
Abstract
Background:
Alzheimer’s disease (AD) pathology is found in the brain years before symptoms are usually detected. An episodic memory (EM) decline is considered to be the specific cognitive sign indicating a transition from the preclinical to the prodromal stage of AD. However, there is still no consensus on the most sensitive tool to detect it.
Objective:
The goal of our study was to determine which EM measures, among three clinically used EM tests and one research EM test, would be optimal to use for detection of early decline in elderly cognitive complainers.
Methods:
318 healthy elderly participants with subjective cognitive complaint were followed for two years. We applied generalized linear mixed models to investigate the effect of baseline brain amyloid and metabolism on the longitudinal evolution of four EM tests.
Results:
Our findings show that participants performed significantly worse in two out of four EM tests (i.e., the Memory Binding Test and the Delayed Matched Sample test 48 items) as their level of brain amyloid load increased. However, we did not find an association between EM measures and brain metabolism. An interaction of the two biomarkers was associated with the number of intrusions in the Memory Binding Test over two years.
Conclusion:
As most clinical trials in AD are now including patients at its early clinical stage, the precise delineation of the transition phase between the preclinical and prodromal stages of the disease is of crucial importance. Our study indicates that challenging EM tests and intrusions are valuable tools to identify this critical transition.
INTRODUCTION
In the past several decades, the Alzheimer’s disease (AD) research framework has seen considerable advances. Due to the substantial progress in clinical biomarkers, AD is now considered a neurodegenerative pathology that can be identified in vivo years before the appearance of the mild cognitive impairment (MCI) that precedes the clinical stage. Staged as a continuum, with dementia representing the final stage of a long period of different pathological brain injuries, preclinical AD refers to the presence of specific physiopathological biomarkers (i.e., amyloidosis, tau, and/or neurodegeneration) without any clinical symptom [1–7]. These biomarkers can be measured via structural neuroimaging (e.g., magnetic resonance imaging, MRI), molecular neuroimaging (with positron emission tomography, PET) and cerebrospinal fluid (CSF) analysis of amyloid or tau-proteins.
Subtle cognitive changes have been reported in AD prior to the clinical stage. Early changes in episodic memory (EM), i.e., the ability to acquire and recollect personally experienced episodes associated with a specific affective, spatial, and temporal context [8–10], can thus be considered as indicative of the transition between the preclinical and prodromal (i.e., MCI with evidence of the presence of specific biomarkers) [7] stages of AD. In the typical form of the disease, a number of studies have highlighted consistent evidence for early onset of EM decline in AD when compared to other cognitive domains. These studies have indeed shown that EM decline would accelerates before (4–8 years before executive function, 7–10 years before other cognitive domains) and would be more predictive of a future AD than the one in other functions [11–17]. Amyloidosis appears to be the earliest biomarker that can be detected in vivo in the AD continuum [7, 18]. Previous studies have shown the presence of brain amyloidosis in cognitively normal elder adults [19, 20], yet in a lesser quantity than in AD patients. High level of amyloid burden in AD and preclinical AD is thought to disrupt the default-mode network, including brain regions that are involved in EM function (i.e., temporal median including hippocampus) [21–25], leading to this subtle decline. Indeed, grouping participants according to their brain amyloid load, some studies have demonstrated an amyloid-related EM decline in preclinical AD [26–29]. In a meta-analysis, Hedden and colleagues estimated a difference of a quarter of standard deviation in EM performance between ‘amyloid-positives’ (i.e., individuals with a significant brain amyloid load) and ‘amyloid-negatives’ [30]. The Free and Cued Selective Reminding Test (FCSRT) [31], a verbal associative EM test, has been widely used in AD clinical assessment and literature. The FCSRT improves initial learning by providing a strategy, pairing a word to be remembered (e.g., grapes) with a corresponding semantic cue (e.g., fruit). Its subscores allow the assessment of different EM processes involved in the memorization of words. Failure in Cued Recall (CR), particularly suggestive of temporo-limbic amnesia [32], has had a longstanding AD diagnostic utility [33] and was recommended as a criterion for the diagnosis of clinical AD [3]. However, in the preclinical stage, some data suggest that free recall performance would decline earlier [34, 35] related to AD biomarkers level [17, 36]. Nevertheless, it has been argued that the classical tools commonly used in clinical neuropsychological assessment to diagnose AD would not be challenging enough to detect and track down the very early cognitive changes in AD for preclinical individuals [37–41]. Since current standard tests used in the diagnosis of AD and MCI were not designed to detect such subtle cognitive changes [40, 42], there is a pressing need to determine and propose reliable cognitive screening measures that are sensitive enough to detect subtle cognitive variations in the preclinical stages of the disease. In this line, Herman Buschke designed the Memory Binding Test (MBT, previously known as the Memory Capacity Test, see Materials and Methods) [43], conceived to be more challenging and more sensitive to very early EM decline. This test notably measures memory binding, which refers to the ability to encode or retrieve independent information as part of a more complex unit [42]. Using MBT, some studies have shown its promising sensitivity in the detection of amyloid-related subtle EM decline compared to FCSRT [40, 44–46]. Furthermore, the binding feature of MBT (i.e., the ability of participants to recall two separately learned items in response to a single category cue) has been significantly related with the risk of decline to an amnestic MCI (aMCI, score ≤ 22/32) [47] or dementia (score ≤ 17/32) [42, 48]. Interestingly, in a recent study by Teipel and colleagues [49], the MBT was used in order to determine the effect of cortical amyloid load, hippocampus and basal forebrain volumes, and education on the cognitive trajectory classes. Their results showed that global amyloid load was associated with a higher probability for an individual to belong to the lowest performing group (in the TIP and List1 + List2 FR scores). An amyloid-related EM decline has also been demonstrated by using visual tests [26], for example the Delayed Matching to Sample task 48 items (DMS48) [50] (see Materials and Methods for details). Indeed, previous studies have shown that recognition tasks could be precociously sensitive in AD [50, 51], due to an early involvement of specific brain structures (i.e., perirhinal and entorhinal cortices) in AD pathology, prior to hippocampal complex involvement [52–54].
Despite the consistent number of neuropsychological tools to assess EM in the verbal and visual domains, it is still not clear today which cognitive endpoint or combination of tests would be the best choice to detect an amyloid-related early subtle decline predicting an ongoing clinical conversion [55]. Previous research has rarely compared various EM measures, including verbal and visual modalities together with biomarkers in a longitudinal study, to determine the most sensitive EM task in a preclinical AD context.
In the present study, we examine the relationship between EM performance measures and AD biomarkers in 318 cognitively normal (CN) elderly participants with cognitive complaint from the INSIGHT-PreAD cohort (INveStIGation of AlzHeimer’s PredicTors in subjective memory complainers) [6]. We chose to focus on memory complainers because some studies have shown that a cognitive complaint in CN subjects may increase the risk of conversion to an MCI or AD [56–58]. Our principal aim is to determine whether the AD biomarker load is associated with EM decline in the verbal in the verbal and visual domains. In order to do achieve this goal, we compared the sensitivity of different EM tests in both modalities using continuous values of common AD biomarkers (amyloidosis and neurodegeneration) [1, 7,59].
MATERIALS AND METHODS
Participants
Participants were recruited from the INSIGHT-PreAD study at the Institute of Memory and Alzheimer’s disease (IM2A, Piti
Three hundred eighteen CN elderly participants, between 70 and 85 years old, were included in the study. All of them met the following inclusion criteria at baseline: age ≥70; presence of a subjective memory complaint; normal score on the Clinical Dementia Rating (CDR = 0), the Mini-Mental State Examination (MMSE ≥27) and the FCSRT (total recall ≥41). Subjects were excluded in case of auditory, visual, or motor impairments, active psychiatric symptomatology, systemic or chronic disease that might interfere with the follow-up.The last subject was included in January 2015. We analyzed the EM performances of the participants for the first two years (24 months, i.e., 3 visits including Baseline).The study INSIGHT-PreAD protocol was approved by the ethics committee of the Piti
Neuropsychological assessment
All participants underwent a comprehensive neuropsychological battery, that evaluated different cognitive processes for EM, language, executive functioning, working memory, praxis, and visuospatial abilities. The level of global cognitive efficiency and level of functioning were respectively evaluated using the MMSE and the CDR exams. Language was assessed with a naming test (DO 80 [60]) and a semantic fluency task (number of animals in 2 min [61]). Praxis assessment [62] and the copy of the Rey-Osterrieth complex figure (ROCF [63, 64]) were administered to assess respectively gesture and visuospatial capacities. Working memory and executive functions were evaluated using Digit and Visuo-spatial Span (forward and backward) from the Wechsler Adult Intelligence Scale (WAIS-III) and the Wechsler Memory Scale (WMS-III) respectively, the Frontal Assessment Battery [65], the Trail Making test and the Lexical Fluency (P words in 2 min; GREFEX versions [61]).
