
Abstract
Background:
The current evidence is inconclusive to support the benefits of aerobic exercise training (AET) for preventing neurocognitive decline in patients with amnestic mild cognitive impairment (aMCI).
Objective:
To examine the effect of a progressive, moderate-to-high intensity AET program on memory and executive function, brain volume, and cortical amyloid-β (Aβ) plaque deposition in aMCI patients.
Methods:
This is a proof-of-concept trial that randomized 70 aMCI patients to 12 months of AET or stretching and toning (SAT, active control) interventions. Primary neuropsychological outcomes were assessed by using the California Verbal Learning Test-second edition (CVLT-II) and the Delis–Kaplan Executive Function System (D-KEFS). Secondary outcomes were the global and hippocampal brain volumes and the mean cortical and precuneus Aβ deposition.
Results:
Baseline cognitive scores were similar between the groups. Memory and executive function performance improved over time but did not differ between the AET and SAT groups. Brain volume decreased and precuneus Aβ plaque deposition increased over time but did not differ between the groups. Cardiorespiratory fitness was significantly improved in the AET compared with SAT group. In amyloid positive patients, AET was associated with reduced hippocampal atrophy when compared with the SAT group.
Conclusion:
The AET and SAT groups both showed evidence of slightly improved neuropsychological scores in previously sedentary aMCI patients. However, these interventions did not prevent brain atrophy or increases in cortical Aβ deposition over 12 months. In amyloid positive patients, AET reduced hippocampal atrophy when compared with the SAT group.
Keywords
Introduction
The prevalence of Alzheimer’s disease (AD), the most common type of age-related dementia, is rapidly increasing while we currently do not have effective treatments [1]. AD dementia is a progressive neurological disorder that is hypothesized to begin with cortical amyloid-β (Aβ) plaque deposition followed by phosphorylated tau accumulation, brain atrophy, and memory impairment [2, 3]. In line with this hypothesis, patients with amnestic mild cognitive impairment (aMCI) are functionally independent in daily life, but they have a higher conversion rate to AD with brain pathologies that are intermediate between AD and normal cognitive status [4–6]. Therefore, aMCI may represent an optimal stage for implementing preventive strategies that may delay the onset of AD dementia manifestation.
The increasing evidence suggests that physical exercise is associated with improved cognitive performance and the reduced AD pathologies in older adults [7]. For example, a 1-year aerobic exercise training (AET) has demonstrated the improved memory and executive function performance that are accompanied by the increased hippocampal volume in cognitively normal old adults [8, 9]. Also, a 10-year history of aerobic exercise engagement has been shown to correlate with the reduced cortical Aβ plaque deposition in cognitively normal adults [10]. In patients with MCI and early AD dementia, a 6-month AET program improved cognitive performance and functional ability [11, 12], and higher physical activity levels were correlated with the reduced Aβ plaque deposition and tau tangle formation [13]. These findings collectively suggest that physical exercise can improve neurocognitive function in old adults, yet no randomized controlled trial (RCT) of AET has been conducted in aMCI patients to examine its efficacies on improving cognitive performance and reducing brain AD pathologies.
Given this knowledge gap, we conducted a proof-of-concept RCT to determine the effect of AET on neuropsychological function, brain volume, and cortical Aβ plaque deposition in patients with aMCI. We hypothesized that a 12-month AET program would improve cardiorespiratory fitness, an index of cardiovascular health [14], and memory and executive function performance, while preventing or slowing global brain and hippocampal atrophy and cortical Aβ plaque accumulation in aMCI patients.
Methods
Trial design
This is a 12-month, single-blinded, parallel RCT of AET versus stretching and toning (SAT, active control) in aMCI patients. Cognitive assessment was conducted at baseline, midpoint (6-month), and trial completion. MRI and amyloid PET were performed at baseline and trial completion in a subset of eligible participants. PET scanning was added to the study protocol a year after trial initiation upon obtaining supplemental funding.
Standard protocol approvals, registrations, and patient consents
This study was approved by the Institutional Review Board of the University of Texas Southwestern Medical Center and Texas Health Presbyterian Hospital Dallas in accordance with the guidelines of the Declaration of Helsinki and Belmont Report. The trial was registered at ClinicalTrials.gov (NCT01146717: Aerobic Exercise Training in Mild Cognitive Impairment Study). All participants gave written informed consent before participation.
Participants
Recruitment was conducted in the Dallas-Fort Worth metropolitan area using community-based advertisements and through the University of Texas Southwestern Medical Center Alzheimer’s Disease Center. Inclusion criteria were men and women aged 55–80 years with aMCI. These criteria were used because in this age range, the prevalence of MCI starts increasing [15] and our previous studies have confirmed safety for conducting exercise training intervention in older adults [16]. An initial telephone interview was conducted to ask potential participants if they had 1) memory concerns, 2) progressive memory decline, and 3) habitual exercise engagement. Subsequently, those individuals who had memory concerns and did not exercise regularly were asked to visit the clinical office for further screening.
