
Abstract
Precision medicine (PM) is an evolving scientific renaissance movement implementing key breakthrough technological and scientific advances to overcome the limitations of traditional symptom- and sign-based phenotypic diagnoses and clinical “one-size-fits-all, magic bullet drug development” in these largely heterogeneous target populations. It is a conceptual shift from ineffective treatments for biologically heterogeneous “population averages” to individually-tailored biomarker-guided targeted therapies. PM is defining which therapeutic approach will be the most effective for a specific individual, at a determined disease stage, across multiple medical research fields, including neuroscience, neurology and psychiatry. The launch of the Alzheimer Precision Medicine Initiative (APMI) and its associated cohort program in 2016—facilitated by the academic core coordinating center run by the Sorbonne University Clinical Research Group in Alzheimer Precision Medicine (Sorbonne University GRC n°21 APM)”—is geared at transforming healthcare, conventional clinical diagnostics, and drug development research in Alzheimer’s disease. Ever since the commencement of the APMI, the international interdisciplinary research network has introduced groundbreaking translational neuroscience programs on the basis of agnostic exploratory genomics, systems biology, and systems neurophysiology applying innovative “big data science”, including breakthrough artificial intelligence-based algorithms. Here, we present the scientific breakthrough advances and the pillars of the theoretical and conceptual development leading to the APMI.
Keywords
HISTORICAL DEVELOPMENT OF PRECISION MEDICINE
The incessant quest to tailor treatments to the individual characteristics of each person has been a long intriguing history. The Ayurvedic system of medicine—dating back to about 5,000 years B.C.—was founded on the principle that different body types and constitutions exist, each being characterized by unique characteristics and responses to the environment, and with individual predispositions to illnesses and reactions to treatments. Conceivably, this theory already represented the core concept of what we call today “precision medicine” (PM). Hippocrates of Kos (c. 460 B.C.–c. 370 B.C.) exerted a major impact over the future development of medicine emphasizing the importance of individual characteristics in determining disease prognosis and treatments [1, 2].
Traditional medicine long followed a “one-size-fits-all” approach based on evidence-based treatments. Simply put, larger groups of different individuals with the same clinically phenotyped late-stage diagnosis were expected to respond to the same treatment [3]. In contrast, the evolution toward PM is personalized, preventive, and predictive. Recent breakthrough technological advances in genomic medicine were the foundational cornerstone of individualized treatments. Historically, the Human Genome Project (HGP) (https://www.genome.gov/12011238/an-overview-of-the-human-genome-project/), a large-scale international research effort launched in 1990 to determine the complete sequence of the human genome and to identify the genes that it contains, is considered as the key milestone achievement for genomic medicine [4, 5]. The HGP, alongside the private effort of the company Celera Genomics, released a working draft of the human genome in 2001 [4] and a complete sequence in April 2003, two years ahead of its original schedule [5]. The results of the HGP clearly demonstrated that variations in the human genome may result not only from single nucleotide polymorphisms, but also from insertions and deletions, copy number variations, and structural variants.
PM is distinct from genetic medicine in monogenic diseases in that the former focuses on complex multifactorial diseases, such as cancer, cardiovascular diseases, diabetes, and neurodegenerative diseases (ND), including Alzheimer’s disease (AD), by considering not only genetic but environmental factors as well [3 , 7]. Similarly, the complex nature of drug response is interpreted by PM and precision pharmacology as a result of complex genetic-environmental interactions [8].
Recognizing the significant advances in PM in light of the human genome mapping, the Food and Drug Administration (FDA) published the Pharmacogenomic Data Submissions (2005) Guidance, the first operative regulatory step to the use of PM research in the area of drug development and approval processes. Then, in October 2013, the FDA issued the report entitled “Paving the way for Personalized Medicine – FDA’s Role in a New Era of Medical Product Development” (https://www.fdanews.com/ext/resources/files/10/10-28-13-Personalized-Medicine.pdf) providing an overview of PM from scientific and clinical practice as well as from the regulatory perspective [9]. In the same period, April 2013, the U.S. President Obama announced the Brain Research through Advancing Innovative Neurotechnologies® (BRAIN) Initiative (http://www.braininitiative.org/) with the goal of accelerating the development and application of advanced technologies to significantly transform our understanding of the human brain.
On January 20, 2015, President Obama announced the Precision Medicine Initiative (PMI) (https://obamawhitehouse.archives.gov/precision-medicine), during his State of the Union Address, stressing a series of actions to promote the development of new PM-based technologies and treatments. This was followed, on January 30, 2015, by the landmark publication of “A new Initiative on Precision Medicine” coauthored by the past HGP-leader and current National Institutes of Health (NIH)-Director Francis S. Collins and the Nobel-prize awardee for Medicine and Physiology (1989, for the discovery of the cellular origin of retroviral oncogenes) Harold Varmus in the New England Journal of Medicine [10].
Under the PMI authority, the U.S. federal government took a crucial role in the basic scientific research behind PM. Specifically, a key element of the PMI is the NIH development of the PMI Cohort Program (PMI-CP) and, subsequently, the All of Us Research Program [9] (see the “Background and Rationale of Precision Medicine” section). Moreover, on November 2, 2018, the NIH decided to further increase the support to the BRAIN Initiative, announcing funding of more than 200 new awards, thus accumulating over 220 million. These new awards include highly advanced and competitive research programs (https://www.braininitiative.nih.gov/) (see Fig. 1).
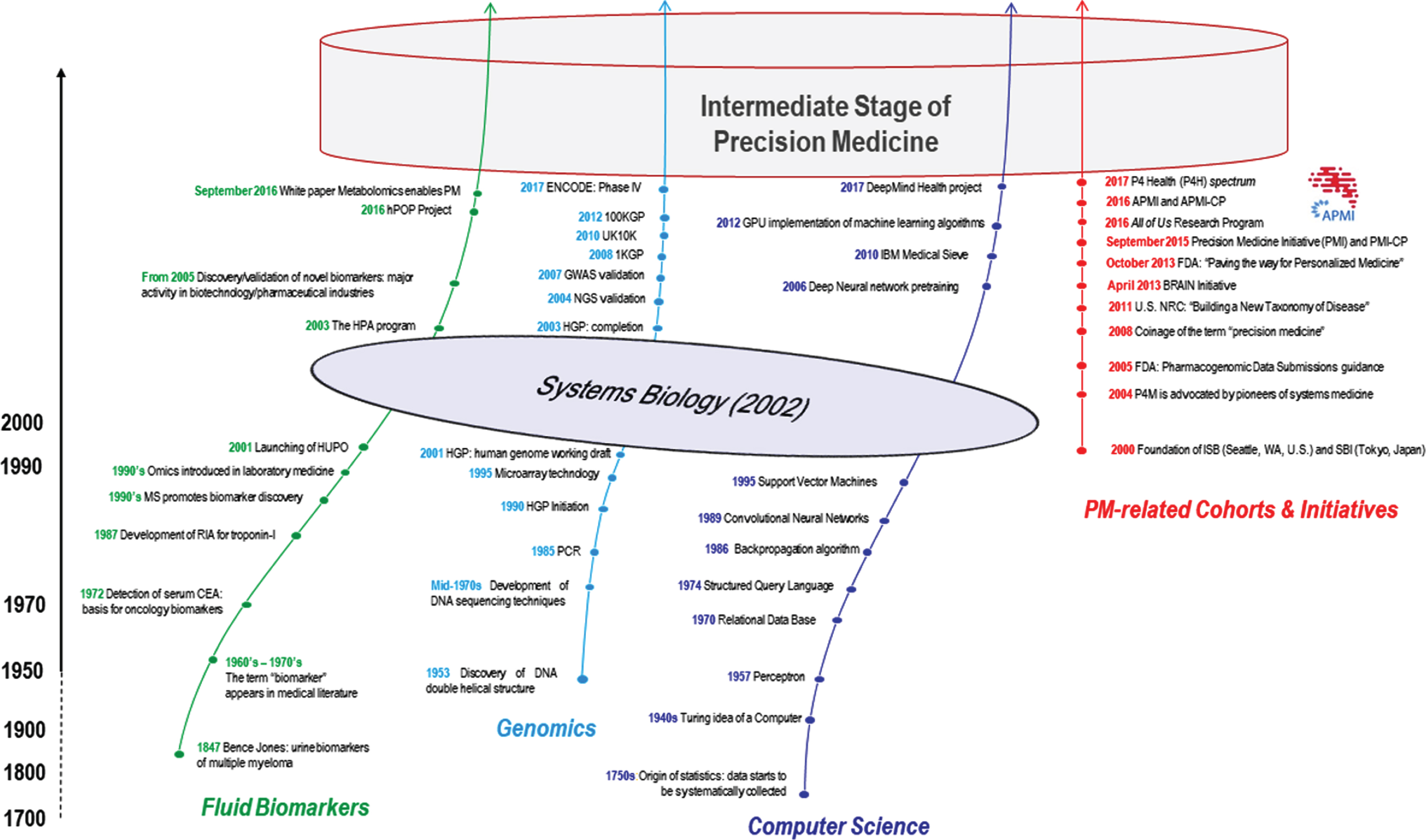
Evolution of PM through breakthrough technological advances. Timelines illustrating the key advances in fluid biomarkers (green line), genomics (light blue line), and computer science (dark blue line) over the last three centuries (1700-present). All of these fields of study contributed significantly (via the proxy passage of system biology [grey ellipse]) to the intermediate stage of precision medicine we are currently witnessing. The red line on the right indicates the timeline of the major collaborative initiatives aimed at implementing the PM paradigm. Notes and abbreviations: On September 2, 2016, a White Paper was developed by the “Precision Medicine and Pharmacometabolomics Task Group”, belonging to the Metabolomics Society (available at http://metabolomicssociety.org/board/scientific-task-groups/precision-medicine-and-pharmacometabolomics-task-group) to discuss the best state of-the-art metabolomics platforms and strategies for collecting, understanding, and disseminating metabolomics data in big precision medicine initiatives (see [101]. 1KGP, 1,000 Genomes Project. A collaborative effort, developed between 2008 and 2015, that contains data for 2,504 individuals from 26 populations. It currently represents the largest public catalogue of human variation and genotype data (available at http://www.internationalgenome.org/about#1000G_PROJECT). 