The entire cognitive assessment, including the EM tests, represented a four hours cognitive exam. All exams were performed on the same day, with half of the evaluations completed in the morning, and the other half in the afternoon. The two verbal EM tests were administered in two separate sessions in order to avoid interferences.
Episodic memory assessment
EM was assessed in the verbal and visual modalities. The FCSRT and the MBT were administered in the verbal modality. As stated above, the FCSRT [31] is an associative memory test widely used in the diagnosis of AD [3, 33]. This test consists of a list of 16 words presented to participants in conjunction with a semantic category (e.g., “fruit”). The testing phase consists in a 2– min Free Recall followed by a CR for items that were not recalled. The same procedure is repeated 3 times. The raters record the number of words recalled both freely (free recall 1 + 2 + 3 = total Free Recall [/FR], /48) and with cues (FR + [CR 1 + 2 + 3] = Total Recall [/TR], /48), along with the efficiency of semantic cueing (= [(FR — TR)/(FR — 48)]) [33]. A recognition phase is performed and, after a 20–min delay, the same procedure is performed one last time (Delayed FR and TR). The neuropsychologist also records intrusion errors, i.e., the produced words that did not belong to the learned corpus.
The second verbal EM test in the study is the MBT. Two lists of 16 words are presented in the same way as in the FCSRT procedure. Both lists are based on the same semantic categories (e.g., ‘Colors’ = ‘Yellow’ for list 1 and ‘Brown’ for list 2). After an immediate CR for each list, the examiner administers a paired CR giving all of the 16 semantic cues (Immediate CR), requiring the participant to indicate from which list each recalled word comes from (List 1 or 2, Immediate Source Recall). The rater also records the total number of recalled pairs for each semantic category (TIP). Then, an immediate FR of all the 32 words, and a CR for the non-recalled items are performed (total FR and CR). Following a 20 min delay, the participants perform a delayed FR, CR and source recall of both lists. As for the FCSRT, the neuropsychologist records the total number of intrusion errors, and specifies whether these intrusions were semantically related (Extra-list intrusions) or not (Extra-Category intrusions). Moreover, when participants are asked to recall the second list items, any words originating from the first list are recorded (Prior-List intrusions).For both of these verbal EM tests, two alternative versions are used from one visit to the next, to minimize repetitioneffects.
The visual modality of EM was tested using the restitution of the ROCF and the Delayed Matching to Sample 48 test recalls (/DMS48 [50]).
For the ROCF, participants were asked first to copy the complex figure. Then, after 3 min and 30 min periods, without previous warning, they were asked to freely reproduce the figure from memory. We used the total score for each recall (Immediate and Delayed, /36) [66].The DMS48, on the other hand, is a visual recognition test in which a series of 48 stimuli is presented to the participants. In a first phase for each image, they are asked to say whether or not they are made up of at least three colors. Then, and again without prior warning, two forced-choice recognition phases are administered after 3 min and 60 min period, presenting target items mixed with distractors. We report here the number of correct recognitions (Immediate and Delayed/48).
Amyloid PET imaging
Participants underwent a PET imaging procedure using a florbetapir (18F-AV–45 [Amyvid™, Avid Radiopharmaceuticals]) injection in order to detect amyloid plaques in the brain [67]. Focusing on targeted brain regions (i.e., left and right precuneus, anterior cingulum, posterior cingulum, parietal, temporal, and orbitofrontal cortex) and normalized with the values of cerebellar and pons regions, a standardized uptake value ratio (SUVr) has been computed for every individual using the CATI platform (Centre d’acquisition et traitement des images, http://cati-neuroimaging.com). The details of the imaging procedure and SUVr threshold are presented in previous studies [6, 68].