The diagnosis of aMCI was based on Petersen criteria [4], as modified by the Alzheimer’s Disease Neuroimaging Initiative project (http://adni-info.org). All subjects had a global Clinical Dementia Rating (CDR) scale of 0.5 with a score of 0.5 in the memory category, in addition to objective memory loss as indicated by education-adjusted scores on the Logical Memory subtest of the Wechsler Memory Scale-Revised (WMS-R), and a Mini-Mental State Exam (MMSE) score between 24 and 30.
Clinical evaluation was further performed according to the recommendations from the Alzheimer’s Disease Cooperative Study (http://adni-info.org). To focus upon the prevention of AD dementia, we excluded those who have already been diagnosed with AD or other types of dementia, or have major neurological, vascular, or psychiatric disorders such as stroke and psychosis. In addition, participation in regular exercise within the last 2 years, sleep disorders including clinically diagnosed or self-reported sleep apnea, uncontrolled hypertension, diabetes, and a history of smoking within the past 2 years were excluded (detailed inclusion and exclusion criteria are presented in ClinicalTrials.gov: NCT01146717). Severe obesity with body mass index≥35 kg/m2 was also excluded to safely implement exercise training program. To ensure physical activity level before enrollment, each of the aMCI patients wore an Actical accelerometer for 1 week (Actical, Philips Respironics, USA), and those patients who spent > 90 minutes of moderate-to-vigorous physical activity (>4.0 METs) per week were also excluded. MRI and PET scans were optional and performed in a subset of eligible participants without contraindications such as metal implants or claustrophobia.
Randomization and blinding
A randomized, single-blind, placebo-controlled trial design (AET versus SAT groups) was used in this study. SAS V9.2 was used to generate the stratified, randomization lists using a blocking factor of 4. Patients were stratified by age (55–70 and 71–80) and sex (men and women). Investigators conducting the primary and secondary outcome measurement were blinded to treatment assignment. Participants were instructed to maintain their normal daily activities aside from the assigned interventions and were instructed not to disclose their group assignment or to discuss their interventions during outcome measurements or meeting with other participants.
Intervention
Aerobic exercise training (AET) program
The dose and intensity of the AET program were based on each individual’s fitness level assessed with peak oxygen uptake (VO2) testing, and progressively increased as participants adapted to previous workloads. Specifically, the program started with a frequency of 3 exercise sessions per week for 25–30 minutes per session at the intensity of 75–85% of maximal heart rate that was measured during peak VO2 test at baseline. At week 11, participants started alternating between 3 and 4 exercise sessions per week for 30–35 minutes per session, and at the weeks in which they performed 3 exercise sessions per week, a high intensity exercise session was introduced which consists of 30 minutes of walking at the intensity of 85–90% of maximal heart rate (e.g., brisk uphill walking). After week 26, participants performed 4-5 exercise sessions per week for 30–40 minutes, including two high intensity sessions. Each exercise session included a 5-minute warm-up and a 5-minute cool-down. Any modes of aerobic exercise were allowed as long as they maintained the prescribed training dose and intensity, as monitored by changes in heart rate during each of the exercise sessions (Polar RS400, Polar Electro, USA). Of note, this AET program meets the national physical activity guidelines for older adults [17] and has been used in our previous studies that showed significant improvement of cardiorespiratory fitness in sedentary individuals older than 65 years of age [16].
Stretching and toning (SAT) program
SAT exercise was used as an active control group to keep participants engaged with the same level of attention received from the investigators as those for the AET group. The frequency and duration of SAT program were the same as the AET program. A SAT routine that focuses on the upper and lower body was used. In this group, participants were asked to keep their heart rate below 50% of maximal heart rate during each session. At week 19, we introduced a second set of full body stretches that are more advanced than the previous set. At week 26, we introduced a set of low resistance theraband exercise that focuses on strengthening the upper and lower body.
In both AET and SAT programs, each participant was supervised for the first several weeks until they could comfortably exercise by themselves at home. During the study period, they were asked to perform assigned intervention on top of their regular physical activities. To ensure adherence to each program, participants were required to make a training log in addition to heart rate monitoring. Each month, participants visited the clinic to download heart rate data and review their training log together with an exercise physiologist to ensure implementation of the prescribed training programs. When adherence to exercise programs were not met with the prescribed intensity, duration, and frequencies, in-person and/or telephone meetings were held to solve the issues and encourage participants to continue the program. The total amount of exercise performed by the AET group over 12 months was calculated by the training impulse (TRIMP) score, which is calculated by multiplying the duration of exercise session by the average heart rate achieved during each session weighted for exercise intensity [18].
