
Abstract
Background:
Gait impairment is observed in early stages of dementia, such as mild cognitive impairment (MCI), and is associated with morphological brain volume changes like atrophy.
Objective:
This study aims to characterize the brain’s grey matter (GM) volume covariance associated with gait speed in patients with amnestic mild cognitive impairment (aMCI) and non-amnestic MCI (naMCI).
Methods:
Gait speed was measured in 171 patients with MCI (age 72.0±5.1; 36.8% female; 41 with aMCI and 130 naMCI) at normal and rapid gait speeds. Brain GM covariance networks were computed using voxel-based morphometry, using the main neural correlates of gait speed in each group and for each walking condition as seed regions.
Results:
Normal gait speed correlated with GM volume in the left frontal cortex in patients with aMCI, and in bilateral caudate and left putamen in those with naMCI. Rapid gait speed correlated with GM volume in the bilateral caudate and right cerebellum in naMCI, but without any GM region in aMCI. For normal gait speed, the left caudate nucleus volume in naMCI covaried with subcortico-frontal regions, while the left frontal cortex covaried with cortical regions involving the frontal cortex in aMCI. For rapid gait speed, subcortico-frontal regions were similar as for normal speed in naMCI.
Conclusion:
Brain GM volume covariance associated with gait speed varies according to the type of MCI; it involved subcortico-frontal regions for patients with naMCI and the frontal cortex in those with aMCI.
Keywords
INTRODUCTION
Gait and cognitive performance decline with cognitive impairment, especially in older adults with neurological diseases like Alzheimer’s disease (AD) and non-AD dementia [1, 2]. Gait impairments are more severe in patients with non-AD dementia than in AD patients [1, 3]. They are even observed before the dementia stage [1, 2], such as in patients with mild cognitive impairment (MCI). MCI-related gait impairments depend on the subtype of MCI [1, 2]. They are more frequent in patients with amnestic MCI (aMCI) than those with non-amnestic MCI (naMCI) (31.5% in aMCI versus 19.4% in naMCI) [4]. The phenotype of gait impairment also depends on the subtype of MCI; gait velocity being more affected in naMCI than in aMCI [3, 4], especially in dual task condition (i.e., walking while talking) [5]. Performance of gait parameters in patients with MCI, especially dual task-related gait changes, predict the conversion to dementia [6]. In contrast to the influence of MCI subtypes on gait phenotypes, the morphological brain volume changes associated with gait impairment in patients with MCI (and its subtypes) are poorly studied.
Functional and morphological changes related to gait performance differ between normal aging and MCI, and also among MCI subtypes [7, 8]. Impaired functional connectivity between sensorimotor and frontoparietal networks has been related to slow gait speed in MCI [8]. Slow gait speed has also been associated with larger ventricular volume in MCI, even after adjusting for age, cerebrovascular conditions, and cognitive performance [7]. Few studies have investigated a morphological pattern of brain regions associated with slow gait in MCI subtypes [9, 10]. Decreased grey matter (GM) volumes have been associated with dual-task related slow gait speed in patients with MCI; these GM volumes being different between aMCI and naMCI: low GM volumes of the occipital gyrus, the cuneus, the precuneus, the parahippocampal gyrus, and the cingulate gyrus have been reported in patients with aMCI, whereas only low GM volume of the frontal lobe has been shown in patients with naMCI [10]. Additionally, in a walking task involving various aspects of locomotion (i.e., gait and balance conditions) such as the Timed Up and Go (TUG), increased TUG time was associated with lower total white matter, total GM, and left and right hippocampal volume in patients with naMCI, but not in patients with aMCI [9]. These findings suggest that the pattern of decreased brain volumes associated with MCI-related gait performance depends on the subtype of MCI (i.e., aMCI versus naMCI).
In addition to the methods assessing functional and structural connectivity, anatomical structural covariance—a method measuring the brain’s topographical organization—allows to map the pattern of covariance between volumes of different GM regions that subserve a particular motor or cognitive function, such as gait speed [11]. In a recent study using anatomical structure covariance methods, we demonstrated that the volumes of distinct brain regions were positively associated with gait speed in aging depending on the walking conditions (i.e., normal walking, rapid walking, or walking while talking) in non-demented older adults [12]; lower gait speed being associated with lower GM volumes. However, the non-demented older participants included in this study combined cognitively intact individuals with aMCI and naMCI patients, preventing a distinction between older adults with intact cognition and those with early sign of neurodegeneration.
