
Abstract
Background:
Dementia with Lewy bodies (DLB) is the second most common degenerative dementia in older people. However, rates of misdiagnosis are high, and little is known of its natural history and outcomes. Very few previous studies have been able to access routine clinical information for large, unbiased DLB cohorts in order to establish initial presentation, neuropsychological profile, and mortality.
Objective:
To examine in detail, symptom patterns at presentation and their association with outcomes, including mortality, in a large naturalistic DLB cohort from a secondary care sample.
Methods:
A retrospective cohort design was used to identify a DLB cohort (n = 251) from Cambridgeshire and Peterborough NHS Foundation Trust (CPFT). Information relating to first consultation, diagnosis, and DLB diagnostic features were extracted.
Results:
A wide range of presenting complaints and differential initial diagnoses were identified for the cohort. Along with memory loss (27.1%) and hallucinations (25.4%), low mood (25.1%) was noted as a key presenting complaint among the DLB cohort. Rates of REM sleep disorder were considerably lower (8.4%) than would be expected. Deficits in non-amnestic cognitive domains were associated with reduced mortality compared with amnestic-only presentations.
Conclusion:
Individuals later diagnosed with DLB present initially to secondary care with a wide range of symptoms and complaints, some of which are not immediately suggestive of a DLB diagnosis. More examinations of large cohorts such as this are needed to further elucidate the complex presentation and clinical course of DLB, and to confirm whether amnestic-only presentation confers a worse outcome.
Keywords
INTRODUCTION
Despite reports that Dementia with Lewy bodies (DLB) is the second most common type of degenerative dementia and accounts for 4-7% of dementia cases seen in secondary care [1, 2], DLB is still largely under-diagnosed. There are several factors that likely contribute to the under-diagnosis of DLB, including relative lack of awareness of clinicians of some of the diagnostic features, failure to ask about these during patient assessment, and a lack of appreciation of the many and varied ways in which DLB can present [3]. The recently published fourth consensus report of the DLB Consortium revised and broadened the clinical features required for probable and possible DLB [4], increasing the number of key DLB feature to four by adding REM sleep behavior disorder (RBD) to fluctuating cognition, recurrent visual hallucinations, and spontaneous Parkinsonism. The Consortium also highlighted the importance of a number of supportive features that can aid with clinical decision making for diagnosing probable and possible DLB, such as repeated falls, urinary incontinence, anxiety, and depression [4].
Previous research has shown that as well as greater mortality and poorer outcomes [5–9], DLB also has a distinct neuropsychological profile compared to AD, despite the overlap in symptom profiles. It has been acknowledged that DLB patients can have more complex clinical presentations due to symptoms such as visual hallucinations and sleep disorders. In an assessment of one of the largest published DLB cohorts (n = 634), Fereshtehnejad and colleagues [10] found higher occurrences of depression, stroke, and migraine in the DLB compared to an AD cohort (n = 9161). Such large-scale assessments of DLB cohorts utilizing large scale population-level data sources are rare. Much has been published tracking and characterizing the clinical progression of dementia and AD over time [11–13]. However, similar in-depth examinations of DLB cohorts with large sample size, multiple follow-ups, or pooling different sources of clinical information are difficult to find.
More examples like that of Fereshtehnejad et al. [10] are required in order to examine the naturalistic presentation and progression of DLB. By including information relating to various risk factors, symptoms, and comorbidities from an unbiased DLB cohort (e.g., those not selected for a research study), we can examine in detail the early presentation of DLB, its progression, and the underlying mechanisms that impact outcomes. The development of electronic clinical records and the technology that makes structured and open-text clinical records searchable and anonymous, such as the Clinical Record Interactive Search (CRIS) [14] and Clinical Records Anonymisation and Text Extraction (CRATE) [15] systems, provides potential for creating large, research databases for unbiased disease cohorts. Previous studies have shown how these research databases can then be utilized to examine mortality rates across dementia sub-groups [6], specific predictors for mortality and cause of death [16], care home and hospital admissions and their costs [17–19], and disease progression [20].