100KGP, 100,000 Genomes Project. A UK-based project aims at sequencing 100,000 genomes from UK National Health Service (NHS) patients, with the ultimate goal to introduce whole genome sequencing into routine clinical practice in the UK (available at https://www.genomicsengland.co.uk/the-100000-genomes-project/). It was launched in late 2012. APMI, Alzheimer Precision Medicine Initiative (available at https://www.apmiscience.com/); APMI-CP, Alzheimer Precision Medicine Initiative Cohort Program (available at https://www.apmiscience.com/). ENCODE, ENCyclopedia Of DNA Elements. A public research consortium, supported by the National Human Genome Research Institute (NHGRI), aimed at identifying all functional elements in the human and mouse genomes. The ENCODE Project started in 2003 with a pilot phase focused on 1% of the human genome. Then, two additional phases (ENCODE 2 and ENCODE 3), conducting whole-genome analyses on the human and mouse genomes, were accomplished. After recognizing that supplementary effort was needed to understand the catalog of candidate regulatory elements compiled, the NHGRI funded the fourth phase of ENCODE (ENCODE 4), on February 2017, to further scrutinize its work to appreciate the human and mouse genomes (available at https://www.genome.gov/10005107/the-encode-project-encyclopedia-of-dna-elements/). FDA, Food & Drug Administration; GPU, Graphic Processing Unit; GWAS, genome-wide association study. HBP, Human Brain Project. A European Commission (EC) Future and Emerging Technologies (FET) Flagship, initiated on October 1, 2013, that aims at creating a cutting-edge research infrastructure allowing scientific and industrial researchers to advance knowledge in neuroscience, computing, and brain-related medicine (available at https://www.humanbrainproject.eu/en/). HGP, Human Genome Project (available at https://www.genome.gov/12011238/an-overview-of-the-human-genome-project/). HPA, Human Protein Atlas. A Swedish-based research program initiated in 2003 aiming at mapping all the human proteins in cells, tissues, and organs using integration of omics technologies, including mass spectrometry-based proteomics, transcriptomics and systems biology (available at https://www.proteinatlas.org/about). hPOP, Human Personalized Omics Profiling project. A project designed to study the variance of molecular biomarkers across a large number of healthy volunteers. A multiomics approach is used to explore the genome/epigenome, transcriptome, proteome, and metabolome of the healthy individuals (available at http://med.stanford.edu/hpop/about_hupo_study.html). HUPO, Human Proteome Organization. An international scientific organization, launched on February 9, 2001, supporting proteomics research via international collaborations by promoting the development of new explorative methodologies (available at https://www.hupo.org/about-hupo). IBM, International Business Machines Corporation. The American multinational information technology company headquartered in Armonk, New York, U.S. manufacturing computer hardware, middleware, and software (available at https://www.ibm.com/). ISB, Institute for Systems Biology. A non-profit biomedical research organization established in Seattle, WA, U.S., by Dr. Leroy Hood, in 2000, pioneering the paradigm of systems biology (available at https://systemsbiology.org/). NGS, next-generation sequencing; NRC, National Research Council; P4H, P4 Health spectrum: a Predictive, Preventive, Personalized, and Participatory continuum for promoting health span; P4M, Predictive, Preventive, Personalized, and Participatory Medicine (see the Glossary reported in Table 3 for the definition); PCR, polymerase chain reaction; PM, precision medicine; PMI, Precision Medicine Initiative; PMI-CP, Precision Medicine Initiative Cohort Program. SBI, Systems Biology Institute. A non-profit private research institution established in Tokyo, Japan, by Dr. Hiroaki Kitano, in 2000, with the aim of promoting systems biology research and its application to medicine and global sustainability (available at http://www.sbi.jp/aboutSBI.htm). UK10K, United Kingdom 10,000 Genomes. A UK-based project that used a low-coverage whole-genome sequencing strategy to identify variants from approximately 4,000 healthy individuals from two well-studied British cohorts. In addition, causal mutations for three types of diseases (rare disease, severe obesity, and neurodevelopmental disorders) were investigated by high-coverage exome sequencing of 6,000 patients (available at https://www.uk10k.org/ and https://www.uk10k.org/goals.html). The project started in late 2010.
In summary, from a historical perspective, it would appear that modern PM is grounded in what can be called a holistic, exploratory systems-level approach, as originally proposed by the Ayurvedic system of medicine and by Hippocrates. Although the original idea of PM dates back millennia, breakthrough advances in biomarker discovery and validation—highlighted by technological advances in multimodal high-throughput “omics” and “multiomics” sciences as well as in neuroimaging and advanced experimental/computational methods—are anticipated to pave the way toward their application in preventing and treating common complex diseases.
Breakthrough in biomarker development
During the past decades, fluid biomarkers have been increasingly implemented in clinical and research routine in different fields of medicine (see Fig. 1). During the 1960s, the term “biomarker” started to consistently appear in the medical literature based on the biochemical abnormalities associated with the presence of several different disease conditions [11 –15]. Apart from AD (which is the focus of the current review and perspective), a striking example in the field of neurodegenerative research is the measurement of progranulin concentrations in plasma/serum for the identification of carriers of progranulin mutations [15]. In the 1990s, accelerator mass spectrometry, able to accelerate ions to extremely high kinetic energies before mass analysis, was introduced to facilitate biomarker discovery in biological samples, thus paving the way for the subsequent introduction of “omic” technologies in clinical chemistry and laboratory medicine, which can be dated back to the early 1990s [16]. In brief, the first high-throughput “omic” technologies were aimed at the non-targeted and non-biased detection of genes (genomics), proteins (proteomics), transcripts (transcriptomics), metabolites (metabolomics), and lipids (lipidomics) in clinical samples. The most peculiar aspect of these approaches is that a complex system can be described more thoroughly only if considered as a whole, according to the evolving hypothesis-free exploratory paradigm of systems biology, also referred to as network biology or integrative biology [17, 18]. In April 2003, the International Human Genome Sequencing Consortium completed the HGP (https://www.genome.gov/11006929/2003-release-international-consortium-completes-hgp/), therefore initiating the discovery of genetic disease biomarkers. As of 2005, discovery, development, and validation of novel biomarkers have become a major scientific activity, not only in academia but also in biotechnology and the pharmaceutical industries [19, 20].
Breakthrough in computer science: historical overview
PM relies substantially on big data as well as on bioinformatic analysis of large datasets. More advanced medical areas, such as oncology, already take advantages of big data collection and sharing within the research community. Moreover, these massive amounts of data and their integration into a single disease modeling may provide opportunities to develop advanced methods and, eventually, improve clinical diagnosis and predict patient outcomes.
Due to the development of big data platforms, new challenges arose. It is estimated that the overall size of data for research purposes and healthcare will reach 25,000 petabytes in 2020 [21]. This is relevant to PM which aims at gathering large amounts of information, storing and analyzing them through the systems medicine approach, which is exponentially growing thanks to advanced technologies and computational power.
At the root of computer science, the theory of statistics provides a first guidance on the choice between alternative possibilities, which is a foundation for the interpretation of data, such as demographics in the late 17th century [22]. Computer science is an evolving field that already contributed to medical advances. By the mid-20th century, Turing had developed the idea of a computer, which radically supported the storing and processing of data [23]. Later, in 1970, Codd proposed a digital database based on the relational model of data [24] which helped the storage and organization of data and is still the standard, nowadays, through the use of the Structured Query Language (SQL), created in 1974 [25]. While hardware was becoming more efficient, being able to store an increasing amount of data and process them more quickly, computer scientists were developing the algorithmic theory to process even larger and highly complex datasets. Machine learning opened up the field to more intricate and detailed brain-inspired algorithmic research, with the creation of the artificial neural networks (ANN) modeling. These are frameworks enabling different artificial neurons, the perceptron [26], to work together using the Werbo’s back propagation algorithm, proposed in 1975 [27]. The creation of ANN computing logical functions facilitated the exploration of neural computation in the 1940s [28], including models by which brain networks might learn via supervisory feedback [29] or efficiently encode environmental statistics in an unsupervised manner [30] (see Fig. 1).
Support vector machines (SVM) algorithm is of great interest [31] since it is able to generalize the classification of unlabeled data and is an efficient tool for processing large amounts of data.
A new class of deep, feed-forward ANN, inspired by the animal visual cortex—the convolutional neural network (CNN)—facilitated the image processing thanks to its sparse connectivity between neurons, as one example. It was first theorized in the 1980s and, finally, implemented and generalized for several types of data using the latest graphic processing unit (GPU) [32] by 2012. This type of deep ANN paved the way to a new subdiscipline of machine learning, deep learning, that was able to make diagnoses as accurate as those made by physicians in several clinical fields [33].