This study aims to characterize the brain GM volume covariance associated with gait speed in patients with aMCI and naMCI. As gait performance and neural correlates differed between aMCI and naMCI [13, 14] and brain GM volume covariance differs between MCI subtypes [15], we hypothesized that brain GM volume covariance associated with gait speed will differ between patients with aMCI and naMCI. Establishing the structural brain region associated with gait speed in patients with aMCI and naMCI will disentangle the pathophysiological mechanisms associated with gait impairment in older adults with early signs of dementia.
MATERIAL AND METHODS
Design
The current study uses a subgroup of participants enrolled in the “Gait and Alzheimer Interactions Tracking” (GAIT) study [16]. This study used a cross-sectional design with the global aim to examine the relationship between spatiotemporal performance and brain structures in cognitively healthy individuals (CHI), and in patients with MCI and major neurocognitive disorders.
Participants
For the current study, we selected participants with MCI—aMCI and naMCI—from participants enrolled in the GAIT study. Participants were recruited between November 2009 and November 2015. They were referred to the memory clinic of Angers University Hospital (France) for cognitive complaint. A total of 41 patients with aMCI and 130 with naMCI were identified using the following inclusion criteria: community-dwelling individuals aged 65 years and over with an adequate understanding of French. Exclusion criteria were acute medical illness in the past month, extrapyramidal rigidity of the upper limbs, neurological and psychiatric diseases other than cognitive impairment, severe medical conditions affecting gait with an inability to walk for 15 minutes unassisted, dementia, morphological or vascular abnormalities (i.e., normal pressure hydrocephalus, stroke) on the brain MRI, absence of brain MRI, and absence of gait speed quantification.
Clinical assessment
Participants had a standardized medical examination, neuropsychological and gait assessments, and MRI of the brain. Age, sex, the number of drugs taken daily, use of psychoactive drugs including benzodiazepine, antidepressant and neuroleptic, body mass index (kg/m2), Mini-Mental Status Examination (MMSE) [17] and Frontal Assessment Battery (FAB) scores [18] were recorded. In addition, a comprehensive neuropsychological assessment was performed during a face-to-face interview by a neuropsychologist. The diagnosis of cognitive status (i.e., MCI) was made during a multidisciplinary meeting. MCI was defined according to international standard criteria [19] and two subtypes were distinguished: aMCI and naMCI. Patients with isolated memory deficits were included in the aMCI group, while those with non-memory domain deficits (i.e., attention, language, or executive function) in the naMCI group. Walking speed at steady-state walking was measured with a GAITRite® system (Gold walkway, 972 cm long, active electronic surface area 792×610 cm, total 29,952 pressure sensors, scanning frequency 60 Hz; CIR System, Havertown) following the European guidelines for spatiotemporal gait analysis in older adults [20]. Participants were asked to walk 1) at their usual self-selected walking speed and 2) rapid walking speed in a quiet well-lit corridor, and wearing their own footwear. Each participant completed one trial per walking condition. To avoid acceleration and deceleration effects, participants started walking one meter before reaching the electronic walkway and completed their walk one meter beyond it.
Brain volume assessments
Imaging of the brain was performed with a 1.5-Tesla MRI scanner (Magnetom Avanto, Siemens Medical Solutions, Erlangen, Germany). The MRI was performed within 3 months after the clinical assessment. A standard MRI protocol was applied [21] and included 3D T1-weighted magnetization-prepared rapid acquisition gradient echo (MP-RAGE) axial images (acquisition matrix = 256×256×144, FOV = 240 mm×240 mm×187 mm, TE/TR/TI=4.07 ms/2170 ms/1100 ms). Image preprocessing was performed using SPM12 running on MATLAB 7.14.0.739 (Mathworks, Natick, MA, USA). The images were segmented into GM and white matter. Affine registered tissue segments were used to create a custom template using the DARTEL (diffeomorphic anatomical registration using the exponentiated lie algebra) approach [22]. For each participant, flow fields were calculated during a template creation, which described the transformation from each native GM image to the template. These templates were then applied to each participant’s GM image. The VBM analysis was based on modulated GM images, where the GM value for each voxel was multiplied by the Jacobian determinant derived from spatial normalization to preserve the total amount of GM from the original images [23]. The resulting modulated and normalized images were then smoothed with a Gaussian kernel of 8 mm FWHM. Furthermore, the volumetric 3D T1-weighted images were segmented using the FreeSurfer software package (version 5.1.0) to calculate total cranial brain and white matter abnormality (WMA) volumes [22]. WMA has been defined as small-scattered foci of MRI signal abnormalities (T1 hypointensities) in the cerebral white matter. WMAs calculated on T1 images with this method have been shown to be highly correlated with manual and semi-manual measurements from T2/FLAIR (r > 0.93 when including extreme values; >0.72 when excluding extreme values) [24].
