
Abstract
The relationship between Alzheimer’s disease (AD) treatment patterns and healthcare costs is unknown. Administrative claims data from the MarketScan Commercial and Medicare databases covering 2010 through 2016 were used to identify the comorbidities, treatment patterns, and healthcare costs in the three years prior to and one year post medical diagnosis of AD in 21,448 patients with no treatment and 57,970 patients with treatment. Pre-index mean annual costs ranged from $14,228 to $26,876, and post-index mean annual costs ranged from $21,052 to $45,685 depending on age and treatment timing. After adjusting for baseline characteristics, patients 50–100 years old who initiated treatment with an FDA approved drug prior to or concurrent with diagnosis had healthcare costs 9%–19% lower in the year following diagnosis than those who did not receive treatment. Early or concurrent treatment is associated with lower overall healthcare costs in the year following AD diagnosis.
INTRODUCTION
Alzheimer’s disease (AD) is a neurodegenerative condition characterized by progressive memory loss and deterioration of non-memory cognition, including language, as well as motor skills [1]. Symptoms usually begin with mild cognitive impairment (MCI) before progressing to significant cognitive and functional impairment, leading to death within 8–10 years of diagnosis [2, 3]. The Alzheimer’s Association estimates that over 5 million adults in the United States suffer from the disease, and the prevalence is expected to nearly triple by 2050 [1, 4].
There is a high economic burden associated with AD and as the disease progresses, so too does the demand for healthcare resources [5–7]. Individuals with AD require careful clinical care to manage the impact of their diminishing cognitive and functional capabilities on their well-being. Evidence suggests that as the disease progresses, the delivery of care becomes fragmented and costs increase due to the complexity of the care required, often resulting in skilled nursing support or institutionalization [8, 9].
Although there is no treatment that cures or halts the progression of AD, medications have been approved to ameliorate symptoms and boost cognitive performance [10]. FDA-approved medications to treat AD include three acetylcholinesterase inhibitors (donepezil, galantamine, and rivastigmine) and one N-methyl-D-aspartate receptor antagonist, memantine [11]. These medications have been shown to stabilize or slow cognitive, functional, and behavioral decline resulting in reduced healthcare utilization [12–14]. Treatment may improve clinical outcomes and reduce healthcare costs [15, 16], but determining the optimal time to initiate treatment is challenging in a disease where confirmed diagnosis often comes several years after symptoms initially present [17].
Examining the clinical and demographic characteristics, and treatment patterns associated with AD may better inform both clinicians and payers about the natural history of the disease. The purpose of this study was to use administrative claims data to examine the differences in symptoms and healthcare costs between treated and untreated AD patients in the years immediately preceding and following diagnosis, and to examine the effect of treatment timing on healthcare costs following diagnosis. Separate analyses were conducted for patients aged 50–64 years old and those 65–100 years old at diagnosis. A secondary objective was to describe differences observed between these age groups.
METHODS
Study design and data source
This retrospective cohort study utilized de-identified US administrative claims data from the IBM MarketScan® Commercial Claims and Encounters Database and MarketScan® Medicare Supplemental and Coordination of Benefits Database to identify and characterize patients with newly diagnosed AD between January 1, 2010 and December 31, 2016. Patients were stratified by payer type (commercially insured [50–64 years] and Medicare [65–100 years]) to allow for age-group specific conclusions and to account for the clinical differences among early-onset AD patients. The index date was set as the first occurrence of the AD diagnosis code, and the study period comprised the index date, the 36-month baseline period, and the 12-month follow-up period. Patients were also stratified by the presence and sequence of treatment during the study period. Baseline characteristics and outcomes were described for all cohorts.
Data source
The MarketScan Commercial Database contains healthcare experience of over 25 million employees and their dependents (annually), covered under a variety of fee-for-service and capitated health plans. The MarketScan Medicare Database contains the healthcare experience of over 2 million individuals annually with Medicare supplemental insurance paid for by employers. Both the Medicare-covered portion of payment (represented as Coordination of Benefits amount) and the employer-paid portion are included in this database. Each database captures the inpatient medical, outpatient medical, and outpatient prescription drug data for its respective covered population, and together they form a nationally representative sample of insured individuals living in the US [18].
All database records are de-identified and fully compliant with United States patient confidentiality requirements, including the Health Insurance Portability and Accountability Act (HIPAA) of 1996. The databases have been evaluated and certified by an independent third party to be in compliance with the conditions set forth in Sections 164.514 (a)-(b)1ii of the HIPAA privacy rule regarding the determination and documentation of statistically de-identified data. Because the study used only de-identified patient records and did not involve the collection, use, or transmittal of individually identifiable data, Institutional Review Board (IRB) approval to conduct this study was not necessary.
