
Abstract
Background:
There is a conflicting literature on the association between the use of antihyperglycemic drugs and dementia risk.
Objective:
The goal of this case-control study was to analyze the association between the use of antihyperglycemic drugs and dementia risk in patients followed in general practices in Germany.
Methods:
This study included patients with type 2 diabetes mellitus who had received a first dementia diagnosis in 972 general practices in Germany between January 2013 and December 2017 (index date). Controls without dementia were matched (1:1) to cases by age, gender, index year, and physician. Two multivariate regression models were used to study the association between the use of antihyperglycemic drugs and dementia risk. Model 1 included all antihyperglycemic drugs prescribed to patients regardless of the prescription duration, whereas Model 2 only included the longest therapy prescribed to each patient.
Results:
There were 8,276 diabetes patients with dementia and 8,276 diabetes patients without dementia included in this study. In Model 1, glitazones were associated with a decreased dementia risk (odds ratio [OR] = 0.80), whereas insulin was associated with an increased risk of developing the condition (OR = 1.34). In Model 2, metformin, prescribed as monotherapy (OR = 0.71) or as dual therapy with sulfonylureas (OR = 0.90), was associated with a decrease in the likelihood of subsequently being diagnosed with dementia. By contrast, the combination of basal insulin and bolus insulin (OR = 1.47) and premix insulin (OR = 1.33) were risk factors for dementia.
Conclusion:
Metformin and glitazones were negatively associated with dementia, while insulin was positively associated with dementia.
INTRODUCTION
Dementia is a chronic condition that affects 5–7% of people aged≥60 years worldwide [1]. The number of individuals living with dementia is expected to reach approximately 66 million in 2030 and 115 million in 2050. In Germany, more than 1.5 million people suffer from dementia, and the costs associated with this disorder are considerable [2–4]. Therefore, there is a need to better identify patients who are at a particular risk of developing dementia in this country.
A 2013 meta-analysis of prospective observational studies (n = 28) showed that diabetes is positively associated with all-type dementia, Alzheimer’s disease, and vascular dementia [5]. Although its exact mechanisms of action remain poorly understood, the effects of diabetes on cognition are likely mediated by hyperglycemia, decreased insulin secretion, obesity, increased oxidative stress, and inflammation [6]. Thus, treating people affected by diabetes may help reduce their risk of subsequently being diagnosed with dementia. However, there is a conflicting literature on the association between the use of antihyperglycemic drugs and dementia risk [7–15]. Several studies have suggested that these drugs have a protective effect [7, 15], whereas others have found that they have no significant impact on dementia risk [8, 12] or that they themselves are risk factors [8–10].
Therefore, the goal of this case-control study was to analyze the association between the use of antihyperglycemic drugs and dementia risk in patients followed in general practices in Germany.
METHODS
Database
The present retrospective study was based on the nationwide Disease Analyzer database (IQVIA). This database contains demographic, clinical, and pharmaceutical variables anonymously obtained by IQVIA from a nationwide sample of general and specialist practices [16]. The quality of these data is assessed on a regular basis, and it has been shown that the Disease Analyzer database is representative of German practices [16]. Finally, several studies focusing on antihyperglycemic drugs [17] and dementia [18] have already been conducted using this database.
Study population
This study included patients with type 2 diabetes mellitus (International Classification of Diseases, 10th revision [ICD-10]: E11) who had received a first dementia diagnosis (ICD-10: F01, F03, G30) between January 2013 and December 2017 (index date) in 972 general practices in Germany. The inclusion criteria were as follows: 1) observation of at least 365 days prior to the index date; 2) at least one prescription for antihyperglycemic drugs within 365 days prior to the index date; 3) documentation of at least one hemoglobin A1c level (HbA1c); and 4) age≥60 years at index date. After applying similar inclusion criteria, controls without dementia were matched (1:1) to cases by age, gender, index year, and physician. The index date for the controls was a randomly selected visit date between January 2013 and December 2017 (Fig. 1).
