
Abstract
Oxidative stress plays an essential and early role in the pathophysiology of Alzheimer’s disease (AD). Alterations in the redox state in AD and in mild cognitive impairment (MCI) patients appear in the brain and at peripheral level. Given that it is easier to study the latter, most of the research has been focused on plasma. However, the analysis of redox parameters in whole blood cells (including erythrocytes and leukocytes) has not really been investigated. Moreover, the association of these parameters with Mini-Mental State Examination (MMSE) clinical scores, has scarcely been studied. Therefore, the aim of the present work was to analyze several redox markers in whole blood cells from male and female MCI and AD patients. Antioxidant (superoxide dismutase, catalase (CAT), glutathione peroxidase (GPx), and reductase (GR) activities, and reduced glutathione (GSH) concentration) together with oxidant parameters (oxidized glutathione (GSSG) and thiobarbituric acid-reactive substances (TBARS)) were investigated using MCI and AD (10 women and 10 men in each group) and their age-matched control groups (15 women and 15 men). The results show an altered redox state in whole blood cells from AD patients (higher CAT, GSSG/GSH, TBARS and lower GPx, GR, GSH). Some of these redox parameters are already affected in MCI patients (higher TBARS and lower GPx and GR activities) in both sexes and, consequently, they could be used as markers of prodromal AD. Since GR, GSH, GSSG, and GSSG/GSH were found to be associated with MMSE scores, they seem to be useful clinically to monitor cognitive decline in AD progression.
Keywords
INTRODUCTION
Due to the increasing average lifespan, the clinical relevance of Alzheimer’s disease (AD) is exponentially rising and is expected to become a pandemic and public health burden. Thus, it is estimated that the prevalence of AD may reach > 115 million worldwide by 2050 [1]. The sporadic form, which is the most common cause of AD (>95% of cases) has a late age of onset and it is strongly associated with aging [2, 3]. One of the main obstacles of a potential AD cure is that it is only diagnosed in later stages of the disease, in which there is already irreversible brain damage. However, numerous longitudinal follow-up studies clearly demonstrated that AD dementia is preceded by a long asymptomatic (preclinical) phase followed by a transitional stage with mild cognitive impairment (MCI) [4–6]. Thus, this intermediate stage offers an important opportunity for possible diagnosis, prevention and therapeutic interventions. It is now recognized that only a combination of biomarkers will define a patient-specific signature to diagnose AD in the future [7]. Although the accumulation of amyloid and tau proteins is considered the core pathologic hallmark for AD, other factors such as oxidative stress and inflammation, contribute enormously to its complex pathophysiology. In this context, it is now well established that oxidative stress plays a pivotal role in the pathophysiology and the progression of AD. Nunomura et al. [8] showed that oxidative stress in brain precedes the development of the neuropathological hallmarks of AD such as the extracellular senile plaques formed by amyloid-β (Aβ) peptide and the neurofibrillary tangles consisting of abnormally phosphorylated tau protein. In fact, some evidence has suggested that the Aβ deposition in certain neurons may be considered an effort to protect these cells against damage due to oxidative stress [9–11]. Aβ deposition has also been associated with neuronal lipid, protein, and DNA oxidation in animal models of AD [12–14], whereas in humans, oxidative damage to biomolecules has also been reported in the brain of both AD and MCI patients [15, 16]. In addition, several studies have shown that the oxidative alterations in AD and in MCI patients are not only limited to the brain but they have also been detected in the blood compartment [17–19]. Nevertheless, both establishing the right pattern of redox markers to analyze as well as choosing the most appropriate sample type remain a challenge in AD. Most of the studies have been focused on the search for redox markers in plasma or serum [19, 20]. However, the redox status of erythrocytes is essential for adequate oxygen delivery to the whole body. In fact, an impaired oxygen delivery to the brain causing neuronal AD dysfunction, has been considered an important factor in AD [21]. Moreover, the redox state of immune cells has been shown to be crucial for their adequate defensive functioning [17]. Actually, a higher oxidative stress has been linked to a premature immunosenescence in leukocytes from AD patients and to an uncontrolled higher release of pro-inflammatory mediators which also contributes to AD pathology [17].
Therefore, in order to identify non-invasive redox markers that can be used for an early diagnosis of AD, we decided to investigate several parameters of oxidative stress in whole blood cells (containing erythrocytes and leukocytes). Thus, antioxidant enzyme activities and compounds (superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase (GPx), glutathione reductase (GR), and reduced glutathione (GSH) concentration) as well as pro-oxidant compounds (oxidized glutathione (GSSG) and thiobarbituric acid-reactive substances (TBARS)) were investigated in whole blood cells from MCI and AD patients. In addition, differences by sex were also considered. Moreover, the relationship between each of the redox parameters studied and the degree of cognitive performance assessed by the Mini-Mental State Examination (MMSE) were also investigated.