Study population
The primary study population consisted of subjects with claims-based evidence of AD. Patients were eligible for inclusion if they had ≥2 non-diagnostic medical claims with an International Classification of Diseases Ninth/Tenth Revision Clinical Modification (ICD-9/10-CM) diagnosis code for AD[ICD-9-CM: 331.0, 290.0; ICD-10-CM: G30.0, G30.1, G30.8, G30.9, F03.90, and F03.9] in any position on the claim, or ≥1 medical claim with a diagnosis code for AD and ≥1 prescription fill for an AD medication during the study period. AD medications included donepezil, rivastigmine, galantamine, and memantine.
The first AD medical claim was used to define the index date. Patients were required to be ≥50 years but ≤100 years as of the index date and have continuous health plan enrollment with pharmacy coverage for ≥36 months before and ≥12 months after the index date. Continuous enrollment ensures all healthcare resource utilization that results in an insurance claim is captured over the specified time. A unique patient identifier ensured that patients could be followed across changes in payers and transitions between the Commercial and Medicare databases. Patients were excluded if they had evidence of AD or other severe neuropsychiatric conditions (Parkinson’s disease, unspecified psychosis, essential and other forms of tremor, unspecified late effects of cerebrovascular disease, dementia with Lewy bodies, hallucinations, and idiopathic normal pressure hydrocephalus) in the baseline period.
Patients with ≥2 claims for AD and no claims for AD medication were assigned to the untreated cohort. Patients with ≥1 prescription fill of an AD medication were stratified into the following three treatment-timing cohorts: 1) concurrent diagnosis and treatment (prescription filled within±60 days of index date); 2) treatment prior to diagnosis (prescription filled >60 days prior to index date); or 3) diagnosis prior to treatment (prescription filled >60 days after index date).
A control population of patients without any claims-based evidence of AD or other severe neuropsychiatric condition during the study period were identified. Controls were matched 1:1 with AD patients based on age, sex, and geographic region. Control patients were assigned an index date to match the index date of their matched AD patient and were enrolled for the 36-month baseline and 12-month follow-up. This control population was intended to serve as a reference group for added perspective when analyzing costs among AD patient groups; therefore, direct 1:1 matching was employed rather than more rigorous matching which may have been warranted for non-AD versus AD comparative analyses.
Outcomes of interest
Demographic characteristics were captured on the index date. Baseline clinical characteristics were defined based on diagnoses present on baseline period medical claims and included the Charlson Comorbidity Index (CCI) score, AD symptoms, AD precursor conditions (diagnosed altered mental state, amnestic disorder, mild cognitive impairment, and memory loss) and the top 20 most prevalent comorbid conditions at the 3-digit ICD-9-CM code level. All-cause healthcare costs for inpatient services, outpatient services, and outpatient pharmacy services were calculated per-patient per-month (PPPM) and per-year (PPPY) for the baseline and follow-up periods. Costs are the paid amounts of fully adjudicated claims, including insurer and health plan payments as well as patient cost-sharing in the form of copayment, deductible, and coinsurance. All costs were inflated to 2016 US dollars using the medical care component of the Consumer Price Index [19].
Statistics
Study outcomes were reported using descriptive analytic methods. Mean and standard deviation (SD) were reported for continuous variables, and statistical significance was determined using Student’s t-tests. Frequencies and percentages were reported for categorical variables, and statistical significance was determined using Chi-square tests.
Generalized linear models were used to compare all-cause follow-up healthcare costs of the treatment sequence cohorts to the untreated cohort adjusted for baseline characteristics. Non-AD control patients were not included in the modeling, as this was intended to analyze the impact of treatment timing within an AD patient population. Cost models were run with and without the inclusion of baseline cost as an additional covariate. The models used a log link and gamma error distribution functions that conform to the non-normal cost distributions that are typical of healthcare costs.
Inverse probability of treatment weighting (IPTW) was used to adjust for differences in baseline patient characteristics between the three treatment sequence cohorts and the untreated cohort. A propensity model was fit with the four cohorts as the multinomial outcome. A weight was calculated for each patient as the inverse of the adjusted probability of receiving their actual treatment. The cost models were weighted with the IPTWs.
The following covariates were included in all models: age, sex, CCI, symptoms of AD, and comorbid conditions as indicated in (Supplementary Table 1). The alpha level for all statistical tests was 0.05. All data analyses were conducted using SAS version 9.4 (SAS Inc., Cary, NC).
RESULTS
Demographic and clinical characteristics of the study population
A total of 79,418 patients with AD were eligible for study inclusion (Fig. 1). Among the treated patients, 2,372 (4.1%) were aged 50–64 years, and 55,598 (95.9%) were aged 65–100 years. Similarly, among the untreated patients, 944 (4.4%) were aged 50–64 years, and 20,504 (95.6%) were aged 65–100 years.