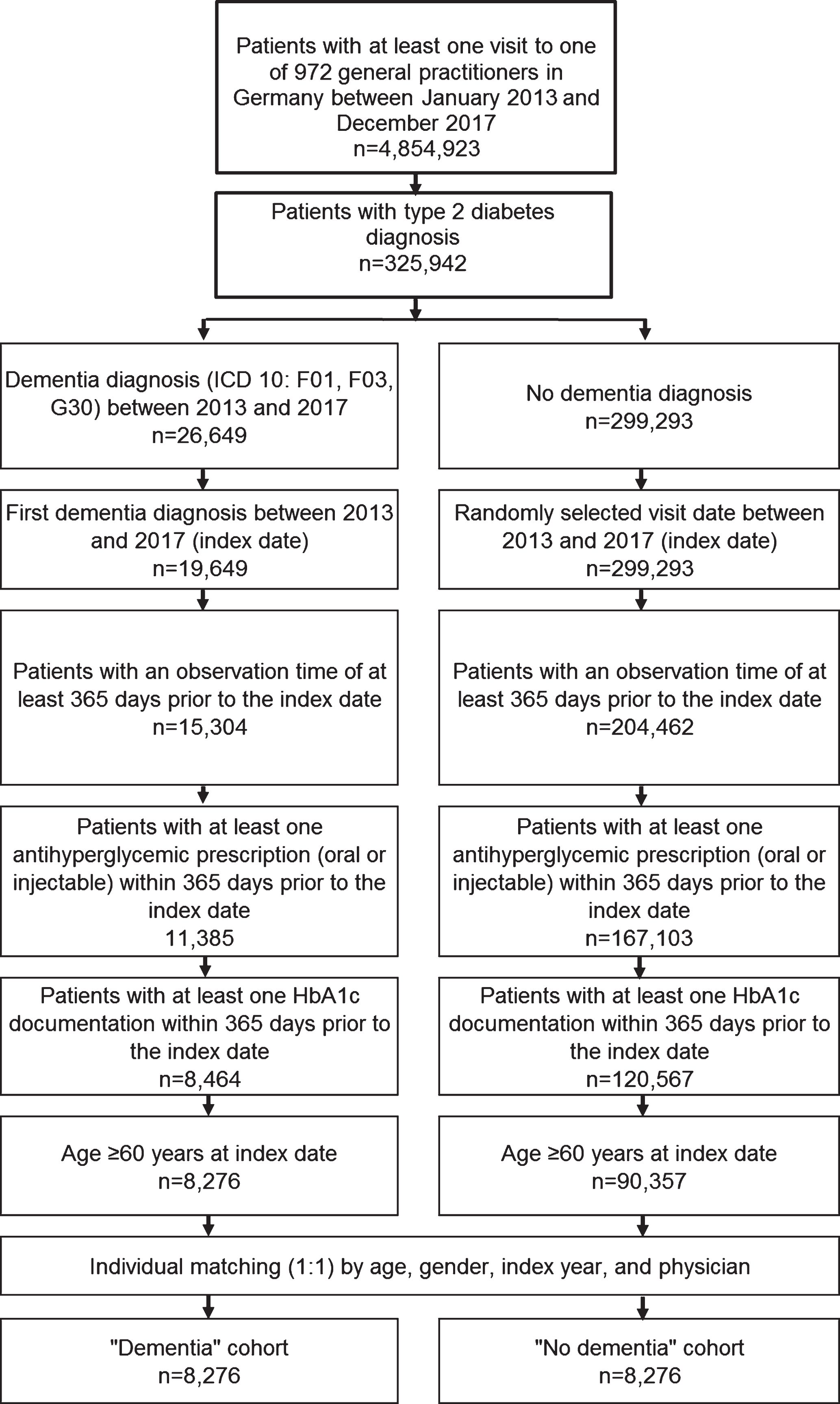
Selection of study patients.
Study variables
Demographic variables included age, gender, and index year. Clinical variables included HbA1c levels prior to the index date, diabetes duration, disorders diagnosed within 365 days prior to the index date (hypertension [I10], hyperlipidemia [E78], coronary heart disease [I24, I25], stroke including transient ischemic attack [TIA; I63, I64, G45], depression [F32, F33], intracranial injury [S06], mental and behavioral disorders due to use of alcohol [F10], mild cognitive impairment [F06.7], and severe hypoglycemia [E16.2]), and drugs prescribed within 365 days prior to the index date (antihypertensive drugs [Anatomical Therapeutic Chemical [[ATC]] by European Pharmaceutical Market Research Association [[EphMRA]]: C03, C07, C08, C09], lipid lowering drugs [C10], antidepressants [N06A], and proton pump inhibitors [A02B2]). These disorders and drugs were included because they had previously been identified as either protective factors or risk factors for dementia [18–23]. Antihyperglycemic drugs included metformin (A10J), sulfonylureas (A10H), dipeptidyl peptidase-4 (DPP-4) inhibitors (A10N), glucagon-like peptide-1 (GLP-1) receptor agonists (A10S), sodium-glucose co-transporter-2 (SGLT-2) inhibitors (A10P), glitazones (A10K), and insulin (basal insulin [A10C2], bolus insulin [A10C1], and premix insulin [A10C3]).