The aim of the study was to identify a retrospective naturalistic cohort of individuals with a diagnosis of DLB from a secondary care sample. We have previously published a survival analysis examining the difference in mortality rates for this same DLB cohort with a comparator group of individuals with AD [6], finding a significantly increased mortality in the DLB group. Here, we present a much more detailed examination of the DLB cohort (n = 251) in terms of their symptoms at presentation, neuropsychological profile and associations between these and mortality.
METHODS
Design and cohort identification
Using a retrospective cohort design, we identified the cohort through anonymized, electronic clinical records of Cambridgeshire and Peterborough NHS Foundation Trust (CPFT), a representative NHS Trust in the UK. A detailed description of the population, sample and case identification for the current cohort has been described previously [6]. To summarize, all patients with electronic clinical records in CPFT between 2005 and 2012 (inclusive; study period and in line with protocol) were searched using key word and acronym searches based on DLB (e.g., ‘Lewy’, ‘LBD’, ‘DLB’) in order to identify possible cases. The searches resulted in 983 possible unique cases. A manual search by two experienced clinicians, with knowledge of diagnostic criteria and symptom presentation in dementia, of the 983 cases returned 304 with a diagnosis of DLB. These were further reduced to 251 cases who had been given a new diagnosis of DLB between 2005 and 2012. Cases where the DLB diagnosis had been given by a CPFT clinician and it was the most recently recorded diagnosis in the patient record were included in the cohort. Diagnoses were given by consultant psychiatrists either directly or in the course of supervising a junior colleague. Any diagnosis given in the general hospital by a band of clinical nurse specialists would have been discussed and agreed by a psychiatrist within the team.
Variables
Information relating to demographics, clinical features, medication use, and clinical course (e.g., dates) were extracted from the structured and free text clinical records. Further detail is provided in Price et al. [6]. For the current investigation, the focus was on the identified DLB cohort in terms of their earliest presentation and the presence of DLB features. For the current DLB cohort, date of birth, sex, and date of death was extracted through structured query language (SQL) searches. All other information was extracted from the structured and free-text clinical records using manual searches.
In terms of timing and clinical course, the date of first consultation (with a clinician) where cognitive impairment was recorded as a problem and the date of DLB diagnosis (by a clinician) by month and year were both extracted from the clinical records. Three groups were identified within the cohort according to when they received their DLB diagnosis: 1) those who presented with cognitive impairment and were diagnosed with DLB on the same date; 2) those who presented with cognitive impairment and who were diagnosed with DLB at a later date with no other explanatory diagnosis given in between; and 3) those who presented with cognitive impairment and where given a diagnosis on the same date that was later changed to DLB. The amount of time between first presentation with cognitive impairment and DLB diagnosis was calculated for groups two and three. Furthermore, information pertaining to the individuals’ presenting complaints that had been noted by the examining clinician when the individual was first seen within CPFT was extracted.
Extensive manual searches were completed by the two experienced clinicians to identify the presence of validated diagnostic DLB features for each individual, present at any stage within their clinical records. These fell into two broad categories: key and supportive. The key features were based on established DLB symptoms in line with the revised criteria for a clinical diagnosis of DLB [4]: amnestic cognitive impairment (e.g., signs of memory loss or impairment), non-amnestic cognitive impairment (e.g., progressive deterioration in attention, visuospatial and/or executive function), fluctuating cognition (e.g., attention, alertness), visual hallucinations, Parkinsonian features (e.g., tremor at rest, Bradykinesia, rigidity, loss of postural reflexes), and RBD. Supportive features included other symptoms that might be associated with DLB (e.g., non-visual hallucinations, depression, repeated falls). The identification of these key and supportive DLB features was completed by the two clinicians experienced in diagnostic criteria and symptom presentation of dementia. In line with the protocol (developed in accordance with the validated diagnostic criteria for DLB), the two experienced dementia clinicians examined the clinical records of each DLB case, which included assessment/diagnostic documents, progress notes, and clinical correspondence from the examining clinicians, for the presence/absence of each key and supportive DLB feature.