MATERIALS AND METHODS
Subjects and clinical classification
A total of 70 volunteers were selected and divided into three experimental groups: control subjects (n = 30), MCI patients (n = 20) and mild AD (mAD) patients (n = 20). All subjects were recruited by the Neurology Department of the Hospital 12 Octubre of Madrid. The AD diagnosis was established according to the guidelines of the National Institute on Neurological Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINDS-ADRDA) [22]. For MCI subjects he following inclusion criteria applied: 1) memory complaint, corroborated by an informant; 2) objective memory impairment detected by neuropsychological evaluation; 3) largely intact general cognitive function; 4) essentially preserved activities of daily living; and 5) non-demented [23]. Disease severity and normal cognitive function was determined by a clinician’s judgment based on a structured interview with the patient and the results of the Spanish Version of the Clinical Dementia Rating (CDR) and the MMSE tests [24]. The MCI group included both amnestic and non-amnestic patients. In both MCI men and women, the proportion of amnestic subjects was 40%. Given that no statistically significant differences in the markers investigated were found between amnestic and non-amnestic patients, data are shown together. All subjects included in the study had at least, a basic education and they were able to read and write. Inclusion criteria for the age-matched control group were no memory complaints and a 0 score on the CDR test and were randomly chosen from the general population. Demographic details and MMSE test results of the different study groups are summarized in Table 1. All subjects were subjected to a clinical survey and physical examination. Those with diabetes, cardiovascular disease, cancer or chronic inflammatory diseases were not included in this study. All procedures were carried out according to the Declaration of Helsinki, and approval was obtained from the corresponding Research Ethic Committees. Written informed consent was obtained from all participants or representatives.
Demographic data and cognitive performance of control group, mild cognitive impairment (MCI) patients and Alzheimer’s disease (AD) patients. Data of age and MMSE score are reported as the first and third quartile, respectively. All control individuals had a CDR score of 0, MCI subjects of 0.5, and AD patients of 1. F, female; M, male; MMSE, Mini-Mental State Examination; CDR, Clinical Dementia Rating; n.e., not evaluated
Extraction of human blood samples
Blood samples were obtained using sodium citrate as anticoagulant. Whole blood cells (including erythrocytes and total leukocytes) were obtained as previously described [25]. Aliquots of peripheral blood were diluted 1:1 in RPMI 1640 (Gibco, Canada) and were incubated 4 h at 37°C in a saturated atmosphere of humidity and CO2. After centrifugation at 900 g 10 min, plasma was removed and whole blood cell pellets were stored at –80°C until used.
Superoxide dismutase activity
SOD activity was measured using a quantitative colorimetric assay kit (EnzyChrom™ ESOD-100, BioAssay Systems, Hayward, CA).
Catalase activity
CAT activity was quantified as previously reported by Beers and Sizer [26] with some modifications [25]. Whole blood cells were resuspended in oxygen-free phosphate buffer (pH 7.4 50 mM). Then, they were sonicated, centrifuged at 3200 g 20 min and supernatants were obtained. H2O2 (14 mM) was used as substrate. Supernatants were diluted 1:1000 prior the assay. The reaction was calculated by following the absorbance decline at 240 nm over 80 s. In the same samples, protein concentration was calculated (BCA protein assay kit (Sigma-Aldrich) and the results are expressed as units (U) of catalase activity/milligram of protein (U CAT/mg protein).
Glutathione peroxidase activity
GPx activity was analyzed by using a previous method [27] with some modifications [25]. Whole blood pellets were resuspended in oxygen-free phosphate buffer (pH 7.4 50 mM). Then, they were sonicated and after centrifugation at 3200 g at 4°C for 20 min, supernatants were collected. Human supernatants were diluted 1:30 prior the assay. Cumene hydroperoxide was used as substrate (cumene-OOH; Sigma). The activity was followed measuring the absorbance decline at 340 nm over 5 min. Protein concentration was calculated as described above. The results are expressed as units (U) of glutathione peroxidase activity/milligram of protein (U GPx/mg protein).
Glutathione reductase activity
GR activity was analyzed following a method previously described [28] with some modifications [25]. Whole blood cells were resuspended in oxygen-free phosphate buffer (pH 7.4 50 mM). Then, they were sonicated, centrifuged at 3200 g at 4°C 20 min and supernatants were collected. Human supernatants were diluted 1:5 prior the assay. GSSG (80 mM) was used as substrate and, by following the absorbance decline at 340 nm over 5 min, the activity was calculated. Protein concentration was evaluated as described above. The results are expressed as units (U) of Glutathione reductase/per milligram of protein (U GR/mg protein).
Glutathione concentration
Both reduced GSH and GSSG were measured following a fluorometric assay [29] with some modifications [25]. This method relies on the reaction capacity that glutathione (both GSSG and GSH) shows with o-phthalaldehyde (OPT), at pH 12 and pH 8, respectively, forming a fluorescent compound. Whole blood cells were resuspended in phosphate buffer (pH 8 50 mM EDTA 0.1 M). Then, samples were sonicated, 7.5 μL of HClO4 (60%) were added and they were centrifuged 10 min at 9500 g. 10 μL from supernatants were dispensed into 96 black plates. For GSH quantification, OPT (1 mg/mL) was dispensed into the wells. For the quantification of GSSG, N-ethylmaleimide (NEM, 0.04 M) was dispensed into each well and after a 30 min incubation, NaOH (pH 12) and OPT were added. After 15 min incubation with OPT, fluorescence was measured at 420 nm. Protein concentration was calculated as described above. Results are expressed as nmol of GSSG/mg protein or GSH/mg protein. In addition, GSSG/GSH ratio was calculated for each sample.