FDG-PET imaging
FDG-PET was performed at baseline to asses regional brain metabolism in participants. Analyses especially targeted four bilateral brain regions [6] previously reported as particularly affected in AD: posterior cingulate cortex, inferior parietal lobule, inferior temporal gyrus [59, 69] and the precuneus. These regions of interest (ROI) means were averaged into a single composite FDG-ROI used in subsequent analyses.
Statistical analyses
To evaluate the influence of baseline AD biomarkers on EM evolution for a 2-year follow-up, we performed separate generalized linear mixed models (GLMMs) for each of 26 cognitive measures. GLMMs are statistical models that allow to study the effects of different variables and their interactions on one specific outcome (e.g., a cognitive test score). These models are well suited for longitudinal assessments as they inherently take into account the repetition of measures in the same participants, and then their correlation structure [70]. A link function was chosen regarding the mechanisms underlying the data generation using logarithm for count data, logit for binomial data and identity for continuous data. Demographic variables (i.e., age, sex, and education), time point (i.e., baseline, one year or two years), as well as amyloid and glucose metabolism were included in the models as fixed effects, and participant as random effects. We also included interaction between both biomarkers in order to study their concomitant impact on EM measures (e.g., impact of the glucose metabolism is globally stronger on EM measures with a high amyloid value than with a low amyloid value); interaction of each biomarker with time to evaluate if baseline biomarkers impact on EM measures was different across time (e.g., impact of the baseline amyloid load is stronger on EM measures at two years of follow-up compare to baseline); and interaction between both biomarkers and time to investigate the different effects of biomarker concomitant impact on EM measures across time (i.e., to evaluate if the concomitant impact of amyloid and glucose metabolism is more stronger at two years of follow-up compare to baseline). Additional non-linear effects of continuous independent variables were tested to compare to linear effects alone when the inspection of scatterplots between EM measures and each continuous independent variable seems to indicate non linearity shape. Main effects and interaction were tested using type II likelihood ratio tests. Cohen’s f2 were calculated using the marginal R2 [71] to estimate effect size. p-values were corrected for multiple comparisons using the Benjamin-Hochberg method.
The participants’ educational level was dichotomized between high (≥12 years of education, equal to or higher than high school diploma) versus moderate to low (<12 years, below high school diploma).
Statistical analyses were performed using R 3.5.0.
RESULTS
Population characteristics
Among all of the 318 participants included at baseline, 317 had both Amyloid and FDG PET measures available, which were included in the analyses. After one year of follow-up, 296 subjects were still included in the cohort, and 282 after two years (see Table 1).
Description of population at baseline
Counts, percentages, means, and standard deviations are shown for the whole INSIGHT-PreAD sample. Values are expressed as Mean values±Standard Deviation [minimum; maximum]. Education: High ≥12 years of education. MMSE, Mini-Mental State Examination.
Our population sample was aged from 70 to 85 years old (mean = 76.03±3.48) and participants were predominantly female (63.41%) with a high educational level (67.82%). At baseline, MMSE scores ranged from 27 to 30 (mean = 28.66±0.95).
EM performances all along the follow-up are presented in Table 2.
Memory tests performances in the Insight-PreAD Cohort
Scores, Median [First Quartile; Third Quartile].
