
Abstract
Background:
The percentage of verbal forgetting (VF%) measure of the Rey Auditory Verbal Learning Test (RAVLT) has been proposed to differentiate patients diagnosed clinically with Alzheimer’s disease (AD) and dementia with Lewy bodies (DLB).
Objective:
To determine if VF% aligns with gold-standard biomarker and autopsy evidence of AD and DLB neuropathology.
Methods:
Clinical, cognitive, sociodemographic, and biomarker data were collected from 315 patients with baseline cognitive impairment and 485 normal controls from the Alzheimer’s Disease Neuroimaging Initiative (ADNI). AD markers included reduced cerebrospinal fluid (CSF) amyloid-β, elevated total-tau and phosphorylated-tau, hippocampal atrophy, and the presence of amyloid plaques and neurofibrillary tangles at autopsy. DLB markers included reduced CSF α-synuclein, preserved hippocampus, atrophied putamen, occipital glucose metabolism, and the presence of Lewy bodies at autopsy. Cognitively impaired participants were classified as ADVF% (n = 190) or DLBVF% (n = 125) based on their RAVLT VF% scores using a 75% cut-off (≥75% = ADVF%, <75% = DLBVF%). Postmortem data were available for 13 ADVF% participants, 13 DLBVF% patients, and six healthy controls.
Results:
ADVF% and DLBVF% participants did not differ on CSF or neuroimaging biomarkers, with the exception of total tau levels which were higher in ADVF%. In the subset of participants with autopsy data, comorbid AD and DLB pathology was most frequent in ADVF% participants, and pure DLB pathology was most frequent in DLBVF% participants, however, these differences were not statistically significant.
Conclusion:
The RAVLT VF% measure does not reliably align with AD and DLB neuropathology in ADNI participants.
INTRODUCTION
Alzheimer’s disease (AD) and dementia with Lewy bodies (DLB) are the two most common forms of neurodegenerative dementia [1]. Although less prominent in DLB, both AD and DLB patients experience persistent memory impairments during the early stages of the disorders [2, 3] making it difficult to differentiate between these disorders. An incorrect diagnosis of AD has both clinical and economic consequences, as patients may have to pay for inappropriate treatments and medical services until a correct diagnosis is given [4, 5]. These costs are not only incurred by patients and their families; indeed, misdiagnoses of AD also costs millions of dollars to society [5]. In research protocols, incorrect diagnoses may result in incorrect conclusions about study findings. As such, an accurate, low-cost measure is needed to correctly differentiate AD from DLB.
Such a measure was recently proposed by Bussè and colleagues [6], who examined whether specific measures of the Rey Auditory Verbal Learning test (RAVLT) [7] could be used to differentiate between these dementias. They found that DLB patients had higher performance in verbal learning (VL) than AD patients, and a lower frequency of verbal forgetting (VF) and reduced recency effect. Statistically, the groups could be distinguished based on percentage of verbal forgetting (VF%), which is a retention index of words recalled after a 20–min delay, adjusted for short-term memory performance. These results suggest that the RAVLT may potentially be used as a simple, easily accessible, low-cost instrument to discriminate these dementias. However, a major limitation to Bussè and colleagues’ study was that the diagnoses of DLB and AD were based solely on the clinical progression of symptoms at a three-year follow-up and were not corroborated with autopsy or biomarker confirmation. This is problematic because misdiagnosis of DLB as AD based on clinical presentation is frequent [8] with sensitivity estimates <33% [9]. Indeed, up to half of individuals who are carefully screened and selected for AD in cohort studies [10] and clinical trials [11] are later confirmed to have DLB pathology at autopsy. It is unknown whether RAVLT measures may be helpful in screening for DLB pathology in individuals presenting phenotypically as AD.