Presently, several companies are trying to exploit the potential of artificial intelligence to move away current medical practice from general solutions toward personalization and precision. For instance, IBM Watson developed a special program for oncologists to provide clinicians with personalized treatment plans [34]. In addition, IBM launched the Medical Sieve program to develop a “cognitive health assistant” with diagnostic abilities for radiological images (https://researcher.watson.ibm.com/researcher/view_group.php?id=4384).
In conclusion, the latest theoretical and practical advances of computer science are expected to substantially reduce medical errors and enhance and accelerate the clinical workflow, ultimately informing differentiated precision therapies and improving short- and long-term health outcomes.
Figure 1 illustrates the evolution of PM through breakthrough technological advances. Key progresses in fluid biomarkers, genomics, and computer science are reported, over the last three centuries, together with the timeline of the crucial collaborative initiatives implementing the PM paradigm.
DEFINITION OF PRECISION MEDICINE
There have been major advances in high-throughput genomic technologies, which are paralleled by significant declines in their operational costs. In addition, clinicians have become increasingly aware that phenotypically similar diseases may be significantly heterogeneous in terms of pathophysiological underpinnings. For this reason, interest in the clinical implementation of PM, defined by the NIH as “an emerging approach for disease treatment and prevention that takes into account individual variability in genes, environment, and lifestyle for each person” (https://ghr.nlm.nih.gov/primer/precisionmedicine/definition), is gaining momentum.
The term “precision medicine” was coined by the Harvard Business School strategist Clayton Christensen in 2008. The original concept was theoretically rooted in the possibility to unambiguously identify the cause(s) of a disease without having to rely on intuition. In 2011, the Committee on A Framework for Developing a New Taxonomy of Disease, convened by the U.S. National Research Council, proposed a new disease taxonomy based on molecular information rather than on the traditional symptom-based approach [35]. Notably, the Committee report was titled “Toward Precision Medicine. Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease” [36].
Disease taxonomy in clinical medicine has traditionally relied on the International Classification of Diseases (ICD), a general framework proposed by the World Health Organization (established in 1948 as a specialized agency of the United Nations that is concerned with international public health) more than one century ago, to track disease incidence in a consistent manner. The ICD has been extensively used in clinical practice as a basis for standardized diagnoses. Moreover, it has been largely employed by financing stakeholders (e.g., insurance companies, national health services) to guide reimbursement practices. As of 2011, the Committee on A Framework for Developing a New Taxonomy of Disease introduced two data repositories (termed “Information Commons” and “Knowledge Network”) to integrate basic research into the molecular bases of diseases with clinical information and patient outcomes. This infrastructure is deemed to play a key role in envisioning a radically new taxonomy paradigm in both biomedical research and clinical medicine [36].
Information on the underlying causes of different illnesses is expanding rapidly, and the “Knowledge Network” of disease aims at summarizing and sharing this growing amount of data between healthcare providers, researchers, and the public. This system is grounded in the “Information Commons”, a repository in which individual molecular data are linked to clinical history, socio-demographic variables, and medical outcomes. The available dataset will be continuously enriched by updates in the participants’ health records as well as by the dynamic contribution from the research community. The data repository termed “Information Commons” shares major similarities with a geographical information system (GIS) like Google Maps. GIS is an infrastructure in which satellites send signals to global positioning system (GPS) receivers; in turn, the GPS receiver calculates the exact latitude/longitude/elevation position at which it is currently located. Similar to Google Maps, the “Information Commons” is an information system capable of capturing, storing, analyzing, managing, and presenting biomedical data in a multilayer manner, ultimately allowing the extraction of complex interrelationships that cannot be captured from each layer alone [36] (see also https://www.nap.edu/resource/13284/precision-med-final.pdf).
In keeping with the proposed new disease taxonomy, the main goal of PM is to identify specific subsets of patients whose illnesses share the same molecular basis, ultimately having the highest likelihood to benefit from a specific therapeutic procedure. The ideal objective of identifying “the best available care for each individual” will be achievable only through the linking of large molecular datasets to individual patient variables. Extensive validation of the originally identified associations will also be needed [36].
Admittedly, the seeds of PM, i.e., those of an individualized treatment tailored on the individual’s specific biological makeup, can be traced back to more than one century ago. A typical example is blood transfusions, which have been (and continue to be) guided by individual blood typing. Needless to say, the formidable advances recently occurring in several fields, e.g., laboratory methods, computational tools, large repositories of biological samples, and high-resolution imaging techniques, will allow PM to be extended to a large number of clinical areas, hopefully resulting in radically renewed and highly effective therapeutic approaches [10, 37].
BACKGROUND AND RATIONALE OF PRECISION MEDICINE
PM questions the traditional “one-size-fits-all/magic bullet therapy” concept, according to which treatments are devised for the “average patient”, into individually-tailored therapeutic modalities guided by specific differences in individual’s genes, environments, and lifestyles [3, 6]. Seminal applications of PM can be found in oncology, in which patients with breast, lung, and colorectal cancers, as well as melanomas and leukemias routinely undergo molecular testing for identifying therapeutically actionable aberrant biological pathways that drive malignant transformation. In this scenario, the objective is to improve survival outcomes and minimize treatment-related adverse events.
Undoubtedly, the large-scale implementation of PM will require strict, coordinated collaborative efforts from different stakeholders in the public and private sectors [3, 6]. In this context, the PMI (https://obamawhitehouse.archives.gov/precision-medicine), implemented and financially supported in the U.S. beginning during the Obama’s administration, has the objective to engage over 1 million individuals whose biological data (genetic variants, microbiota) will be cross-linked with both their lifestyle/environmental information and individual clinical variables (including patient-generated data from biosensors or wearable devices).
The following milestones will be critical to the success of the initiative: 1) a secure data access accompanied by a rigorous privacy protection; 2) the availability of data to qualified researchers who may use them to exercise their creative thinking with an a posteriori approach or, alternatively, to test their a priori hypotheses; 3) a modernization of the regulatory landscape, in conjunction with the FDA, that will facilitate the rapid translation of discoveries from bench to bedside.
In the context of the PMI, the All of Us Research Program (https://allofus.nih.gov/) has the specific goal to extend PM to all fields of clinical medicine through the enrolment of a cohort comprising at least 1 million subjects from the U.S. To this aim, both biological specimens and participant-provided information, including environmental, physiologic, and health data, will be collected. The study is expected to span over at least 10 years, with the first 5-6 years being devoted to active enrolment. Engagement of children is expected within one year of program launch.
The sample size of the All of Us Research Program will be sufficiently large to increase our understanding of a broad spectrum of disease conditions and health outcomes, ultimately offering unprecedented opportunities. These will include the possibility to study the intricate relationships between environmental and genetic risk factors, the clarification of the biological underpinnings of individual response to drugs, the implementation of biosensors, electronic health (e-Health) and mobile health (m-Health) technologies, the discovery and validation of biomarkers of disease risk and resilience, the validation of new disease taxonomies, and the creation of new clinical trial platforms for targeted therapies.
The All of Us Research Program is designed to involve a number of different stakeholders in the public and private sectors and is aiming to create new strategies to engage research participants and share large amount of clinical data within a highly interactive research framework modeled as a dynamic community. The All of Us Research Program biobank (https://allofus.nih.gov/about/program-components/biobank) has been recently established at the Mayo Clinic in Rochester, Minnesota. The goal of the biobank is to collect, store, and distribute biological specimens to qualified researchers that are willing to unravel the individual differences contributing to disease susceptibility and response to treatment. Besides the biobank, the All of Us Research Program has established a Data and Research Support Center (https://allofus.nih.gov/about/program-components/data-and-research-center), whose aims will be to acquire, secure, organize, and provide qualified access to one of the world’s largest datasets for PM researchers. In addition, a network of health care provider organizations (HPO) (https://allofus.nih.gov/about/program-components/health-care-provider-organizations), including regional and national medical centers, community health centers and medical centers operated by the U.S. Department of Veterans Affairs, will allow interested individuals from the U.S. to join the PMI research study, while ensuring an accurate depiction of the marked diversity of the country.
Globally recognized initiatives provided significant evidence coming from research with autosomal dominant mutation carriers, that the pathophysiological mechanisms leading to neurodegeneration and dementia commenced several years if not decades before the appearance of signs and symptoms. These initiatives provide the groundwork for the application and integration of PM approaches into research and development of ND, including AD. This reform movement is currently evolving at different points across the spectrum of ND through the formation of large-scale interdisciplinary international consortia. The Genetic Frontotemporal dementia Initiative (GENFI) (http://genfi.org.uk/) is a consortium including research sites across Europe (UK, Netherlands, Belgium, France, Spain, Portugal, Italy, Germany, Sweden) and Canada. The aim of the program is to explicate the genetic of frontotemporal dementia (FTD), mainly in individuals carrying mutations in the microtubule-associated protein tau (MAPT), progranulin (GRN), and chromosome 9 open reading frame 72 (C9ORF72) genes. By investigating both individuals who developed clinical signs and symptoms and those at risk of developing clinical phenomenology (as carriers of genetic mutations), it is possible to inspect the development of a certain type of pathophysiology and “disease” from its earliest manifestation. GENFI aims at establishing: 1) biomarkers supporting the diagnosis of the disease at its earliest stage and 2) biomarkers enabling to track disease progression. The Dominantly Inherited Alzheimer Network (DIAN) [38] (https://dian.wustl.edu/about/), an international research organization established in 2008 involving trans-continental institutions in the U.S., South America, Europe, Asia, and Australia, was settled to enroll worldwide individuals with early onset familial AD and non-carrier family members (recruited as control subjects) into a big single research study. DIAN contributed to develop basic science studies, a long-term observational study, and several clinical therapy trials. In particular, the DIAN Observational Study aims at identifying changes in individuals carrying mutations in the Presenilin1 (PSEN1), Presenilin2 (PSEN2), or (APP) genes generating dominantly inherited Alzheimer’s disease (DIAD). The DIAN Trials Unit (DIAN-TU) [39] is an international organization focused on planning and managing interventional therapeutic trials for individuals with and at risk of DIAD. These initiatives form a growing global network that will contribute substantially to the evolution of PM throughout the current intermediate stage.
