
Abstract
We examined the cross-sectional association between mushroom intake and mild cognitive impairment (MCI) using data from 663 participants aged 60 and above from the Diet and Healthy Aging (DaHA) study in Singapore. Compared with participants who consumed mushrooms less than once per week, participants who consumed mushrooms >2 portions per week had reduced odds of having MCI (odds ratio = 0.43, 95% CI 0.23–0.78, p = 0.006) and this association was independent of age, gender, education, cigarette smoking, alcohol consumption, hypertension, diabetes, heart disease, stroke, physical activities, and social activities. Our cross-sectional data support the potential role of mushrooms and their bioactive compounds in delaying neurodegeneration.
INTRODUCTION
Emerging evidence has suggested that mushrooms may have neuroprotective properties [1 –5]. However, up to date, only two epidemiological studies have examined cognitive benefits of mushroom consumption in community-living elderly individuals. In the Hordaland Health Study, mushroom intake was linearly associated with better cognitive performance among Norwegians aged 70–74 years [6]. More recently, investigators from the Ohsaki cohort 2006 study showed that frequent mushroom consumption of 3 times per week or more was associated with a 19% reduced risk of incident dementia among Japanese aged 65 years and above [1].
While promising results have been reported from the two studies, it remains unknown if mushroom consumption is associated with reduced odds of having mild cognitive impairment (MCI), which is thought to be a transition phase between normal age-associated cognitive decline and dementia. To answer this question, we analyzed cross-sectional data from 663 community-living elderly who participated in the Diet and Healthy Aging (DaHA) study [7] in Singapore. We hypothesized that mushroom consumption is associated with reduced odds of having MCI, and this association is independent of potential confounders such as age, gender, education level, lifestyle factors, and certain medical conditions that are associated with cognitive impairment. The dose-dependent relationships were examined using appropriate statistical methods.
MATERIALS AND METHODS
Study population
We analyzed data from 663 participants aged 60 and above from the DaHA study who have not been diagnosed with dementia or any psychiatric disorders. The DaHA is a community-based study in Singapore that aims to identify dietary factors that are associated with healthy and functional aging and reduced risk of age-related conditions such as dementia and MCI [7]. Participants were recruited from a geographically defined area in Jurong, west Singapore primarily through home visits to government-built flats in public housing blocks near the Jurong Point Shopping Mall, where our study center was located. In Singapore, the majority of the population live in public housing developed by the Housing and Development Board (HDB) so the study sample largely represents the general population. Eligible participants (aged 60 and above, living in the community) were invited to the study center for interviews and assessments. The DaHA study collected a wide range of data on demographics, lifestyles, diet, health status, medical conditions, cognitive function, psychological wellbeing, etc., within a cross-sectional study design at its baseline from 2011 to 2017. For each of the participants, trained research nurses and research staff conducted data collection at sequentially scheduled study visits (2 to 6 in total according to the eligibility of each of the participants) that were scheduled as closely as possible, typically within one-month time. From the total 901 DaHA participants whose data were available for analysis, we excluded 20 participants whose cognitive status (MCI versus normal cognitive function) was unknown, 40 participants with a clinical diagnosis of dementia or psychiatric disorders, 161 participants with missing data on mushroom consumption, and 17 non-Chinese participants. The remaining sample of 663 Chinese participants consisted of 90 MCI and 573 people with normal cognitive function. There was no difference in age and gender between the final sample of 633 participants and the 181 participants excluded because of missing data on mushroom consumption or unknown cognitive status. However, a high proportion of excluded participants had an education level of equal or less than 6 years (93.4% versus 62.9%, p < 0.001). Also, as related to education level, the mean Singapore modified Mini-Mental State Examination (SM-MMSE) score of excluded participants was lower than that of the final study sample (27.0±2.6 versus 28.2±2.0, p < 0.001).
The study is approved by the National University of Singapore Institutional Review Board (NUS IRB 10-517). All participants provided informed consent before participating in the study.
