
Abstract
Identifying people with amnestic mild cognitive impairment (aMCI), who are at increased risk of developing Alzheimer’s disease, is important for improving early disease management and care. Although self- or informant-reported memory problems constitute one of the diagnostic criteria of aMCI, there is currently little empirical knowledge about the frequency and nature of everyday memory failures in aMCI compared to age-matched healthy controls. Consequently, clinicians rely on their personal judgements when assessing the seriousness of reported memory failures. To address this gap in our knowledge, 32 aMCI participants and 38 healthy controls recorded their everyday memory failures as and when they occurred during a 7-day period, in a portable diary-booklet, by filling in a short questionnaire on a diary page. Descriptions of memory failures were coded into several subcategories of retrospective memory, prospective memory, and absent-minded failures. Results showed that a total number of recorded failures was significantly higher in participants with aMCI than controls. This group difference was mainly due to aMCI participants recording a higher number of retrospective memory failures, while groups did not differ in the number of prospective memory and absent-minded failures. Additionally, while certain types of failures (i.e., forgetting appointments and well-learned procedures) were recorded by a proportion of aMCI patients, they were never reported in a control group. Overall compliance rates were high and did not differ across the groups, suggesting that a structured diary method is feasible to use with aMCI patients, and can provide useful information about everyday memory functioning in this population.
INTRODUCTION
In the absence of effective pharmacological cure, research on dementia is increasingly being focused on identifying individuals at an elevated risk of developing Alzheimer’s disease. A general consensus among clinicians and researchers is that people with mild cognitive impairment (MCI), who are at prodromal stages of the disease, can benefit most from the early disease management and care [1–5]. The most prevalent form of MCI is amnestic MCI (aMCI). This is a somewhat heterogenous diagnostic entity that comprises individuals with subjective memory complaints that are corroborated by deficits in objective episodic memory tests, but the diagnosis of Alzheimer’s disease cannot be reached due to a patient’s preserved daily functioning [6, 7]. The memory deficit in objective tests may either be an isolated one (in a single domain aMCI) or accompanied by deficits in other cognitive domains (in a multiple domain aMCI). Although not all aMCI individuals will develop Alzheimer’s disease, and some may even revert to normal cognitive status [8], they have higher annual conversion rate to the Alzheimer’s disease (10–15%) than the general population (1–2%). Therefore, increasing the accuracy and predictive validity of early diagnostic procedures is of paramount importance.
Currently, there is considerable controversy in relation to a question whether the preserved daily functioning constitutes a valid criterion for the diagnosis of MCI (for a review, see [9]). A growing body of evidence shows that subtle deficits in instrumental activities of daily living (IADL) may be present in MCI [10, 11], and the results of two recent metanalysis [12, 13] demonstrate that MCI is associated with some difficulties in performing complex everyday tasks in such IADL subdomains as finances, shopping, keeping appointments, medication routines, driving, or everyday technology use. However, a more precise understanding of the nature of functional impairments in MCI, to facilitate diagnostic reliability and validity, is lacking. This has been emphasized in a number of recent reviews [14–16].
Okonkwo and colleagues [17] have suggested, for instance, that functional impairments are initially evident in the form of increased performance time and other subtle errors, rather than the more obvious inability to complete a given task. Therefore, an overall assessment of functional ability in various IADL subdomains should be supplemented by more detailed, fine-grained approaches that are designed to capture the subtleties in impairment and an evaluation of performance across multiple dimensions (e.g., time, efficiency, accuracy, number of cues required, error type). In addition, Farias and colleagues [18] have argued that to improve the understanding of daily functioning and the nature of its deterioration in older adults, different daily tasks should be analyzed with respect to the underlying cognitive abilities that they require. Some tasks may depend heavily on long-term memory, for instance, recalling items to be purchased at a store, or navigating a route to the store, while others may rely more on working memory and attentional resources (e.g., keeping track of conversations or habitual tasks such as preparing a cup of tea). Therefore, activities that are broadly construed as instrumental or higher-level functional activities should be further subdivided to reflect the relevant underlying cognitive abilities.
Memory-related functional difficulty in MCI
When analyzing functional impairments in MCI with respect to underlying cognitive abilities, memory-related everyday difficulties should be of particular importance for several reasons. First, memory decline is a defining feature of aMCI, which is the most prevalent subcategory of MCI. It is therefore important to ascertain the degree to which memory impairments observed in neuropsychological tests generalize to everyday life and manifest in functional impairments. This is particularly pertinent given the fact that individuals with aMCI seem to display greater functional difficulty compared to individuals from other subcategories of MCI [11, 19] (see also [12], for a meta-analysis).
Second, multiple memory processes are needed to support the complex activities of daily living. For example, an older individual could fail to post a letter at the post office for multiple reasons, including: 1) being unable to recall having the letter to post; 2) believing the letter was already posted while recalling a recent trip to the post office; or 3) failing to remember to stop at the post office and post the letter when going to a store in the morning. The first two failures would be related to retrospective (episodic) memory, which is the ability to remember information from the past (e.g., remembering that you have formed an intention to do something and whether the intended action has already been completed). The third failure would be related to prospective memory, which is the ability to remember to perform an action at a certain moment in the future and requires stopping an ongoing activity (going to a store) and performing the intended action (posting a letter) when encountering a cue (seeing a post office) (for a distinction between prospective and retrospective memory, see [20–23]).
Research does confirm that several separate memory abilities underlie performance in such IADL subdomains as socialization, finances, medication use, and household activities (see [9] for a review). For instance, Schmitter-Edgecombe et al. [24] reported that the source memory (the ability to link the content of recalled information with who reported it) was a significant and unique predictor of social functioning in MCI. Tan and colleagues [25] found that participants’ scores on the retrospective memory tests were related to their social engagement. In contrast, the prospective memory and temporal order memory scores were unique predictors of both medication usage and household activities in MCI [24]. Finally, memory tests were predictors of how individuals with MCI coped with a complex everyday activity (preparing for a day out) under well-controlled conditions, with retrospective memory scores uniquely predicting the number of subtasks left incomplete and inaccurate, while prospective memory scores predicting how subtasks were sequenced [26]. Naturally, memory is not the only cognitive ability that influences the performance of everyday tasks and it does not exert its influence in isolation from other cognitive processes. For example, the effectiveness of cognitive control has also been found important in IADL production in healthy older adults and those with MCI (see [27], for a review).