Outcomes
The primary outcomes were the California Verbal Learning Test-second edition (CVLT-II) and the Delis–Kaplan Executive Function System (D-KEFS). The CVLT-II and D-KEFS are well-established sensitive measure of memory and executive function [19, 20] and have been used in previous studies that examined the effects of aerobic exercise and fitness [11]. The secondary outcomes were global brain and hippocampal volumes and mean cortical and precuneus Aβ plaque deposition.
Neuropsychological function
The CVLT-II is a verbal 16-item list-learning task that serves as a measure of verbal learning and episodic memory. The standardized total score, which reflects the number of words learned across the 5 learning trials, are reported. Delayed free recall reflects the number of words the participant freely retrieved out of 16 total words following delay [19].
The D-KEFS is comprised of several individual verbal and nonverbal executive function measures. The Trail Making Test consists of 5 tasks, including a visual cancellation task and a series of connect-the-circle tasks. The primary executive-function task is Condition 4 (number-letter switching), which is a visual-motor sequencing task assessing mental flexibility. The Color-Word Interference Test primarily measures the ability to inhibit an overlearned verbal response (i.e., reading the printed words) to generate the conflicting response of naming the dissonant ink colors in which the words are printed. Also, an inhibition/switching condition evaluates both inhibition and cognitive flexibility. The Verbal and Category Fluency Tests measure the ability to generate words fluently in an effortful phonemic format (letter fluency) from overlearned concepts (category fluency) and simultaneously shifting between overlearned concepts [20]. The D-KEFS results are reported using the standardized scores.
Brain volume
High-resolution 3D T1-weighted magnetization-prepared rapid acquisition gradient-echo (MPRAGE) images were collected using a 3-tesla scanner (Achieva 3.0T, Philips Medical System, the Netherlands) with the following parameters: TE/TR = 3.7/8.1 ms, flip angle = 12°, FOV = 256×256 mm, number of slices = 160 (no gap), resolution = 1×1×1 mm3, and SENSE factor = 2.
To measure changes in brain tissue volume, MPRAGE images were processed with the longitudinal stream in FreeSurfer 6 [21]. Specifically, an unbiased within-participant template space and image [22] was created using robust, inverse consistent registration [23]. Several processing steps, such as skull stripping, Talairach transforms, atlas registration, as well as spherical surface maps and parcellations, were then initialized with common information from the within-participant template to increase reliability and statistical power [21]. The global brain and hippocampus were selected as a priori regions-of-interest (ROI) relevant to the AD pathologies [24]. The left and right sides of hippocampus were added together to report the whole volume. The brain volumetric data were normalized to intracranial volume (ICV) and expressed in percentage.
Brain Aβ deposition
Amyloid PET (Siemens ECAT HR scanner) was performed with an intravenous bolus injection of 10-mCi 18F-florbetapir [25]. At 30-minutes post-injection, participants were positioned on an imaging table with the head being secured with Velcro straps and foam wedges to minimize movements. A 2-minute scout scan was acquired to ensure that the brain was completely in the field of view without rotation in either the transverse or sagittal planes. At 50-minutes post-injection, 2 frames of 5-minute PET emission scan and a 7-minute transmission scan were acquired in 3 dimensional mode using the following parameters: matrix size = 128×128, resolution = 5×5 mm, slice thickness = 2.42 mm, and field of view = 58.3 cm. The emission images were processed by iterative reconstruction, 4 iterations and 16 subsets with a 3-mm full width at half maximum (FWHM) ramp filter. The transmission image was reconstructed using back-projection and a 6-mm FWHM Gaussian filter for attenuation correction.
Each participant’s PET image was spatially normalized to a florbetapir uptake template (2×2×2 mm3 voxels) using SPM8 (Well Department of Cognitive Neurology, London, UK) and in-house MATLAB (Mathworks Inc., Sherborn, MA) scripts, and visually inspected for registration quality. Standardized uptake value ratio (SUVR) was calculated using the mean cerebellar uptake as a reference [26]. In addition to the mean cortical SUVR, the precuneus was selected as a priori ROI due to a susceptibility of Aβ plaque accumulation in MCI and AD dementia patients [24]. The mean cortical SUVR was calculated as an average of the posterior and anterior cingulate, precuneus, temporal, dorsolateral prefrontal, orbital frontal, parietal, and occipital SUVRs [27].
Peak VO2
Peak VO2 was measured by a modified Astrand-Saltin protocol using treadmill [28]. The treadmill grade was increased by 2% every 2 minutes until exhaustion while participants walked or jogged at a fixed speed, which was determined by individual fitness level. VO2 was measured during the 2nd minute of each stage using the Douglas bag method. Also, the breath-by-breath VO2, VCO2, respiratory exchange ratio (RER), and ventilation were continuously monitored using an online computer system. Gas fractions were analyzed by mass spectrometry (Marquette MGA 1100) and ventilatory volume was measured by a Tissot spirometer. Blood pressure, 12-lead electrocardiogram, and heart rate were monitored continuously during exercise testing to assess cardiovascular responses.