THE DEVELOPMENT OF THE ALZHEIMER’S PRECISION MEDICINE INITIATIVE
As is the case in most fields of medicine, substantial advancements in detecting, treating, and preventing AD are anticipated to evolve from the generation and implementation of a systematic PM strategy. This approach will likely be based on the success generated in more advanced medical research fields, such as oncology [3 , 7]. Our approach is based on the hypothesis that the disease construct AD is a heterogeneous entity characterized by different multiple genetic and biological subsets. In this regard, the implementation of PM in AD and other ND along the disease spectrum of brain proteinopathies will result in optimized clinical profiles based on biological and genetic features. This approach will produce better responder rates, particularly in early disease-stage clinical trials, thus providing substantial benefits to patients suffering from this devastating disease.
To realize the promise of PM, it is necessary to create a new network with partnerships of several stakeholders cooperating to find novel solutions. This novel network, including academic and community providers, industry, government, consumers, and patient advocacy groups, is expected to help spread pilot initiatives on a national and international scale. For this reason, in order to advance the development of the PM paradigm in AD, the international Alzheimer Precision Medicine Initiative (APMI) and its cohort program (APMI-CP) (Fig. 2), available at https://www.apmiscience.com/, have been recently launched by our consortium at the Sorbonne University and the Pitié-Salpêtrière University Hospital in Paris, France, and conceptually associated with the U.S. PMI and the All of Us Research Program [7].
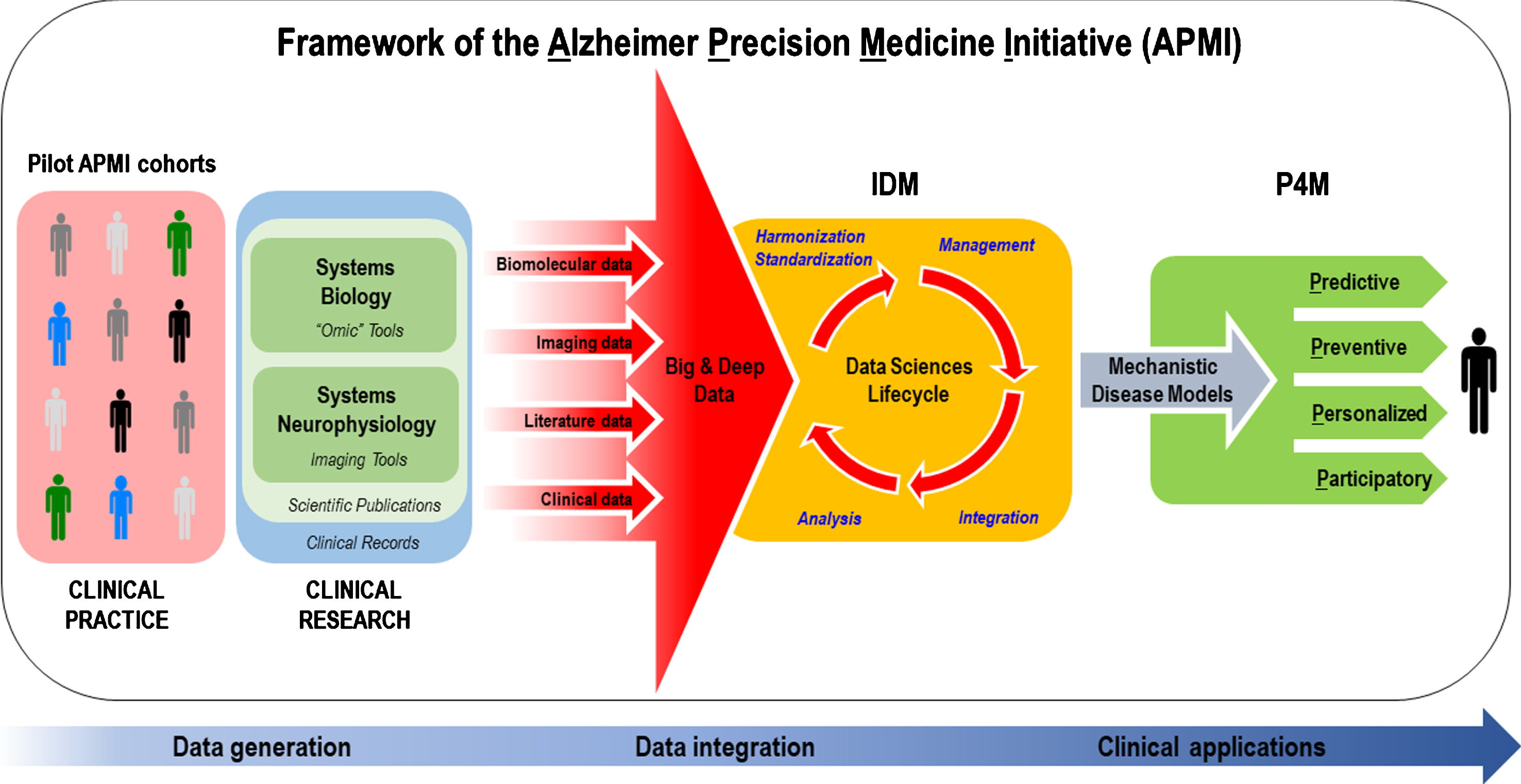
Translational bench-to-bedside data flow within the conceptual framework of the Alzheimer Precision Medicine Initiative (APMI). The IDM-based “Data Sciences Lifecycle” takes advantage of both data-driven and knowledge-driven approaches so that both quantitative data (biomolecular, neuroimaging/neurophysiological, and clinical data) and qualitative data (collected from scientific literature and on-line media), generated through the application of systems biology and systems neurophysiology paradigms, are represented in a harmonized, standardized format to be prepared for proper management within an integrative computational infrastructure. Indeed, the resulting heterogeneous, multidimensional big and deep data are harmonized, standardized, and integrated via computational and data science methods in the form of mechanistic disease models, according to the IDM conception. Disease-specific integrative computational models play a key role in the IDM paradigm and represent the foundations for “actionable” P4M measures in the area of AD and other ND. As a result, the integrative disease models are anticipated to support decision making for: (I) early diagnosis of brain disease progression with mechanistic biomarkers (predictive), (II) screening populations and stratifying individuals at high risk of developing ND based on mechanistic co-morbidities in order to reduce the likelihood of disease and disability (preventive), (III) tailoring treatment to the right patient population at the right time (personalized), and (IV) optimizing “actionable” plans for the benefit of patients based on patient-oriented information gathered in EHR and on patients’ feedback reported in social media. Internet has greatly enabled the participation of individual patients in the healthcare through sharing their experiences in various social media and other online resources (participatory). The output is anticipated to be an “actionable” model that permits the prediction of the trajectory of individual patient-centric detection or treatment within the implementation of the P4M paradigm. EHR, electronic health records; IDM, integrative disease modeling; ND, neurodegenerative diseases; P4M, predictive, preventive, personalized, participatory medicine. Reproduced with permission from [7].
The APMI is an international network of leading interdisciplinary clinicians, scientists, and researchers devoted toward the transformation of Neurology, Psychiatry, and Neuroscience embracing PM, based on complex systems theory [40] (using systems biology [7, 41], systems neurophysiology [7], and systems pharmacology [8]), biomarker-guided integrative disease modeling (IDM) [6, 42], and “big data science” to facilitate health care solutions for brain proteinopathies, protein misfolding disorders, and ND, such as AD (Table 1) [3 , 7]. After decades of failed therapy trials, progress toward the holistic, exploratory systems-based strategy of PM is expected to turn into a new age of biomedical developments hopefully curbing the global AD epidemic in time. Under the APMI umbrella, the estimation of quantitative data-driven models exploring the full spectrum of ND via complex and innovative mathematical/neuroinformatics tools will allow the identification of biochemical, functional, metabolic, morphological, and neuropsychological trajectories of ND, including AD, necessary for the early prediction, prognosis, detection, diagnosis, and prevention, and for precise monitoring of disease-modifying therapies. These outcomes will change clinical practice and the assessment of treatment efficacy in clinical trials, thus paving the way to the development of targeted and biomarker-guided therapies. The APMI International Working Group (APMI-IWG; Principal Investigator Harald Hampel) was created to summon internationally recognized experts in the following areas: blood-based and cerebrospinal fluid (CSF) biomarkers, neurogenetics, neuroimaging and biophysics, bioinformatics, pre-clinical studies, clinical trials development, pharmaceutical industry management, and regulatory affairs.
The main “pillars” of the Alzheimer Precision Medicine Initiative (APMI).The mission of the APMI is to transform Neurology, Psychiatry, and Neuroscience embracing the paradigm of PM based on complex systems theory, using integrative disease modeling to facilitate health care solutions for brain proteinopathies, protein misfolding disorders, and ND, such as AD. This occurs through breakthrough theoretical scientific advances, as follows:
AD, Alzheimer’s disease; IDM, integrative disease modeling; ND, neurodegenerative diseases; P4M, Predictive, Preventive, Personalized, Participatory Medicine; PM, precision medicine.; Modified with permission from [7].