Histopathological confirmation at autopsy is the only definitive diagnostic method [12] and serves as the gold standard for determining the accuracy of clinical diagnoses of AD [13] and DLB [14]. The pathological hallmarks that define AD are amyloid plaques and neurofibrillary tangles (NFTs) [15] and the defining pathology in DLB is the presence of protein aggregates known as Lewy bodies [16]. In premortem studies, in vivo biomarkers have become an essential component of classifying dementias and are the second-best method of confirming clinical diagnoses, after autopsy. Biomarkers for corroborating a diagnosis of AD include reduced levels of amyloid-β (Aβ) and elevated levels of total-tau (t-tau) and phosphorylated-tau (p-tau) in cerebrospinal fluid (CSF), which have been associated with plaques in the hippocampus and neocortex [17] and NFT pathology in several neocortical regions [18], respectively. A third biomarker for AD is medial temporal lobe neurodegeneration seen on structural neuroimaging [19] which is strongly correlated with percent area of amyloid plaques and NFTs but not Lewy body pathology [20]. Relative preservation of medial temporal lobe structures, on the other hand, is a supportive biomarker for the diagnosis of DLB [3] with possible atrophy of basal ganglia structures (e.g., the putamen) [21–23]. Reduced CSF levels of α-synuclein have also been proposed as a biomarker for DLB [24] as this may reflect the buildup of Lewy body pathology [25]. Lastly, occipital hypometabolism is an additional supportive biomarker for DLB [3].
In the absence of diagnostic confirmation from autopsy or biomarker data, no definitive conclusions can be made regarding the usefulness of the cognitive markers proposed by Bussè and colleagues to distinguish true DLB from AD, independent of clinical presentation. The purpose of the current study was to determine if the percentage of verbal forgetting (VF%) measure proposed by Bussè et al. [6] is accurate in differentiating DLB from AD pathology, quantified using in vivo biomarkers and postmortem pathology. Because our aim was to directly test the claims put forth by Bussè and colleagues (i.e., that using VF% as an initial classification measure should robustly distinguish AD from DLB, in the absence of any other markers or clinical indicators), we elected to first classify cognitively impaired participants based on VF%, then to verify whether this classification aligned with more established markers of disease pathology (CSF levels of Aβ, tau, and α-synuclein, as well as integrity of medial temporal lobe structures). Of note, this is how RAVLT scores would be used clinically if a practitioner were to follow Bussè and colleagues’ recommendations and apply VF scores as cognitive markers of AD and DLB. Based on the results of the original study, it was hypothesized that participants who were classified as probable AD based on their VF% scores (ADVF%) would have higher CSF levels of p-tau and t-tau, lower levels of CSF Aβ, and greater hippocampal atrophy compared to participants classified as probable DLB based on their VF% scores (DLBVF%). ADVF% classification was also expected to be associated with significant plaques and tangles at autopsy. In addition, it was hypothesized that DLBVF% participants would have lower CSF levels of α-synuclein, atrophy of the putamen with relative hippocampal sparing, and greater occipital hypometabolism compared to ADVF% participants. DLBVF% classification was also expected to be associated with significant Lewy bodies at autopsy. A sample of healthy controls was included as a benchmark for normal age-related change in CSF protein levels and brain structures.
METHODS
The data used in this study were obtained from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (http://adni.loni.usc.edu/), a large-scale data sharing effort across North America to study the progression of AD. ADNI is led by Principal Investigator Michael W. Weiner, MD and was launched in 2003 as a public-private partnership. The primary goal of ADNI has been to determine whether the progression of mild cognitive impairment (MCI) and AD can be measured by combing serial magnetic resonance (MR) imaging, positron emission tomography (PET), other biological markers, and clinical and neuropsychological assessments. Up-to-date information can be found at http://www.adni-info.org.