Cognitive status was measured using the Mini-Mental State Examination (MMSE). Scores closest to the dates of first consultation where cognitive impairment was noted and DLB diagnosis were extracted.
Physical comorbidity was measured using the Charlson comorbidity index [21]. Calculation methods have been described previously [6]. Individuals were grouped into low (≤2) or high (>2) comorbidity by splitting at the median (2).
As the study was concerned with individuals with a DLB diagnosis between 2005 and 2012 (inclusive), mortality data (e.g., month and year of death) were extracted up until May 2015 (in line with protocol [6]) from automatic updates of the source clinical records from the NHS Spine [22].
Statistical methods
For DLB key and supportive features, counts and percentages were derived. χ2 tests were completed on three key DLB features (visual hallucinations, Parkinsonian features, and RBD) to examine if the rates of these features among the current DLB cohort were different from those that would be expected from rates reported in previous research. These particular three symptoms were chosen as, unlike for fluctuation, it was possible to calculate expected rates from previous published and well-established prevalence rates from large DLB cohorts [4, 23]. Definitions of fluctuation among previous research have varied, including features from cognitive, attentional and/or arousal domains, making it difficult to establish a common prevalence rate [4, 23].
Dates of first consultation and of first recorded DLB diagnosis were manually extracted from the clinical records. Along with those dates, we extracted the contemporaneous MMSE scores where present (e.g., scores closest to first consultation and diagnosis dates). Mean MMSE scores were calculated for the whole cohort. For those who did not received a diagnosis of DLB at their first consultation, the length of time between first consultation and DLB diagnosis was calculated. Furthermore, for these individuals with a time difference, paired t tests were completed to examine changes in MMSE scores from first consultation to diagnosis.
Cox proportional hazard models were used to assess mortality, with R v.3.3.3 and the ‘survival’ (v.2.42.3) and ‘survminer’ (v.0.4.2) packages. The individual’s start date was the date of first consultation where cognitive impairment was recorded, and the end date was date of death or the study end point (1st May 2015; according to CRATE anonymisation procedures all dates are anonymised to the first of the month). If the date of first consultation was unknown (e.g., missing from clinical records), the date of diagnosis was used instead. Initial models were conducted to assess whether the presence or not of all key features affected mortality for the DLB cohort (amnestic cognitive impairments, non-amnestic cognitive impairments, fluctuating cognition, visual hallucinations, Parkinsonian features, and RBD). Given the results of the above models, we also completed additional analyses examining mortality based on the presence of non-amnestic cognitive impairments for the cohort. Models accounting for age, sex, comorbidity, and MMSE score at diagnosis were used. Based on model fitting and assumption checks, a model including age, sex, comorbidity, and the presence (or not) of non-amnestic cognitive impairments was determined as the best fit. Similar models including interactions either demonstrated no interaction effects or were found to have problems with model fit. Data are displayed using survival (Kaplan-Meier) plots.
RESULTS
We have previously published detailed descriptions of the cohort demographic information [6]. In brief, the cohort comprised 129 women (51.4%) and 122 men. The average age at first presentation was 78.8 years (SD = 7.7) and 79.3 years (SD = 7.6) at DLB diagnosis.
Initial diagnosis
Fifty subjects (19.9%; group three as outlined in the Methods) later diagnosed with DLB had received a different initial diagnosis. The majority of these other diagnoses were other forms of dementia, in particular AD (n = 14, 28%, see Table 1). No significant differences were found between the groups in their age at diagnosis, age at death, and MMSE scores at first consultation and diagnosis. The occurrence of key DLB features was also similar across the groups (see Table 2).
Numbers and percentages for initial diagnoses among the cohort
Demographic and clinical details comparing those who received a DLB diagnosis at first consultation (group one and two) and those who did not (groups three).
*Present in clinical records. Significance codes: * p <0.05, ** p <0.01, *** p <0.001.