Translational neuroscience research programs
The APMI facilitated the development and launch of a number of pioneering translational neuroscience research programs, within an interdisciplinary network. Key part of it was the integration of systems biology [7, 41] (Fig. 3A) and systems neurophysiology [7] (Fig. 3B), based on IDM [6, 42], to transform the existing research framework towards PM and precision pharmacology for AD and other ND.
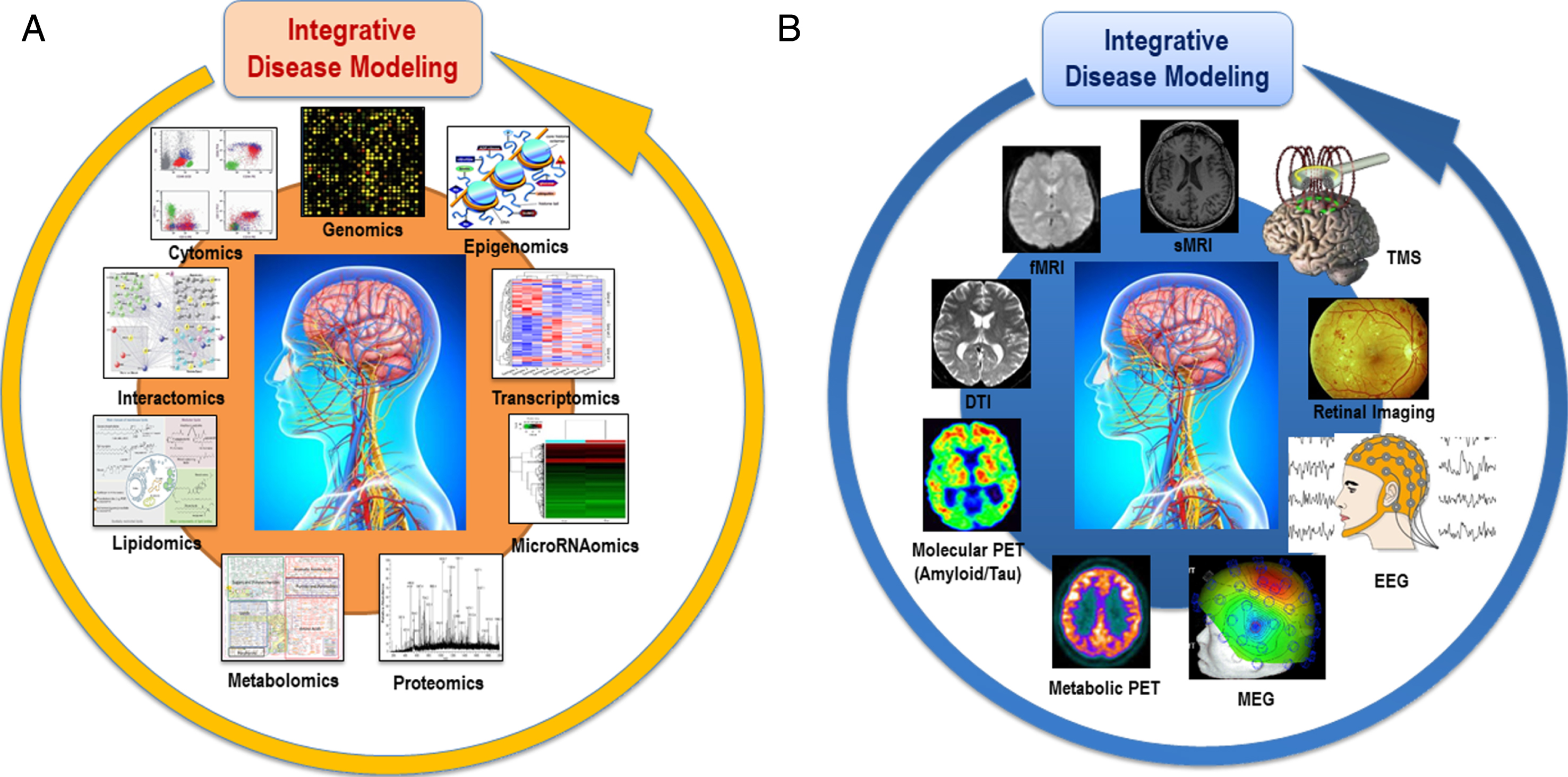
Cohorts stratified according to different multimodal-throughput technological platforms (“omic” sciences) and different neuroimaging modalities are integrated in the disease modeling for classification and prediction of subsets of AD and other ND patients. A) Systems biology is an evolving hypothesis-free, exploratory, holistic (non-reductionistic), global, integrative, and interdisciplinary paradigm using advances in multimodal high-throughput technological platforms that enable the examination of networks of biological pathways, where elevated amounts of structurally and functionally different molecules are simultaneously explored over time at a system level (i.e., at the level of molecules and subcellular compartments, cells, group of cells, tissues, organs, apparatuses, or even whole organisms). According to systems biology, organisms are made of systems which are entities consisting in hierarchically self-organized levels with increasing structural complexity resulting in different emerging properties. B) The paradigm of systems neurophysiology aims at studying the fundamental principles of integrated neural systems functioning by integrating and analyzing neural information recorded in multimodal fashion through computational modeling and combining data-mining methods. This paradigm may be used to decode the information contained in experimentally-recorded neural activity using analysis methods that are able to integrate the recordings of simultaneous, single-modality brain cell activity, such as fMRI or EEG, to generate synergistic insight and possibly infer hidden neurophysiological variables. The ultimate goal of systems neurophysiology is to clarify how signals are represented within neocortical networks and the specific roles played by the multitude of different neuronal components. AD, Alzheimer’s disease; DTI, diffusion tensor imaging; EEG, electroencephalography; MEG, magnetoencephalography; fMRI, functional magnetic resonance imaging, sMRI, structural magnetic resonance imaging; ND, neurodegenerative diseases; PET, positron emission tomography; TMS, transcranial magnetic stimulation. Reproduced with permission from [7].
The following section presents some pioneering examples of funded PM-oriented research programs.
I. The “
1) Defining functional and structural brain connectivity alterations related to the APOE gene profile and regional brain atrophy to determine the genetically-mediated functional and structural network alterations that may predict cognitive decline in at-risk AD individuals, over time, in relation to their amyloid status.
2) Stratifying the aging population along the genetic patterns of single nucleotide polymorphisms associated with neuroimaging phenotypes, namely: structural/functional connectivity and regional brain atrophy.
On these premises, we expect to provide a genetic subset of preclinical at-risk individuals for AD presenting early structural/functional brain alterations leading to defined clinical phenotypes, such as ND, including AD.
3) In a subsequent step, the objective is to determine quantitative data-driven models of disease progression based on the preclinical stages of AD and to identify the most suitable dimensions, among biological and neuroimaging biomarkers, to be integrated in a biologically defined staging model of AD. This biological and neurophysiological staging system is necessary to characterize the preclinical stages of AD as well as prodromal and clinical stages in a dimensional continuum and develop customized treatment strategies at the preclinical stage.
II. The
1) The systems biology component will help integrate different molecular/cellular levels and time phases of pathophysiological mechanisms, including altered genetic-epigenetic signaling pathways, inflammatory/immunological signaling changes, oxidative stress, protein misfolding, axonal depletion, synaptic dysfunction/loss, energy deficits, apoptosis, and neurodegeneration, within the full dimensional spectrum of “ND” or brain proteinopathies leading to neurodegeneration, from earliest preclinical to subtle prodromal to late clinical stages.
2) The systems neurophysiology component will help obtain evidence on the association (and interaction) between structural/functional neural networks as well as brain functional metabolism (via 2-deoxy-2-[fluorine-18]fluoro-D-glucose–positron emission tomography, [18F-FDG-PET]) and molecular imaging (via amyloid-PET) associated with a specific pattern of gene profiles and indicators of cognitive reserve. This will allow stratifying cohorts of individuals, according to specific endophenotypes, within the full dimensional spectrum of “ND” or brain proteinopathies leading to neurodegeneration, from earliest preclinical to subtle prodromal to late clinical stages.
III. The “
IV. The “
The APMI Cohort Program (APMI-CP)
The APMI Cohort Program (APMI-CP) has been established to significantly improve the development of risk and protective factors, early pathophysiological detection, diagnosis and classification, and prevention and treatment of individuals at risk and patients with AD. There are relevant established cohorts [43–49] of the APMI-CP currently investigated (see the Supplementary Material).
The Clinical Research Group Alzheimer Precision Medicine (GRC-APM)
All the APMI-CP foundation cohorts are based on standardized academic university-based expert center inclusion of both cognitively intact individuals at risk of AD and patients with a full range of ND. This approach therefore, providing a wide spectrum of relevant heterogeneous and multidimensional data. The research activity using these cohorts is operatively managed under the innovative structural framework of the recently established Paris Sorbonne University—“Clinical Research Group in Alzheimer Precision Medicine” (GRC n° 21) (“Groupe de Recherche Clinique-Alzheimer Precision Medicine” [GRC-APM]). The GRC-APM (Principal Investigator and Coordinator: Harald Hampel) unites hospital and university-based workgroups, laboratories, clinical and research centers, and investigators under the theoretical umbrella of PM with a thematic focus on AD and other ND. All clinical and multimodal data collected using the APMI-CP cohorts are managed to develop differentiated protocols for the individual participant towards accurate assessment of risk and protection factors, for detection, diagnosis, and biomarker-guided targeted treatments. The GRC-APM is divided into structured operative modules, synergistically interacting on horizontal and vertical levels (see Supplementary Table 1).