Participants
Information regarding CSF biomarkers (Aβ, t-tau, p-tau, and α-synuclein), quantitative numeric MR and PET data, as well as clinical, cognitive and sociodemographic data were obtained from 3,637 participants in ADNI1 (n = 1,386), ADNIGO (n = 355), ADNI2 (n = 1,242), and ADNI3 (n = 654). To remain consistent with Bussè and colleagues’ original methodology [6], participants were excluded if they were demented at baseline (n = 379), had MCI at baseline but never went on to develop dementia (n = 478), or lacked any follow-up data after baseline diagnosis (n = 2,081). Participants who failed ADNI’s intake screening (n = 564), who were missing diagnostic data at baseline (n = 1,068), or who were missing RAVLT scores (n = 1,523) were also excluded, resulting in a final sample size of 800 (many participants fulfilled more than one exclusion criterion). This sample included 485 normal controls (NC) and 315 cognitively impaired individuals at baseline who eventually developed dementia. Follow-up data were collected in six-month intervals after baseline diagnosis until 24 months. After 24 months, follow-up data were collected in 12-month intervals up to a maximum of 156 months. The mean amount of time between baseline and dementia diagnosis was 28.78 months.
Participants in ADNI were classified as normal controls if they had no memory complaints, normal memory function (determined by scoring at specific education adjusted cut-offs on the Logical Memory II subscale from the Wechsler Memory Scaled – Revised), a Mini-Mental State Examination (MMSE) [26] score between 24 and 30 (inclusive), a clinical dementia rating of 0, and were cognitively normal based on the absence of significant cognitive impairment and functions of daily living. Participants were diagnosed with MCI if they or a study partner reported memory complaints, abnormal memory function, an MMSE score between 24 and 30 (inclusive), a clinical dementia rating of 0.5, and had preserved general cognition and functioning such that a diagnosis of dementia could not be made. When participants were diagnosed with dementia, criteria for clinical AD were the same as for MCI except participants must have had an MMSE score between 20 and 26 (inclusive), a clinical dementia rating of 0.5–1.0, and met the NINCDS/ADRDA criteria for probable AD. All participants had available RAVLT values, but data were missing for Aβ (n = 230), t-tau (n = 235), p-tau (n = 230), brain volumetrics (n = 397), α-synuclein values (n = 590), and PET data (n = 646). Missing cases were excluded listwise from individual analyses. RAVLT and autopsy data were available on a separate, partially overlapping sample of 32 individuals.
Participants with cognitive impairment were grouped into either ADVF% or DLBVF% based on their VF% scores. As the aim of this paper was to test the claims put forth in Bussè and colleagues’ original paper, we chose to use to use the 75% cutoff proposed by the authors as the optimal one to distinguish AD from DLB [6]. Participants with VF% scores ≥75% were classified as ADVF% (n = 190) while those with scores <75% were classified as DLBVF% (n = 125). In summary, the final sample in this study consisted of 485 NC, 190 ADVF% participants, and 125 DLBVF% participants.
Cognitive scores
The methods for administering the RAVLT and calculating VF% are described in Bussè and colleagues’ study [6]. Briefly, the RAVLT involves presenting participants with a list of 15 words across five consecutive trials. The list is read aloud, and the participant is asked to immediately recall as many words they can remember. After repeating this procedure for five trials, the participants are read a different list of 15 words (List B) and they are asked to immediately recall as many words as they can remember. Immediately after the List B trial, participants are asked to recall the words from the first list. After 30 minutes of interpolated testing, the participants are asked to recall the words from the first list (delayed recall trial). VF% is obtained by subtracting scores from the delayed recall from Trial 5 and dividing this value by the number of words recalled on Trial 5. In addition, the MMSE was administered to all participants and used as a measure of general cognition.
CSF biomarkers
Baseline CSF samples were collected via lumbar puncture, as described in the ADNI procedure manual (http://adni.loni.usc.edu/methods/documents/). Baseline Aβ, t-tau, and p-tau values were obtained from the UPENNBIOMK_MASTER.csv dataset provided by the University of Pennsylvania. Baseline α-synuclein values were obtained from the CSFALPHASYN_03_21_14.csv dataset provided by the University of Washington.