Mushroom consumption
Community research nurses collected information on the consumption of mushrooms through one-on-one interviews, using a 6-item mushroom consumption questionnaire. The question “how often do you eat the following?” was used in the interview. Responses were recorded as number of portions per day (for those who consumed at least 1 portion per day), per week (for those who consumed mushrooms 1–6 portions per week), or per month (for those who consumed mushrooms less than 1 portion per week). In case the participant was unable to provide an answer, the nurses further probed by asking the participant’s intake over the past one week/over the past month and recorded the responses accordingly. The questionnaire included six mushrooms that are commonly consumed in Singapore: 1) mushroom, golden; 2) mushroom, oyster; 3) mushroom, shiitake; 4) mushroom, white button; 5) mushroom, dried; 6) mushroom, button, canned, drained. For each item, the participants were asked to report the frequency of consumption at portion unit. A portion was defined as a standard serving, that is one three-quarter cup of cooked mushrooms with an average weight of around 150 g. A show card was used as a visual aid to explain portion size to participants. Total mushroom intake was calculated based on response to the six items. All responses were then standardized to the number of portions per week using the following formula:
Mild cognitive impairment
We used the Singapore modified Mini-Mental State Examination (SM-MMSE) [8] to assess global cognitive function and further assessed cognitive domains in detail using a structured neurocognitive assessment battery. A local version of the Clinical Dementia Rating (CDR) [9] was also administered. Two senior consultant psychiatrists (EHK, RM), the Principal Investigator of the DaHA study (LF), and the clinical assessment team made the consensus diagnosis of MCI according to Petersen’s criteria [10] with necessary modifications according to local context and clinical judgements and consensus of the expert panel. In particular, an MCI diagnosis was made by the panel if there was clear cognitive decline and deficits based on available information and clinical judgments but no self-reported cognitive complaints from the participant. In our local setting, the lack of subjective complaint in early cognitive decline could potentially be explained by low education level and misconception of cognitive deficits as part of normal aging; under such scenario, consensus diagnosis was reached based on clinical judgements. For objective evidence of cognitive impairment, we used tests with published local norms [11]. This set of age- and education- specific norms was produced using data from a group of cognitively normal community-living elderly in Singapore. Cut-off points of objective impairment were determined by subtracting 1.5 standard deviations from mean values of the test scores for each of the subgroups. We also diagnosed dementia and psychiatric disorders according to criteria in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) and excluded participants with such diagnoses from this analysis because dietary changes are likely to happen as the consequence of those conditions.
Covariates
The DaHA cohort collected information on a wide range of variables at baseline. In the main analysis, we considered the following as potential confounders: age, gender, education (≤6 years versus >6 years), current cigarette smoking, consuming alcohol at least once a week, hypertension, diabetes, heart disease, stroke, physical activities (daily, 1–6 times/week, less than once a week), social activities (daily, 1–6 times/week, less than once a week). In further analysis, we controlled for additional variables such as body mass index (kg/m2), arthritis, cancer, and the consumption of meat (daily, 1–6 times/week, less than once a week), green vegetables (daily versus less than once a day), fruits (daily, 1–6 times/week, less than once a week), and nuts (daily, 1–6 times/week, less than once a week).
Statistical analyses
We used chi-square test and the Mann-Whitney U test to compare various characteristics between MCI and cognitively normal participants. We used logistic regression models to examine the association between mushroom intake and MCI, treating mushroom consumption as a categorical (<1/week, 1-2/week, >2/week) or a continuous variable (portion/week). We considered different structures for the model forms. Model 1 is a basic model without adjusting any confounder; model 2 is a joint model which adjusted for age, gender, education, cigarette smoking, alcohol consumption, hypertension, diabetes, heart diseases, stroke, physical activities, and social activities. Further logistic regression analysis with additional adjustment of variables such as body mass index, arthritis, cancer, and the consumption of meat, green vegetables, fruits and nuts were conducted to assess the robustness of the association. We then conducted a nonparametric spline modeling to further assess the potentially non-linear dose-dependent relationship in greater detail. We also repeated the main analysis of logistic regression for males and females separately to examine the potential role of gender in modulating the relationship between mushroom consumption and MCI. Additional analysis was conducted by controlling for psychiatric disorders (primarily depressive and anxiety disorders) in a logistic regression model instead of excluding participants with such disorders from analysis. Those results were reported in the text only. All analyses were performed using R, a software environment for statistical computing and graphics and IBM SPSS Statistics for Windows, Version 25 (IBM Corp, Armonk, NY, USA).