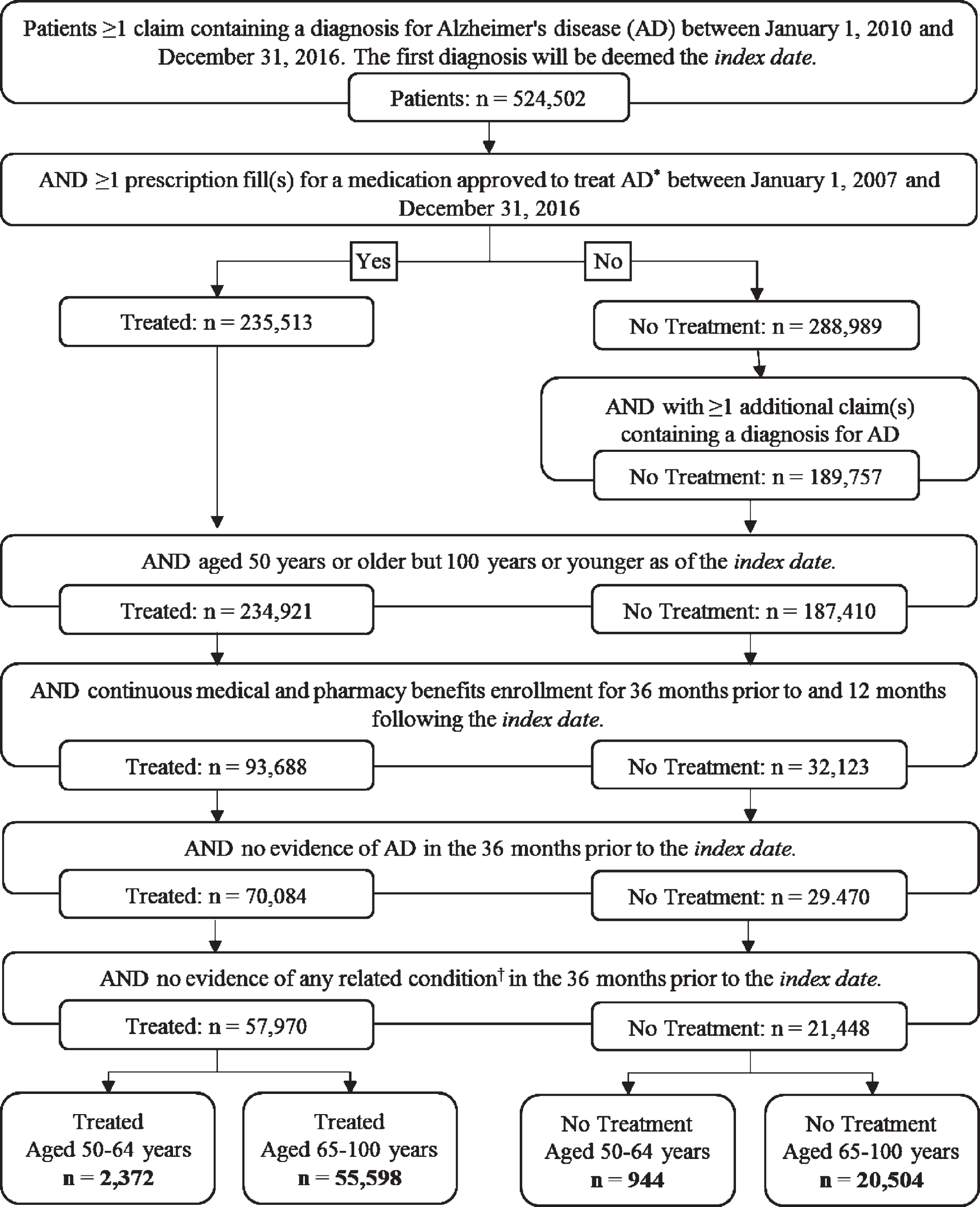
Patient selection. *donepezil, rivastigmine, galantamine, memantine. †Parkinson’s disease, unspecified psychosis, vascular dementia, essential and other forms of tremor, unspecified late effects of cerebrovascular disease, dementia with Lewy bodies, hallucinations, idiopathic normal pressure hydrocephalus, or another exclusionary condition.
Among patients aged 50–64 years, the mean was approximately 60 years old. There were no differences in gender among treated (54.9% female) and untreated patients (53.7% female) (Table 1). The average CCI (mean±standard deviation [SD]) was lower among treated patients than among untreated patients (1.5±2.0 versus 2.1±2.4, p < 0.001), indicating a slightly lower comorbid burden among treated patients. Treated patients were more likely than untreated patients to have AD related symptoms (88.3% versus 69.2%; p < 0.001) and more than twice as likely to have at least one AD precursor condition (69.4% versus 33.4%, p < 0.001). Memory loss was the most common AD precursor condition (treated: 61.3% versus untreated: 22.6%, p < 0.001) followed by MCI (treated: 18.3% versus untreated: 6.1%, p < 0.001). Between the treatment sequence cohorts, all AD precursor conditions and all dementia conditions due to other causes were most common among those who received treatment more than 60 days prior to AD diagnosis and least common among those who received treatment more than 60 days after diagnosis.