Neuroimaging biomarkers
All participants underwent 1.5 Tesla structural magnetic resonance imaging (MRI) brain scans which were performed at regular intervals throughout the ADNI study. Only the initial scan, performed between screening and baseline, was used for the present study. More information regarding ADNI MRI protocols can be found at http://adni.loni.usc.edu/methods/mri-tool/mri-analysis/. Preprocessed analyzed volumetrics were downloaded from the University of Arizona SPM voxel-based morphometry dataset (UASPMVBM.csv). Regional volumetrics of interest for the present study included the hippocampus and putamen. These volumes were corrected for whole-brain size.
Half of all ADNI participants also underwent fludeoxyglucose PET (FDG-PET) scans at regular intervals throughout the ADNI study. Participants did not have a PET scan if they were pregnant or at risk for pregnancy, had a history of radiation therapy, or had undergone radiation for research purposes in the past year. Additionally, participants who were determined to have a focal lesion on MRI did not undergo PET. As with the MRI scans, only the initial scan performed at baseline was used for the present study. The data were downloaded from the Banner Alzheimer’s Institute, Phoenix Arizona NMRC Summaries dataset (BAIPETNMRC_04_12_18.csv). More information regarding ADNI PET protocols can be found at http://adni.loni.usc.edu/methods/.
Hypometabolic convergence index (HCI) was used as a measure of brain metabolism, extracted from ADNI dataset BAIPETNMRC_09_04_14.csv. The detailed methodology for computing HCI from PET data has been described previously [27]. Briefly, the HCI represents the proportion of participants’ brain voxels that are hypometabolic compared to controls and overlap with voxels that are hypometabolic in AD patients compared to controls. As such, it is a measure of the extent to which the cerebral metabolic patterns correspond to those seen in typical AD. Occipital HCI, corrected for whole-brain HCI, was the main PET measure of interest.
Autopsy data
Autopsy data were extracted from ADNI dataset NEUROPATH_04_12_18.csv. Histopathological assessments were performed by participating centers, and a standard set of fixed tissue blocks or sections and frozen tissue were shipped to the ADNI Neuropathology Core (ADNI-NPC) as described in the ADNI neuropathology manual (http://adni.loni.usc.edu/methods/documents/). Hematoxylin and eosin stains were applied to formalin-fixed, paraffin wax-embedded tissue blocks, and routine immunohistochemistry was performed using the following antibodies: p-tau (PHF1), Aβ (10D5), phosphorylated α-synuclein, and phosphorylated TDP-43 (pTDP-43). Neuropathological diagnoses were made following the operational criteria for the classification of AD and other pathologies defined by the National Alzheimer’s Coordinating Center (NACC) [28]. In the present study, autopsy variables were binarized into no/mild (Braak stages 0–3) or moderate/severe NFT (Braak stages 4–6); no/mild or moderate/severe amyloid plaques; and absent or present Lewy bodies. Participants were considered to have ‘pure AD’ if they had moderate/severe NFT or plaques, with Lewy bodies absent (n = 8), ‘comorbid AD+DLB’ if they had moderate/severe NFT or plaques, with Lewy bodies present (n = 12), ‘pure DLB’ if they had no/mild NFT and plaques, with Lewy bodies present (n = 5), or ‘no pathology’ if they had no/mild NFT and plaques with Lewy bodies absent (n = 7). The mean amount of time between RAVLT administration and autopsy was 74.38 months.
Statistical analyses
The statistical analyses were run using IBM SPSS Statistics 24. All variables of interest except age were non-normally distributed (Shapiro-Wilk p < 0.05), therefore non-parametric analyses were used. Kruskal-Wallis tests were used to compare age, years of education, MMSE scores, and in vivo biomarker data across the three groups (NC, ADVF%, and DLBVF%), followed by pairwise comparisons using Dunn tests with Bonferroni corrections to test the hypothesis that VF% classification corresponds to dementia biomarkers. Sex and APOE ɛ4 status (≥1 allele = positive; recognized as a major susceptibility gene for AD [29]) were compared between groups using χ2. Autopsy data were not included in these analyses. To minimize multiple comparisons, all brain measures were analyzed bilaterally.