COLLABORATIVE APMI “HUB” NETWORKS AND INITIATIVES WORLDWIDE
The APMI is continuously expanding and consolidating a worldwide collaborative network with other hubs, including relevant initiatives, consortia, and research programs/projects. There are primary international platforms thematically and conceptually linked to the APMI (Table 2).
List of primary international platforms thematically and conceptually linked to the Alzheimer Precision Medicine Initiative
DPUK, Dementias Platform United Kingdom; EPAD, European Prevention of Alzheimer’s Dementia; EU JPND, European Union Joint Programme - Neurodegenerative Disease; WBP, Women’s Brain Project.
Dementias Platform United Kingdom (DPUK)
Established in 2014, the Dementias Platform UK (DPUK) (https://www.dementiasplatform.uk/) is a public-private partnership developed by the Medical Research Council (MRC). Its main goals are to improve early detection of dementia disorders, advance research in innovative treatments, and ultimately disease prevention. The DPUK is assembling one of the world’s largest population studies in the field of dementia, with over two million participants aged >50 years (including general population, people at-risk of developing dementia, and subjects diagnosed with early-stage dementia). The project, involving 22 study groups within the UK, will maximize the potential of UK cohort studies through a coordinated research environment.
Interestingly, DPUK shares electronic data through a portal (the “DPUK Data Portal”, available at https://portal.dementiasplatform.uk/) enabling rapid testing of new research designs. Among the active studies under way within this environment, the EU funded study called Integration and Analysis of heterogeneous Big Data for Precision Medicine and suggested Treatments for different Types of Patients (iASiS, available at http://project-iasis.eu/) intends to design a unified conceptual plan to represent various sources of data. It aims at combining information from large volumes of genomics data, imaging databases, and medical records to allow better individualized diagnosis and treatment strategies in AD. Among the cohorts included in the portal cohort directory, the UK Biobank project [50–52] (https://www.biobank.ac.uk) is playing a prominent role. This is a prospective cohort study including more than 500,000 volunteer participants in the UK, aged between 40 and 69 at recruitment (between 2006 and 2010). It collects both large-scale genetic-genomic and phenotypic data as well as health-related information about all participants, such as biological measurements, blood- and urine-based biomarkers, body and brain imaging scans, and lifestyle parameters [50–52]. By examining the link between genome variation and common human diseases, the UK Biobank aims at improving the prevention, diagnosis, and treatment of several life-threatening diseases, including cancer, heart diseases, stroke, diabetes, and dementia disorders.
European Union Joint Programme - Neurodegenerative Disease (EU JPND) Research
The European Union Joint Programme - Neurodegenerative Disease (EU JPND) Research (http://www.neurodegenerationresearch.eu/) was established in 2009 with the goal of tackling the growing burden of ND on the European society by involving 24 EU countries. The key idea behind JPND is that dementia is a global challenge that cannot be solved by any country alone. Therefore, large-scale, data-driven, collaborative efforts are the most promising way to yield robust knowledge and groundbreaking changes in ND. PM has been identified by the JPND Scientific Advisory Board as a key approach to achieve this goal. On March 22, 2017, the JPND convened a panel of 23 experts to promote the implementation of PM for dementia research at the European level. The key conclusions of the workshop were as follows: 1) the traditional study of the genetic underpinnings of neurodegeneration should be further expanded to include a systems biology approach [7, 41]; 2) dementia research will benefit from forging new alliances with other scientific disciplines (e.g., physics/engineering) to gain more insights on the overwhelming complexity of living systems; 3) academia institutions should gain access to hi-tech devices from industry, including wearable technologies, with the goal of introducing artificial intelligence into research on neurodegeneration; 4) there is a growing need to understand how dementia disorders are intertwined with other common diseases, including diabetes and cardiovascular diseases; 5) dementia research will benefit from computer modelling to accelerate the traditional clinical trial process in line with the approach used by the Association for Predictive Medicine Avicenna Alliance (http://avicenna-alliance.com/), which is exploiting a technological work-map for implementing in silico clinical trials; 6) data access and communication should be encouraged through different research communities to implement a systems biology approach [7, 41]. The experts further maintained that “omic” technologies should be mainly utilized to improve the stratification of dementia syndromes on a biological mechanistic level within PM.
European Prevention of Alzheimer’s Dementia (EPAD) program
The European Prevention of Alzheimer’s Dementia (EPAD) program [53] (http://ep-ad.org/) is a European collaboration between academic and private sectors. Its main aim is to create a platform to design and conduct phase II Proof-of-Concept clinical trials in secondary prevention of AD. Recent failures in phase III clinical trials in AD have clearly shown that novel approaches to drug development are required. Specifically, the EPAD program will use Bayesian statistics to enhance the efficiency of analyzing the available data. The adaptive randomization will generate more data on doses that appear to be more effective, ultimately improving dose selection for phase III [54]. Other common problems that the EPAD Longitudinal Cohort Study (LCS) (https://clinicaltrials.gov/ct2/show/NCT02804789) will address are as follows: 1) high rates of screening failure, 2) issues in patient stratification, and 3) absence of a run-in period in the pre-randomization phase. The EPAD LCS will involve 5,000 subjects who had undergone a thorough assessment in terms of cognition [55], neuroimaging, core CSF biomarkers, clinical outcomes, and genotyping. All participants will undergo an annual assessment to optimize stratification for trial inclusion. The development of an EPAD site network across the European Trial Delivery Centers will be crucial to ensure the success of this initiative. The EPAD program is expected to overcome the current study methodology, ultimately providing a better patient stratification before embarking on phase III trials.
AETIONOMY Project
Current disease classification systems, including the International Classification of Disease (ICD), are based on phenotypes defined according to: 1) clinical symptoms and 2) results of laboratory, neuroimaging, and instrumental examinations. The innovative AETIONOMY project (https://www.aetionomy.eu/en/background.html) aims at developing a “mechanism-based taxonomy” based on the biological pathways involved in the pathophysiology of diseases. The ultimate goals of the project are: 1) to guide the classification of disease classes and subclasses and 2) to generate value for developing ontologies or knowledge-based disease models. Disease-specific ontologies may allow knowledge exchange across different disciplines. Furthermore, ontology-driven mining approaches can be useful for modeling disease mechanisms. In this context, the “Alzheimer’s Disease Ontology” (ADO) is the disease ontology representing the domain knowledge specific to AD. The AETIONOMY project was recently featured in a key paper including a call for proposals to establish mechanism-based taxonomies for ND [56]. In summary, the consortium will serve as a useful source for exploring the underlying mechanism of neurodegeneration, while promoting the development of new preventive approaches.
The Women’s Brain Project (WBP)
Founded in 2016, the Women’s Brain Project (WBP) (http://womensbrainproject.com/) aims at inspiring a global discussion on sex and gender determinants of female vulnerability to brain and mental disease involving scientists, drug developers, regulators, and policy makers to propose solutions. Basic, clinical, social, and artificial intelligence research is supported in order to identify tools for better diagnosis, treatment, and care in brain and mental health conditions affecting women. In the era of PM, there is a critical need to determine whether the risk factors are the same for women and men. For women, sex-specific hormonal changes, such as early or premature menopause and cardiometabolic risk factors, among others, have been documented and are now being carefully inspected [57, 58].
The WBP proposes a personalized way to develop and perform prevention strategies, medical treatments, and caregiving accompanied by technologies improvement, based on consideration of sex and gender differences.
INNOVATION AND ACTION PLAN OF THE APMI
The implementation of PM in research and development of AD and other ND is anticipated to facilitate and establish a novel, original scientific taxonomy and a distinguished working lexicon and terminology, which is currently evolving through an intermediate development stage (see the glossary reported in Table 3), for reality-based medicine, which detects evidence from real-life scenarios [3,6–8, 3,6–8]. PM integrates evidence from advanced data on vast amounts of clinical samples with genomics and the other “omic” sciences, digital pathology analyses on clinical specimens, clinical neuroimaging studies, artificial intelligence, e-Health and m-Health records, and other data parameters allowing the development of tailored therapies. The novel radical and transformational approach of PM to disease prevention and treatment is based on the specific “biological make-up”, genetic/epigenetic, biochemical, phenotypic, lifestyle, and psychosocial characteristics, of the individual and is focused on identifying which therapeutic strategy will be effective for which subject.
Glossary reporting the evolving lexicon and terminology of the Alzheimer Precision Medicine Initiative (APMI)
AD, Alzheimer’s disease; EHR, electronic health records; GWAS, genome-wide association study; P4M, Predictive, Preventive, Personalized, Participatory Medicine; PM, precision medicine; PoC, Proof-of-Concept. Modified with permission from [7, 8].
Combined translational exploratory systems biology [7, 41] and systems neurophysiology [7] strategies, based on IDM [6, 42] (Fig. 3A, 3B), applied to AD and other ND within the APMI conceptual framework, support the discovery and development of multimodal biomarkers allowing the detection of dysfunctional systems underlying the pathophysiologies of the disease [59, 60]. The identification of multidimensional biomarkers charting the spatio-temporal trajectories of distinct, complex brain pathophysiological mechanisms permits the development of targeted translational applications assisting clinicians in providing effective pharmacological therapies customized to biomarker-guided subgroups of AD patients, i.e., pathway-based therapies (Fig. 4) [8].