Demographic and baseline clinical characteristics of patients with Alzheimer’s disease (AD) aged 50–64 years with commercial insurance
*Bivariate comparisons made between the all treated and no treatment cohorts. †Includes all AD precursor conditions, dementia due to other causes, and other related symptoms. CCI, Deyo-Charlson Comorbidity Index; SD, Standard deviation.
The mean age of patients aged 65–100 was approximately 3 years older (p < 0.001) among untreated patients compared to treated patients (Table 2). The majority of patients were female (treated: 61.1% versus untreated: 65.5%, p < 0.001), and untreated patients had the highest mean CCI score (2.8±2.6, p < 0.001). Among treated patients, 44.9% had a diagnosis for at least one AD precursor condition, compared with 31.5% of untreated patients (p < 0.001). As in the 50–64 cohort, memory loss (treated: 33.5% versus untreated: 14.1%, p < 0.001) and MCI (all treated: 9.6% versus no treatment: 5.1%, p < 0.001) were the most common AD precursor conditions.
Demographic and baseline clinical characteristics of patients with Alzheimer’s disease (AD) aged 65–100 years with Medicare coverage
*Bivariate comparisons made between the treated and no treatment cohorts. †Includes all AD precursor conditions, dementia due to other causes, and other related symptoms. CCI, Deyo-Charlson Comorbidity Index; SD, Standard deviation.
When comparing across the age groups, a higher proportion of patients aged 50–64 years (82.9%) had at least one AD related symptom compared to patients aged 65–100 years (73.5%) (Supplementary Table 2). Patients aged 50–64 years were more likely to have been diagnosed with AD precursor conditions (except for altered mental state), and depressive, mood, or anxiety disorders. Conversely, patients aged 65–100 years were more likely to have dementia due to other conditions.
Healthcare costs and utilization
Across both age cohorts, untreated patients incurred higher unadjusted mean annual healthcare costs during both the period preceding AD diagnosis and during the post-diagnosis follow-up periods than any of the treated subgroups (Fig. 2a). Among patients aged 50–64 years, this was driven by increased annual spending on inpatient services both in the baseline ($4,196±$17,364 versus $10,582±$27,476, p < 0.001) and follow-up period ($7,552±$31,230 versus $22,651±$84,868, p < 0.001) for