Next, to test the hypothesis that dementia classification would be associated with histopathological findings at autopsy, participants with autopsy data (‘pure AD’, ‘comorbid AD + DLB’, ‘pure DLB’ and ‘no pathology’) were compared on VF% scores (above or below the 75% cut-off) using χ2. The statistical significance threshold was set at α= 0.05 for all analyses. Effect sizes are reported as Cohen’s r, where 0.1, 0.3 and 0.5 are considered small, medium and large effect sizes, respectively [30].
RESULTS
Participant characteristics
ADNI participant characteristics are summarized in Table 1. There were no differences between the three groups with regards to age (χ2 (2) = 0.736, p = 0.692). Years of education was statistically different between groups (χ2 (2) = 6.313, p = 0.043), but pairwise comparisons were not significant at the individual level. Sex was non-evenly distributed across groups (χ2 (2) = 15.822, p < 0.001). There were roughly equal proportions of males and females in the control and ADVF% groups; however, the DLBVF% group had a greater number of males than females. MMSE scores also differed between groups (χ2 (2) = 268.342, p < 0.001). Control participants had significantly higher scores than ADVF% participants (p < 0.001) and DLBVF% participants (p < 0.001). ADVF% participants also had significantly lower mean scores than DLBVF% participants (p = 0.012). A significant interaction was also found between APOE ɛ4 status and diagnosis (χ2 (2) = 116.838, p < 0.001). There were fewer carriers compared to non-carriers in the control and DLBVF% groups, while there were more carriers than non-carriers in the ADVF% group.
ADNI participant characteristics
*p < 0.05 between ADVF% and DLBVF% groups.
CSF biomarkers
All biomarker data are summarized in Table 2. Baseline levels of CSF Aβ (χ2 (2) = 150.134, p < 0.001, r = 0.51; Fig. 1A), t-tau (χ2 (2) = 128.788, p < 0.001, r = 0.48; Fig. 1B), p-tau (χ2 (2) = 85.732, p < 0.001, r = 0.39; Fig. 1C), and α-synuclein (χ2 (2) = 9.400, p = 0.009, r = 0.21; Fig. 1D) differed between groups. However, post-hoc analyses revealed that ADVF% and DLBVF% participants differed from each other only on levels of t-tau (p = 0.021, r = 0.18) and marginally on levels of Aβ (p = 0.056, r = 0.16). They did not differ from each other on levels of p-tau (p = 0.180, r = 0.13) or α-synuclein (p = 1.000, r = 0.01). Control participants had significantly higher levels of Aβ (p < 0.001, r = 0.52) and α-synuclein (p = 0.027, r = 0.20) than ADVF% participants, and lower levels of t-tau (p < 0.001, r = 0.49) and p-tau (p < 0.001, r = 0.39). Control participants also had significantly higher levels of Aβ (p < 0.001, r = 0.33) and lower levels of t-tau (p < 0.001, r = 0.28) and p-tau (p < 0.001, r = 0.24) than DLBVF% participants, as well as marginally higher CSF levels of α-synuclein (p = 0.055, r = 0.20).