Thirdly, some population-based studies with long-term follow-up show that self-reported everyday memory problems predict future dementia or Alzheimer’s disease independent of objective memory test performance [28, 29]. The relationships between subjective memory scores and subsequent dementia were found to be quite strong in these studies, with a double to fourfold elevated risk of developing dementia, and even stronger for the Alzheimer’s disease in a follow-up that ranged from 5 to 17 years.
Our present knowledge about specific difficulties in the performance of complex everyday tasks that are caused by deficient memory processes in MCI is very scarce. One source of this knowledge comes from studies in which questionnaires of everyday memory functioning have been used in both MCI and healthy adult groups. These studies seem to consistently show that the MCI groups experience a higher frequency of everyday forgetting compared to the healthy adult groups, with everyday forgetting measured with both self-report [30, 31] and informant-report [18, 31]. Self-assessment of forgetting usually involves participants evaluating the frequency of everyday memory failures that they experience in various everyday memory tasks (i.e., forgetting names, words, directions, thread of thought in conversations, what they are currently doing, etc.).
While the questionnaire studies seem to support the difference between healthy older adults and individuals with MCI in the overall frequency of everyday forgetting, knowledge about which specific types of memory failures may help discriminate individuals with MCI from healthy older adults is lacking. Indeed, in most memory questionnaires, different everyday memory failures that rely on distinct memory abilities (e.g., retrospective and prospective memory), often constitute one dimension or a subscale of the questionnaire (e.g., Memory Functioning Questionnaire [32]; Multifactorial Memory Questionnaire [33]; Cognitive Failures Questionnaire [34]; Everyday Memory Questionnaire [35]; Everyday Cognition [18]; but see Prospective and Retrospective Memory Questionnaire [22], for an exception). As a result, it would be difficult for questionnaire studies to fill this gap.
Another source of knowledge comes from a few studies in which the performance of memory-based tasks was compared in healthy older adults and individuals with MCI in the context of their everyday lives. However, these studies were limited mostly to prospective memory and their results are inconsistent, with the MCI groups performing either as well [36, 37] or worse [38, 39] than the healthy older adults. For example, Thompson et al. [36] asked participants to remember to turn on a handheld electronic organizer once per day for two days at a predetermined time and tap a response box that automatically appeared on the screen. Their aMCI group did not show deficits on this naturalistic task compared to healthy controls. In contrast, Delprado et al. [38] found impairments in aMCI participants on two naturalistic prospective memory tasks which involved 1) calling the research office at four specified times across two weeks and leaving a message, and 2) generating one’s own prospective memory tasks for the week and, at the end of the week, indicating whether each task had been successfully completed. This inconsistency in results is surprising given that prospective memory deficits in MCI have been well documented on laboratory-based measures (see [40], for a meta-analysis).
The present study
The aim of the present research was to fill in the existing gap in our knowledge about difficulties in the performance of everyday tasks that are caused by deficient memory processes in aMCI by asking healthy older adults and individuals with aMCI to keep a structured diary of everyday memory failures for 7 days. Every time participants forgot something or made an error, they had to provide a brief description of their memory failure and complete a short questionnaire on a diary page.
To the best of our knowledge, this is the first diary study of everyday memory failures in MCI. The study was conducted to enhance the understanding of the nature of functional impairments in aMCI, which could help the clinicians to improve the diagnosis of aMCI, by investigating memory-related everyday problems that can help discriminate memory complaints made by healthy older adults from those made by individuals with aMCI.
In addition, the present study addressed the need for finer-grained analyses of everyday difficulties in MCI with respect to relevant underlying cognitive abilities. To this aim, we used a modified version of the coding system, originally used by Kvavilashvili et al. [41], to classify the descriptions of memory failures into subdomains of the three main categories of lapses reflecting distinct memory functions. Specifically, recorded failures were classed into several subdomains of retrospective, prospective and absent-minded lapses. While retrospective and prospective memory lapses reflect problems with long-term memory for the past events and to-be-performed future actions, respectively, absent-minded lapses involve forgetting information that is necessary for ongoing processing of intended or habitual actions and are more reflective of problems with working memory and attention resources (see [21, 42], for the same distinction). We also compared the three categories of lapses in terms of the circumstances in which they occurred as well as how upsetting and serious for their everyday functioning the participants found them to be. It was interesting to see if participants with aMCI rated their memory failures as more serious or upsetting than the healthy control group.
So far, diary methods have been successfully used to capture everyday memory failures in young adults [43–45] and healthy older adults [46–48]. The validity of the diary method as a measure of everyday memory failures has been confirmed by showing that the number of memory lapses was significantly and negatively related to a level of memory abilities, as assessed by laboratory-based memory measures [45, 47]. A recent longitudinal diary study [47] used a version of the daily diary in which healthy older adults were instructed to indicate at the end of each day, which of the sixteen everyday memory failures had occurred during the day (the list of failures was taken from Memory Functioning Questionnaire [32]). Forgetting names and words was the most commonly reported lapse at baseline, which is consistent with the results of the laboratory-based studies on aging and word-finding [49], and older adults reported an increase in the frequency of these lapses at a 5-year follow up. Importantly, it was the daily diary, but not the Memory Functioning Questionnaire, that was sensitive to changes in the frequency of memory failures with increasing age and significantly related to the participants’ scores in a neuropsychological memory test.
However, one may question whether a diary of everyday memory failures can also be used successfully in individuals with aMCI. There are several reasons for supporting the idea that individuals with aMCI will be able to accurately record their everyday memory difficulties in a diary. First, as mentioned above, self-reports of individuals with aMCI on the questionnaires of everyday memory functioning do show a higher level of everyday forgetting compared to healthy older adults, which suggests that individuals with aMCI have an insight into their everyday memory-related difficulties [18, 31]. Findings are less clear from research in which differences between the self-reporting of cognitive and functional abilities and informant reporting have been compared in the MCI and healthy older adult participants [50–53]. These studies have produced conflicting results in terms of the accuracy of self-reports relative to reports of informants. Some studies showed bigger differences between self-reports and informant-reports in the MCI group, compared to the healthy adult group, with a tendency to underestimate deficits by the MCI group [51]. In contrast, other studies showed that the difference scores for the MCI groups were not significantly different from those of the control groups [53]. This inconsistency can be explained by the results of some studies which suggest that the tendency to underestimate deficits can jeopardize the validity of self-reports only in those participants who represent the more severe end of aMCI diagnosis, by having a score of 0.5 on the Clinical Dementia Rating Scale [50, 52]. Therefore, in the present study, we used the Petersen’s diagnostic criteria for aMCI that are different from the Clinical Dementia Rating Scale [6, 7] (see the Method section for details) and appear to screen for the less severe end of aMCIdiagnosis [54].