Relationship between EM performances and biomarkers
Results of GLMMs for each EM measures are presented in the Supplementary Material. There were no significant main effects of the FDG ROI mean value on any memory score regarding verbal and visual modalities with and without correction for multiplicity. A non-linear effect of Amyloid PET SUVr was found for several EM measures. Thus, a squared effect of SUVr was added in GLMMs for some MBT (Immediate and Delayed Source, Intrusions, Prior list intrusions and Extra list intrusions), FCSRT (TR, Index of cueing, FR Delayed, TR Delayed, Intrusions and Perseverations), and Rey-Osterrieth (Immediate and Delayed Recall) measures. However, there was still a significant main effect of the Amyloid PET SUVr value in two out of four memory tests, i.e., the MBT and the DMS48 after correction for multiplicity. Regarding the MBT, a higher SUVr value was associated with lower scores on the MBT FR of both lists (A + B), both in the immediate and delayed conditions (p = 0.036 and p = 0.019, respectively; Fig. 1). Likewise, a higher SUVr value is associated with lower DMS48 Immediate (after 3 min) and Delayed (after 1 h) scores (both p = 0.019; Fig. 1). Nevertheless, trends can be noted on some measures of FCSRT: Immediate recall and FR scores (both p = 0.068), and in delayed FR (p = 0.077).

Estimated Marginal Means of EM measures associated with amyloid SUVr values. Only scores with significant corrected p-values were shown. Estimated Marginal Means and their confidence intervals were calculated from GLMMs without interactions involving amyloid SUVr. These figures shown the main effect of amyloid SUVr on EM measures. MBT, Memory Binding Test; DMS-48, Delayed Matched to Sample test 48 items.
Furthermore, we found no significant interaction between Amyloid PET SUVr value and FDG ROI mean after correction for multiplicity. The interactions between each of these variables and time were not found to be significant after correction for multiplicity. Interestingly, considering the interaction of Amyloid PET SUVr, FDG ROI mean and Time, a significant effect was observed regarding the total number of intrusions in the MBT, and more precisely in the extra-list intrusions (i.e., items semantically linked but not presented in both lists) (both p = 0.049, Fig. 2).
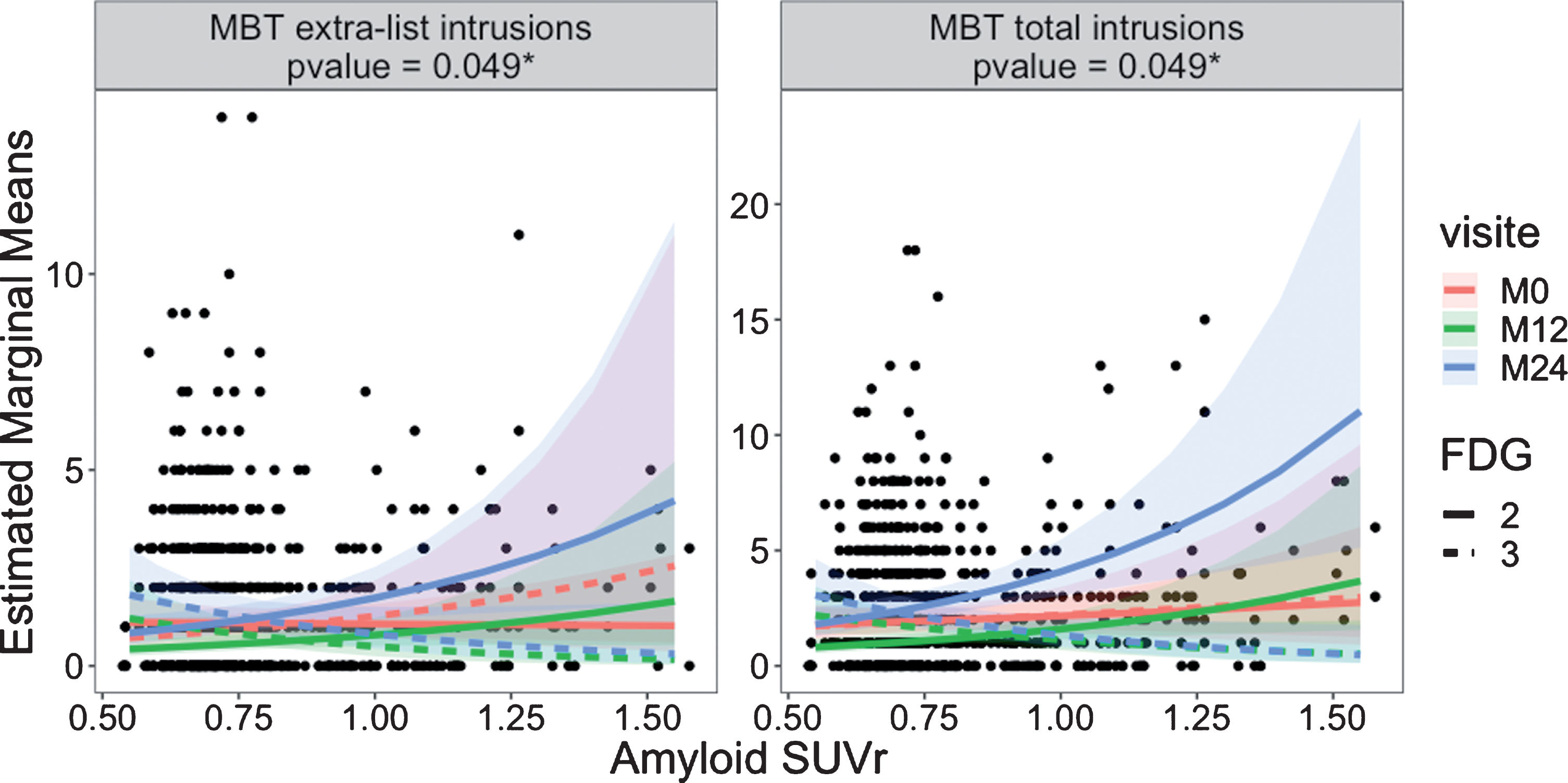