RESULTS
The mean (SD) or N (percentage) of each variable was tabulated (Table 1), presenting comparisons between MCI and normal aging participants. MCI participants had a higher age than cognitively normal participants; MCI participants had a higher proportion of hypertension, diabetes and stroke, and were less active in social activities. MCI participants also had lower MMSE scores and lower intake of mushrooms. There was no statistically significant difference on other variables.
Description of the study sample based on cognitive status
1Obtained by using chi-square test or Fisher Exact Test for categorical variables and Mann-Whitney U test for continuous variables.
Results from logistic regression are shown in Table 2. Participants who consumed >2 portions of mushrooms per week had lower odds of having MCI (OR = 0.43, 95% CI 0.24–0.75, p = 0.003); this relationship remained statistically significant after adjusting for demographic, lifestyle, and medical conditions in model 2 (OR = 0.43, 95% CI 0.23–0.78, p = 0.006). Similar results were found when mushroom intake was treated as a continuous variable: the OR associated with one portion increase in mushroom intake was 0.78 (95% CI 0.66–0.93, p = 0.005) in the adjusted model. Further adjustment for body mass index, arthritis, cancer, and the consumption of meat, green vegetables, fruits, and nuts in model 3 did not change the results significantly; the adjusted odds ratio was 0.48 (95% CI 0.26–0.89, p = 0.021) for participants who consumed greater than 2 portions of mushrooms per week. Results from spline analyses showed consistent results with logistic regression on the reverse relationship between mushroom consumption and the odds of having MCI. Mushroom consumption was associated with reduced odds of having MCI and this was significant at consumption of 0.75 portions/week (reference: 0 portion/week); the slope became less steep at higher mushroom consumption level (Fig. 1). Stratified analysis based on gender showed broadly similar findings in males and females. The adjusted odds ratio associated with consuming >2 portions of mushrooms per week was 0.27 (95% CI 0.08–0.97, p = 0.045) in men and 0.43 (95% CI 0.21–0.88, p = 0.02) in women. When participants with psychiatric disorders were included, further adjusting for psychiatric diagnosis in addition to all variables in model 2 produced similar results: the adjusted odds ratio was 0.39 (95% CI 0.22–0.70, p = 0.002) for participants who consumed greater than 2 portions of mushrooms per week.
Mushroom consumption (as categorical variable) and mild cognitive impairment