The peak VO2 was defined as the highest VO2 measured from a > 30-second Douglas bag during the last stage of testing. The criteria to confirm that peak VO2 was achieved included an increase in VO2 < 150 ml despite increasing work rate of 2% grade, a RER > 1.1, and heart rate < 5 beats/min of age-predicted maximal values. In all cases, at least two of these criteria were achieved, confirming the identification of peak VO2 based on the American College of Sports Medicine guidelines [17]. Our previous studies show that by using these methods, peak VO2 can be measured reliably in sedentary older adults [16].
Apolipoprotein E (APOE) genotype
Peripheral blood mononuclear cells were cryopreserved in the media containing 50% human serum on the day of blood sample collection. For genotype analysis, one million cells were thawed and DNA extracted using the DNeasy Blood and Tissue kit (Qiagen). APOE genotype was identified using TaqMan SNP genotyping assays (Life Technologies). APOE genotype data were available from 36 participants [29].
Sample size estimate
Sample size estimation for this proof-of-concept RCT was based on potential improvements in neuropsychological performance with AET in cognitively normal healthy older adults due to the lack of similar RCTs in MCI patients at the time of trial initiation [7]. We anticipated that the scores of memory and executive function assessment would improve by∼0.6 standard deviations (SD) after 12 months of AET (treatment) compared with the SAT group (control). Assuming a 15% attrition rate and an α-level of < 0.05, 70 participants provides 80% power to detect an effect size of 0.60. Sample size estimates were not performed for MRI and PET scans because they were optional in this trial.
Statistical analysis
The primary analysis was based on intent-to-treat, maximum likelihood estimation using all available data from the randomized subjects (n = 70). Linear mixed model (LMM) was used to analyze the interaction effect of group (AET versus SAT) and time (baseline, 6-months, versus 12-months). In the model, intercept was specified as a random effect, and a compound symmetry covariance structure was used to account for within-individual correlations across time points. To corroborate the results of LMM analysis, complete case analysis was performed by the two-way repeated measures analysis of variance (ANOVA). In LMM and ANOVA, post-hoc multiple pairwise comparisons were corrected by the Bonferroni method in case of a significant group-by-time interaction.
The secondary analysis was performed to examine whether changes in outcome measures are different between the AET and SAT groups in amyloid positive patients. The amyloid positivity was determined by the mean cortical SUVR≥1.10 [25]. We also performed simple correlation analysis to examine whether changes in cognitive and imaging outcome measures are correlated on an individual basis. Independent samples t-test and chi-square test were used elsewhere to compare the AET and SAT groups. Estimated marginal means with 95% confidence intervals are reported from LMM and ANOVA analyses whereas means and standard deviations were used to present demographic characteristics. Statistical significance was set a priori at p < 0.05. All analyses were performed using SPSS 20.0 (IBM Corporation, Armonk, NY, 2011).
Results
The flow of participants through the study is presented in Fig. 1. Recruitment was conducted from June 2010 to June 2014, and data collection was completed in September 2016. Of the 70 aMCI patients randomized, 22 subjects (31%) withdrew from the study. Those subjects lost attrition were younger (62±5 versus 66±7 years, p = 0.016), included more women (19 women versus 4 men lost from the study, p = 0.011), and had a larger total brain volume (71.1±4.6 versus 68.5±4.0% ICV, p = 0.026) than those who remained in the final analysis. The difference in total brain volume was abolished after adjusting for age.

Flowchart for the exercise trial in patients with amnestic mild cognitive impairment (aMCI). The aMCI patients were randomized to 12 months of aerobic exercise training (AET) or stretching and toning (SAT) program.
Demographic characteristics are presented in Table 1. Across all participants, global cognitive function, as determined by the MMSE, showed a mean score of 28.9. The mean score of WMS-R Logical Memory delayed recall was 8.94, indicating mild memory impairment as would be expected for an aMCI sample. 86% of our aMCI patients were amyloid positive at baseline. APOE4 carriers and hypertension were present in 33% and 34% of participants, respectively. Overall, demographic characteristics were not different between the AET and SAT groups.
Subject demographics by randomization groups
Values represent mean±standard deviation. Amyloid PET data were available from 42 patients, and its positivity was determined by the mean cortical standardized uptake value ratio greater than 1.10. APOE genotype was collected in 36 participants (18 SAT and 18 AET). AET, aerobic exercise training; APOE, apolipoprotein E; SAT, stretching and toning; WMS-R, Wechsler Memory Scale-Revised.