A second reason is that a diary method can be, on the whole, a better choice for analyzing everyday difficulties in MCI, compared to questionnaire-based assessment. Questionnaires use large time frames and therefore place high demands on participants’ ability to recall memory failures. In contrast, the diary method minimizes the amount of time elapsed between an experience and the account of this experience by allowing participants to record their memory failures as and when they occur. Therefore, it greatly reduces demands placed on participants’ memory and eliminates the biases introduced by retrospection, such as faulty reconstruction, state-congruent recall, giving more weight to the peak levels, and to the most recent levels of experience, etc. (see [55] for a more detailed discussion). Furthermore, some recent studies show that when online methods are used to measure metacognition (predictions about the performance on the memory task), the insight of individuals with MCI into their memory functioning is as good as that of healthy older adults [56].
Finally, it can be argued that the task of keeping a diary is itself a prospective memory task, i.e., participants need to remember to keep the diary with them all the time and record each lapse they experience. This could be more challenging for individuals with aMCI and could jeopardize the validity of the results due to under-reporting. To address this issue and minimize demands placed on participants’ memory to keep a diary, we contacted each participant twice a day during the entire period of keeping a diary to remind them about their task. In addition, we used a post-diary interview and a post-diary questionnaire to control for possible group differences in the difficulty of keeping a diary and compliance with the task instructions.
In sum, we compared everyday memory failures recorded in the diaries by healthy older adults and individuals with aMCI that were coded as prospective, retrospective, or absent-minded lapses. Based on the results of the questionnaire studies on everyday memory functioning [18, 31], we expected the aMCI group to experience overall more failures than the control group. Retrospective (episodic) memory deficit, as measured by neuropsychological tests, is a defining feature of aMCI [6, 7], and therefore we expected individuals with aMCI to have more retrospective memory lapses compared to healthy older adults. Although the previous findings on prospective memory deficits in aMCI are not clear, with substantial deficits on laboratory-based tasks [40] and conflicting results when tasks are performed in the context of everyday life [36–39], we still expected the aMCI group to have more prospective memory lapses than healthy older adults. We did not expect group differences in the number of absent-minded lapses, because they are one of the most commonly reported memory failures both in young [23] and in healthy older adults [57], which suggests that their very frequent occurrence may be a normal part of everyday functioning and healthy aging.
METHODS
Design
The design was a 2×2 mixed-factor design, with Group (aMCI versus healthy controls) as a between-subjects factor and Memory lapse (retrospective versus prospective versus absent-minded) as a within-subjects factor.
Participants
A total of 43 healthy older adults and 39 aMCI participants were recruited. The study was approved by the National Research Ethics Service Committee-Cambridgeshire and Hertfordshire. For all participants, exclusion criteria included: (a) head/brain injuries, (b) history of cerebrovascular disease, (c) history of alcohol or substance dependence, (d) medical, neurological, or psychiatric disorders resulting in cognitive dysfunctions, (e) age less than 60 years. Fluency in English and adequate vision and hearing were also required. Exclusion criteria were assessed in the initial phone screening. Individuals who passed the screening were invited to take part in two sessions, during which participants were asked to keep a 1-week diary of daily memory lapses and completed a battery of standardized neuropsychological tests. All participants were retired.
MCI participants
The MCI participants were referred from Specialist Mental Health Teams for Older People and Early Memory Diagnosis and Support Services (memory clinics). They all had MCI diagnosis via multidisciplinary diagnostic consensus (i.e., neurological, psychiatric, radiological, neuropsychological, and functional assessment). The majority (87%) were diagnosed within the preceding couple of weeks of the start of the study and the remaining 13% were diagnosed not longer than two months before the study. The clinical diagnosis was confirmed using the inclusion criteria that satisfied the diagnostic criteria of aMCI [6, 7]: (a) the presence of a subjective memory complaint (i.e., the patient sought professional assessment due to concerns about memory decline); (b) objective memory impairment evidenced by a score at or below 1.5 SD of the mean of age-matched peers on at least one test of the neuropsychological screening battery that assessed episodic memory (see the Neuropsychological evaluation section); (c) not meeting the Diagnostic and Statistical Manual of Mental Disorders’ (DSM-5) criteria for dementia [58], (d) preserved general cognitive function as confirmed by a normal score on the Mini-Mental State Examination (MMSE; [59]) (normality cut-off score: 24; [60]); (e) maintained activities of daily living, or the slight impairment in the instrumental activities of daily living, as measured by the Lawton Instrumental Activities of Daily Living scale (the Lawton IADL; [61]), which should not show a deterioration in more than one task/domain of daily living; (f) absence of severe depression, as confirmed by a score below 20 on the Geriatric Depression Scale 30 (GDS30; [62]). The Lawton IADL is commonly used in the diagnosis of MCI and assesses a person’s ability to use a telephone, do laundry, shopping, prepare food, maintain house, handle finances, take medication, and use transport.
Two aMCI participants withdrew after the first session, during which diary booklets for recording memory lapses were distributed, and one aMCI participant lost his booklet after the first session. Another aMCI participant did not return the diary, because he had found keeping a diary to be too much burden for him. Finally, three aMCI participants did not keep a diary as requested; although they understood the instructions for the diary at the time the booklet was given to them, they did not know how to fill it in later on. The final sample consisted of 32 aMCI participants.
Four aMCI participants from the final sample, in addition to their episodic memory deficits, scored 1.5 standard deviations or more below age-appropriate means on at least one of the tests of short-term memory, attention and executive functions, and therefore satisfied the criteria of multiple domain aMCI [6, 7].