aBasic model, no adjustment. bAdjusted for age, gender, education, cigarette smoking, alcohol consumption, hypertension, diabetes, heart diseases, stroke, physical activities, social activities. cAdjusted for all variables in model 2 + body mass index, arthritis, history of cancer, and the consumption of meat, green vegetables, fruits, and nuts.
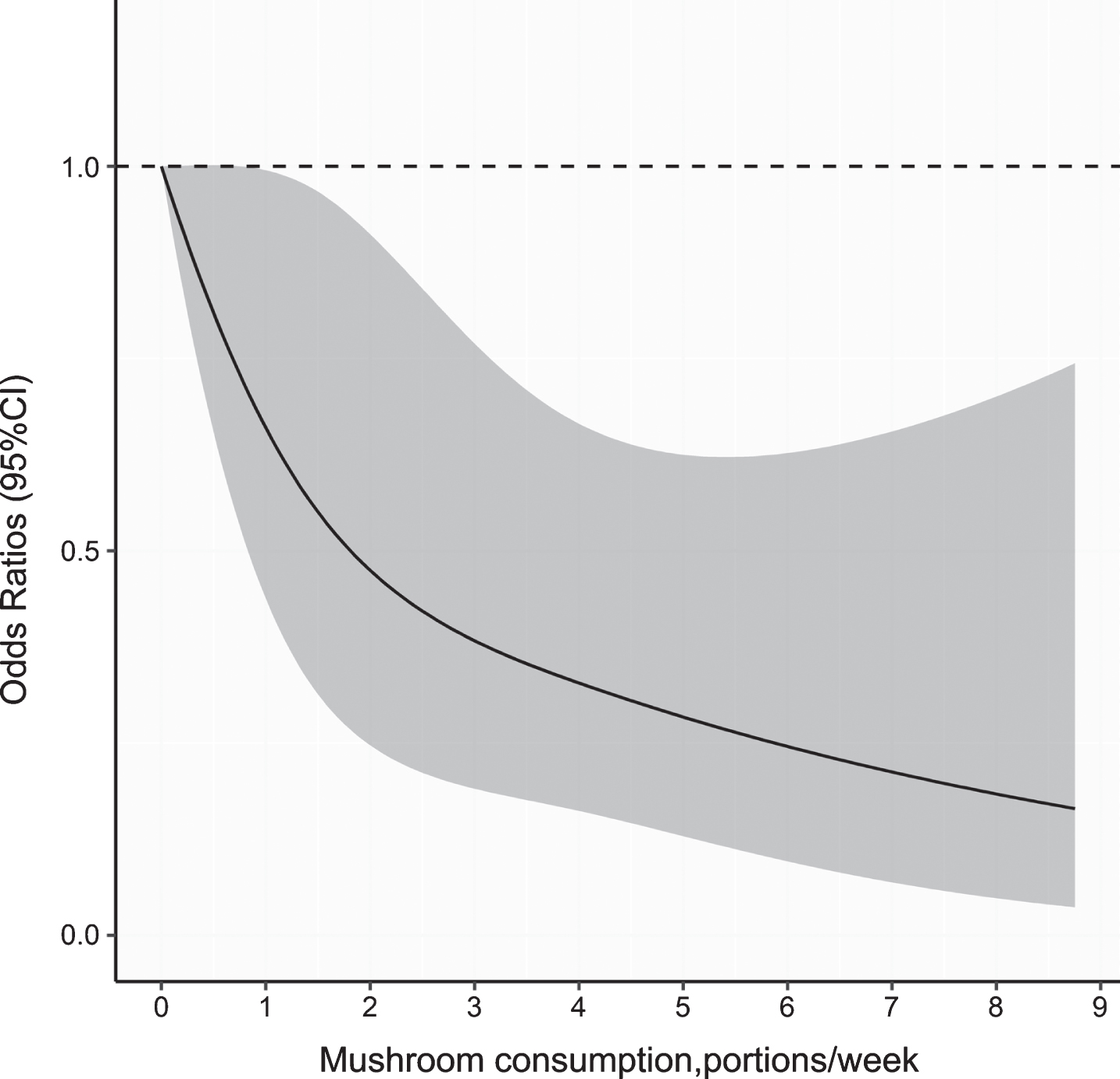
Functional dependence of mild cognitive impairment on mushroom consumption (treated as a continuous variable): the solid curve is estimated via the smoothing spline approach. Adjusted for age, gender, education, cigarette smoking, alcohol consumption, hypertension, diabetes, heart diseases, stroke, physical activities, social activities.
DISCUSSION
Using data from the Diet and Healthy Aging Study in Singapore, we found that mushroom consumption was associated with reduced odds of having MCI. The reduction was significant for participants who consumed greater than 2 portions of mushrooms per week.
Our findings are consistent with earlier studies that have examined the relations between mushroom consumption and cognitive health in aging among community-living elderly. Using data from the Hordaland study, Nurk and colleagues found that mushroom consumers had better performance on all six cognitive tests as compared with non-consumers; the dose-response association of mushrooms on cognitive performance tended to be linear [6]. Our logistic regression and spline analysis confirmed the approximate linear relationship between mushroom intake and cognition, we further identified a critical threshold of 2 portions per week (from logistic regression) and 0.75 portions per week (from spline analysis) since only consumption above this amount was associated with statistically reduced odds of having MCI. Using logistic regression, we found that those who consumed greater than 2 portions of mushrooms per week had lower odds of having MCI (OR = 0.43, 95% CI 0.23–0.78); this is in line with findings from the study conducted by Zhang and colleagues using data from the Ohsaki cohort study, in which a statistically significant finding was revealed for participants who consumed mushrooms 3 times or more per week (adjusted Hazard Ratio = 0.81). The observed effect size appears greater than that observed in the Japanese study [1]. However, the Japanese study was a prospective cohort study with incident dementia as the study outcome while ours is a cross-sectional study focusing on MCI; furthermore, the Japanese study adjusted for consumption of other foods in their main analysis. Hence, direct comparison of effect sizes in the two studies is not appropriate.