treated and untreated patients, respectively. Among patients aged 65–100, the differences were more moderate between groups, though untreated patients spent on average $3,524 PPPY more on inpatient costs and $4,988 PPPY more on outpatient medical costs in the follow-up period than treated patients. In both age cohorts, untreated patients were more likely than treated patients to have at least one inpatient admission (50–64:32.5% versus 20.7%; 65–100:45.9% versus 37.3%) and spent more time in the hospital (50–65:0.62 days versus 0.35 days; 65–100:0.66 days versus 0.51 days) in the follow-up period (all p < 0.001).
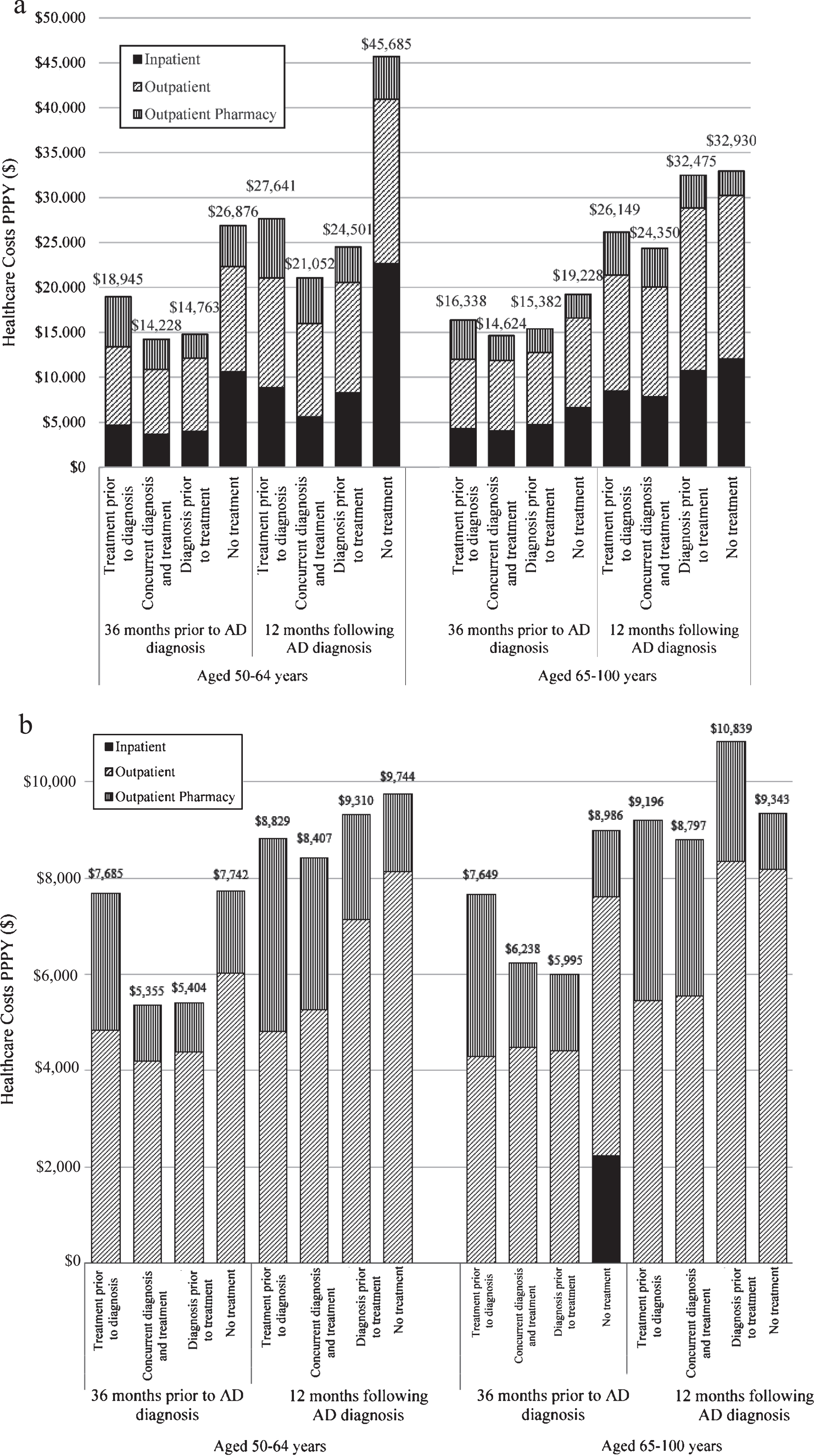
a. Mean annual costs for patients with Alzheimer’s disease (AD) by treatment sequence and age group. PPPY, per person per year. b. Median annual costs for patients with Alzheimer’s disease (AD) by treatment sequence and age group.
Among treated patients aged 50–64 years, total mean annual healthcare costs in the follow-up period were lower for patients with concurrent treatment and diagnosis ($21,052 PPPY) than those who were diagnosed first ($24,501 PPPY) or treated first ($27,641 PPPY). Median annual healthcare costs also followed the same pattern (Fig. 2b). This trend was also observed in patients aged 65–100 years. Healthcare costs in the follow-up period were $24,350 PPPY for patients with concurrent treatment and diagnosis, $26,149 PPPY for patients who were treated first, and $32,475 PPPY for patients who were diagnosed first. This is despite patients who were diagnosed first having the lowest pharmacy costs in the follow-up period among age groups.
When total mean costs are charted PPPM for both age cohorts, with the time of AD diagnosis as month 0, two trends are revealed (Fig. 3A, B). First, all AD patients have a spike in healthcare costs in the months surrounding AD diagnosis, and this spike is largest for untreated patients. Second, compared to matched non-AD controls whose costs remain steady over the study period, healthcare costs for AD patients appear to be rising even prior to diagnosis, diverging in both age groups in the 6 to 3 months prior to diagnosis. The differences in monthly costs between the non-AD controls and AD treatment groups is larger in the younger cohort where the non-AD controls are comparatively healthier given a lower burden of age-related healthcare needs.
