and good for executive functions (Cronbach’s Alpha = 0.8).
Behavioral and psychological symptoms
Prevalence and severity of most of the NPS were higher in the AD group compared with the control group (Fig. 2; Table 2). The NPI-Q dimensionality reduction lead to the following subscales: Apathetic-depressive: which included the composite score of both symptoms (Cronbach’s Alpha = 0.78); Restless: which included the composite score of anxiety, irritability, agitation, aberrant motor behavior and night-time behavior disturbances, with (Cronbach’s Alpha = 0.8); and the Frontal-Psychotic: which included the composite score of delusions, hallucinations, euphoria and disinhibition (Cronbach’s Alpha: 0.76). Appetite and eating abnormalities did not load in any of the above-mentioned scales, reason why it was excluded. In the control group the changes observed in Frontal-Psychotic subscale were mainly due to disinhibition scores accounted by three subjects.

Proportion of neuropsychiatric symptoms across CDR groups.
Determinants of functional impairment
In a first exploratory analysis with the whole group; a model which explained 70.1% of the variance of the global ADL (T-ADLQ total score) was obtained (F(4,136) = 83.15; p < 2.2e-16, adjusted R2 = 0.701), That included: the Apathetic-depressive (β= 0.40, t = 5.98, p = 1.82e-08), the Frontal-Psychotic subscales (β= 0.17, t = 4.23, p = 4.14e-05), the memory (β= –0.41, t = 0.06, p = 3.18e-09) and the executive factor (β= –0.23, t = –2.97, p = 0.003). We further analyzed individual measures of apathy and depression, because both NPS has been reported to be related as important and independent NPS in AD [38, 39] (Fig. 3).

Correlation between global functionality and cognitive (A, B), behavioral subscales (C, D), and independent measures of apathy (E) and depression (F).
Determinants of functional impairment in each specific ADL subdomain in the different CDR categories
We found that regression models have different fits depending on the cognitive status and the subdomain of ADL; explaining between 32 to 65% of the variability of IADL, 26 to 55% of the variability of BADL and 20 to 47% for that of a-ADL. The regression models were better suited for determining the variability of functional impairment in AD patients than in the control group. We considered of “significant clinical relevance” only those models that explained ≥30% of functional impairment. The variables that better determines functionality in IADL in controls and in all ADL subdomains in the CDR 0.5 ADD patients were depression and apathy severity, and frontal Psychotic sub score. In the CDR 1&2 group the best determinants of functionality in BADL were global cognition, while memory impairment was for IADL impairment (Table 3).
Determinants of Impairment in ADL subdomains across CDR groups
Standardized coefficients are shown. *p < 0.05, **p < 0.01, ***p < 0.001.
DISCUSSION
The present study addressed a detailed analysis of the functional impairment in the different subdomains of ADL as well as their cognitive and neuropsychiatric determinants in a convenience sample of cognitively normal controls and ADD patients with different degree of dementia severity.
One of the principal novelties of our approach was the comprehensive assessment of ADL, separating ADL in three subdomains of different complexity including further: BADL, IADL, and a-ADL by using the T-ADQL scale [23]. First of all, we evaluated the proportion of functional impairment in every ADL subdomain across the different CDR categories, as expected our results showed that functional impairment worsens as the disease progresses and it is more pronounced in a-ADLs and IADLs (over 40%) than BADLs (6%) in both groups of ADD (Table 2, Fig. 1). The a-ADL impairment was significantly larger than the IADL at each CDR categories, confirming that a-ADL correspond to a subdomain of ADL that need to be differentiated from IADL. Importantly, a huge proportion of cognitively normal elders had a-ADL impairment reaching 17% ±17, which is quite similar to the 22±11% reported by De Vriendt with an specific a-ADL subscale [12]. The large variance in a-ADL, demonstrates the important variability in the performance in those more complex ADL in cognitively normal elders. These limitations may be due to multiple factors, like differences in sociocultural background, or motivational aspects [11] but also could be a prodromal sign of a dementia disorder [6].
One of our more interesting findings was the dissociation of the influence of NPS and CI on functional impairment at different CDR status, being the NPS the main determinants of IADL and a-ADL impairment in the CDR 0 and CDR 0.5 group, while in the mild to moderate severity ADD group (CDR 1 and 2), the main determinants of functional impairment in BADL and IADL were CI and secondly NPS. This dissociation have been previously reported by Rog (2014), where he found that for MCI, apathy/depression were the most important determinants for ADL impairment, while cognition was the best one in dementia by using the Ecog as the ADL scale [17]. These results are in line with recent studies that had questioned that the first clinical manifestation of AD is cognitive decline, instead proposed to be the NPS [14, 40] or even the a-ADL impairment [41, 42].
Regarding NPS we found that 93% of ADD patients and 39% of the control group had at least one behavioral symptom (by using the NPI-Q ≥1) (Fig. 2). Being the most frequent NPS in the ADD group: apathy (72%), depression (61%), and irritability (60%), while in the controls were: Nighttime Disturbances (20%), apathy (14%), and irritability (14%) (Fig. 2). These prevalences are quite similar to those reported in other studies using the NPI or NPI-Q [16, 43–46]. Because we used the NPI-Q instead the NPI, we could only measure the presence and severity of NPS, but not their frequency, nevertheless both scales had a high correlation (r = 0.7 to 0.9) [29, 30]. We further reduced the NPS into less variables by conducting a factor analysis, yielding into three NPS subscales: apathy/depression, restless/agitation, and mixed frontal/psychotic scales (Fig. 2); these subscales are quite similar to NPI-Q subscales reported in previous publications including large sample cohorts [47–49].