Thiobarbituric acid-reactive substances concentration
Quantification of TBARS was achieved using the commercial kit “Lipid peroxidation (MDA) Assay Kit” (Biovision, USA). To prevent further peroxidation of lipids during the preparation of the sample or during the heating step, the antioxidant butylated hydroxy-toluene (BHT) was added to the lysis buffer at a final concentration of 0.1 mM. Briefly, whole blood cells were resuspended in 300 μl MDA lysis buffer (containing BHT), sonicated and centrifuged at 13000 g for 10 min. Supernatants were collected, mixed with thiobarbituric acid (TBA) and incubated in a water bath at 95°C for 60 min. Then, after centrifugation at 13000 g 10 min, supernatants were obtained, added into a 96-well plate and absorbance at 532 nm was measured. Protein concentrations were calculated as described above. Because TBA reacts with more aldehydes than malondialdehyde, we will refer to the results obtained as TBA-reactive substances, even though the concentrations were related to a standard curve using malondialdehyde alone, and therefore, the results are expressed as nmol MDA/mg protein.
Statistical analysis
Statistical analysis of the results was performed with SPSS 21.0 (SPSS, Chicago, IL, USA) software. For comparison of variables, the nonparametric Kruskal-Wallis test was carried out followed by Mann-Whitney U test to determine significant differences between groups. The Pearson correlation coefficient was used to test for correlation between redox parameters and MMSE scores from MCI and AD patients. Two-sided p < 0.05 was considered the minimum level of significance.
RESULTS
The main characteristics of the three groups of individuals enrolled in this study are reported in Table 1. There was the same proportion of men and women in each group. The three groups comprised subjects from the same age interval. Compared to healthy controls, a higher proportion of patients with MCI and AD were apolipoprotein (APOE) ɛ3/ɛ4 carriers. The results regarding antioxidant parameters are shown in Fig. 1. AD patients showed higher CAT activity (p < 0.001) and lower GPx and GR activities and GSH concentration (p < 0.001) than age-matched controls, and even lower GPx activity and GSH concentration than MCI patients (p < 0.01). MCI patients also showed higher CAT activity (p < 0.001) and lower GPx and GR activities (p < 0.001) than controls. With respect to oxidant parameters (Fig. 2), AD patients showed higher GSSG, GSSG/GSH ratio, and TBARS concentrations (p < 0.05 for GSSG; p < 0.001 for GSSG/GSH and TBARS) than age-matched controls. MCI patients showed higher GSSG/GSH ratio (p < 0.01) and TBARS concentration (p < 0.001) than controls. Within MCI and AD groups, subjects were further classified depending on the APOE genotype, although no statistically significant differences were found in any redox marker due to the presence of APOE ɛ3/ɛ3 or ɛ3/ɛ4 genotype.
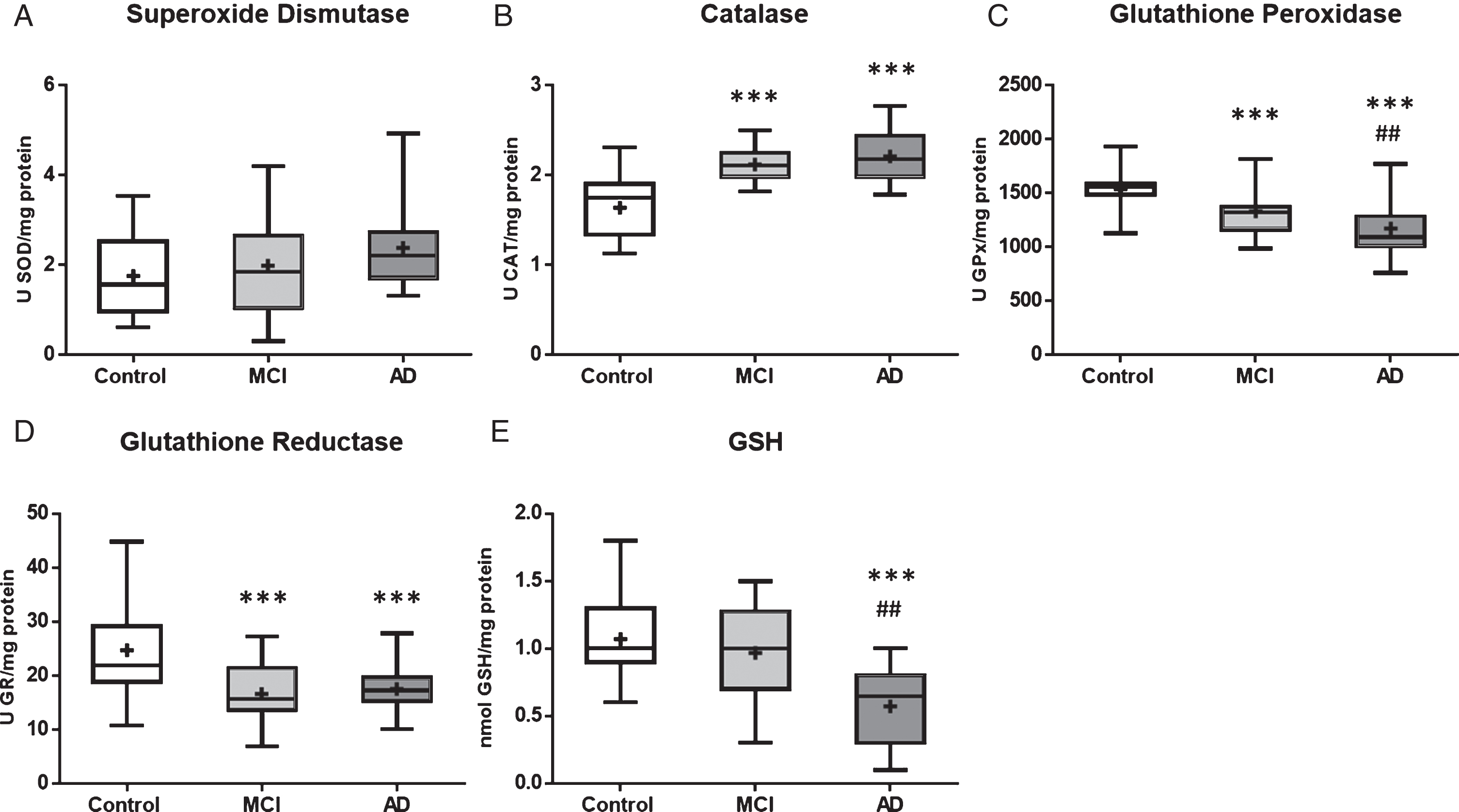
Antioxidant parameters in blood cells from mild cognitive impairment (MCI) and Alzheimer’s disease (AD) patients versus age-matched controls. A) Superoxide dismutase activity; B) Catalase activity; C) Glutathione peroxidase activity; D) Glutathione reductase activity; E) Reduced glutathione concentration. The central rectangle spans the first to the third quartile (the interquartile range or IQR) and the horizontal bar depicts the median of data. Error bars depict the highest and lowest point within each data set. ***p < 0.001 with respect to age-matched controls. # #p < 0.01 with respect to MCI patients.