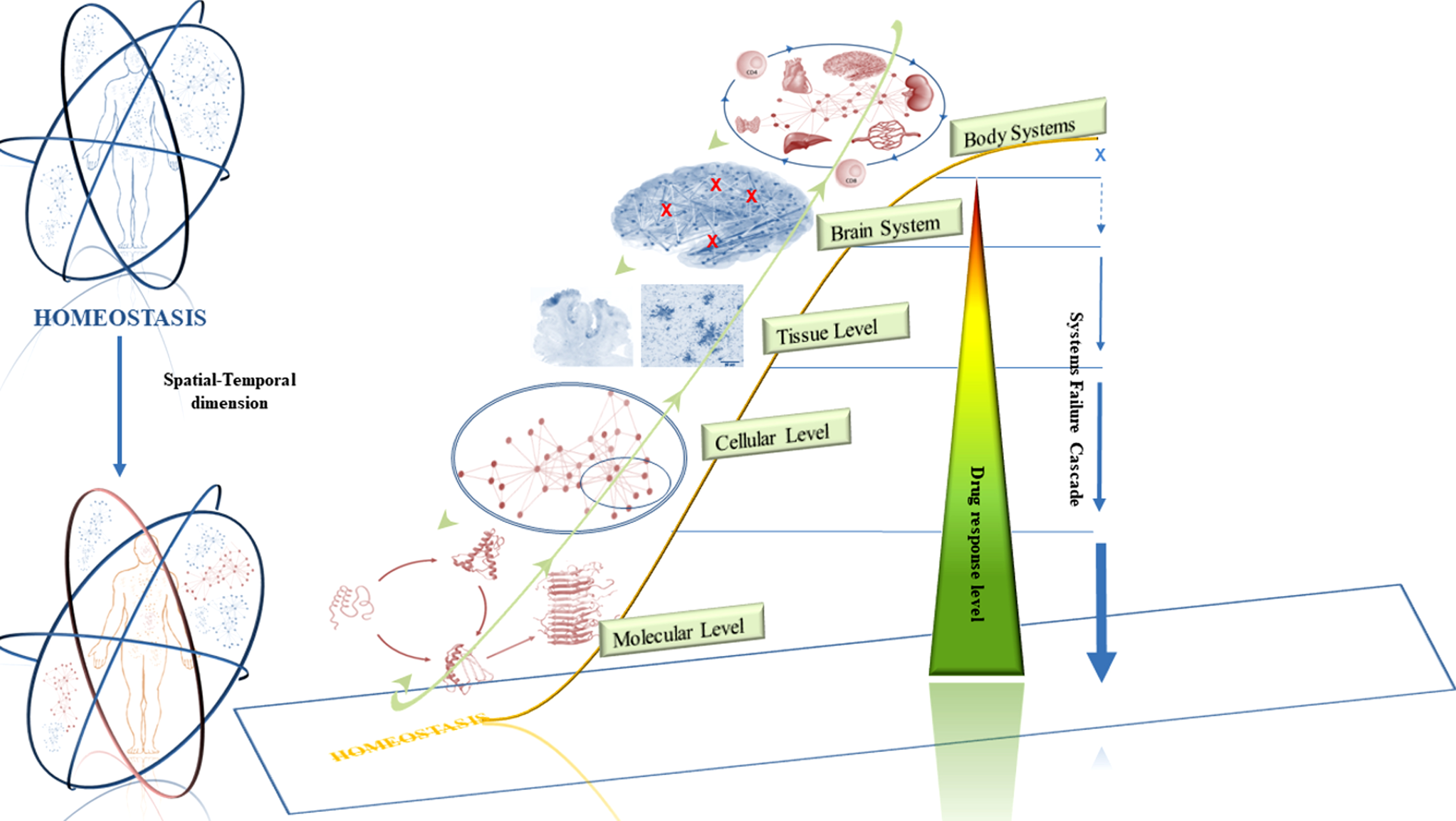
Trajectory of pathophysiological mechanisms across the continuum of systems multiscale hierarchical self-organization, from systems homeostasis to system failure: conceptual basis for pathway-based therapies. The preservation of human systems homeostasis is strictly related to the interactions between genomic/epigenomic factors and environmental factors (the circles). Such interactions show a non-linear fashion with complex dynamic that changes over time and are essential, at the individual level, for biological adaptation and survival to stressors and, at extra-individual level, for genetic adaptation and evolutionary transitions (trans-generational process under the natural selection). Of note, the impact of a genetic mutation on a single organism may lead to wide-ranging severe maladaptive effects even though from an evolutionary trans-generational perspective this may represent a primary driver for optimized survival and reproduction. Therefore, adaptive responses are differently distributed in space and time scales, across body systems and individuals and serve at different key roles consistently with the individual, extra-individual and the trans-generational level. Unrevealing the spatial–temporal coordinates of adaptation across multilevel networks and systems (from molecular pathways to cellular processes to organ large-scale network until systems) will uncover key notions essential for the comprehensive understanding of complex diseases. At a higher level of complexity, the main challenge is to achieve a unified theory of genetic adaptation leading to evolution. Thus, an individual vulnerability to stressors exists with an individual threshold of stress responses activation and failure. The non-linear orange-shaped line represents the entire spectrum of pathophysiological mechanisms across all systems levels, during the course and progression of disease. Such alterations originate from initial adaptation processes leading through triggers, drivers, thresholds to a point of decompensation. The green circle surrounding the five levels represents the marked interplay among the different hierarchical self-organized biological and physiological levels. Such interactions support the hypothesis that the initial loss of homeostasis might originate and occur at every level taking into account that a single level potentially affects the whole dynamic interrelated system and, therefore, initially or ultimately the entire affected organism. The
In this regard, substantial advances in the discovery, development, and validation of AD-mechanism related biomarkers have set the groundwork for an exciting era of multimodal investigations, promoted by the APMI, integrating different modalities and biological fluid analyses [59 , 61–64]. Multidimensional biomarkers result from neurogenetics [65 –67], neurochemistry through biological fluids [68 –70], namely blood (plasma/serum) [71 –78] and CSF [79 –82], and structural/functional/metabolic neuroimaging [83 –85]. The longitudinal dynamics and predictive performance of this multimodal approach have not been yet fully established and needs to be inspected in terms of sensitivity, specificity, and predictive power. They should also be examined according to their condition, either alone or in combination [86 –88]. Additionally, in this dynamic scenario, guidance from regulatory agencies and industry stakeholders in the AD biomarker discovery area are necessary [89, 90]. Thanks to this evolving spectrum of biomarkers and modalities, a multistage diagnostic setting in which blood-based biomarker tests represent the entry point preceding MRI, CSF examination, and PET imaging is envisioned (Fig. 5). In particular, blood-based biomarkers have an excellent potential to be routinely and rapidly assessed in all health-care settings and in asymptomatic individuals due to minimal invasiveness, cost-efficiency, accessibility, and reduced time and resource utilization compared to neuroimaging- and CSF-based techniques. In the coming years, more comprehensive arrays of multimodal biomarkers will be validated and qualified for clinical practice and pharmacological trials as well as for distinctive context-of-use (COU) such as: 1) screening asymptomatic individuals for AD pathophysiology; 2) stratifying individuals by risk of developing AD-related clinical decline; 3) predicting the clinical onset in individuals positive for AD pathophysiology to facilitate and optimize enrollment in clinical trials; and 4) monitoring the disease progression. Additional profiling, i.e., genomic, steps may be executed as part of multimodel interventions targeted to definite patient subgroups [7 , 91]. Standardized protocols for collecting and recording multimodal data and advanced integrative statistical modeling are needed to allow the comparison and the combination of big samples and datasets. This is required to conduct very large-sample-size research that will advance the molecular understanding of the disease [8].
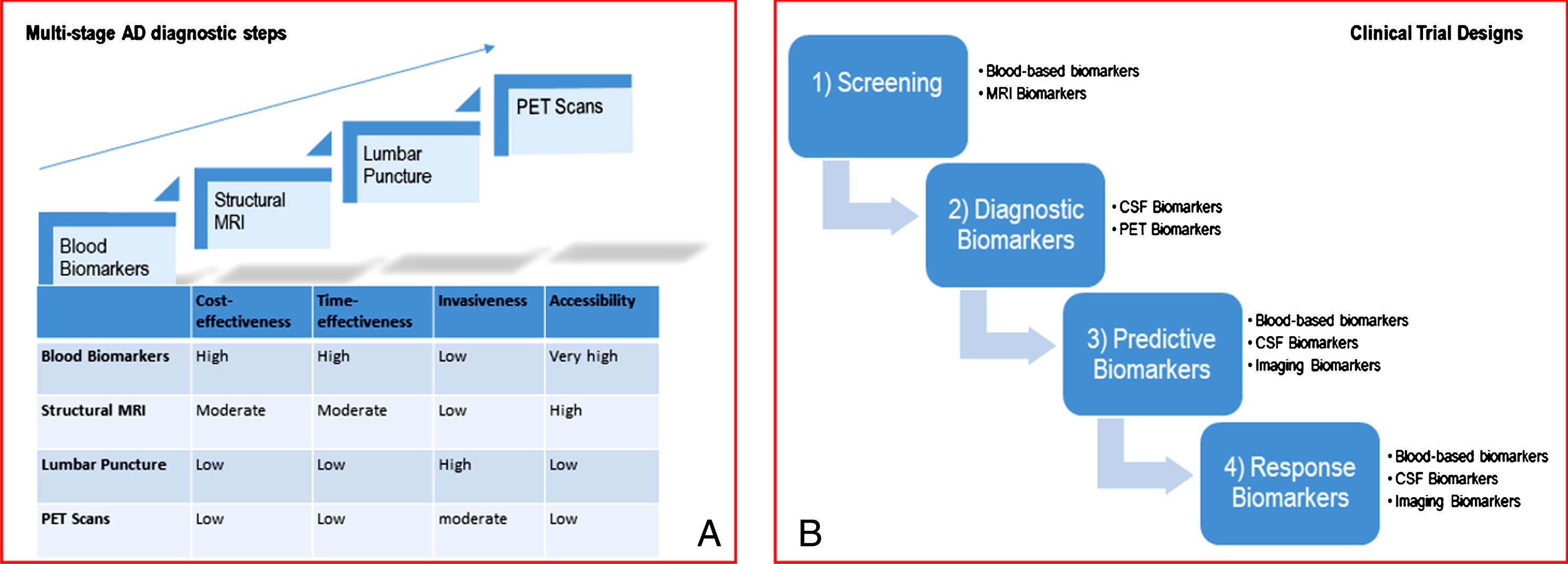
Evolving spectrum of biomarkers and modalities. A) The ideal biomarker should be minimally-invasive, unexpansive, practical, rapid and reliable with low level of expertise required. Therefore, in the clinical-setting, biomarkers should be assessed in a multistage diagnostic workout carried-out along four steps (blood biomarkers, structural MRI, lumbar puncture, PET scans) according to the overall balance among the following factors: cost-effectiveness, time-effectiveness, invasiveness and accessibility. B) Biomarkers represent one strategy to tailor therapy. The idealistic markers for ND would enable their implementation in screening, diagnosis, progression of the disease, and monitoring of the response to therapy. Therefore, in clinical trials, biomarkers can be used for several purposes: 1) to identify people eligible for the trial, i.e., those considered at high risk for ND (screening biomarkers); 2) to guide clinical diagnosis (diagnostic markers); 3) to optimize treatment decisions, providing information on the likelihood of response to a given drug (predictive biomarkers); 4) to detect and quantify the response rate to treatment (response markers). MRI, magnetic resonance imaging; ND, neurodegenerative diseases; PET, positron emission tomography. Reproduced with permission from [7].