Earliest reported presenting complaint
Within the first consultation, it was noted that clinicians identified up to three presenting complaints for each individual within the cohort (n = 251): 118 individuals (47.4% of the whole cohort) had one, 105 individuals (42.2%) had two, and 24 individuals (9.7%) had three presenting complaints (see Table 3). Of all the presenting complaints (n = 490), it was noted that memory loss, hallucinations and low mood were the most common with rates of approximately a quarter each (27.1%, 25.3%, and 25.1% of all presenting complaints, respectively).
Numbers and percentages for earliest presenting complaints (n = 490)
Time between first consultation and DLB diagnosis
Over half the cohort were found to have presented for the first time and received a DLB diagnosis on the same date (group one as outlined in the Methods). For those with a time difference between these dates (n = 120, 47.8%), the mean time was 53.6 weeks (SD = 53.4).
Cognitive scores at first consultation and DLB diagnosis
Among the 120 individuals who had a time difference between their first consultation and DLB diagnosis (groups two and three as outlined in the Methods), MMSE scores were present at both time points for 69 (27.5% of the whole cohort). For these individuals, the mean time between first consultation and receiving a DLB diagnosis was 48.0 weeks (SD = 44.5 weeks). Furthermore, there was a significant decrease in MMSE scores from first consultation (M = 22.8, SD = 4.4) to diagnosis (M = 20.3, SD = 5.6), t (68) = 3.91, p <0.001.
Key and supportive DLB features
Within Table 4, we have presented an overview of DLB features identified by the researchers within the cohorts’ clinical records from their first presentation to death/end of the study period. A χ2 test found that the current DLB cohort had a similar rate of visual hallucinations as would be expected from previously reported rates (observed rate = 70.5%, expected rate = 75.0% [4, 21]; χ21 = 2.35, p = 0.12). The rates of Parkinsonian features were slightly less than would be expected (observed rate = 63.0%, expected rate = 80.0% [4, 21]; χ21 = 44.1, p <0.001).
Presence of key and supportive DLB features among the cohort at any time. Multiple features could be present in one individual, including both amnestic and non-amnestic impairments
Note. Among key and supportive features, only one individual had missing data.
The current DLB cohort displayed significantly lower rates for RBD than would be expected from previously reported rates (observed rate = 8.4%, expected rate = 76.0% [4, 21]; χ21 = 626.34, p <0.001). The presence of supportive features for the DLB cohort was more varied compared to the key features described above. By far the most common feature was visuospatial disturbance, with nearly half the cohort having evidence of this feature within their record (49.4%). After this, repeated falls (31.5%) and depression (21.5%) were the most common supportive features.
Mortality based on key DLB features
The best model was selected through a stepwise comparison procedure. Hazard ratios, 95% confidence intervals, and p values from all models examined are presented in Table 5. We first examined a model (M1) assessing mortality based on the presence/absence of all key DLB features (amnestic cognitive impairment, non-amnestic cognitive impairment, fluctuating cognition, visual hallucinations, Parkinsonian features, and RBD), and controlling for relevant confounding variables (age, sex and comorbidity). The presence of non-amnestic cognitive impairment (HR = 0.57, Z = -3.43, p <0.001) was the only core diagnostic criterion found to predict mortality. As was expected, age at diagnosis (HR = 1.05, Z = 4.15, p <0.001) was also significant. Furthermore, the presence of Parkinsonian features (Z = 1.70, p = 0.09) approached significance as a predictor.
Cox proportional hazard models including models for all key features and those focused on the DLB non-amnestic cognitive impairments
Significance codes: * p <0.05, ** p <0.01, *** p <0.001; †Best fit model; Log rank test was between those who survived and those who died. LR, likelihood ratio; HR, hazard ratio; NA, not applicable; Note. It was not possible to run a LR test between M2 and M3 due to missing data.
Given the results of this first model, we then focused on the presence/absence of non-amnestic cognitive impairment among the cohort and assessed its influence on survival, along with a number of covariates. In a simple model assessing the difference in mortality between those who were reported as having non-amnestic cognitive impairments versus those who did not, there was a significant difference, χ2 (1, N = 250) = 10.8, p <0.05 (see Fig. 1). The median (raw) length of time to death for those who had non-amnestic cognitive impairments was 3.7 years (95% CI: 3.48–4.08) compared to 2.8 years (95% CI: 2.67–3.53) for those who did not. Further details about the two groups are presented in Table 6.