Longitudinal Estimated Marginal Means of EM measures associated with amyloid SUVr values for fixed FDG values (i.e., two and three). Only scores with significant corrected p-values were shown. Estimated Marginal Means and their confidence intervals were calculated from GLMMs. These figures represented the interaction between visit, amyloid SUVr, and FDG on EM measures. MBT, Memory Binding Test. In order to make a 2D representation of the tree-way interaction with two continuous values (i.e., Amyloidosis and FDG) and one categorical (i.e., Time), we calculated the Estimated Marginal Means for arbitrary values of FDG, i.e., 2 and 3.
DISCUSSION
The aim of the present study was to determine whether there is an influence of baseline values of AD biomarkers on the longitudinal evolution of EM in CN elderly participants. The originality of our study consists in the investigation of various EM measures, regarding verbal and visual domains, to shed light on neuropsychological tools that could be used to detect early cognitive decline associated with AD pathology. Our findings show that various types of EM are associated with different levels of brain amyloid load, whereas hypometabolism does not seem related to influence EM performance. Moreover, intrusions seem to be longitudinally impacted by bothbiomarkers.
Baseline biomarkers and EM performances
Regarding verbal EM, we observed a significant effect of amyloidosis (SUVr) on overall FR of both MBT lists during the immediate and delayed conditions. Conversely, the FSCRT was not significantly related to the SUVr level (yet demonstrating a trend for Immediate and Free Recalls, both p = 0.068). This contrast between the significant effect of amyloidosis observed in the MBT but not in the FCSRT is consistent with previous studies [44–46], suggesting a better sensitivity of the MBT to early amyloid-related EM decline. As stated above, the MBT and the FCSRT share some characteristics. Both of them include FR and TR measures in immediate and delayed conditions. Nonetheless, the use of two lists of words in the MBT allows the efficient evaluation of binding capacity, i.e., the integration of independents information from different sources which involves the hippocampal formation [72–75]. The MBT binding measure, i.e., the TIP, has been demonstrated to efficiently separate individuals with dementia and aMCI from CN elderly in cross sectional analyses, and to be highly predictive of incident aMCI and dementia [47, 48]. These findings support the binding hypothesis. Nevertheless, in our study, this measure was not significantly related to biomarker charge. This pattern of results suggests that the MBT TIP cannot be considered an early sensitive score in the preclinical asymptomatic population. Moreover, these results do not support the idea that binding, which would decline before recalls, would be an appropriate measure to detect subtle cognitive changes in the preclinical phase.