Intervention effects
Neuropsychological outcomes are presented in Table 2. Baseline cognitive scores were similar between the AET and SAT groups. Over time, both groups improved slightly on the total CVLT-II score and D-KEFS trail making, color-word inhibition, and category fluency scores. With regard to interaction effects, the 6-month D-KEFS score of letter fluency test improved in the AET group; however, this effect did not persist after 12 months. The CVLT-II long delayed free recall score improved in the SAT group at 12-month assessment; however, this effect was not seen from complete case analysis that included the subjects who completed intervention programs (Supplementary Table 1).
Neuroimaging outcomes are presented in Table 3. At baseline, the SAT group showed a higher level of mean cortical 18F-florbetapir uptake than the AET group. Over time, the global brain and hippocampal volumes decreased and the precuneus 18F-florbetapir uptake increased in both groups. The mean cortical 18F-florbetapir uptake did not change after 12 months. These results did not alter with adjustment for the baseline group difference in mean cortical 18F-florbetapir uptake and were similar to those observed from complete case analysis (Supplementary Table 2).
Neuropsychological test scores by randomization groups
Values represent estimated marginal means (95% confidence interval) and p-values calculated from linear mixed model (LMM). n is the number of observations at each time point. p < 0.05 are bolded. *versus baseline within the same group. The Bonferroni correction was applied for multiple pairwise comparisons. Higher scores reflect better cognitive performance. AET, aerobic exercise training; CI, confidence interval; CVLT-II, California Verbal Learning Test-second edition; D-KEFS, Delis–Kaplan Executive Function System; SAT, stretching and toning.
Brain volume and 18F-florbetapir uptake by randomization groups
Values represent estimated marginal means (95% confidence interval) and p-values calculated from linear mixed model (LMM). n is the number of observations at each time point. p < 0.05 are bolded. AET, aerobic exercise training; CI, confidence interval; ICV, intracranial volume; SAT, stretching and toning; SUVR, standardized uptake value ratio.
After 12 months, AET significantly improved peak VO2 by∼10% when compared with the SAT group (Fig. 2 and Supplementary Table 3), while peak heart rate and RER and body mass were similar between the groups or at each time point. The average compliance to exercise training programs was 69%, which is calculated by the ratio of prescribed exercise sessions over the actually completed exercise sessions in which participants achieved the target heart rate. The TRIMP scores showed substantial individual variability and were not correlated with changes in peak VO2 (Supplementary Figures 1 and 2).
The secondary analysis focused on amyloid positive patients exhibited the reduced hippocampal atrophy in the AET group when compared with the SAT group (Fig. 3 and Supplementary Table 4). The correlation analysis of cognitive and imaging outcome changes did not show significant result across all subjects or within each group. The observed study power, effect sizes, and effective sample sizes based on the current study findings of cognitive performance, brain volume, and amyloid are provided in Supplementary Table 5.
Adverse events
During the study, 11 adverse events occurred. During peak VO2 testing, 4 had arrhythmia, 1 had foot pain, and 1 had mouth pain caused by a mouthpiece. During AET, 1 fell from treadmill, 2 reported ankle pain, and 1 had knee pain. After the PET scan, 1 experienced headache. The number of participants who experienced adverse events was not different between the SAT and AET groups.
Discussion
The main findings from this study are four-fold. First, although there was no group difference after 12 months of AET and SAT in aMCI patients, participation in both exercise programs was associated with slight improvements in memory and executive function scores. Second, AET and SAT programs did not prevent brain atrophy or precuneus Aβ plaque accumulation. Third, AET program significantly improved cardiorespiratory fitness when compared with the SAT program. Fourth, within amyloid positive patients, AET attenuated hippocampal atrophy when compared with the SAT group.
Participation in both AET and SAT programs was associated with improved cognitive performance in aMCI patients. These associations may be attributed to either the practice effects of repeated testing and/or the effects of both programs on neuropsychological function. While practice effects are common on neuropsychological measures [30], patients with MCI and AD dementia have shown the attenuated effects when compared with healthy older adults [31, 32]. Thus, the small yet statistically significant improvements in neuropsychological scores in both groups could reflect improvements beyond practice alone. In this regard, our SAT program included low-intensity resistance theraband exercise that might have contributed to cognitive improvements, as demonstrated by previous resistance training studies [33, 34].
Accumulating evidence suggests that AET improves cognitive performance in healthy older adults [7–9]. However, its effect for preventing or slowing cognitive decline in those who already have increased risks for developing AD and other related dementias remains controversial. Recently, the Agency for Healthcare Research and Quality (AHRQ) reported that the current evidence is inconclusive to support the benefits of AET for preventing cognitive decline in patients with MCI or AD dementia [35]. Furthermore, consistent with our findings, the Mental Activity and eXercise (MAX) trial showed that in older adults with cognitive complaints, 3 months of AET and stretching programs were both associated with improved global cognitive function [36]. In addition, the EXercise for Cognition and Everyday Living (EXCEL) study, a 6-month RCT of AET and resistance training, showed that the only resistance program significantly improves the Stroop test and an associative memory task in probable MCI patients [34]. Conversely, several studies demonstrated the benefits of AET for improving cognitive performance in MCI patients. The high-intensity AET program showed the sex-specific effects for improving executive function in aMCI patients [37]. Moreover, multicomponent exercise training that included walking and resistance exercise showed improvements in MMSE and Logical Memory scores in aMCI patients [38].