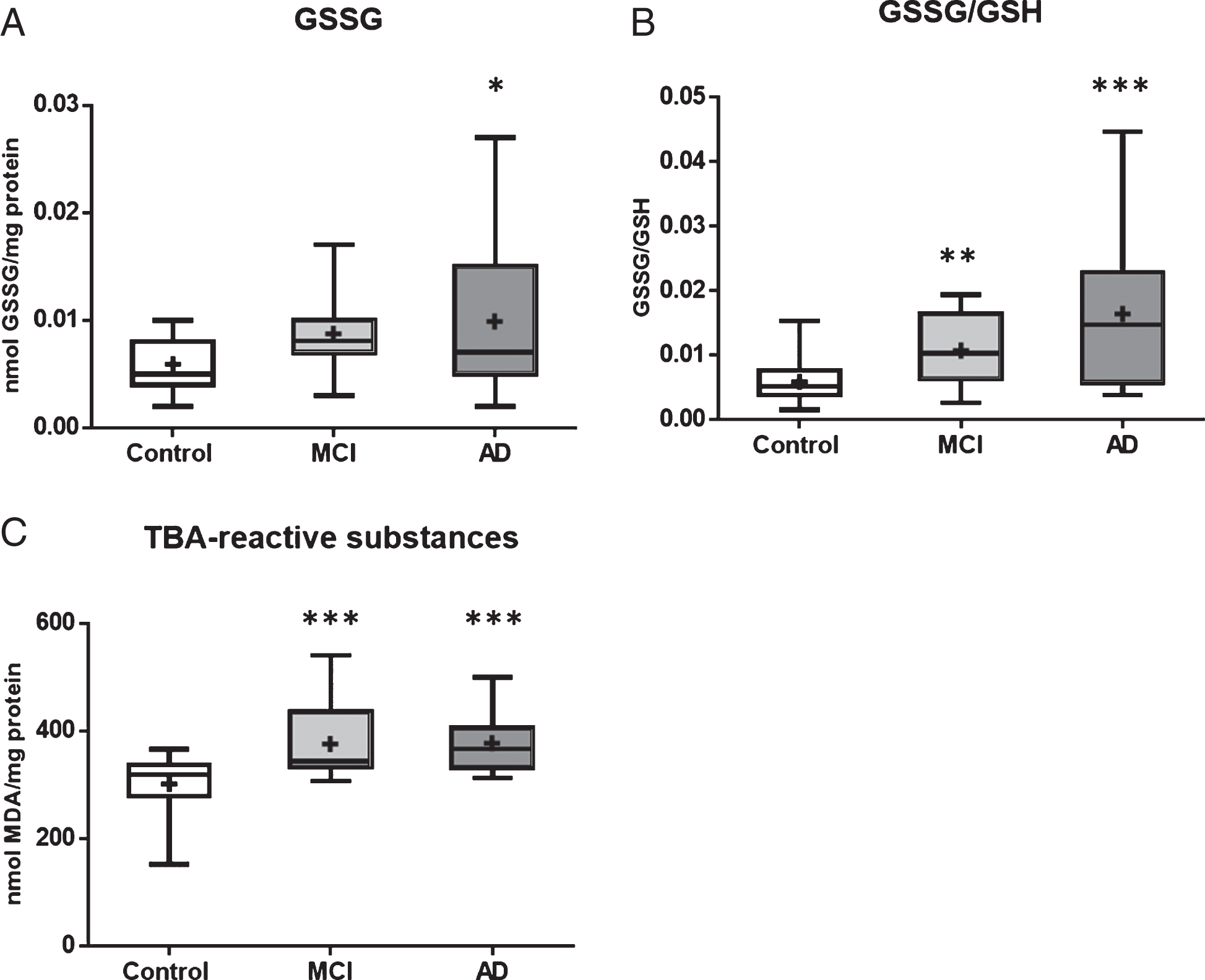
Oxidant parameters in blood cells from mild cognitive impairment (MCI) and Alzheimer’s disease (AD) patients versus age-matched controls. A) Oxidized glutathione (GSSG) concentration; B) GSSG/GSH ratio; C) TBA-reactive substances concentration. The central rectangle spans the first to the third quartile (the interquartile range or IQR) and the horizontal bar depicts the median of data. Error bars depict the highest and lowest point within each set of data. *p < 0.05; **p < 0.01; ***p < 0.001 with respect to age-matched controls.