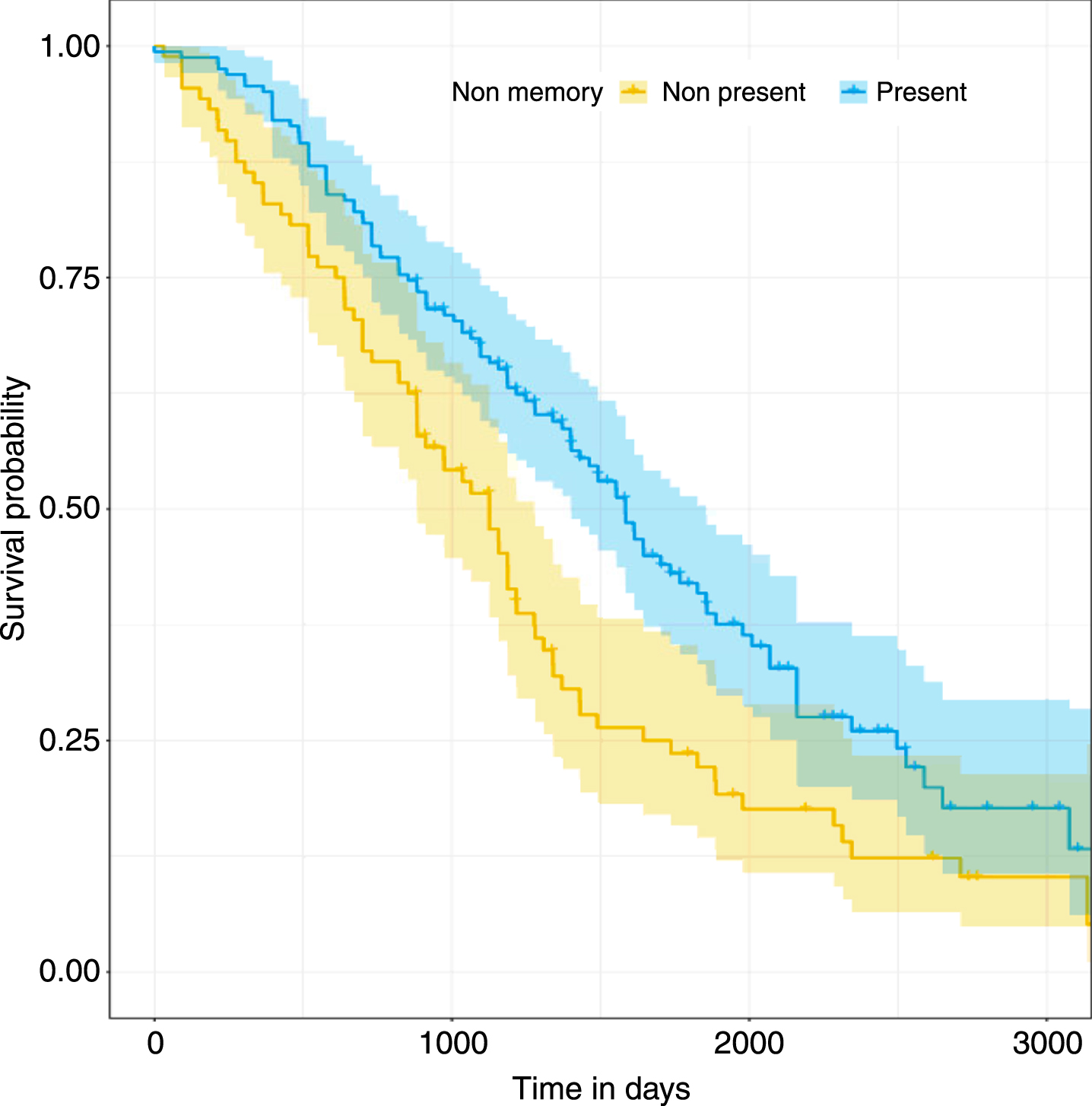
Mortality rates of individuals with DLB, with and without non-amnestic cognitive impairments.