Ethics
The study was conducted in accordance with the ethical standards set forth in the Helsinki Declaration (1983). The study protocol was approved by the Angers Ethics Committee, France. Each participant gave written informed consent for research.
Statistics
The participants’ characteristics were summarized using means and standard deviations or frequencies and percentages, as appropriate. Participants were separated into aMCI and naMCI. Comparisons between groups were performed using an unpaired t-test or Chi-square test, as appropriate. First, brain GM volumes were mapped according to gait speed. To do so, gait speeds for the two walking conditions (normal and rapid walking) were entered as covariates of interest in two separate multiple regression models in which aMCI and naMCI participants were entered as two separate groups. T-contrasts were set to identify voxels that correlated with gait speed in each group assuming that decreased gait speed would be associated with decreased GM volumes. The significance of each effect of interest was determined using the theory of Gaussian fields (40). A cluster-corrected p-value of <0.05 was used as a statistical threshold. Each model was adjusted by age, sex, total intracranial volume, and WMA. A correction for non-stationary smoothness was applied using the implementation of this method in the VBM5 toolbox, which is necessary to avoid false positives or decreased sensitivity when using cluster-size tests (37).
Secondly, to determine the brain GM volumes’ covariances associated with gait speed, the peak voxels in each group reported in the previous analysis were used as regions of interest (ROIs) to seed brain GM volume covariance (in each group separately). The brain GM volumes within these ROIs were calculated and extracted from a 4-mm radius sphere around the coordinates of these ROIs from the modified GM images. A correlation analysis was performed by entering the extracted brain GM volumes from each ROI as the covariate of interest. The seed regions were included in the identified brain GM volumes’ covariance analyses associated with gait speed. Each model was adjusted by the same covariates (i.e., age, sex, total intracranial volume, and WMA) and with the non-stationary smoothness correction as in the second analysis, and a cluster-corrected p-value of <0.05 was used as a threshold. Specific contrasts were set to identify each ROI voxel that expressed a positive correlation.
RESULTS
Clinical characteristics are presented in Table 1. This sample of 171 patients with MCI (age: 72.0±5.1) with a majority of men (63.2%) is not highly educated (less than 2% completed high school or university). Both groups of patients with MCI presented similar global cognitive performances (MMSE = 27.1±1.9) with better executive performances in the aMCI group than the naMCI group. The group of naMCI took more drugs per day than the aMCI group. However, both MCI subtypes are taking the same amounts of psychoactive drugs. The group of aMCI tends to walk faster than the naMCI group (111.1±14.8 versus 104.8±20.0 cm/s; p = 0.068). Total cranial volume and total white matter abnormality volume were similar between both groups. Rapid gait speed was correlated with MMSE (r = 0.27; p = 0.002), while it was borderline for usual gait speed MMSE (r = 0.17; p = 0.053) in naMCI. No correlation between gait speed (i.e., rapid and usual) and MMSE was reported in aMCI. Furthermore, no correlation between gait speed (i.e., rapid and usual) and FAB was reported in naMCI and aMCI.
Clinical characteristics of participants (n = 171)
MCI, mild cognitive impairment; SD, standard deviation; MMSE, Mini-Mental Status Examination; FAB, Frontal battery assessment; *Comparisons based on unpaired t-test or Chi-square test, as appropriate; †including benzodiazepine, antidepressant and neuroleptic; ‡high school and above; ||defined as MRI signal abnormalities (i.e.; T1 hypointensities) and measured using FreeSurfer software. p-value significant (i.e., <0.05) indicated in bold.
Significant correlations between gait speed and brain volume are presented in Table 2 for naMCI and in Table 3 for patients with aMCI. For the normal walking condition, gait speed was correlated with GM volume in left frontal cortex (inferior orbitofrontal gyrus) in patients with aMCI and in bilateral striatum in those with naMCI. For the rapid walking condition, walking speed was correlated with the GM volume in bilateral striatum and right cerebellum in patients with naMCI, but in no regions for those with aMCI.