Statistical analyses
Descriptive analyses were carried out for all basic characteristics and mean±SD was calculated for age. Two multivariate regression models were used to study the association between receiving antihyperglycemic drugs and the risk of developing dementia. Model 1 included all antihyperglycemic drugs prescribed to patients regardless of the prescription duration (e.g., one month, one year, or five years). In this model, the reference group for each antihyperglycemic treatment (e.g., metformin) was the absence of a prescription of this treatment (e.g., no metformin). Model 2 only included the longest therapy prescribed to each patient. For example, if one individual was prescribed metformin for one month and insulin for a period of five years, only insulin was included in the subsequent analyses. In this model, each antihyperglycemic therapy of interest was compared to all other antihyperglycemic therapies. Both models were adjusted for mean HbA1c value prior to the index date, diabetes duration, co-diagnoses, and co-therapies. A p-value of <0.05 was considered statistically significant. All analyses were carried out using SAS 9.4 (SAS Institute, Cary, USA).
RESULTS
This study included 8,276 diabetes patients with dementia and 8,276 diabetes patients without dementia. The mean age of study participants was 79.7 years (SD = 6.9 years), and 56.2% of patients were women (Table 1). The most frequent comorbidity in the year prior to the index date was hypertension (cases: 89.0%; controls: 91.1%), while the most commonly prescribed treatments were antihypertensive drugs (94.8% and 92.4% respectively). The results of the first multivariate logistic regression model are displayed in Table 2. Glitazones were associated with a decreased risk of developing dementia (odds ratio [OR] = 0.80; 95% confidence interval [CI]: 0.68–0.95), whereas insulin was associated with an increased dementia risk (OR = 1.34; 95% CI: 1.24–1.44). Among the different types of insulin, both basal insulin (OR = 1.18; 95% CI: 1.07–1.29) and premix insulins (OR = 1.31; 95% CI: 1.19–1.44) were risk factors for the diagnosis of dementia. HbA1c levels between 7.5% and 8.4% (OR = 1.14; 95% CI: 1.03–1.26) and higher or equal to 8.5% (OR = 1.39; 95% CI: 1.22–1.59) were additional risk factors for the subsequent diagnosis of dementia. Table 3 shows the results of the second multivariate logistic regression model. Metformin prescribed as monotherapy (OR = 0.71; 95% CI: 0.66–0.76) or as dual therapy with sulfonylureas (OR = 0.90; 95% CI: 0.89–0.92) was associated with a decreased risk of being affected by dementia. By contrast, the combination of basal insulin and bolus insulin (OR = 1.47; 95% CI: 1.32–1.63) and premix insulin (OR = 1.33; 95% CI: 1.14–1.56) were risk factors for dementia. Finally, there was a positive association between HbA1c levels and dementia (7.5–8.4% : OR = 1.20, and 95% CI: 1.09–1.32;≥8.5% : OR = 1.55, and 95% CI: 1.37–1.76).
Basic characteristics of study patients after (1:1) matching by age, sex, index year, and physician
Association between the use of antihyperglycemic drugs and dementia in type 2 diabetes patients followed in 972 general practices [Model 1: ever use versus never use]
*Multivariate logistic regression, adjusted for mean HbA1c value prior to the index date, diabetes duration, co-diagnoses, and co-therapies.
Association between the use of antihyperglycemic drugs and dementia in type 2 diabetes patients followed in 972 general practices [Model 2: longest therapy class/combination prior to index date]
*Only therapies with a prevalence of at least 3% are displayed. **Multivariate logistic regression, adjusted for mean HbA1c value prior to the index date, diabetes duration, co-diagnoses, and co-therapies.
DISCUSSION
This retrospective study, including more than 16,500 patients with type 2 diabetes mellitus, found that dementia was negatively associated with metformin and glitazone use and positively associated with insulin use. Moreover, people with high HbA1c levels were more likely to be diagnosed with dementia than those with low HbA1c levels.
The first major finding of this study is that metformin use was negatively associated with dementia. Several studies in the past decade have focused on the association between the use of metformin and dementia risk. In 2011, Hsu and colleagues showed in 127,209 participants that type 2 diabetes with (hazard ratio [HR] = 1.62) or without (HR = 2.41) oral agents was a risk factor for dementia [7]. When restricting the analysis to people with diabetes, metformin (HR = 0.76), sulfonylureas (HR = 0.85), and a combination of metformin and sulfonylureas (HR = 0.65) decreased the risk of developing dementia. More recently, in a 2017 study of 17,200 new metformin users and 11,440 new users of sulfonylureas, Orkaby et al. reported that the risk of developing dementia was significantly lower in patients who received metformin than in those who received sulfonylureas (HR = 0.67–0.78) [14]. This finding was corroborated by using an adjusted regression model in veterans under the age of 75 (HR = 0.89). In line with these results, we found that the use of metformin as monotherapy or as dual therapy with sulfonylureas was associated with a significant decrease in the subsequent risk of developing dementia. Taken together, these findings support the hypothesis that metformin is a neuroprotective molecule. Interestingly, a recent study conducted in diabetic mice reported that neuroinflammation and the loss of hippocampal neurons decrease in the presence of metformin and that the use of this antihyperglycemic drug leads to improvements in spatial memory [24].