Healthy controls (HC)
HC were recruited through advertisements in the local community and lunch and social clubs for older adults as well as a database of the older adult volunteers maintained by the second author. Inclusion criteria for the HC group were: (a) absence of a subjective memory complaint (i.e., had not sought professional assessment due to concerns about memory performance); (b) a score within or above 1.5 SD of the mean of age-matched peers on each test of the neuropsychological screening battery assessing episodic memory; (c) a score ≥27 on the MMSE; (d) no impairment in the instrumental activities of daily living, as indicated by a maximum score on the Lawton IADL; (e) absence of severe depression, as confirmed by a score of below 20 on the GDS30.
Two HC withdrew after the first session, in which booklets for recording memory lapses were distributed, and another HC lost his booklet after the first session. Two HC provided diary data that could not be used; handwriting of one participant was unreadable and the other participant filled in the booklet as a classic diary, i.e., on each page he described what he was doing that day. The final sample consisted of 38 HC.
Table 1 shows demographic details of the final sample. A series of independent samples t-tests and a chi-square test (for gender) revealed no significant differences between aMCI and HC on the demographic variables (p
s
> 0.10), except for two tests. The MMSE scores were significantly higher in HC than in aMCI individuals (p < 0.001; d = 1.25). However, all aMCI participants scored at or above the cut off score of 24 (range 24–30). The Lawton IADL scores were also significantly higher in HC than in aMCI individuals (Zadjusted = 3.01, p < 0.01). However, all aMCI participants scored at least 7 on the 8-point Lawton IADL scale. The mean scores on the Geriatric Depression Scale 30 were entered into a 2 (group: aMCI, HC)×2 (Session: 1 versus 2) mixed ANOVA with repeated measures on the last factor. Participants had better mood in Session 2, after keeping a diary of memory lapses for one week, compared to Session 1, when they were given a diary to keep, F(1, 68) = 10.58, p < 0.01,
Demographic characteristics as a function of group (aMCI participants versus healthy controls)
aMCI, amnestic mild cognitive impairment; NART, National Adult Reading Test; Mood, Geriatric Depression Scale 30; MMSE, Mini-Mental State Examination; Lawton IADL, the Lawton Instrumental Activities of Daily Living scale; Health at present (1 = poor, 5 = excellent); Health compared to peers (1 = significantly worse, 3 = same, 5 = significantly better).
Measures
Neuropsychological evaluation
Standardized tests were administered to all participants to assess episodic memory, short-term memory as well as attention and executive functions. The episodic memory tests included the Hopkins Verbal Learning Test–Revised (HVLT-R; [63]), consisting of three Immediate Recall and one Delayed Recall tests, and several tests from the Wechsler Memory Scale–3rd edition [64]: Logical Memory Subtest (Immediate Recall and Delayed Recall); Verbal Paired Associates (Immediate Recall and Delayed Recall); two tests of short-term memory (Digit Span Forward and Digit Span Backward). The attention and executive function tests included Verbal Fluency Test: Letter Fluency [65], and Category Fluency [66], and the Trail Making Test (TMT): Part A and B [67].
A series of independent samples t-tests (aMCI versus HC) were conducted on the mean scores of all the tests from the battery. Significant group differences were obtained for all the tests, except for the Digit Span Forward and the Verbal Fluency: Letters, with HC group outperforming the aMCI group (see Table 2). Given that there were 28 participants with a single domain aMCI (episodic memory deficits only) and only 4 participants with a multiple domain aMCI (episodic memory deficits as well as deficits in other cognitive functions), the effect sizes for episodic memory tests were markedly higher than for the tests measuring short-term memory, attention and executive functions.
Mean scores on neuropsychological test battery in participants with aMCI and healthy controls and effect sizes in Cohen’s d for results of series of t-tests on these scores
aMCI, amnestic mild cognitive impairment; HC, healthy controls; HVLT, Hopkins Verbal Learning Test; WMS, Wechsler Memory Test. For each test, a high score indicates a better performance with the exception of scores referring to time used to complete the Trail Making Test (A and B). Differences between aMCI and HC are indicated by *p < 0.05, **p < 0.01, ***p < 0.001.
Paper diary
The diary study was designed in accordance with the guidelines for paper and pencil diaries [55, 68], i.e., the diary had been piloted on an aging population, each entry took no more than 2–3 minutes to complete, a diary booklet was portable, and participants were thoroughly trained about how to keep a diary. Two recommended compliance-enhancing procedures were also introduced, i.e., we maintained ongoing contact with participants during the diary keeping period and the diary instructions required participants to write down not only the time when they had a memory failure, but also the time when they recorded it.
More specifically, participants received an A5 paper diary booklet, containing 32 identical pages, one page to be completed for each everyday memory failure experienced. In addition to describing each failure and reporting when it happened and when it was recorded, participants had to answer several questions about circumstances in which the failure occurred. The following items were presented on each diary page: 1. When did you have a memory error? Or when did you realize you made an error? (Date and time); 2. When did you record it here? (Date and time); 3. Describe your memory error (free text entry); 4. What was your mood immediately before the error (a 5-point scale: 1 = very unhappy to 5 = very happy, plus don’t know); 5. How relaxed or stressed were you immediately before the error (a 5-point scale: 1 = very relaxed to 5 = very stressed, plus don’t know); 6. How serious was the memory lapse (1 = insignificant, 2 = minor, 3 = somewhat significant, 4 = significant, 5 = very significant/potentially dangerous); 7. Were there or could there have been any consequences? (free text); 8. How upset are you by the memory lapse? (1 = not at all upset, 2 = a little, 3 = somewhat, 4 = quite; 5 = very upset); 9. Describe the emotions you felt in response to your lapse, if any (free text); 10. If you later recovered from this error, describe when and how (free text). This question allowed participants to describe when and how they remembered what they had previously forgotten.
Diary Compliance Questionnaire
A diary compliance and feedback questionnaire were completed after the diary-keeping phase. Participants had to indicate whether they carried the diary with them every day of the study (yes/no). If the ‘no’ option was chosen, they indicated how many days they did not. They had to rate how easy they found keeping the diary with them at all times (very easy, somewhat easy, somewhat difficult, very difficult). Participants also had to estimate what percentage, out of all the memory failures they had experienced in the 7-day period, they were able to record fully and in the form of acknowledged/‘ticked’ lapses (see the Procedure subsection). They had to indicate whether they found the process of recording memory failures useful in any way (yes/no). If the ‘yes’ option was chosen, they were asked to describe in what way it was useful. Finally, they indicated whether they thought that recording memory failures had any effect on the number of failures experienced on a 7 point-scale (1 = significantly reduced the number of failures, 4 = had no effect, 7 = significantly increased the number of failures).