Previous data were analyzed including total population. Then, an additional analysis was performed subdividing groups by sex. With respect to sex-related differences in antioxidant parameters (Fig. 3), control men showed higher SOD and GR activities (p < 0.01; p < 0.05) and lower CAT (p < 0.05) than control women. Within MCI and AD patients no significant differences in antioxidant parameters were found due to sex. Nevertheless, AD women showed higher SOD and CAT activities (p < 0.01; p < 0.05) and lower GPx, GR, and GSH concentration (p < 0.05) than age-matched control women. AD men showed higher CAT activity (p < 0.001) and lower GPx, GR, and GSH (p < 0.001) than age-matched control men and also lower GPx (p < 0.001) and GSH (p < 0.05) than MCI men. With respect to individuals with MCI, MCI women showed lower GPx and GR activities (p < 0.01; p < 0.05; respectively) than control women, whereas MCI men showed higher CAT (p < 0.001) and lower GPx (p < 0.05) and GR activities (p < 0.01) than control men. With regard to oxidant parameters (Fig. 4), no statistically significant differences were found within sexes, either in control, MCI, or AD groups. However, both AD men and women displayed higher GSSG/GSH ratios (p < 0.05; p < 0.01; respectively) and higher TBARS (p < 0.01) than their controls. In addition, both MCI men and women showed higher TBARS (p < 0.05; p < 0.01; respectively) than their sex-matched controls.
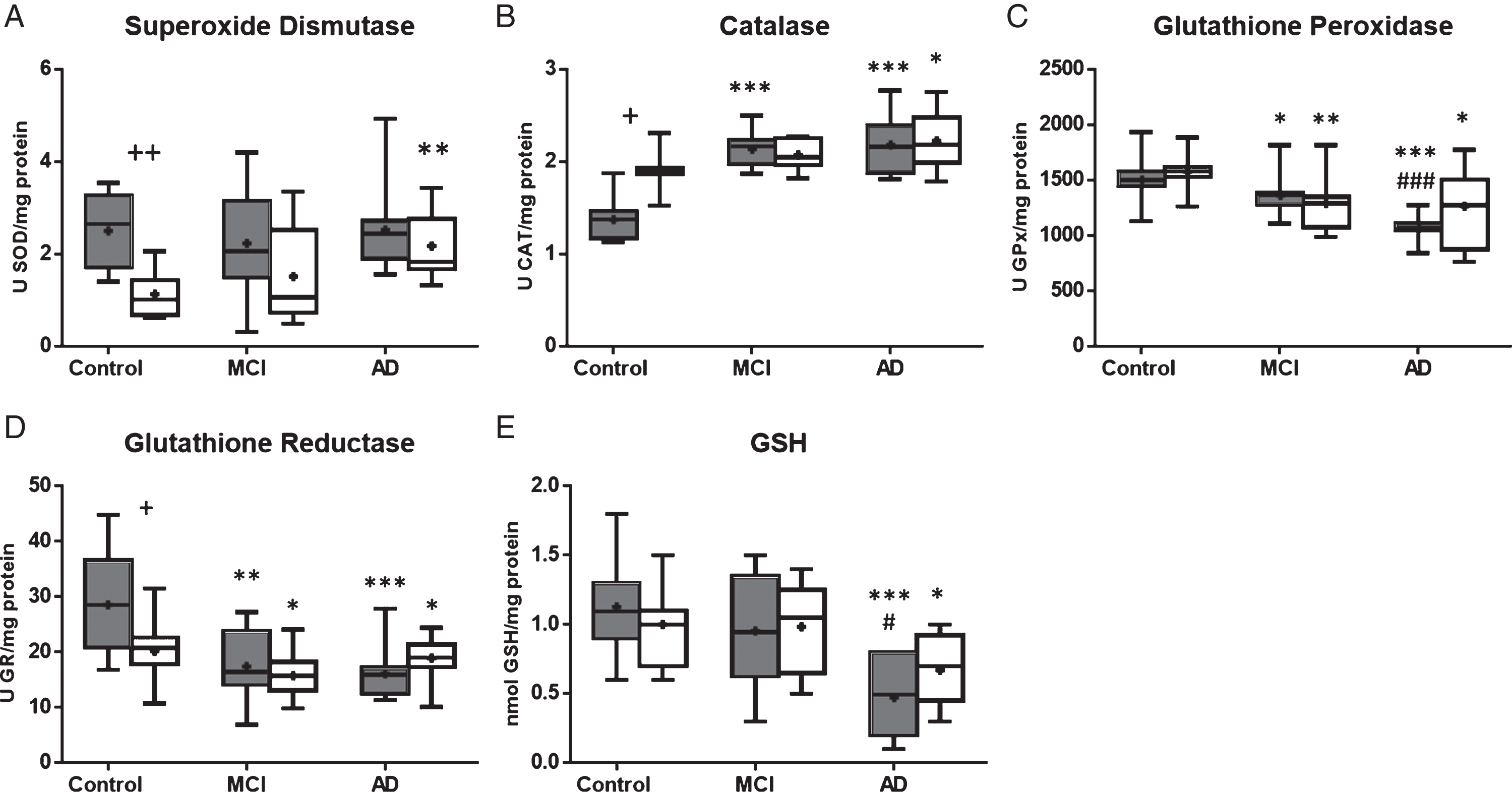
Antioxidant parameters in blood cells from men (grey boxes) and women (white boxes) with mild cognitive impairment (MCI) (N = 10, both men and women groups) and Alzheimer’s disease (AD) patients (N = 10, both men and women groups) versus age-matched controls (N = 15, both men and women groups). A) Superoxide dismutase activity; B) Catalase activity; C) Glutathione peroxidase activity; D) Glutathione reductase activity; E) Reduced glutathione concentration. The central rectangle spans the first to the third quartile (the interquartile range or IQR) and the horizontal bar depicts the median of data. Error bars depict the highest and lowest point within each set of data. *p < 0.05; **p < 0.01; ***p < 0.001 with respect to age and sex-matched controls. #p < 0.05; # # #p < 0.001 with respect to sex-matched MCI patients. +p < 0.05; ++p < 0.01 between sexes within the same group.