The growing relevance of sex-related differences both in neural anatomy and function has emphasized the role of sex as a critical factor for AD patient stratification and development of individualized treatments. Recently published evidence provided by the emerging APMI movement, in cooperation with the WBP, points to distinct sex-specific patterns of clinical and biological disease manifestation as well as sex differences in the rates of progression, cognitive decline and brain atrophy, indicating sex as a key variable in disease heterogeneity [57, 58]. Elucidating sex differences in disease phenotypes is a first fundamental step toward PM in AD, using multimodal, biomarker-guided, and sex-sensitive approaches for disease prevention and detection as well as therapy development [57, 58].
Following the PM approach, the APMI is focusing on AD as an essential model of a chronic non-linear dynamic complex polygenic neurodegenerative brain disease, with a need for an accurate staging system across all the stages of disease progression, from earliest preclinical to first prodromal to late clinical stages. In particular, the use of multidimensional longitudinal datasets offers a unique opportunity to build data-driven models of disease progression. Charting the longitudinal trajectories of AD related systems and biomarkers (through “liquid biopsy”) is a practical way to establish biological staging. The dynamical model of AD progression will include specific normative definitions of the disease progression, such as the link of Aβ accumulation in a certain brain region with the alteration of a given cognitive task. Moreover, the model will allow assessing the normal variations in the estimated trajectory of data change and the pace at which such trajectories are monitored, thus highlighting the inter-individual variability in the disease progression trajectories. Risks factors, such as sex, the APOE ɛ4 genotype, or the premorbid intelligence or education level will be correlated with the modes of variability in the age at disease onset, pace of disease progression, and relative timing and ordering of biomarker changes.
The aim is to substantially extend the understanding of disease pathophysiology and help develop solutions for optimized healthcare management of all individuals within the full spectrum of AD. The outcomes of the research programs so far developed under the umbrella of the APMI (“MIDAS”, “PHOENIX”, “POSEIDON”, “VISION”) will facilitate and inform controlled pharmacological and non-pharmacological clinical intervention trials based on identified intermediate endophenotypes as well as systems-based diagnostic and candidate surrogate biomarker studies. Ultimately, the APMI will pave the way to the development of prospective longitudinal studies aimed at in vivo analyzing a comprehensive multimodal biomarker array to enrich risk prediction of cognitive decline along the full disease continuum in different subsets of people.
The interdisciplinary character of the multimodal approaches undertaken by the APMI research programs emphasizes the importance of the concept of reverse translation. Clinical studies and trials generate data which are then verified by basic research, thus allowing the validation of reality-driven questions raised in clinical studies. Reverse translation of clinical observations into hypothesis generation is getting increasing relevance: translational research works from bench to bedside and back again with the goal of improving patient care. Research across fundamental sciences, epidemiology, clinical sciences, as well as advanced education, constitutes the basis of successful translational medicine.
The APMI brings together scientists from various methodological fields, continents and countries in order to advance and accelerate innovative and cutting-edge neuroscience, transforming the fields of Neurology and Psychiatry [6, 7]. Several APMI associated research teams synergistically collaborate through cross-disciplinary research programs. This multilevel interdisciplinary network is required to foster dynamic scientific advances. The next generation of researchers is expected to realize a much more matured potential of PM and, therefore, to further develop expertise in highly complex informatics-based approaches and biomedical technologies.
The APMI will facilitate a “team science” approach [92], i.e., a collaborative effort involving the abilities and the expertise of several professionals of different fields, to integrate a multidisciplinary conception of health and disease. This is illustrated by profound scientific investigations in the following areas:
CONCLUSIONS
PM is currently reaching a first intermediate development stage and, therefore, not yet widely implemented in clinical practice. Apart from oncology, clinical medicine continues to be strongly grounded on the traditional paradigm to cure the disease, and not the patient (with his/her own unique, diverse and complex matrix of multi-system characteristics). We have to be patient and need to realize that road ahead toward true PM is a very long and winding road and that major paradigm shifts, including the questioning of prevailing scientific dogmas and ideologies, will be required to move from philosophical and political programmatic statements to scientific and medical reality. Although the exciting APMI journey has just begun, we may say it is the end of a promising beginning, global pioneering efforts must continue and have the potential to further pave the way for a future of medicine, in which drugs will truly help prevent diseases and cure the individual in an personal, tailored, and targeted fashion, the right patient at the right time, with a minimum of tolerability issues, affordable for societies, and accepted and embraced by the medical and political establishment. We envision that the APMI will integrate and merge into a global holistic comprehensive PM evolution, across current traditionally fragmented and historically constructed disease and specialty barriers.
Footnotes
ACKNOWLEDGMENTS
This research benefited from the support of the Program “
Dr. Harald Hampel is supported by the AXA Research Fund, the “Fondation partenariale Sorbonne Université” and the “Fondation pour la Recherche sur Alzheimer”, Paris, France. Ce travail a bénéficié d’une aide de l’Etat “Investissements d’avenir” ANR-10-IAIHU-06. The research leading to these results has received funding from the program “Investissements d’avenir” ANR-10-IAIHU-06 (Agence Nationale de la Recherche-10-IA Agence Institut Hospitalo-Universitaire-6).
We thank Dr. Patrizia A. Chiesa and Emma Ducos for their helpful input and feedback.
Lisi Flores AGUILAR (Montréal), Claudio BABILONI (Rome), Filippo BALDACCI (Pisa), Norbert BENDA (Bonn), Keith L. BLACK (Los Angeles), Arun L.W. BOKDE (Dublin), Ubaldo BONUCCELLI (Pisa), Karl BROICH (Bonn), Francesco CACCIOLA (Siena), Juan CASTRILLO (Derio), Enrica CAVEDO (Paris), Roberto CERAVOLO (Pisa), Patrizia A. CHIESA (Paris), Jean-Christophe CORVOL (Paris), Augusto Claudio CUELLO (Montréal), Jeffrey L. CUMMINGS (Las Vegas), Herman DEPYPERE (Gent), Bruno DUBOIS (Paris), Andrea DUGGENTO (Rome), Valentina ESCOTT-PRICE (Cardiff), Howard FEDEROFF (Irvine), Maria Teresa FERRETTI (Zürich), Massimo FIANDACA (Irvine), Richard A. FRANK (Malvern), Francesco GARACI (Rome), Hugo GEERTS (Berwyn), Filippo S. GIORGI (Pisa), Manuela GRAZIANI (Roma), Marion HABERKAMP (Bonn), Marie-Odile HABERT (Paris), Harald HAMPEL (Paris), Karl HERHOLZ (Manchester), Eric KARRAN (Cambridge), Seung H. KIM (Seoul), Yosef KORONYO (Los Angeles), Maya KORONYO-HAMAOUI (Los Angeles), Todd LANGEVIN (Minneapolis-Saint Paul), Stéphane LEHÉRICY (Paris), Simone LISTA (Paris), Jean LORENCEAU (Paris), Dalila MANGO (Rome), Mark MAPSTONE (Irvine), Christian NERI (Paris), Robert NISTICÓ (Rome), Sid E. O’BRYANT (Fort Worth), George PERRY (San Antonio), Craig RITCHIE (Edinburgh), Simone ROSSI (Siena), Amira SAIDI (Rome), Emiliano SANTARNECCHI (Siena), Lon S. SCHNEIDER (Los Angeles), Olaf SPORNS (Bloomington), Nicola TOSCHI (Rome), Steven R. VERDOONER (Sacramento), Andrea VERGALLO (Paris), Nicolas VILLAIN (Paris), Lindsay A. WELIKOVITCH (Montréal), Janet WOODCOCK (Silver Spring), Erfan YOUNESI (Esch-sur-Alzette).