There were inconsistent findings on mushroom consumption and cognition among middle-aged men and women in the Doetinchem Cohort study [12]. In this study, mushroom consumption was correlated with faster processing speed but not performance on other cognitive domains or change of cognitive function over time. Again, important differences in study design (for example: cognitive function and decline versus MCI as the study outcome) and key characteristics of the study population (for example: younger age and better education of participants of the Doetinchem cohort as compared with the DaHA study) prevent direct comparisons between the two studies. Indeed, comparing findings from epidemiological studies is often not feasible because of reasons mentioned above. For replication purposes, future studies need to adopt similar study design and methods to enhance comparability. A meta-analysis could then be conducted to pool accumulated evidence together.
The observed correlation between mushrooms and reduced odds of MCI in our study sample is biologically plausible. Certain components in mushrooms, such as hericenones, erinacines, scabronines and dictyophorines may promote the synthesis of nerve growth factors [4]. Bioactive compounds in mushrooms may also protect brain from neurodegeneration by inhibiting production of amyloid-β and phosphorylated tau, and acetylcholinesterase [5]. Mushrooms are also one of the richest dietary sources of ergothioneine (ET) [13, 14]. ET, a thione-derivative of histidine (reviewed in [15]) is an unique putative antioxidant and cytoprotective compound [15 –18]. While humans are unable to synthesize ET, it can be readily absorbed from diet (main source is mushrooms) and actively accumulated in the body and the brain via a specific transporter, OCTN1 [19 –22]. Our recent study in elderly Singaporeans revealed that plasma levels of ET in participants with MCI were significantly lower than age-matched healthy individuals [23], leading us to believe that a deficiency in ET may be a risk factor for neurodegeneration, and increase ET intake through mushroom consumption might possibly promote cognitive health.
The strengths of our study include the comprehensive information on mushroom intake and clinical diagnosis of MCI. We also carefully adjusted for a number of potential confounders using multivariable analysis. However, there are also limitations. With a cross-sectional study design, causal inference between mushroom intake and MCI cannot be made. It is possible that mushroom consumption decreased after the development of cognitive impairment. Also, the results were based on the self-reported information on mushroom intake and other dietary factors, which may not be accurate, especially for those who were cognitively impaired; under-reporting and over-reporting cannot be ruled out. Thirdly, although we adjusted for a wide range of confounding factors, there could be residual confounding from unmeasured factors which could have inflated the effect size estimates. To overcome those limitations, a longitudinal follow-up study with a larger sample size, peripheral biomarkers of both ET and age- and dementia related biomarkers should be conducted in the future. While evidence from our study and previous epidemiological studies is suggestive, whether increasing mushroom consumption will reduce cognitive decline and cognitive impairment remains established. Promising results have been reported from a small scale clinical trial that used a specific type of mushroom (Yamabushitake) as the intervention [4]; however, more data are needed before a definitive conclusion can be drawn. We are aware that effective prevention may require multiple nutritional changes (for examples: homocysteine-lowering B vitamins [24, 25], tea and tea compounds [26, 27], etc.) to achieve public health impact, but as a necessary first step the efficacy of each of the promising candidate should be assessed separately [27]. Mushrooms or active ingredients from mushrooms, such as ET, represent potential interventions.
In summary, using community-based data in Singapore, we found that mushroom consumption was associated with reduced odds of MCI. Based on current evidence, we propose that mushroom consumption could be a potential preventive measure to slow cognitive decline and neurodegeneration in aging.
Footnotes
ACKNOWLEDGMENTS
This work is supported by the National University of Singapore Virtual Institute for the Study of Ageing [grant number VG-8]; the Alice Lim Memorial Fund, Singapore [grant number ALMFA/2010]; the National Medical Research Council of Singapore [grant numbers NMRC/TA/0053/2016 and NMRC/1264/2010/082/12]; the Training and Research Academy at Jurong Point, Singapore; the Lee Kim Tah Holdings Ltd., Singapore; the Kwan Im Thong Hood Cho Temple, Singapore; and the Presbyterian Community Services, Singapore.