Correlation between gray matter regions and gait speed for normal walking and rapid walking in non-amnestic MCI individuals
*p≤0.001 uncorrected; ***p≤0.05 cluster-corrected. Max T, maximum T statistic of each cluster; R, right; L, left; s.c., same cluster.
Correlation between gray matter regions and gait speed for normal walking and rapid walking in amnestic MCI individuals
*p≤0.001 uncorrected; ***p≤0.05 cluster-corrected. Max T, maximum T statistic of each cluster; R, right; L, left; s.c., same cluster.
Based on the first analysis, the left putamen (MNI coordinates: –20, 18, 8) for patients with naMCI and the left inferior orbitofrontal cortex (MNI coordinates: –38, 41, –14) for those with aMCI were selected as ROIs for the normal walking condition; and the right putamen (MNI coordinates: 20, 17, 2) was selected for patients with naMCI for the rapid walking condition. Structural covariance analysis was obtained using these ROIs as seeds (Tables 4 and 5; Figs. 1–3).
Gray matter structural covariance networks associated with in non-amnestic MCI individuals (p≤0.05 cluster-corrected)
Max T, maximum T statistic of each cluster; R, right; L, left; s.c., same cluster.
Gray matter structural covariance networks in amnestic MCI individuals (p≤0.05 cluster-corrected)
Max T, maximum T statistic of each cluster; R, right; L, left; s.c., same cluster.
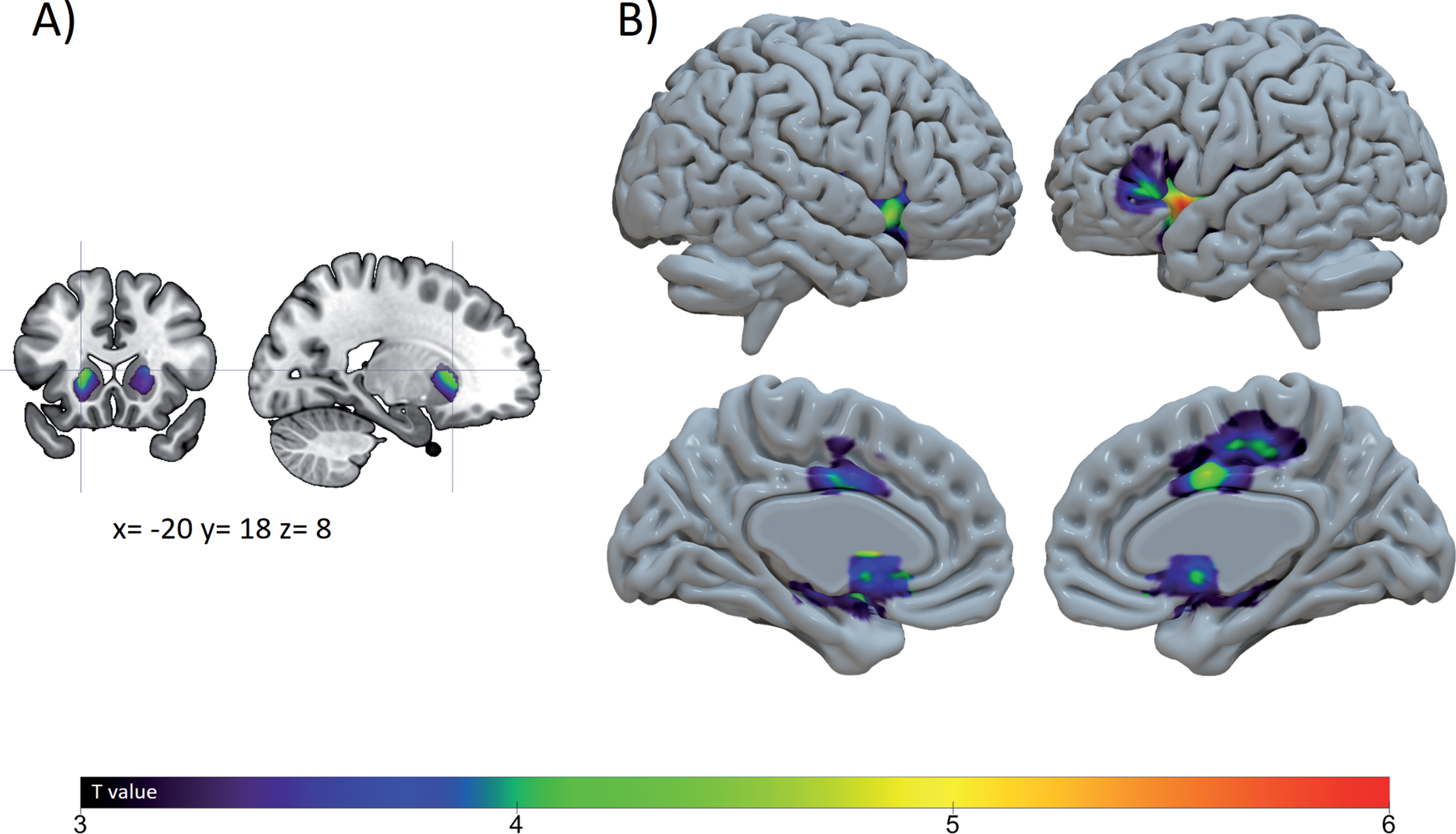
Correlations and structural covariance analysis between gray matter volume and normal gait speed in non-amnestic MCI. Correlation between gray matter regions and normal gait speed in non-amnestic MCI (A) and gray matter structural covariance networks obtained by using this ROIs as seed (B).