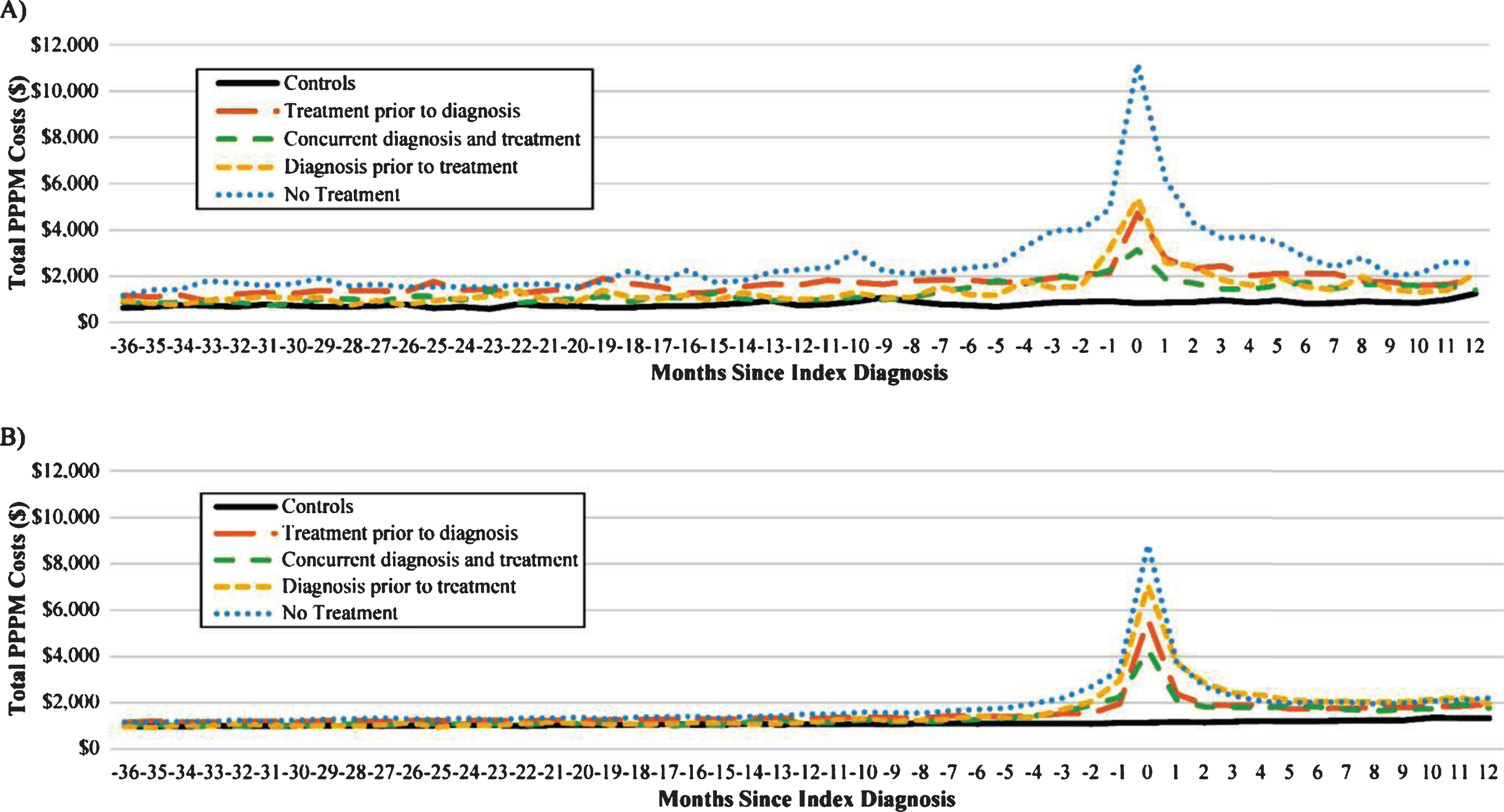
Monthly mean costs for patients with Alzheimer’s disease (AD) by treatment sequence, (A) aged 50–64 years with commercial insurance (B) aged 65–100 years with Medicare coverage. PPPM, per-person per-month.
After using multivariate methods to adjust for differences in baseline demographic and clinical characteristics, among patients age 50–64, those who received treatment concurrently with a diagnosis of AD showed the greatest adjusted cost savings (19%, p < 0.001) compared to untreated patients (Fig. 4 and Supplementary Table 3). Those patients with treatment prior to diagnosis, as well as those with diagnosis prior to treatment, had significantly lower adjusted costs compared to untreated patients (p < 0.05).