Our results show that MBT FR performances were significantly related to the level of amyloidosis in line with previous findings. Indeed, using the FCSRT in longitudinal follow-up, Grober and colleagues [34, 35] already demonstrated that FR would be among the first EM and cognitive measure to decline in the preclinical trajectory. This preclinical FR decline has been related to pathological biomarker levels [17, 36]. Papp and colleagues [46] proposed that the sensitivity of FR versusTR may depend on the preclinical stage so that reduced FR is associated with amyloidosis alone (Stage 1), while decline in TR may represent progression to amyloidosis and neurodegeneration (Stage 2). Reduced FR has been interpreted as an encoding/retrieval impairment [36], which would precede the emblematic AD storage deficit (coined as amnesia of hippocampal type) and could be related to the subtle executive dysfunction observed in amyloid-β+subjects [29, 76–78]. Considering the continuous SUVr values in our participants, we observed the same pattern with the level of amyloidosis significantly impacting verbal EM performance in the MBT FR (Immediate and Delayed), but not in TR. Conversely, we did not observe any relationship between hypometabolism and verbal EM. This, result may seem surprising at first, but we considered a meta-ROI for FDG PET SUVr analyses, composed of ROIs which are associated with clinical AD [59–69]. However, these ROIs are not directly related to memory performance (e.g., unlike medial temporal [79–81] or frontal regions [79, 81–83]). According to the chronological EM evolution proposed above [46] these findings would confirm that our patients are at a very early stage.
Regarding the assessment of EM on the visual modality, we found a significant effect of SUVr level only on DMS48 scores, both immediate and delayed, with a decrease in performance coming with an augmentation of amyloidosis (both p < 0.02). In previous studies, Barbeau and colleagues showed that the DMS48 could be sensitive early in the course of AD [50] due to modifications in the right medial temporal lobe [51]. Indeed, they noticed that before reaching the hippocampus itself, AD pathology chronologically affects sub-hippocampal regions first (i.e., perirhinal cortex and entorhinal) [52–54], which are known to be involved in visual recognition tasks [84, 85]. More recently a longitudinal study has shown that visual recognition memory tasks may be useful in anticipating covert cognitive decline in aMCI patients [86]. Our results confirm that evaluating sub-hippocampal functions using visual recognition memory tasks like the DMS48 test may be useful in detecting early cognitive decline in preclinical stages of the disease.On the other hand, the second visual EM test, the ROCF memory scores, does not discriminate between our participants according to their level of brain amyloidosis or metabolism. A possible explanation of this difference could be related to the underlying cognitive mechanisms of these tasks. Whereas the DMS48 mostly relies on automatic processes of recognition, the ROCF involves executive strategy mechanisms for spontaneous retrieval [87, 88]. As previously stated, in the course of preclinical AD, the onset of decline in EM appears to be years before that in executive functioning [11, 16]. Thus, it seems that episodic processes such as visual recognition memory and retrieval capacity in a memory binding task may be affected earlier compared to other cognitive functions such as executive functioning.
Longitudinal evolution of EM scores
Regarding longitudinal evolution, previous studies report early and subtle EM changes in individuals that are asymptomatic-at-risk for AD [26–28, 90]. These changes occur within a relatively short longitudinal interval (around 18 to 36 months) [26, 89–92]. For a 24-month follow-up, we expected to detect at least a tendency in the longitudinal evolution of our population. However, our results do not show any differential longitudinal effect of amyloidosis, nor of neurodegeneration on EM performance with participants having the same evolution regardless of their biomarker load. This absence of significant differences in the longitudinal investigation could be due to the short follow-up of our study compared to some other previous cohorts we mentioned [26, 89–92]. Alternatively, it may result from the efficacy of compensatory mechanisms that maintain the level of brain functioning despite the existence of structural brain changes. Additional factors should be considered such as longitudinal changes in cortical oscillatory activity in participants positive for amyloid-β deposition, as indicated by the power ratio of EEG [6].
Interestingly, a differential longitudinal effect can be seen in the number of intrusions in verbal EM only in the MBT when combining the two biomarkers. Indeed, our models revealed a significant effect of the interaction between brain amyloid, metabolism and time on the number of intrusions (extra-list and total). Intrusions are typically observed in AD [93–99] and are even presented as a good and sensitive cognitive marker [93, 101]. Before the clinical onset, recent studies demonstrated that intrusions could be good markers of future progression to MCI and mild dementia [101], or identify high amyloidosis in MCI patients [102]. In line with previous studies our findings show that asymptomatic participants produce more intrusions in the MBT in follow-up assessments depending on their AD biomarker load, suggesting that semantically-related intrusions in verbal memory tests can be considered as a good early cognitive marker in follow-up studies.