The three subscales of NPS showed different association with functional impairment across the CDR status. Apathy/depressive and frontal-psychotic subscales were very important in controls and CDR 0.5, while the restless subscale had a major role in functional impairment only for the CDR 1&2 group. Apathy and depression are the most prevalent NPS in AD, and as in our cohort, they have been reported to coexist in about 32% of AD patients [50], but also have been reported as independent NPS in controls and AD patients [38, 39] thus we further analyzed both symptoms separately (Fig. 3, Tables 2 and 3).
Our results are consistent with previous investigations that have reported that the presence, number, and severity of NPS are associated with CI and functional impairment in cognitively normal elders and across ADD continuum [43–45, 52]. Longitudinal studies suggested that NPS increases the risk of functional impairment, cognitive decline and disability [17, 53–59], specifically apathy is associated with an approximately 2-fold increased risk of dementia in memory clinic patients [60]. Nevertheless, there is an important heterogeneity in the association between functional impairment and specific/s NPS/s. This could be explained by factors related to the methodology to assess NPS (individual NPS versus clustering) and/or in the type of population studied [48].
However, apathy have been found as one of the most important NPS related with functional impairment [61], in dementia [17, 63], and even in non-demented elders [17, 60]. Apathy, widely defined as a marked loss of motivation [64], is the most prevalent neuropsychiatric symptom in neurologic pathologies and in AD [15, 65]. In our study apathy symptoms were one of the most prevalent in ADD and controls, present in 72% of ADD subjects, being severe (AESi >37) in more than 60% of them, which is similar to the previously reported prevalences [61]. In contrast to depression, it increased significantly as dementia progressed (Table 2, Fig. 2) [38]. The main novelty of our results was that the contributions of apathy to functional impairment differ according to the ADL subdomain and the stage of dementia. Apathy severity was the main determinant for those more complex ADL: IADL and a-ADL, and the second most important for BADL impairment in the CDR 0.5 patients for which our model predicted more than 50% of the functional impairment variability. For cognitively normal controls apathy also had an important role in IADL limitations. Our results are in line with the goal directed behavior model, that postulates that behavior is the result of a coordinate motivational, cognitive, and motor process [66, 67]. Based on this model, the new international consensus criteria of apathy defined apathy as “a quantitative reduction of goal-directed activity in comparison to the patient’s previous level of functioning” [68]. Our results suggest that apathy and ADL impairment are both manifestations of a quantitative reduction of self-generated voluntary and purposeful behaviors [66].
Dysfunction in neuroanatomical networks related with IADL impairment and apathy in ADD are very similar, being associated with hypometabolism and volume loss in the anterior cingulate, frontal [69, 70], parietal [69–72], and temporal areas [69, 72]. Moreover, the severity of functional impairment [72], and apathy [73] have been correlated with increased AD biomarkers indicating that both could be manifestations of neurodegeneration in AD patients.
Depressive symptoms were also associated with impairment in all subdomains of ADL, with a more important role in controls and CDR 0.5, even surpassing the importance of apathy in the association with a-ADL in the controls, the BADL in the CDR 0.5, and IADL in the CDR 1&2. Results that are in accordance with the fact that depression is one of the main causes of disability at all ages according to the World Health Organization data. Nevertheless, the contribution of depression as a determinant of disability in the CDR 1&2 ADD patients could be under estimated compared to controls and CDR 0.5, because depression was measured with a self-rated scale, which could be less reliable in subjects with more severe cognitive impairment (Fig. 3) [32].
Concerning the association between cognitive impairment and functional impairment, in the CDR 1&2 group, global cognition was an important determinant only for BADL impairment, while memory and executive functions subscores had an important role in more complex ADL impairment: IADL and a-ADL at every stage of AD. The association with unspecific and simple measures of cognition had been traditionally been related with ADL [74], while memory and executive functioning are usually associated with IADL and are predictive of future decline in IADL [35, 75]. One possible explanation why episodic memory plays an important role in IADL is that our ability to fulfil future more complex actions is strongly dependent on episodic memory [35]. Regarding executive dysfunction, planning, sequencing capacity, and monitoring are prerequisites for successful IADL performance [74].
Finally, the main limitation of our study was that the assessment of functional impairment and NPS were done by informant-based questionnaires, which are susceptible to reporter biases [76].
Other limitations are the small sample size of elderly without cognitive impairment, and the recruitment method of the participants. Further population-based studies are required to explore the meaning of complex functional impairment and their main determinants.
In conclusion, the determinants of functional impairment vary according to the severity of ADD and the subdomain of functional impairment. NPS, mainly apathy, are the most important determinants of that more complex ADL impairment: IADL and a-ADL in the CDR 0.5 and cognitively normal controls. Conversely, for the CDR 1&2 group, cognitive impairment was the most relevant determinant in BADL impairment. Our study contributes to clarify the association between NPS and cognitive decline with complex and basic ADL impairment in normal elderly and AD patients, information needed for planning prevention and management of dependence in the elderly.