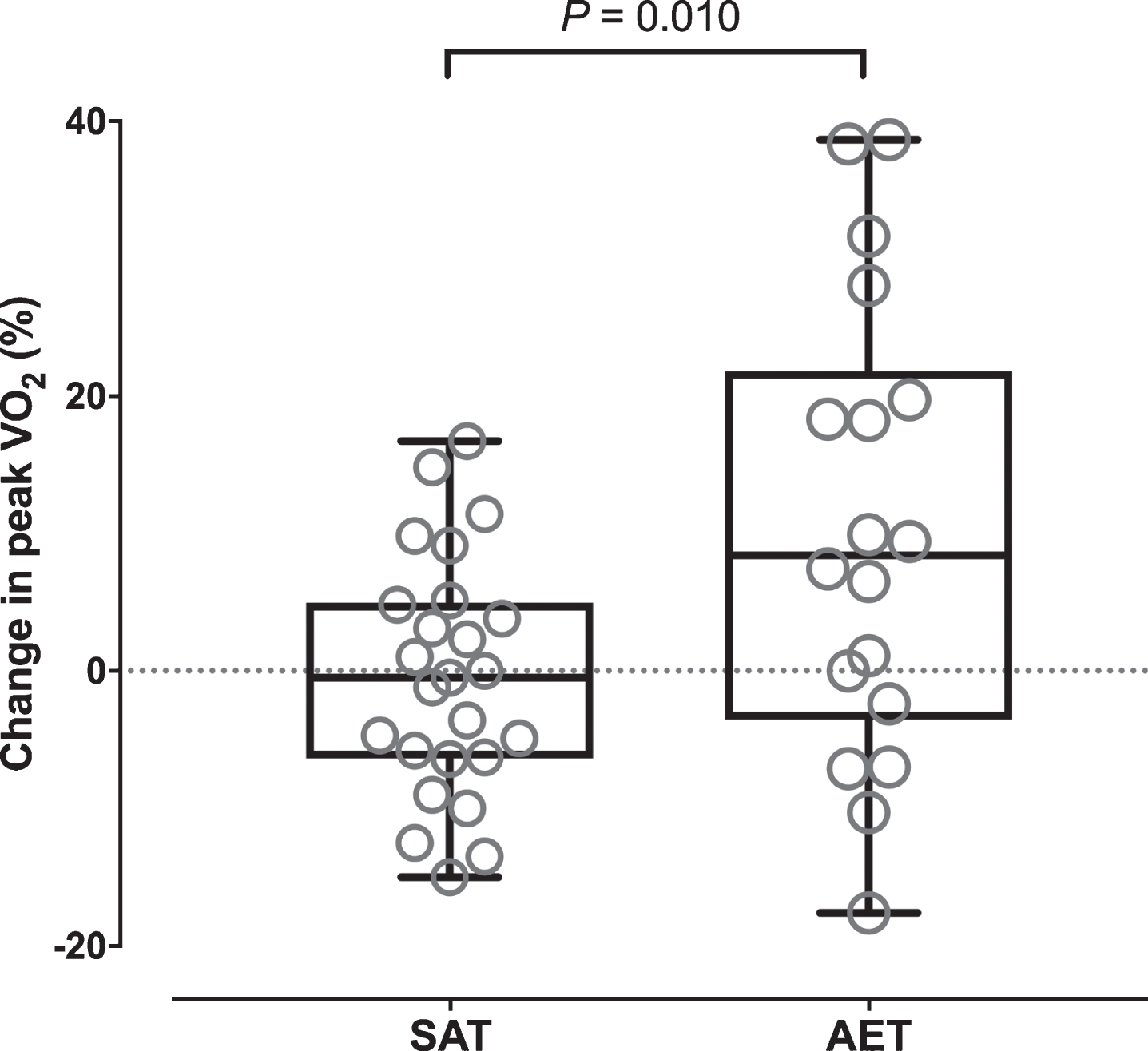
Percent changes in peak oxygen uptake (VO2) over 12 months of aerobic exercise training (AET, n = 18) versus stretching and toning program (SAT, n = 25) in patients with amnestic mild cognitive impairment. p-value was calculated by independent t-test based on complete case analysis.