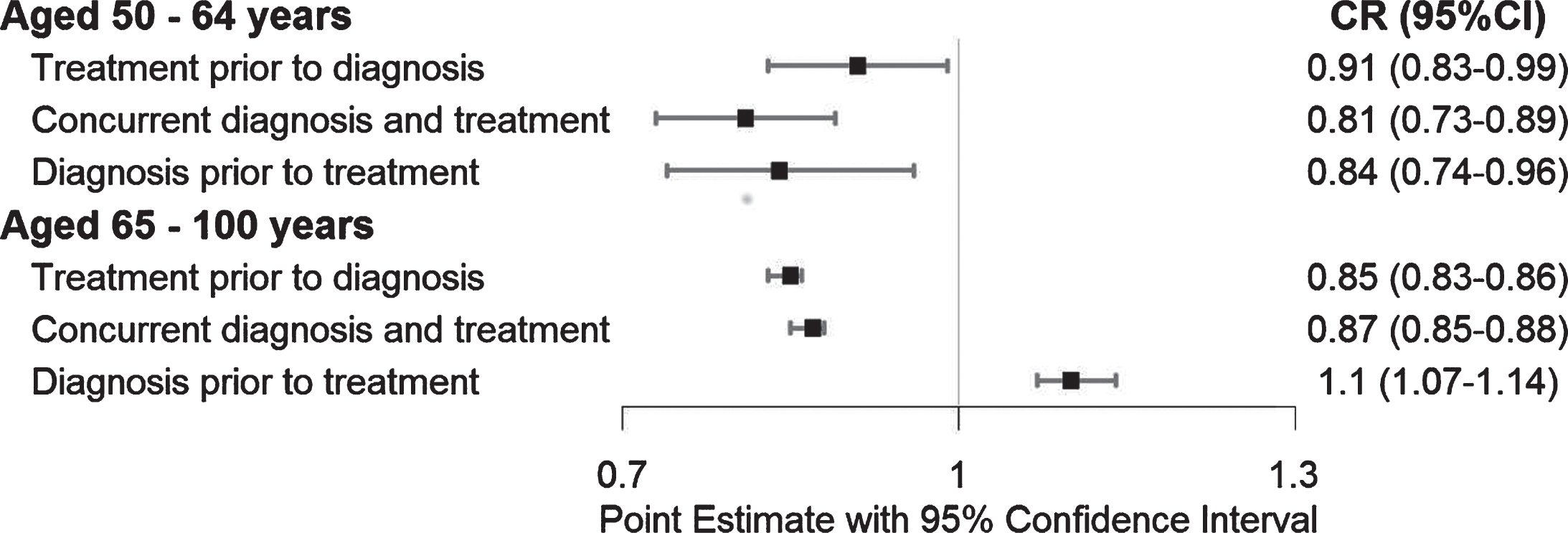
Forest plot of adjusted total post-index all-cause cost ratios. CR, cost ratio; CI, 95% confidence interval.
Among patients aged 65–100, those who received treatment first and those with concurrent diagnosis and treatment cost approximately 15% less than untreated patients (cost ratios 0.85–0.87; p < 0.001) in the year following diagnosis. Patients who started treatment more than 60 days after diagnosis had healthcare costs 10% higher than those who did not receive treatment (p < 0.001). This finding of a treatment subgroup having higher adjusted costs than untreated patients was seen in the 65–100 age group, but not the 50–64 age group.
These multivariate analyses were performed with and without adjusting for baseline healthcare costs, and this sensitivity analysis showed no difference in the overall trends (Supplementary Table 3).
DISCUSSION
In this real-world study of AD patients aged 50–100, patients who received pharmaceutical treatment at least 60 days prior to or concurrent with their diagnosis had significantly lower all-cause medical costs in the year following diagnosis. After multivariate adjustment for baseline symptoms and comorbid conditions that may influence a patient’s propensity to be treated early, early or concurrent treatment was associated with 9% to 19% lower costs when compared with no treatment.
As roughly a quarter of patients diagnosed with AD did not receive treatment in the year following diagnosis, closing this treatment gap has the potential to measurably reduce the cost and burden of AD patients on the healthcare system. It is impossible to determine from claims data what drove the decision not to treat certain patients; however, there are differences in the baseline characteristics which may be suggestive. First, patients who did not receive treatment had a higher overall comorbidity burden, as measured by CCI, than those who did receive treatment. Second, patients who did not receive treatment had a different profile of AD symptoms than treated patients. Prior to diagnosis, untreated patients were more likely to have a diagnosis of altered mental state, delirium, encephalopathy, or a depressive/mood/anxiety disorder than treated patients, and they were less likely to have a diagnosis of MCI, memory loss, or dementia. The lack of memory-related symptoms being diagnosed on a medical claim does not necessarily mean that the patient was free of memory issues. Diagnoses on medical claims depend on both physician evaluation and awareness of symptoms, discernment to include symptom diagnoses on paperwork, and symptom awareness and self-reporting by the patient. All these factors may have contributed to the lower rate of memory-related symptoms in the untreated patients and/or affected physician treatment behavior.
This administrative claims-based analysis was limited to utilizing coded ICD diagnoses on medical claims to determine patient symptoms and AD diagnosis. Detailed physician notes, diagnostic test scores such as the Mini-Mental State Examination (MMSE), and severity of the symptoms are not accessible via claims data. These limitations pertaining to unmeasurable patient characteristics are inherent to all administrative claims-based analyses. ICD diagnosis codes are recorded on medical claims for reimbursement purposes rather than research purposes, so it is important to consider the possibility of misclassification. A recent systematic review of studies comparing dementia coding and an expert-defined reference dementia determination found adequate positive predictive value and sensitivity for AD coding with variability across study methodologies [20]. In the present analysis, a misclassification of illness-induced delirium or memory loss due to other severe illnesses as AD may have contributed to the higher healthcare utilization and costs in the untreated group. One could assume that the misclassification is less likely to affect the treated groups because physicians prescribing treatment for a condition may be more likely to correctly diagnose the condition on the medical claims. The requirement for untreated patients to have more than one medical claim with a diagnosis for AD was included to attempt to ameliorate this potential limitation.