Procedure
Participants were tested individually by the first author, predominantly at the participant’s home. Two sessions were conducted a week apart. At the beginning of Session 1, participants completed the consent form, demographic items and health ratings. An experimental task was then conducted which was part of another study [69]. The participants were then trained for about 25 minutes on how to keep a diary of everyday memory failures. It was stressed that people of all ages complain that they forget things they know they should remember and that these memory failures take different forms, which was followed by examples of retrospective, prospective, and absent-minded lapses. The three categories as such, were not explicitly mentioned or defined. Three examples of lapses from each category were provided, and the order of category presentation was counterbalanced across participants. To ensure that participants understood the idea of everyday memory failures, they were asked to give examples of memory lapses they had recently experienced.
Participants were then asked to record any everyday memory failures that occurred over the next seven days, starting from waking the day after the briefing (Day 2), so that only full days were recorded. Participants were urged to keep the diary with them at all times and to record memory failures immediately, or as soon as possible after their occurrence. However, participants were also informed that it would not always be possible, or appropriate, to record failures, because of activities such as driving or during meetings. If that was the case, and to minimize making retrospective entries, they were advised that if they could not complete the diary page immediately and later felt that they could not recall key characteristics, they could record them as a tick (on a grid, with rows for the appropriate day, on the inside front cover of the paper diary). They were also urged to record each failure they would experience, no matter how trivial or unimportant it may seem to them. Each item on the diary page was then explained. The experimenter discussed possible answers to each question with the participant, using the examples of everyday memory failures that had been provided by the participant.
In addition to the verbal training, participants were given written instructions on how to complete their paper diary. Written instructions were provided on the last page of the paper booklet so that participants could consult them any time when keeping a diary. Finally, participants completed the Geriatric Depression Scale 30.
During the week when participants were keeping the diary, we contacted each participant twice a day through a text message or a phone call, whatever the participant preferred, to remind them to record everyday memory failures. At the beginning of Session 2, the experimenter took the diary booklet and discussed the experience of keeping a diary with the participant. The participant was also asked to fill in the Diary Compliance Questionnaire. The neuropsychological test battery and the Geriatric Depression Scale 30 were then completed. Each session lasted about two hours.
Coding participants’ descriptions of memory failures
The analyses of diary entries in terms of the types of memory failures were based on a coding system developed by [41] and used in subsequent diary studies in healthy young and older adults [70]. In Kvavilashvili et al. [41], young and older participants were asked to describe their most recent memory failure. The descriptions of memory failures were subjected to thematic content analysis, using a bottom up approach without any pre-existing classification scheme, except the expectation that the failures would broadly fall into retrospective and prospective memory domains. However, researchers were surprised to find that participants also often nominated absent-minded slips and errors as memory failures, and consequently all descriptions were classed into retrospective, prospective and absent-minded categories. This classification system is also in line with a current theoretical approach to memory functioning that delineates several distinct memory systems [71], and specifically distinguishes working memory [72] from long-term (retrospective) memory, on the one hand, and prospective memory from retrospective memory, on the other [20].
In the coding system, retrospective memory lapses refer to forgetting information from the past and include forgetting: words, names, items from shopping lists, facts, locations as well as forgetting that actions have already been completed. Prospective memory lapses refer to forgetting to perform an intended activity at a particular point in the future and include both forgetting to do things a few minutes later and in the longer term. Absent-minded lapses refer to forgetting information that is necessary for ongoing processing and action regulation that should be maintained in working memory. They include temporary loss of the content of intention (Why am I here?; forgetting to say something), action swap (doing one thing instead of another), not finishing a started sequence, omissions (missing a step in a sequence), commission errors (doing the same action again), misplacing things, losing track of sequence (of sub-tasks or operations), and disorientation (regarding the day, date or time). Using the coding system, all diary entries were coded by the first and second authors (independently and being blind to participant group) into the three categories of failures. Inter-rater reliability between the coders was almost perfect, Cohen’s weighted κ= 0.91, SE = 0.02 [73], and disagreements were resolved by discussion. Out of 517 diary entries that were provided by the participants, only two were found, by both coders, too vague for coding and were excluded from the further analyses.
RESULTS
Both parametric and non-parametric methods of analysis were used depending on the type of the dependent variable used. The effect size, as measured by partial eta-squared (
Measures of compliance and usefulness of diary keeping in aMCI and healthy controls
The two groups did not differ reliably in terms of how many participants kept the diary with them every day for the entire 7-day period (91% in the aMCI group and 95% in the control group), χ2 (1, N = 71) = 0.48, p = 0.49. In addition, t-tests for independent samples did not reveal group differences in the number of days during which participants kept the diary with them (see Table 3); a minimum number of days during which participants kept a diary was 5 for both aMCI participants and healthy older adults. However, individuals with aMCI found keeping a diary with them more difficult and felt they reported the smaller percentage of total number of failures experienced, compared to healthy older adults (see Table 3).
Mean (standard deviation) days of keeping a diary, percentage of lapses recorded, difficulty of keeping a diary and effect of keeping a diary on the number of lapses in participants with aMCI and healthy controls, and results of independent samples t-test
aMCI, amnestic mild cognitive impairment; HC, healthy controls; Difficulty of keeping a diary (1 = very easy, 2 = somewhat easy, 3 = somewhat difficult, 4 = very difficult); Effect of keeping a diary on the number of lapses (1 = significantly reduced the number, 4 = had no effect, 7 = significantly increased the number).
In addition, t-tests for independent samples did not reveal group differences in the effect that the process of recording failures had on the number of failures experienced, i.e., whether participants thought it significantly reduced or increased the number of lapses (see Table 3). All but one participant claimed that keeping a diary either reduced the number of failures experienced (ratings of 1–3 on the scale) or did not have any effect on the number of failures (rating of 4 on the scale). For both groups, one-sample t-tests revealed that the mean ratings of the effect of keeping the diary on the number of failures experienced were significantly lower from a rating of 4 (indicating ‘no effect’): the aMCI group t(31) = –2.98, p < 0.01, d = 0.53, the control group t(37) = –3.70, p < 0.001, d = 0.60.