Altogether, our results support previous research that showed an amyloid-related cognitive decline in EM capacities [15, 30].
Limitations
This study has some limitations. First of all, the duration of the follow-up was only two years after inclusion. In some previous studies, participants begin to demonstrate different cognitive patterns later in the follow-up [103]. Second, in order to compare our participants, we used cognitive data from three time points that have been compared with the baseline biological measurements (FDG and Amyloid PET). Since these variables (level of amyloid, brain metabolism) evolve across time, it would have been interesting to combine and compare biological and cognitive evolutions. Finally, the Effect Sizes (ES, i.e., Cohen’s F2, see Supplementary Material) are relatively weak, in comparison with other studies [26, 104]. For example, Lim and colleagues [90] reported that ES are estimated to range between 0.11 to 0.2 in MCI clinical studies (versus our F2 are range between –0.004 to 0.11). Nonetheless, this could be explained by the inclusion/exclusion criteria of our study which, being quite restrictive in the definition of normal cognition (i.e., integrating several cognitive measures as well as a functional measure), would have made it possible to obtain relatively early population in the evolution of a possible AD pathology. All our subjects were selected to be CN at the beginning of the study [6]. Being normal on our inclusion criteria (i.e., MMSE, CDR, and FCSRT-TR), we expected the participants to perform in the standard range, or with a negligible deviation, on other cognitive battery tests. This allows only short ranges for our cognitive variables within the investigated follow-up period.
Conclusion
To summarize, our aim was to determine the most sensitive EM test associated with AD biomarkers. Our findings suggest that more challenging memory tests (MBT and DMS48) and intrusions in verbal EM (MBT) may be useful for the detection of the transition phase between preclinical and prodromal stages of AD mediated by amyloid deposition among elderly memory complainers. These results are important to consider to target the opportune time window for clinical trial inclusions in the early phase of AD and to detect the very early decline in EM.
INSIGHT-preAD Study Group
Audrain C, Auffret A, Bakardjian H, Baldacci F, Batrancourt B, Benakki I, Benali H, Bertin H, Bertrand A, Boukadida L, Cacciamani F, Causse V, Cavedo E, Cherif Touil S, Chiesa PA, Colliot O, Dalla Barba G, Depaulis M, Dos Santos A, Dubois B, Dubois M, Epelbaum S, Fontaine B, Francisque H, Gagliardi G, Genin A, Genthon R, Glasman P, Gombert F, Habert MO, Hampel H, Hewa H, Houot M, Jungalee N, Kas A, Kilani M, La Corte V, Le Roy F, Lehericy S, Letondor C, Levy M, Lista S, Lowrey M, Ly J, Makiese O, Masetti I, Mendes A, Metzinger C, Michon A, Mochel F, Nait Arab R, Nyasse F, Perrin C, Poirier F, Poisson C, Potier MC, Ratovohery S, Revillon M, Rojkova K, Santos-Andrade K, Schindler R, Servera MC, Seux L, Simon V, Skovronsky D, Thiebaut M, Uspenskaya O, Vlaincu M.
INSIGHT-preAD Scientific Committee Members
Dubois B, Hampel H, Bakardjian H, Colliot O, Habert MO, Lamari F, Mochel F, Potier MC, Thiebaut de Schotten M.
Footnotes
ACKNOWLEDGMENTS
The INSIGHT-PreAD study was promoted by INSERM in collaboration with ICM, IHU-A-ICM and Pfizer and has received a support within the “Investissement d’Avenir” (ANR-10-AIHU-06). The study was promoted in collaboration with the “CHU de Bordeaux” (coordination CIC EC7), the promoter of Memento cohort, funded by the Foundation Plan-Alzheimer. The study was further supported by AVID/Lilly. This research publication benefited from the support of France Alzheimer.