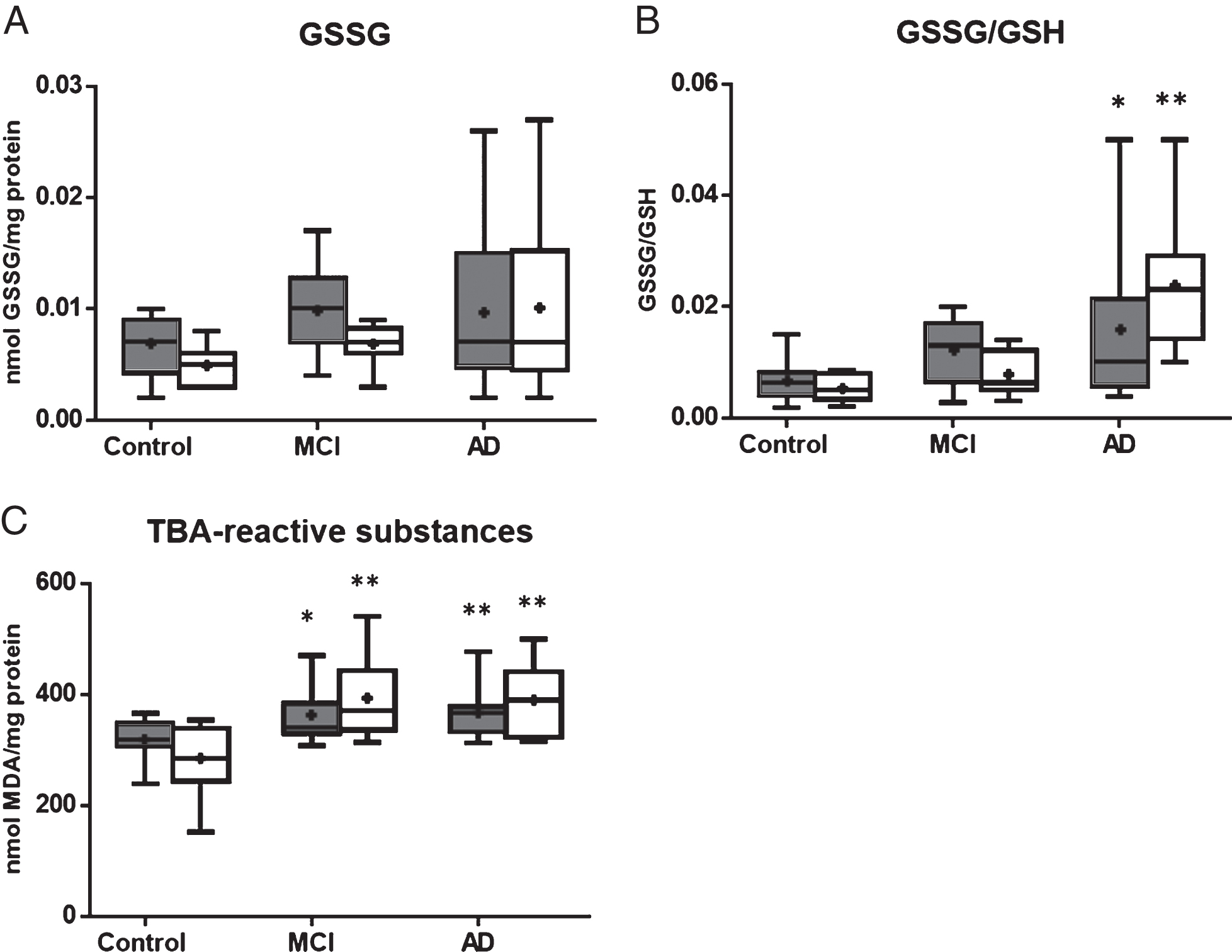
Oxidant parameters in blood cells from men (grey boxes) and women (white boxes) with mild cognitive impairment (MCI) (N = 10, both men and women groups) and Alzheimer’s disease (AD) patients (N = 10, both men and women groups) versus age-matched controls (N = 15, both men and women groups). A) Oxidized glutathione (GSSG) concentration; B) GSSG/GSH ratio; C) TBA-reactive substances concentration. The central rectangle spans the first to the third quartile (the interquartile range or IQR) and the horizontal bar depicts the median of data. Error bars depict the highest and lowest point within each set of data. *p < 0.05; **p < 0.01 with respect to age and sex-matched controls.