Finally, the two groups did not differ reliably in terms how many participants found the process of recording memory lapses useful to them (59% in the aMCI group and 58% in the control group), χ2 (1, N = 71) = 0.20, p = 0.90. The reasons that participants provided for the diaries to be useful to them were similar in both groups and could be classed into four distinct categories. The first two categories referred to becoming more realistic and accurate about memory functioning (it helped me not to dismiss my memory failures; makes you aware of the extent of the problem) as well as making participants aware that their memory failures were not as serious as they had thought previously (made me aware that my memory failures were not quite as bad as I thought; it was comforting that all were insignificant and caused me no great concern). The third category referred to diary providing participants useful insights into what their failures were like (I noticed they were sometimes in “batches”; made me realize where my weaknesses are). Finally, participants reported that keeping a diary made them more focused and attentive to their memory functioning, which resulted in them having fewer memory lapses (it made me more aware, so I did not have many lapses; helped me to remember slightly more). All examples in brackets are the reasons provided by individuals with aMCI.
Types of memory failures in aMCI and HC
The mean number of failures recorded was 9.44 in the aMCI group (SD = 6.84; range: 0–19) and 5.61 in the HC group (SD = 3.81; range 3–32). In the aMCI group, the coding resulted in 161 diary entries with retrospective memory lapses (54%), 72 prospective memory lapses (24%), and 64 absent-minded lapses (22%). In the HC group, there were 94 entries classed as retrospective memory lapses (43%), 59 prospective memory lapses (27%), and 65 absent-minded lapses (30%).
To assess the hypothesis that aMCI participants would report significantly more memory failures than HC, particularly in the retrospective and prospective category, the number of everyday memory failures in each category were entered into a 2 (group: aMCI, HC)×3 (type of lapse: retrospective, prospective, absent-minded) mixed ANOVA with repeated measures on the second factor. Overall, aMCI participants reported memory lapses more often than HC, F(1, 68) = 8.73, p < 0.01,
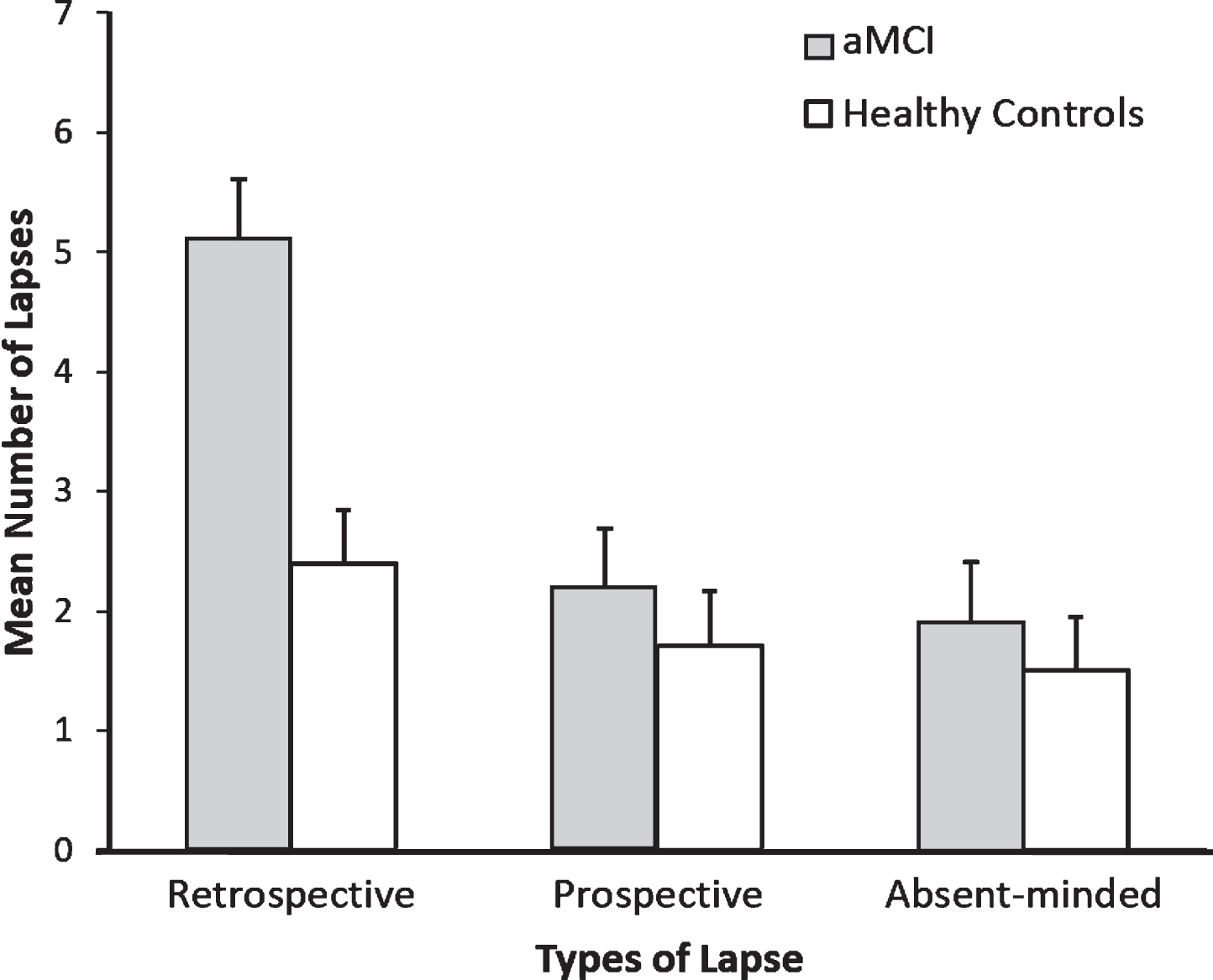
Mean Number of Memory Lapses as a Function of Type of Lapse (Retrospective Memory versus Prospective Memory versus Absent-minded) and Group (aMCI participants versus Healthy Controls). Error Bars Represent 1SE of the Mean.
An additional set of tests showed that the main effect of type of lapse was significant in aMCI participants, F(2,67) = 12.12, p < 0.0001, η 2 p = 0.27, but not the HC group, F < 1. Post hoc tests revealed that, for the aMCI group, the number of retrospective memory lapses was significantly higher than the prospective memory lapses and absent-minded lapses (ps < 0.0001), which did not differ from each other (p = 0.997).