Demographic and clinical details for those who had and did not have non-amnestic cognitive impairments
Significance codes: * p <0.05, ** p <0.01, *** p <0.001.
In a model (M2) whose predictors were age, sex, comorbidity, and the presence/absence of non-amnestic cognitive impairments on mortality, age (HR = 1.04, Z = 4.09, p <0.001) and non-amnestic cognitive impairments (HR = 0.57, Z = -3.57, p <0.001) were significant predictors of mortality. Sex approached significance, with a suggestion of women living longer (HR = 0.8, Z = -1.71, p = 0.09). We tested a similar model (M3) that included age, sex, comorbidity, and MMSE score at diagnosis as well as the presence/absence of non-amnestic cognitive impairments. Similar results were found, with age (HR = 1.04, Z = 3.55, p <0.001) and non-amnestic cognitive impairments (HR = 0.55, Z = -3.16, p <0.001) as significant predictors. Given that the numbers included in model 3 were reduced due to missing data within MMSE scores and given the similar results across models 2 and 3, model 2 was established as the best fit.
DISCUSSION
Main findings
Before beginning an extensive assessment of the cohorts’ key DLB features, we examined earliest presentation and initial diagnoses among the cohort. When assessing the earliest presenting complaint, in line with DLB criteria [4, 23], memory loss and hallucinations were identified as two of the most frequent among the whole cohort. Interestingly, in this cohort, low mood was also one of the most common presenting complaints. This is in line with the growing body of evidence showing that DLB patients have higher rates of depression compared to AD and other forms of dementia [24–26], and it is notable that depression remains a suggestive clinical feature in the revised DLB diagnostic criteria [4]. Beyond the more common presenting complaints, a wide range of others occurred less frequently (in less than 5% of cases). Some of these were similar to the key DLB criteria such as forms of memory loss (e.g., fluctuating cognitive impairment), hallucinations and related phenomena (e.g., illusions), and parasomnia (e.g., RBD). Others, however, are not known as established symptoms or features of DLB (e.g., self-harm, behavioral disturbance, somatic delusions) and may not suggest a diagnosis of DLB on first presentation. DLB patients are known to present with more complex neuropsychological profiles than other forms of dementia [9]. This can be clearly seen within the present cohort, with the wide range of presenting complaints identified by clinicians.
Within our cohort, approximately 20% had received an initial diagnosis other than DLB on their first consultation where cognitive impairment was recorded by a clinician. This is a considerably lower rate than that found in the Lewy Body Dementia Association (LBDGA) survey of 962 carers who reported an initial diagnosis different to that of DLB in 78% of cases included in the survey [27, 28]. On a positive note, over half the cohort did receive a diagnosis of DLB on the date of their first consultation and it should be noted that our cohort has much better generalizability than a heavily-selected survey population given that the cohort were identified through anonymized clinical records. Similarly, to other studies, we also found that the most common misdiagnoses were other forms of dementia (e.g., AD, vascular dementia) [27, 29]. After these, there was a wide range of disorders identified for the cohort, ranging across forms of depression, delusional disorder, and Charles Bonnet syndrome. Despite validated diagnostic criteria [4] and biomarkers that can be used for diagnosis [30, 31], there are considerable differences in reported DLB prevalence rates [32–33] with some reports suggesting that two out of three cases of DLB are incorrectly identified in routine clinical care [34]. It could be that, similar to the rates of RBD discussed below, there is a lack of awareness among the diagnosing clinicians about DLB and its presenting features. Hallucinations and low mood were two of the most frequent presenting complaints among our cohort. Features which are not immediately associated with a diagnosis of DLB.