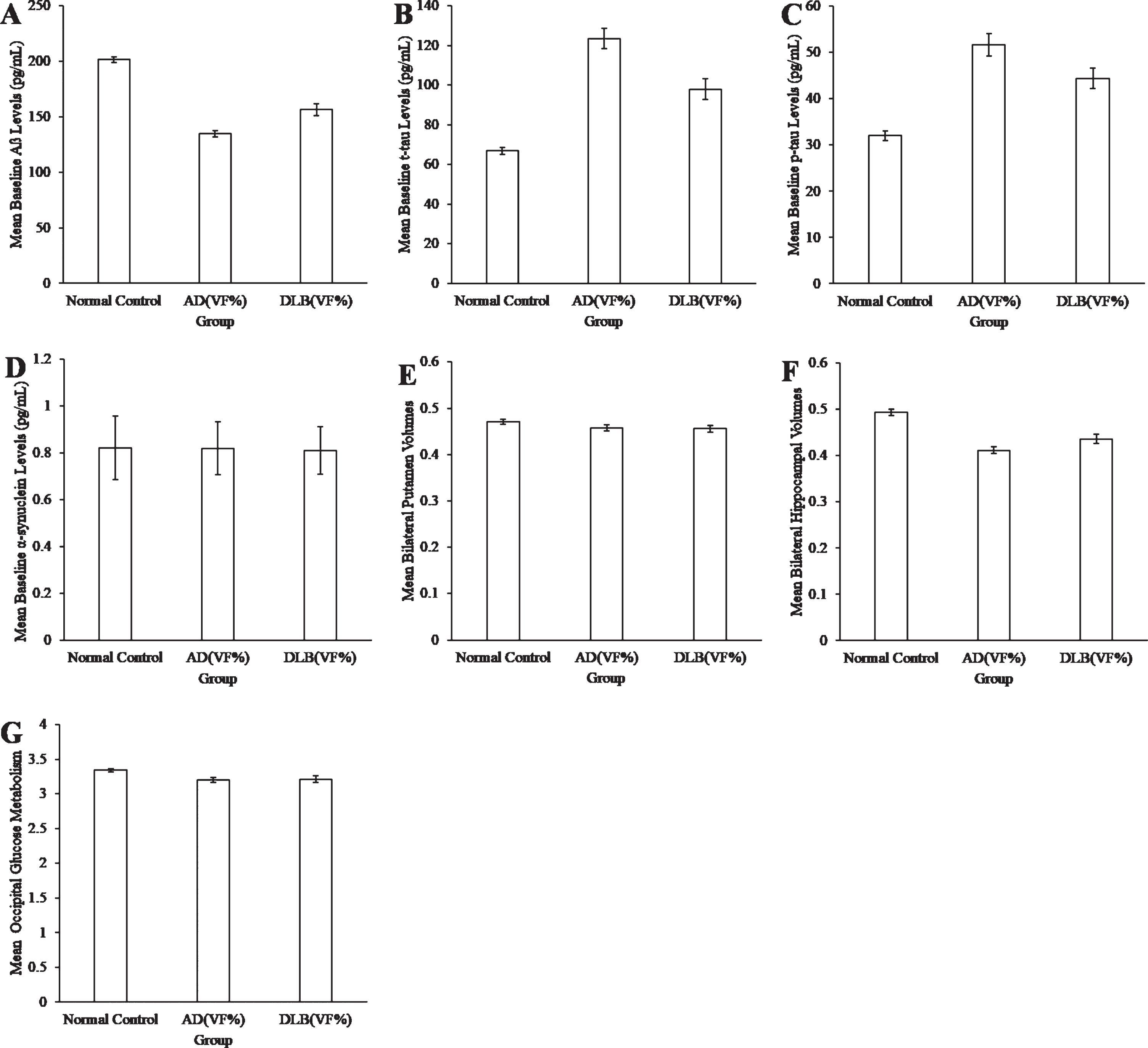
Mean CSF Aβ (A), CSF t-tau (B), CSF p-tau (C), CSF α-synuclein (D), putamen volume (E), hippocampal volume (F), and occipital glucose metabolism (G) of normal controls and patients diagnosed as AD or DLB based on their VF% scores. Error bars represent the standard error of the mean (SEM).
Biomarker data
Neuroimaging biomarkers
As for neuroimaging biomarkers, there were no significant group effects for the volume of the putamen (χ2 (2) = 3.348, p = 0.188, r = 0.09; Fig. 1E). There was a significant group effect for the volume the hippocampus (χ2 (2) = 56.672, p < 0.001, r = 0.38; Fig. 1F). Controls had significantly larger hippocampi than ADVF% participants (p < 0.001, r = 0.40) and DLBVF% participants (p < 0.001, r = 0.32), but hippocampal volume did not differ between the two patient groups (p = 0.355, r = 0.11). There was also a significant effect of occipital glucose metabolism between groups (χ2 (2) = 9.609, p = 0.008, r = 0.25; Fig. 1G). Post-hoc analyses revealed that control participants had significantly higher occipital glucose metabolism than ADVF% participants (p = 0.012, r = 0.26) but not DLBVF% participants (p = 0.114, r = 0.20), while occipital glucose metabolism did not differ between the two patient groups (p = 1.000, r = 0.04).