The results of the above analyses were the same when four participants with multidomain aMCI were excluded from the analyses. Numerically, each participant with multidomain aMCI had more retrospective memory lapses than other types of lapses taken together.
Most participants recorded their failures in full, and the number of ticks to acknowledge that they had had a failure, but could not describe it in the diary, was very low in both groups. Unequal variance t-test did not reveal significant group differences in the number of ticks that the participants did make (M aMCI = 0.47, SD aMCI = 2.30; M HC = 0.47, SD HC = 1.23) (p = 0.991). When we included ticks in the number of failures recorded, the pattern of results was the same as when only the number of fully described failures was taken into account, i.e., aMCI participants reported memory lapses more often (M = 9.91, SD = 8.39) than HC (M = 6.08, SD = 5.11), t(68) = 2.48, p < 0.05, d = 0.55.
As an additional analysis, we examined a relationship between participants’ scores on the episodic memory tests and the number of recorded prospective, retrospective and absent-minded failures. No significant correlations were obtained for the aMCI group. However, six measures of episodic memory (out of eight measures used in the study, see the Neuropsychological evaluation section) positively corelated with the number of prospective memory lapses in the healthy adult group (Pearson’s coefficients ranged from 0.22–0.49), indicating that those who had higher scores on episodic (retrospective) memory tests recorded more prospective memory failures in the diary. This finding was unexpected, however, and due to relatively small sample sizes, it should be taken with caution.
Seriousness and distress ratings for memory failures in aMCI and HC
We performed a series of ANOVAs on mean ratings of mood before the failure, stress before the failure, how serious the failure was and how upset the participant was by the failure in each category of lapses (see Table 4). The mean ratings were entered into a 2 (group: aMCI, HC)×3 (type of lapse: retrospective, prospective, absent-minded) mixed ANOVAs with repeated measures on the second factor. Only the main effect of the type of lapse on seriousness ratings was statistically significant, F(1.974, 63.165) = 3.26, p < 0.05,
Mean (standard deviation) mood before the failure, stress before the failure, how serious the failure was, and how upset the participant was by the failure in participants with aMCI and healthy controls
aMCI, amnestic mild cognitive impairment; HC, healthy controls; All ratings were made on 5-point scales. *These analyses were conducted on much smaller sample because many participants did not have lapses that belonged to all three types of lapses so they were excluded from the analyses.
For the vast majority of memory failures (81%), participants did not report any consequences. When consequences of memory failures were reported, they were not dramatic or dangerous, but were nevertheless, unpleasant and disturbing as they could involve 1) delays, 2) wasting time or money, 3) re-organizing the schedule, 4) additional work or journeys, and 5) socially embarrassing situations (e.g., calling someone by the wrong name or forgetting to do something important). The number of lapses for which consequences were reported was calculated for each type of memory lapse separately. These numbers entered into a 2 (group: aMCI, HC)×3 (type of lapse: retrospective, prospective, absent-minded) mixed ANOVA with repeated measures on the second factor, but no statistically significant effects were obtained (p s > 0.10).
Subcategories of failures within each broad category
To perform more fine-grained comparisons of types of memory failures experienced by individuals with aMCI and healthy older adults, we delineated several subcategories of lapses within each broad category of retrospective, prospective and absent-minded lapses. This coding scheme was primarily based on the memory failure coding system developed by Kvavilashvili et al. [41], and the subcategories of failures in each broad category that their system provided (see section on ‘Coding participants’ descriptions of memory failures’). However, the content analysis of lapses provided by the participants in our study enabled us to delineate more subcategories within each broad category than the original coding system provided. Using this new coding scheme, diary entries that belonged to one broad category of lapses (retrospective, prospective or absent-minded) were coded by the first and second authors (independently and being blind to participant group) into several subcategories of lapses within this category. Inter-rater reliability between the coders was almost perfect for all three broad categories: retrospective memory lapses: Cohen’s weighted κ= 0.92, SE = 0.02; prospective memory lapses: κ= 0.94, SE = 0.02; absent-minded lapses: κ= 0.95, SE = 0.02 [71]. All the subcategories that were delineated, with the number of lapses from each subcategory reported by individuals with aMCI and healthy older adults, are presented in Table 5.
Number of lapses in each specific subcategory of retrospective, prospective and absent-minded lapses in participants with aMCI and healthy controls
aMCI, amnestic mild cognitive impairment; HC, healthy controls. *indicates significant group difference at p < 0.05; the examples of lapses are provided in the Results section.
Due to a large number of subcategories and the fact that many participants did not have any lapses reported in a particular subcategory, the assumptions of normality were violated for the numbers of lapses within subcategories. Therefore, we used non-parametric Mann-Whitney tests to compare aMCI and HC in terms of the number of lapses in each subcategory. The tests revealed significant group differences in four subcategories: forgetting well-learned procedures (U = 494.00, p < 0.01), forgetting to keep appointments (U = 513.00, p < 0.05), forgetting to carry out regular duties at home (U = 488.50, p < 0.05) and omitting one action in the sequence (U = 512.00, p < 0.05).
Six participants from the aMCI group (19%) reported forgetting well-learned procedures (one of them twice), compared to no participants (0%) in the HC group. Individuals with aMCI reported failures such as: (i) Not having a good day, finding everything difficult. I have cooked Sunday lunch since 1952 but keep stopping to keep checking on everything. Frustrating; (ii) Forgot which card I needed at the station check point. The assistant took the right ticket; (iii) Put 2 pizzas in the oven thinking it was already heated but discovered I had switched on the top oven not the main one. I had forgotten which switch to use even though I have been using it for two years; (iv) Visited daughter at Letchworth could not find the road back when driving.
Five participants from the aMCI group (16%) reported forgetting about appointments (one of them twice), compared to no participants (0%) in HC. The examples of failures from the MCI group were: (i) Forgot about appointment with a dentist; (ii) Arranged to go out in the afternoon with a friend. Forgot all although it did not cause any problems this time; (iii) Forgot I am due to babysit the 2 boys from 4pm until 10 pm. Until my husband reminded me about dinner for tonight.
Eight participants from the aMCI group (25%) reported forgetting to carry out regular duties at home (four of them more than once), compared to 4 (10%) in the HC group (one of them more than once). Participants reported failures such as: (i) Forgot of dustbin to get out; (ii) Forgot to make bread; (iii) Forgot to turn the central heating off before leaving the house for the day; (iv) Cutting the grass and forgot to prepare lunch.