There was also a negative association between the prescription of glitazones and dementia. In 2015, Heneka and colleagues observed in a prospective cohort study including 145,928 subjects aged≥60 years that dementia incidence was reduced by long-term use of pioglitazone [11]. In addition, they found a negative association between the use of pioglitazone and dementia risk in initially non-insulin-dependent diabetes mellitus patients (relative risk [RR] = 0.53). This risk was comparable to that of people without diabetes in the group of people who received the drug for less than eight calendar quarters. Later, in 2018, researchers from Taiwan estimated in 204,323 individuals with type 2 diabetes that the risk of developing dementia was significantly lower in participants aged≥65 years on metformin + pioglitazone than in those on metformin + sulfonylurea (HR = 0.56) [15]. It also tended to be lower than in those on other metformin-based dual therapies. Moreover, the likelihood of being diagnosed with dementia was reduced in people aged≥18 years receiving pioglitazone compared to those receiving other second-line glucose-lowering drugs. Glitazones belong to the family of peroxisome proliferator-activated receptor gamma (PPAR-γ) agonists, drugs known to prevent the neuropathological and behavioral changes brought about by Alzheimer’s disease and other dementias [15, 25]. Of particular interest is the fact that PPAR-γ, a molecule expressed in the brain, inhibits the secretion of proinflammatory molecules, promotes mitochondrial biogenesis, and reduces amyloid-β generation [26].
Another important finding of this retrospective study is that insulin use was a risk factor for developing dementia. Since opposite results have been obtained in the past, this finding must be interpreted with great caution. For example, in 2012, Imfeld et al. showed in a case-control study including 7,086 individuals aged 65 and older that there was no significant association between the prescription of insulin and the risk of developing Alzheimer’s disease (adjusted OR = 1.01; 95% CI: 0.58–1.73) [8]. Two years later, Cukierman-Yaffe and colleagues reported regarding a relatively young cohort of individuals with dysglycemia that insulin and omega-3 fatty acids did not have a significant impact on the rate of change of cognitive test scores and on the incidence of probable cognitive impairment [27]. Probably, the impact of insulin on Alzheimer’s disease and other dementias may be mediated by hypoglycemia. In 2013, Yaffe et al. showed in 783 older adults with diabetes mellitus that hypoglycemia was associated with a twofold increase in the subsequent risk of developing dementia (HR = 2.1) [21], with hypoglycemia contributing to dementia via brain damage [28] or loss of ionic homeostasis [29]. In 2016, Khunti and colleagues showed in a study including 27,585 people from 24 countries that 46.5% of type 2 diabetes patients treated with insulin reported hypoglycemia [30]. As the prevalence of hypoglycemia is underestimated in the database used, the mediating role played by hypoglycemia in the relationship between antihyperglycemic drugs and dementia can only be assumed.
Finally, there was a positive relationship between HbA1c levels and dementia risk. In 2015, Ramirez and colleagues observed in 1,342 elderly individuals followed in primary care practices that HbA1c levels≥7% significantly increased the risk of developing all-cause dementia (OR = 5.08) or Alzheimer’s disease (OR = 4.68) [31]. More recently, in 2017, researchers from the U.S. estimated in 8,888 participants aged≥50 that a one-unit increase in HbA1C corresponded to a 0.05 SD decrease in memory score per decade [32]. Moreover, in 2018, Zheng and colleagues showed that a 1 mmol/mol increment in HbA1c was significantly associated with an increased rate of decline in global cognitive scores, memory scores and executive function scores [33]. Taken together, these findings clearly underline the major role played by HbA1c levels and chronic hyperglycemia in the association between diabetes and cognitive decline/dementia.
Although these results are of great interest, the present study is subject to several limitations that should be mentioned at this point. Firstly, since we only included patients followed by general practitioners, and since a high number of patients may have been followed by neurologists only, the findings of this study may have been biased. Secondly, there was no information about compliance, adherence, and persistence with antihyperglycemic drugs, although these factors may have affected the subsequent risk of developing dementia. Thirdly, since we had no data regarding diabetes severity (e.g., renal or ocular complications), it is possible that differences in severity have biased our analyses. The strengths of this work are the number of patients and general practices available for analysis and the use of real-world data pertaining to diagnoses in primary care practices where diagnoses are continuously documented, allowing for unbiased exposure assessment (no recall bias).
Metformin and glitazone use were negatively associated with dementia risk, while insulin use was positively associated with dementia risk. High HbA1c levels were an additional risk factor for the development of this neurological condition. Further longitudinal studies are warranted to gain a better understanding of the relationship between the prescription of antihyperglycemic drugs and dementia.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/18-0808r1).