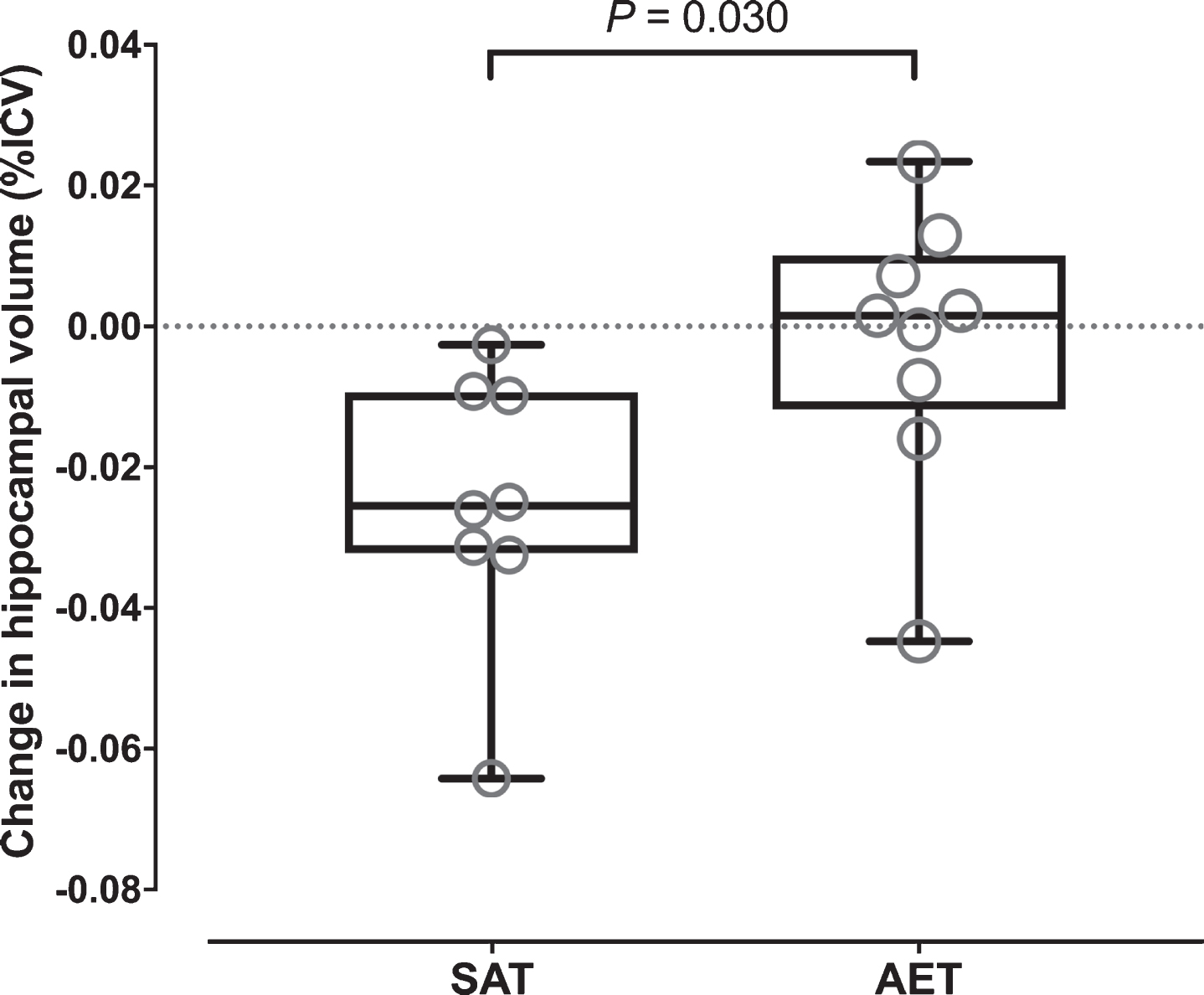
Changes in the hippocampal volume over 12 months of aerobic exercise training (AET, n = 9) versus stretching and toning program (SAT, n = 8) in amyloid positive aMCI patients. p-value was calculated by independent t-test. aMCI, amnestic mild cognitive impairment.
In this study, we observed that although AET or SAT could not prevent or slow brain atrophy and cortical Aβ accumulation over 12 months across all participants, hippocampal atrophy was reduced by AET in amyloid positive participants when compared with the SAT group (Fig. 3). Previously, a 10-year history of aerobic exercise engagement has been shown to inversely correlate with the lower level of mean cortical Aβ deposition in cognitively normal old adults [10, 39]. In addition, 6 months of AET intervention increased bilateral hippocampal volumes in old MCI women, [40], and another 6-month trial with multicomponent exercise program prevented the global cortical atrophy in aMCI patients [38]. Moreover, a 26-week RCT of AET and SAT programs showed that individual changes in cardiorespiratory fitness were associated with changes in memory performance and hippocampal volume in patients with probable AD dementia [12]. Our findings that hippocampal atrophy was reduced by AET in amyloid positive participants suggest that the hippocampal plasticity in response to AET may be sensitized in the presence of brain amyloid in amnestic MCI patients [41]. However, a careful interpretation of our findings is needed because the small sample size of this study and changes in brain AD pathology is not necessarily related to improvement in neurocognitive function as demonstrated in pharmacological AD drug trials [42].