Our cohort had similar rates of visual hallucinations to those expected from established rates [4, 23]. However, the rates of Parkinsonian features, and in particular RBD, were below what would be expected. It is unclear if these findings are due to differences in our DLB cohort or a lack of awareness among clinicians for these key diagnostic criteria. In terms of disease progression and outcomes, we found that the presence of non-amnestic cognitive impairments was the only key feature that affected mortality. Individuals who had features of non-amnestic cognitive impairments (e.g., deficits in attention, visuospatial, and executive function) documented within their clinical records lived slightly longer (difference between medians was nine months) than those who did not and were 43% less likely to have died by the end of the study. Numerous previous examples have shown that, compared to AD and Parkinson’s disease cohorts, individuals with DLB present with greater deficits in attention, visuospatial abilities, and executive function measures [35–37]. These differences in non-amnestic cognitive impairments are pronounced and can be seen early on in prodromal DLB and AD [38]. Our finding of those with non-amnestic cognitive impairments living longer is slightly inconsistent with these previous results.
When examining this result, consideration should be paid to previous research examining the differences between pure DLB and those with mixed AD-DLB. The number of DLB patients with associated AD is unclear given the low numbers of studies assessing this group; however, some reports suggest that between 50-80% of DLB patients have AD pathology [39]. Compared with pure DLB, patients with mixed AD-DLB have been shown to have poorer survival, higher nursing home admittance risk, and worse memory performance [39–41]. If our current cohort are presenting with greater AD pathology, these amnestic cognitive impairments (e.g., more pronounced deficits in memory performance) may have appeared as the main presentation and received greater consideration rather than the accompanying deficits in attention, visuospatial and/or executive function. It should be noted that the current study focuses only on a DLB cohort and the number of previous examinations of pure DLB comparing to mixed AD-DLB are low (predominantly containing small DLB sample sizes). Even with these small DLB sample sizes, it has been shown that individuals with DLB present with greater variability in their cognitive performance [42]. Added to this is the complication of distinguishing pure DLB from mixed AD-DLB. Recent research has reported low identification rates among clinicians for mixed AD-DLB [35].
Strengths and limitations
The current investigation benefited from a larger sample size than many previously published examinations of DLB cohorts. The use of an anonymized database derived from routinely collected clinical records removed sampling bias in relation to diagnosed cases; the cohort was selected based on a protocol developed from diagnostic criteria by experienced clinicians. The extensive searches for key and supportive DLB features reduced the chances of recall bias. The use of structured and free text clinical records allowed a large amount of diagnostic, temporal and neuropsychological information to be gathered on the whole cohort and enabled an in-depth examination to be completed. A number of limitations should also be noted. Clinical records are not created for the purpose of research and therefore data was missing for some variables. Certain demographic and cognitive status information was inconsistently reported and missing for the vast majority of the cohort. A protocol was developed according to diagnostic criteria; however, there is still the possibility of misclassification of cases, particularly given the nature of DLB. Although the sample is larger than many previously published cohorts, it is limited by the fact that it was completed within one NHS Trust in the UK. The manual searches were completed by experienced clinicians and in line with the protocol; however, there is still the possibility for error within the case identification and examination of DLB features.
Conclusions and future research
Here, we have presented an in-depth focused examination of what we believe to be one of the largest assembled clinical DLB cohorts, covering their symptom presentation, neuropsychological profile and mortality as predicted by key DLB features. The current study emphasizes the wide range of symptoms with which patients with DLB can present, and the complex profile of this disease. We highlight low mood as an important feature. Furthermore, those DLB patients who presented with non-amnestic cognitive impairments where found to live slightly longer compared to those who didn’t. It should be noted that this is an area lacking extensive assessment in the past. In order to distinguish DLB from other dementia types and all its subtypes, more studies like ours need to be conducted, using larger cohorts from different locations and combining multiple sources of clinical data. Our future aim is to develop the DLB cohort extensively and complete detailed assessments with comparisons to non-DLB disease dementia controls (e.g., AD, vascular dementia). Such DLB databases, with non-DLB controls, would allow more precise measurement of the prodromal presentation of pure and mixed DLB, as well as the clinical progression and outcomes for both.