In both age cohorts, patients with a record of MCI or memory loss in the baseline period were more likely to receive treatment prior to or concurrent with diagnosis. However, these AD precursor conditions were twice as likely to be diagnosed in the treated 50–64-year-old cohort compared to the treated 65–100-year-old cohort. One strength of this analysis is the separate description and contrasting of these two age groups which is lacking in the current literature. One possible explanation for the younger cohort having higher rate of MCI and memory loss diagnoses prior to the AD diagnosis is that physicians may be more likely to diagnose MCI and memory loss in in this age group where AD is less prevalent. In older age groups memory loss and MCI may be more often considered normal age-related change and go undiagnosed. Presentation of these symptoms at an earlier age may elicit additional diagnostics and symptom evaluation before the definitive AD diagnosis is recorded.
Understanding the optimal timing of treatment initiation for clinical and cost outcomes is important for informing disease management strategies and is pertinent to all stakeholders. In this analysis, initiating treatment at the time of initial diagnosis was associated with lower adjusted costs, but patients who receive early treatment may differ in other ways from those who do not receive treatment. Physicians who diagnose and treat may be more skillful and provide more cost-effective care. Patients who receive treatment have fewer comorbidities and may therefore be less costly. To reduce the impact of this potential selection bias where treatment timing may be influenced by many underlying measurable and unmeasurable patient characteristics, we utilized a combination of IPTW and multivariate regression to control for differences in baseline characteristics and account for an underlying propensity for early treatment. While it is common to use instrumental variables to account for the endogeneity of the independent variable, a suitable instrumental variable that predicted treatment timing while also being unrelated to costs, was not available in the patient claims data. Therefore, IPTW and multivariate regression were chosen as the best approach to analyze the association. One of the greatest strengths to this analysis is the utilization of these multivariate modeling techniques to control for patient characteristics that may have contributed to cost differences. However, there remains the limitation of unmeasurable confounding due to factors that are not recorded in administrative claims data, such as physician attributes and symptom severity.
In the cost analysis, two differences stood out between the age cohorts. First, the 50–64 no treatment cohort had substantially higher inpatient costs than any other subgroup though they were also less likely to have an inpatient admission than the older cohort. Further analysis could determine if this was due to differences in conditions being treated or differences in negotiated costs of care between commercial and Medicare payers. Second, among patients aged 65–100 years, those who were treated after AD diagnosis had significantly higher adjusted all-cause costs in the follow-up period compared to untreated patients. This can be observed in the unadjusted PPPM costs three to four months into the follow-up period where patients treated after diagnosis experience higher costs than those untreated. This increase may be explained by higher follow-up healthcare utilization and medication costs during the period when physicians are starting patients on treatment.
The limitations of this study are similar to other administrative claims-based studies. First, although the MarketScan Databases are comprised of a variety of employer-sponsored health plans, the data generated from this study may not be generalizable to the broader Medicare population, particularly those receiving traditional, fee-for-service Medicare. Second, claims are designed to track health care services rendered by providers for administrative purposes and are subject to miscoding and under-coding errors. Third, pharmacy claims represent the filling of a prescription, but this does not ensure the medication was taken as prescribed. Fourth, although patients were required to have 36 months pre-index enrollment without an AD diagnosis it is still possible that patients may have received AD diagnoses more than 36 months prior and have been misclassified as incident cases. Fifth, the findings from this study may not be generalizable to those with less stable health insurance due to the requirement of 36-months pre-index and 12-months post-index enrollment in benefits. In addition, the 12-month post-index enrollment requirement inherently limited our analyses, and the generalizability of findings, to those who survive at least 12 months following the AD diagnosis. Finally, claims data do not capture all factors relevant to predicting the likelihood of early treatment, such as physician awareness, social and family interactions, etc.; therefore, there may be residual, unmeasurable confounding factors not accounted for by the multivariate modeling.
In this study of the real-world analysis, we found that initiating treatment at the time of, or prior to, initial diagnosis is associated with lower costs in the year following AD diagnosis. AD patients exhibit a high burden of AD-related symptoms in the three years preceding AD diagnosis suggesting an opportunity for early treatment targeting to improve patient outcomes. These economic results may help inform early disease management strategies to improve the future delivery of treatment and reduce the demand for healthcare resources following diagnosis.