There are several potential mechanisms that may explain improved cognitive function in our aMCI patients. These include, but not limited to, the improved cerebral perfusion and white matter fiber integrity and the increased release of neurotrophic factors such as brain-derived neurotrophic factor (BDNF). For example, physically active middle-aged and older athletes have shown better cognitive performance than their sedentary control subjects, as accompanied by the higher posterior cingulate perfusion [43, 44]. The cerebral neuronal fiber integrity measured by diffusion tensor imaging has also been shown to benefit from exercise training in older adults [45, 46]. During physical exercise, skeletal muscle contractions can upregulate the hippocampal BDNF expression [47] and may lead to the adult hippocampal neurogenesis [8, 48]. Therefore, improved cognitive performance in aMCI patients may be explained by these physiological mechanisms(s) that we did not address specifically in this study.
Although our AET program significantly increased peak VO2 at group level, substantial individual variability was observed, which included several participants who did not change or even decreased their peak VO2. We think that this individual variability is related to a few potential reasons. First, this trial used home-based exercise program, and this flexibility in program may have influenced participants’ adherence to the prescribed training. Second, non-responders are common in many exercise training studies, although its underlying mechanism remains to be elucidated. Several studies have suggested that trainability is predicted by genetic determinants and about 20% of the general population does not respond to exercise training [49]. Nevertheless, in our study, the prevalence of non-responders was higher than reported, which suggests that non-adherence to the program and inadequate stimulus of exercise training intensity are likely to be the main reason for the observed individual variability.
This proof-of-concept investigation has several strengths. First, this is the first study in aMCI patients to assess the effects of AET on neuropsychological function and imaging biomarkers of AD, including cortical Aβ plaque deposition. Second, 12 months of intervention offered a relatively long-time window to track changes of these measurements. Third, the test-retest reliability of cognitive function, brain volume, Aβ deposition, and peak VO2 assessments showed strong intra-class correlations and indicates the robustness of our measurements (Supplementary Table 6). Fourth, peak VO2, the gold standard measure of cardiorespiratory fitness, provided an objective measurement of exercise benefits on cardiovascular heath [14], and the criteria to monitor the improvement of physical fitness in previously sedentary aMCI patients.
This investigation has several limitations. First, sample size was small, though it was designed as a proof-of-concept study. Also, the attrition rate was high (∼31%), which may bias outcome measures. MRI and PET scans were completed only in a subset of eligible participants, and PET scanning was implemented after trial initiation. In addition, completion rates of MRI and PET scans were 59% and 52%, respectively. Therefore, caution should be taken when interpreting our findings. Second, given the reported benefits of resistance exercise on neuropsychological function [33, 34], our SAT program, which included theraband low resistance exercise, may not have been an ideal control group. However, having an active control group improved participants’ motivation in the study and provided similar investigator contact and attention to both the AET and SAT participants. Third, APOE genotype analysis was performed only in a subset of participants which limited statistical power to analyze the interaction effect of APOE genotype and treatment on outcome measures (e.g., APOE4 carrier/non-carrier versus amyloid+/-). Previous studies have reported that AET-related improvement of cognitive performance is attenuated in APOE4 carriers [50]. The cortical Aβ deposition has also been shown to correlate with a 10-year history of exercise participation in cognitively normal APOE4 carriers [39]. Therefore, our findings could have been influenced by the APOE4 status and need confirmation by the future studies with a larger sample size. Fourth, the lack of naming tests (e.g., Boston Naming Test) in our cognitive outcome measures may have limited a sensitivity in detecting intervention effects because anomic aphasia is a common and initial impairment in AD dementia patients [51]. At last, a lack of the cognitively healthy elderly group limited us to compare the observed neurocognitive changes with healthy control subjects.
Despite these limitations, participation in AET or SAT program was associated with improved performance on memory and executive function tests in previously sedentary aMCI patients, although these changes were small and the interventions did not prevent progression of brain atrophy and Aβ deposition. Peak VO2 significantly increased in the AET group, reflecting improved cardiovascular health. In amyloid positive patients, hippocampal atrophy was attenuated by AET. Collectively, these findings suggest benefits of both AET and SAT exercise on neuropsychological function in aMCI patients. Further studies are needed to better understand the impact of exercise training on neuroimaging biomarkers of AD dementia in older adults.
Footnotes
Acknowledgments
We thank each of the study participants for their effort and time contributing to the study.
This work was funded by the National Institutes of Health (R01AG033106, R01HL102457, P30AG012300, and K99HL133449).
The 18F-florbetapir PET radiotracer was provided to the study by Avid Radiopharmaceuticals.