In addition, the individual association of each redox parameter with cognitive decline was further investigated to order to identify which redox marker can be used to distinguish between MCI and AD patients. For this purpose, the Pearson correlation coefficient was calculated for each redox marker and the MMSE scores obtained for MCI and AD groups together, including men and women. Regarding antioxidant parameters, a statistically significant positive correlation was found between GR activity and GSH concentration (R = 0.350, R = 0.371, respectively, p < 0.05) and MMSE score. With respect to oxidant parameters, a statistically significant negative correlation was found between GSSG concentration and GSSG/GSH ratio (R = –0.373, R = –0.332, respectively, p < 0.05) and MMSE score.
DISCUSSION
Research on AD is moving forward at a very rapid pace. Clinical investigators are trying to move the diagnostic threshold for dementia and AD back to earlier stages of progression, while other scientists are correspondingly attempting to define biomarkers and genetic susceptibilities that will add specificity to the clinical diagnoses. As such, research in MCI will be likely to push back the threshold of recognition to an earlier state in the disease process to allow intervention at an earlier point than is currently done in typical AD clinical trials [30].
In AD, oxidative stress is one of the earliest events occurring prior to the onset of symptoms and it has been recognized as an essential contributor to the pathogenesis and progression of the disease [8, 32]. Products of free radical damage, such as aldehydes or lipid hydroperoxides, may diffuse into the blood where they can be detected. Moreover, it has been found that blood-brain barrier (BBB) permeability significantly increases in both AD and vascular dementia as compared to aging controls [33, 34]. Increased BBB permeability has been shown to trigger a chain of events leading to neuronal dysfunction and damage, as well as to specific clinical syndromes, including dementia [35]. In this context, oxidative stress has been shown to contribute to an increase in BBB permeability [36]. Consequently, oxidative stress parameters represent potential biomarkers in blood for diagnosis of AD. In addition, other diseases accompanied by free radical production, such as diabetes or cardiovascular diseases, may influence the presence of free radical products in the blood. This could explain the fact that the results of oxidative stress markers in AD, in several studies, have not been consistent using blood samples [37]. Another limitation towards the establishment of oxidative stress markers for an early AD diagnosis relies on the use of different sample types of study, such as plasma, serum, mononuclear blood leukocytes, isolated erythrocytes, or whole blood cells (containing leukocytes and erythrocytes). Thus, most of the studies have been focused on plasma and serum samples [38–46]. However, the redox status of plasma is highly influenced by diet, and most antioxidant enzymatic defense systems and compounds are intracellular. In a previous study from our group, it was demonstrated that the redox state of whole blood cells (erythrocytes and leukocytes) reflects that of isolated neutrophils, evidenced by higher GSSG/GSH ratio and MDA concentration in severe AD patients compared to mild AD patients and controls [17]. Therefore, in the present study whole blood cells were used given that this sample type is clinically more feasible, reproducible, cost effective, easy to implement and apply, compared to purified and isolated neutrophils and mononuclear blood leukocytes [17].
The results from the present study highlight the existence of an altered redox status in whole blood cells from AD patients and interestingly, some of the altered redox parameters are already affected in MCI patients. Given that the regulation of the redox balance in bloodstream is complex and in order to have a wide picture, several antioxidant and oxidant parameters were investigated in the present study. The results reveal that AD patients have higher CAT activity, GSSG and TBARS concentrations, and GSSG/GSH ratios, and lower GPx and GR activities, and GSH concentrations, compared to age-matched controls. In addition, MCI patients have a higher CAT activity and TBARS concentration, and lower GPx and GR activities than age-matched controls.
Regarding antioxidant enzyme activities, which constitute the first line of defense against generation of free radicals, we found striking differences. The significance of antioxidant changes upon conditions of oxidative stress is strongly under debate, since antioxidants might be induced by oxidative stress (and therefore their activity/levels may increase) or else consumed (thus decreasing their activity and levels) [47]. Our results demonstrate that SOD activity was similar between MCI and AD patients and control individuals, which agrees with previous reported results [48–50], although higher SOD activity was found in AD women compared to age and sex-matched controls. Other studies have also found higher SOD activity in erythrocytes from AD patients by analyzing total population, which consisted mainly of women [51, 52]. With respect to CAT activity, both MCI and AD patients show higher catalase activity, which has also been found in other studies [52, 53]. This higher enzymatic activity could probably be a compensatory mechanism to counteract the increased H2O2 that has been reported in these patients. On the contrary, GPx activity was found to be lower in MCI and AD patients compared to control subjects, as has been previously reported [50]. Both CAT and GPx catalyze the conversion of H2O2 into water. The question is why does CAT activity increase and GPx decrease in MCI and AD patients? From a kinetic point of view, GPx has a much higher affinity for H2O2 than CAT, therefore, H2O2 is principally degraded by GPx in normal conditions. However, when the H2O2 concentration increases, as in severe oxidative conditions, the CAT contribution for its degradation concomitantly increases [54]. In addition, CAT mediates conversion of H2O2 into water without requiring additional reducing equivalents and thus, no energy is required from the cell [55]. Therefore, this could be the reason why CAT activity is enhanced and GPx activity is diminished in both MCI and AD patients. Moreover, GPx also catalyzes the reduction of lipidic peroxides in addition to H2O2, thus acting on more sensitive cellular targets. McCay et al. [56] showed that GPx protects biological membranes by preventing lipid peroxidation propagation. Thus, the impaired GPx activity found in blood cells from MCI and AD patients would exacerbate the accumulation of lipid peroxidation products. In fact, in the present study, it was found that MCI and AD patients have higher TBARS concentrations in whole blood cells compared to age and sex-matched controls. Given that lipid peroxidation is a damage marker of oxidative stress, it has been proposed as one of the most promising markers in AD diagnosis [57]. Some authors suggested that lipid peroxidation in the brain might be one of the factors responsible for cognitive deterioration, and a negative correlation between MDA concentration in plasma and severity of the AD stage has been reported [37, 58]. However, we found no association between TBARS concentration in blood cells and MMSE scores, which could be due to the lack of AD patients in more advanced stages of the disease.