Neuropathology
There was a marginally significant interaction between autopsy findings and diagnostic classification based on VF% scores (χ2 (2) = 12.455, p = 0.053; r = 0.62; Table 3). ADVF% and DLBVF% groups had roughly even proportions of participants with pure AD pathology (4/13 and 3/13, respectively), but ADVF% participants had more frequent comorbid AD and DLB pathology (7/13) than did DLBVF% participants (4/13). Fewer ADVF% participants had pure DLB pathology (1/13) or no pathology (1/13) compared to DLBVF% participants (4/13 and 2/13, respectively). Most control participants had no pathology (4/6), though one had significant pure AD pathology and one had comorbid AD and DLB pathology.
Autopsy sample characteristics
DISCUSSION
This is the first study to use gold standard biomarker and autopsy data to determine if the VF% measure of the RAVLT is accurate in differentiating AD and DLB neuropathological markers. In contrast to Bussè and colleagues’ study [6], the results from the present study do not robustly support the hypothesis that VF% is accurate in differentiating DLB from AD pathology. These results do not appear to be confounded by age or years of education.
Participants classified as AD and DLB based on their VF% scores did not display biomarker levels consistent with our hypotheses; the groups did not differ on most biomarkers, with the exception of CSF t-tau which was more elevated in ADVF% participants. One possible explanation for these results is that VF% classification results in categorization that is more closely tied to AD severity than to underlying pathology (i.e., VF% ≥75% representing worse severity). However, because the two patient groups did not differ with regards to age, this is unlikely. Additionally, the biomarker data displayed a wide range of high and low levels that should have been captured by the VF% measure had it been accurate in discriminating DLB and AD pathologies. Autopsy data showed that nearly half (46%) of the cognitively impaired participants had comorbid DLB and AD pathology, which was also not captured by the VF% measure.
Another explanation for these findings is that the participants in both patient groups may have had significant overlapping AD and DLB pathology, which may have obscured clear between-group differences in biomarker profiles; although most participants had no autopsy data, comorbid pathologies were common in those with available data, consistent with prior reports of comorbid AD and DLB pathologies at death [10, 11]. For instance, hippocampal atrophy in the DLBVF% group may be due to concomitant AD pathology, as hippocampal atrophy has been strongly correlated with percent area of plaques and NFTs [20]. Similarly, elevated CSF p-tau and t-tau and reduced Aβ in the DLBVF% group may also be due to comorbid AD pathology, with these biomarkers having been linked to greater number of plaques in the hippocampus and neocortex [17] and more severe NFT pathology in several neocortical regions [18]. Unfortunately, many participants were missing data for CSF protein values and structural brain volumes, potentially resulting in a lack of power to detect group effects, though the small effect sizes suggest minor existing differences.
Although CSF biomarkers are now a recommended biomarker to corroborate a diagnosis of AD [31], there has been some deliberation in the literature regarding their usefulness to distinguish between AD and DLB. Specifically, some studies have found that CSF Aβ levels do not differ between AD and DLB patients [32–34] suggesting that Aβ may not be a reliable biomarker to distinguish these diseases. That CSF Aβ did not robustly differentiate between AD and DLB may not be surprising, as both AD and DLB are known to display amyloid pathology [15, 35]. Similarly, there is conflicting evidence in the literature regarding whether CSF α-synuclein is a useful biomarker in differentiating AD from DLB, with some studies reporting lower levels of α-synuclein in DLB compared to AD [24, 36] and others reporting no difference [37]. It is thus possible that the results from our study reflect the inconstancy of CSF biomarkers to reliably associate with AD and DLB pathological processes. CSF t-tau may be more useful in differentiating AD and DLB pathologies, though effect sizes for t-tau remained small in the present study. However, even more robust biomarkers such as hippocampal atrophy and postmortem pathologies were not different between the patient groups, tentatively suggesting that VF% is not accurate in differentiating AD and DLB. Although these results are not consistent with Bussè et al.’s findings [6], they do corroborate previous findings that memory impairments are common amongst biomarker-diagnosed AD and DLB patients [38].