Correlations and structural covariance analysis between gray matter volume and rapid gait speed in non-amnestic MCI. Correlation between gray matter regions and rapid gait speed in non-amnestic MCI (A) and gray matter structural covariance networks obtained by using this ROIs as seed (B).

Correlations and structural covariance analysis between gray matter volume and normal gait speed in amnestic MCI. Correlation between gray matter regions and normal gait speed in amnestic MCI (A) and gray matter structural covariance networks obtained by using this ROIs as seed (B).
For the normal walking condition, the brain regions anchored to the left putamen covaried with an extended cluster including the bilateral putamen, pallidum, insula and inferior frontal gyrus (left pars triangularis and right pars orbitalis), the left superior temporal gyrus and the right rolandic operculum; and an additional smaller cluster in the right middle cingulate cortex in patients with naMCI (Table 4; Fig. 1). The brain regions anchored to the seed of the left orbitofrontal cortex covaried with a large cluster extending from the left orbitofrontal cortex to right medial frontal gyrus in patients with aMCI (Table 5; Fig. 3).
For the rapid walking condition, the brain regions anchored to the right putamen covaried with the same two clusters found for the normal walking condition in patients with naMCI, with the additional involvement of the left hippocampus and right parahippocampal gyrus in the large cluster (Table 4; Fig. 2).
DISCUSSION
This study aimed to characterize the brain GM volume covariance associated with gait speed in patients with aMCI and naMCI separately. We first identified two different GM regions correlated with normal gait speed: the left putamen in patients with naMCI and the left inferior orbitofrontal cortex in those with aMCI; for the rapid gait speed condition, we only found a cluster in the right putamen in patients with naMCI, but no GM regions associated with rapid gait speed in those with aMCI. The covariance analysis revealed similar brain volumes associated with normal and rapid gait speed in patients with naMCI including bilateral subcortico-frontal regions. For patients with aMCI, covariance analysis revealed a “pure” frontal region associated with normal gait speed.
The GM covariance analysis associated with normal and rapid gait speeds in patients with aMCI and naMCI revealed a double dissociation. The neural substrate of gait control differs between patients with aMCI and naMCI: GM patterns associated with gait speed during dual task performance (i.e., walking while counting) have been already reported as different between those with aMCI and naMCI [10]. This double dissociation is also supported by the correlation between gait speed and global cognition in naMCI, while no correlation was reported in aMCI. Various factors may explain these differences between patients with aMCI and naMCI. The morphological pattern of atrophy differs between patients with aMCI and naMCI [25, 26]. Risk factors also vary between patients with aMCI and naMCI [19], especially for cardio- and cerebrovascular risk factors that are more prevalent in naMCI than in aMCI [27]. The underlying neuropathological substrates—with an increased amyloid deposition in patients with aMCI in comparison to those with naMCI [28]—may also contribute to these differences. This double dissociation between aMCI and naMCI revealed by the GM covariance associated with gait speed suggests differences in the neurobiological bases of gait speed between aMCI and naMCI. Future studies should include additional facets of gait, such as clinical gait characteristics (i.e., frontal versus parkinsonian gait), in order to confirm these different brain networks involved in gait control between aMCI and naMCI.