The glutathione cycle is one of the most important intracellular mechanisms that play a key role in the preservation of an adequate intracellular redox state [59]. In the present study, AD patients showed lower GR activities and GSH concentrations, together with higher GSSG concentrations and GSSG/GSH ratios. Nevertheless, MCI patients only showed lower GR activity compared to age-matched controls. Thus, these results suggest that this activity gets impaired in early stages of the disease whereas in more advanced stages of AD an accumulation of GSSG and an exhaustion of GSH occur. Interestingly, the parameters involved in the glutathione cycle (GR, GSH, GSSG, GSSG/GSH) were the most directly related to the degree of cognitive impairment, measured by MMSE, in accordance with other studies [60, 61].
With respect to AD prevalence, it is known that its incidence is higher in women than in men and this cannot simply be attributed to the higher longevity of women versus men, because it is also higher in young ages [62]. Thus, there must be a specific pathogenic mechanism to explain the higher incidence of AD cases in women. The results from the present study demonstrate that in the absence of pathology there are statistically significant differences in antioxidant activities due to sex, whereas in MCI and AD individuals, these differences were no longer noticeable. It has been suggested that sex-related differences could be related to the role of sexual hormones. Estrogens are known to upregulate the expression of SOD and GPx [62]. However, post-menopausal women experience a sharp fall in estrogens whereas men generally experience a more gradual age-related decline in testosterone [63]. This difference between how rapidly and significantly the female versus male primary sex hormones decline could explain in part why women are more vulnerable to oxidative stress in the elderly and why the incidence of AD is higher in women than in men.
Despite not having found sex-related differences between MCI and AD individuals, it was observed that whereas the alterations in antioxidant defense mechanisms were more significant in AD men than in AD women in comparison to their respective controls (such as higher CAT and lower GPx and GR activities and GSH concentration), the increase in oxidant compounds was more significant in AD women than in AD men (in GSSG/GSH ratios and TBARS concentrations) compared to their respective controls. Thus, these results suggest that the increased oxidative damaged products found in women, are not the result of an impaired antioxidant defense system but rather the consequence of the overproduction of reactive oxygen species, as has been previously suggested [64]. According to this, it has been reported that mitochondria from old female mice produce more reactive oxygen species in the presence of Aβ peptide than those from old male mice [62].
In addition to age and sex, the presence of the ɛ4 allele in APOE gene has been recognized as a major risk for sporadic AD [65–67]. However, its relationship with oxidative stress is controversial. A few studies have found a relationship between the ɛ4 allele APOE genotype and peripheral markers of oxidative damage, such as higher hydroxyl radical levels [68] and MDA [40] in plasma than those without this allele. However, others have found no differences [69], similar to that observed in the present study. The lack of statistically significant differences in our study could be due to the small number of patients with the ɛ4 allele in APOE.
In conclusion, the major strength of our study is that we performed analysis in blood cells from patients with MCI and AD. With this kind of sample, we have demonstrated that some redox markers were affected in AD patients (lower GPx and GR activities and GSH concentrations and higher CAT activity and TBARS concentrations) with respect to control age-matched individuals. Interestingly, some of these markers were already altered in MCI patients from both sexes (such as GPx and GR activities and TBARS concentration) and therefore, could be used for early diagnosis of AD. In addition, other redox markers such as GR activity, GSH and GSSG concentrations, and GSSG/GSH ratios were found to be associated with cognitive decline. Even though these associations were modest due to the small sample size included in the present study, our data highlight the importance and the impact of peripheral redox state and homeostatic systems during the early cognitive decline leading to dementia. However, because oxidative stress and damage occur in several diseases (including other types of dementia), another group of demented subjects, distinct from AD, should be included in future studies. Still, given the easy obtainability of the sample type used and the simplicity of the assays performed, the combination of some redox whole blood cell markers, such as GPx and GR activities and TBARS concentration could be used to define their MCI stage. However, others like GR activity, GSH and GSSG concentrations, and GSSG/GSH ratios have potential to be used in monitoring the progression of AD, once the pathology is established, in the clinical setting. Thus, we believe that the integration of several of the investigated parameters into a mathematical model could be used as a more reliable and consistent tool in the clinical setting. Nevertheless, a longitudinal design should be performed in order to elucidate the relationship between these markers and the course of the disease. Thus, although preliminary, these results could provide a benchmark for future work aimed at finding prognostic markers of AD.