The neuropathology data were also inconsistent with the original hypothesis, though autopsy findings should be considered cautiously due to the substantial time lag between RAVLT administration and death (approximately 6 years). It is possible that initial associations between RAVLT scores and postmortem findings were washed out by the accumulation of comorbid pathology over the years following baseline cognitive assessment. We believe this is unlikely, as comorbidities were not systematically associated with longer time prior to autopsy in our sample (Table 3). Furthermore, prior work has found that individuals with cognitive impairment due to AD or DLB pathology can be differentiated based on cognitive performance during the MCI stage, several years before autopsy [39]. Rigorous time-lagged designs can help to untangle the progression and accumulation of disease in clinico-pathologic studies; however, the small sample size in the present study allowed only for a primarily descriptive exploration of these results. Of the 13 ADVF% with available autopsy data, most participants had either pure AD (31%) or comorbid pathologies (54%), consistent with previous findings that patients with comorbid pathology tend to have a neuropsychological and clinical profile similar to AD [40]. On the other hand, those with DLBVF% were roughly even split across the ‘pure AD’ (23%), ‘pure DLB’ (31%), and ‘comorbid’ (31%) postmortem classification groups. These results suggest that while a high VF% score is positively associated with the presence of AD pathology (pure or comorbid), the RAVLT is less useful in determining which patients have DLB pathology. Unfortunately, due to the very small number of participants with available autopsy data in this study and to the long clinico-pathologic lag, no strong conclusions can be drawn and results should be replicated independently in other work.
There were several methodological differences between the current study and Bussè and colleagues’ study [6] that may account for the conflicting results. While Bussè and colleagues examined whether VF% scores differ between clinically diagnosed AD and DLB, the present study examined whether VF% could distinguish AD and DLB pathology independent of the clinical diagnosis. Thus, our study was carried out under the premise that the clinical diagnosis of AD may be wrong, as misdiagnosis based on only clinical symptoms is common [8], and our primary question of interest was whether VF% could decipher patients who present clinically as AD but have a high likelihood of underlying Lewy body pathology. A second important difference is that Bussè and colleagues recruited a sample of local participants, which may reflect a better representation of AD and DLB patients than the ADNI database which is highly enriched for AD.
The major limitation to this study is that the ADNI database is specifically selected and enriched for AD. As a result, the number of pure DLB patients in the present study may have been limited. Because of this limitation, the results from the present study may not be generalizable to a broader population. A second important limitation was the considerable amount of missing data in ADNI datasets. In light of positive associations between VF% classification and some diagnostic markers (i.e., APOE ɛ4 status, histopathology data) as well as the almost medium effect sizes for the pairwise comparisons for t-tau and p-tau, it is possible that our hypothesis may have been supported had our study been sufficiently powered to detect positive associations with CSF and neuroimaging biomarkers. Finally, the high degree of overlapping pathology in the already small sample of participants with autopsy data makes it difficult to differentiate the role of these pathologies and their contribution to the clinical manifestations of each patient group, including VF%. In order to find significant differences in a population with a high degree of overlapping neuropathology, a large number of patients with postmortem data will need to be recruited for future studies.
In conclusion, the RAVLT VF% measure does not appear to reliably align with AD and DLB neuropathology. However, due to the selective nature of the ADNI database, future studies will need to be conducted with a less restrictive sample to draw firm conclusions regarding the usefulness of VF% in distinguishing AD from DLB.
Footnotes
ACKNOWLEDGMENTS
Data collection and sharing for this project was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
This work was supported by an Alberta Innovates Summer Research Studentship (MJS) and a Canada Research Chair (BLC). The authors also gratefully acknowledge statistical assistance from Dr. Audrey Schnell, and administrative support from Ms. Alexandra Wall.