Gait speed in patients with aMCI is associated with cortical frontal regions. Cortical thickness in the frontal lobe has been previously related to executive function in a study contrasting executive performances in patients with aMCI [29]. Executive functions play a major role in the control of gait in older adults [30–32]. Furthermore, motor disturbances in AD have been associated with an amyloid-mediated cholinergic dysfunction [33]; these latter findings, associated with the observation of a dense cholinergic innervation of the frontal lobe, support the association of this frontal network with gait speed in aMCI [34]. However, no GM region was associated with rapid gait speed in aMCI; this absence of association may reflect that rapid gait speed represents a “very” automatic behavior relatively independent of brain control (akin to automatic gait control in younger adults [35]). The vulnerability of the frontal lobe of patients with aMCI and the tight relationship between gait and executive functions may explain that “pure” frontal regions are associated with gait speed in aMCI.
A bilateral subcortico-frontal network has been associated with gait speed in patients with naMCI. Especially, the left putamen has been associated with normal gait speed, while the right putamen with rapid gait speed. Putamen volume in both right and left sides has been associated with faster gait decline in older adults [36]. This dissociation between left and right putamen for normal and rapid walking, respectively, may refer to the different brain control underlying walking at normal and rapid gait speeds [12]. The putamen has been associated with gait speed in various neurological conditions, such as stroke [37] or multiple sclerosis [38]. NaMCI subtype, as opposed to aMCI, is less often associated with an underlying AD pathology, but frequently with dementia with Lewy bodies or frontotemporal dementia [19, 39]. Gait is more frequently and severely disturbed in patients with naMCI in comparison to those with aMCI [3, 27] (as presented in the current cohort, with slower gait speeds in naMCI than in aMCI). Similarly, the presence of gait abnormalities in non-demented older adults is a predictor of the development of a non-AD dementia [2], especially vascular dementia [1]. The combination of neurodegenerative diseases affecting the subcortical regions (i.e., dementia with Lewy bodies) and the cortical ones (i.e., frontotemporal dementia) found in patients with naMCI and the presence of gait abnormalities related to these conditions [40, 41]—that are even present at the stage of MCI [42]—may contribute to this subcortico-frontal network related to gait speed in patients with naMCI.
Comparing the GM volume covariance associated with gait speed in such a high number of patients with aMCI to those with naMCI represents the main strength of this study. However, this study is not without its limitations. First of all, we should acknowledge that participants were recruited from a memory clinic; that may consecutively limit the generalization of the study’s findings to the entire aging population (i.e., recruitment bias). Furthermore, we do not have a control group composed of older adults without MCI or cognitive complaint that would allow comparing the gait-related brain changes in MCI subtypes and cognitively normal older adults. Second, in comparison to other network-based or connectivity neuroimaging approaches, structural covariance networks are estimated on a group of images and not on an individual basis, which limits the ability to directly correlate individual performance with the integrity of the structural covariance network. Thirdly, we should highlight that our study sample includes a larger number of naMCI than aMCI patients (130 versus 41) and that the naMCI group may include a variety of conditions from non-neurodegenerative (i.e., anxiety, depression) to neurodegenerative (mainly non-AD conditions, such as dementia with Lewy bodies or frontotemporal dementia). Fourth, the structural covariance analysis precludes correlation of behavioral/cognitive score with the integrity of the network, as these networks are population-based covariance maps. Results from multivariate approaches can be more easily interpreted as brain networks given that they simultaneously evaluate covariance of features across brain regions and cognitive/behavioral measures. In comparison to multivariate approaches, univariate approaches employ very conservative voxel-wise multiple comparison corrections, which can limit statistical power.
In conclusion, the GM volume covariance associated with gait speed reveals distinct brain regions in patients with aMCI and those with naMCI: cortical regions involving the frontal lobe in patients with aMCI and subcortico-frontal regions in patients with naMCI. This analysis demonstrated various underlying brain changes associated with gait modification in older adults in early stages of dementia. These results provide a rationale for the rehabilitative strategies that may be used for improving gait in patients with aMCI and naMCI.
Footnotes
ACKNOWLEDGMENTS
We acknowledge all participants included in the present study.
The study was financially supported by the French Ministry of Health (Projet Hospitalier de Recherche Clinique national n°2009-A00533-54). Gilles Allali is supported by a grant from Swiss National Science Foundation (320030_173153).