In contrast to the pattern of differences presented above, an absent-minded failure of omitting one action in the sequence was reported more often in the HC group. Six healthy older adults (16%) experienced such failures (three of them twice), compared to no participants (0%) in the aMCI group. The examples of failures from the HC group were: (i) Removed milk from the fridge to put in husbands tea, put it back in the fridge without pouring it in his tea, (ii) Got tea bags out intending to refill storage jar, put them back in the cupboard without realizing I hadn’t refilled the jar, (iii) Set up laptop to watch DVD. Sat down to watch and realized no DVD.
DISCUSSION
There is growing evidence to show that aMCI is associated with subtle deficits in performing complex everyday tasks [12, 13]. However, it is not clear which specific types of everyday difficulties are particularly pronounced in people with aMCI, as compared with healthy older adults, and how they relate to distinct cognitive abilities that underlie the performance on daily tasks. Therefore, we compared, for the first time, participants with aMCI and a matched group of normally aging healthy adults on various types of difficulties that were related to distinct memory abilities. To capture those memory-related problems, we used a diary of everyday memory failures, which is a novel methodology to study functional impairments in aMCI.
Several important findings emerged from this comparison. First, in line with our predictions and the results of previous questionnaire studies, which assessed the overall frequency of memory failures in healthy and cognitively impaired older adults [18, 31], the aMCI group recorded overall more memory failures compared to the healthy adult group. Second, and again in line with our predictions, individuals with aMCI had substantially more retrospective memory lapses than the control group. This is a novel finding which shows that retrospective memory impairments, observed in neuropsychological tests, generalize to everyday life and manifest in more frequent difficulties in performing daily tasks that are caused by deficient retrospective memory. These difficulties are not restricted to failures of recalling names and words, but include, for instance, such frequent lapses as not remembering what participants were told or where they hid something at home (see Table 5).
However, contrary to predictions, we did not find any group differences in the number of prospective memory lapses. This seems to suggest that prospective memory deficits found on laboratory-based tasks [40] may not generalize to everyday life and is consistent with two previous studies, which also did not find these deficits in the context of everyday life [36, 37]. Finally, in accordance with our expectations, the MCI group reported experiencing absent-minded lapses with the same frequency as the control group. It is worth noting that retrospective memory lapses were not only more frequent in aMCI, compared to controls, but they were also a prevalent form of memory failures reported by individuals with aMCI, which was not the case in the healthy older adult group who recorded equal numbers of retrospective, prospective and absent-minded lapses.
A possible explanation of an unexpected lack of group differences in the number of prospective memory lapses is that in everyday life, compensatory strategies (e.g., writing lists, keeping a daily planner, using calendars), when used successfully, can minimize prospective memory deficits. Indeed, both laboratory and naturalistic studies show that the use of compensatory strategies enhance prospective memory performance [75, 76]. However, there seems to be something unique about how individuals with aMCI use compensatory strategies in their day-to-day life. When the first author was conducting sessions at participants’ homes, she noticed that spouses of individuals with aMCI helped them greatly to cope with everyday prospective memory tasks by taking over many of the aMCI participants’ duties and constantly reminding them about delayed intentions that they still needed to remember. This informal observation was in line with the research data showing that other people are vitally important in how individuals with MCI cope with prospective memory tasks in everyday life. For example, Delprado et al. [38] compared participants with aMCI to healthy older adults on the use of strategies to help to remember about intentions in day-to-day life and found strategy use a distinguishing feature between the two groups, with healthy older adults using more written strategies, whereas individuals with aMCI relied more on another person providing a reminder. Furthermore, Thomas and Marsiske [19] found that individuals with MCI experienced greater improvement, compared to healthy older adults, due to verbal prompting when theywere performing naturalistic tasks in well-controlled conditions.
To investigate whether having an opportunity to rely on another person contributes to minimizing prospective memory deficits in the everyday life of individuals with aMCI, future studies should compare prospective memory failures in individuals who live with someone and those who live on their own, in both aMCI and healthy adult groups. As only a small number of the participants in our sample lived on their own (9 healthy controls and 12 individuals with aMCI), we were not able to conduct such comparisons. However, the average number of prospective memory failures experienced by the aMCI participants who lived with their spouses was numerically much lower (1.80), compared to the aMCI participants who lived on their own (2.83), and this difference was numerically smaller in the healthy adult group (1.57 and 2.33).
It is worth noting that when prospective memory lapses did occur, both individuals with aMCI and healthy older adults considered them more serious, compared to retrospective memory lapses. This is understandable, given that prospective memory failures particularly undermine older peoples’ ability to lead safe and independent life, and makes it unlikely that participants overlooked prospective memory lapses when keeping their diaries. However, an unexpected positive relationship between the performance on the episodic memory tests and the number of prospective memory lapses in the healthy adult group may suggest that the episodic memory deficit may somewhat reduce the ability of aMCI individuals to report forgotten intentions. It may be that the poorer episodic memory the person has, the less likely they are to spontaneously remember at some point that they forgot to do something. For example, the person with poorer episodic may be more likely to forget for good that they intended to contact a friend or watch a movie on TV, so they may not be aware that they had such intentions. If this is a case, MCI individuals may be less likely, compared to healthy older adults, to spontaneously remember previously forgotten intentions and therefore less aware of the intentions they had.
To find more evidence in relation to this issue, we analyzed participants’ descriptions of the circumstances in which they remembered about previously forgotten intentions (i.e., their responses to a question about how they recovered from a failure). We found that, for both MCI individuals and healthy older adults, forgotten intentions were quite often recovered not through spontaneous remembering, but because the person found evidence that they had forgotten about something (e.g., they smelled the burnt toast, they realized that they had forgotten about an appointment when they saw an entry in their calendar the next day, they discovered pills left in the box). However, we also found that the percentage of prospective memory lapses that were accompanied by the recovery descriptions that clearly indicated spontaneous remembering was significantly higher in the healthy adult group (39%), compared to aMCI individuals (21%), p < 0.05. This finding is in accordance with our speculations that a lower ability of aMCI participants to spontaneously remember about forgotten intentions may have also contributed to the lack of evidence for prospective memory deficits in aMCI. Still, the results of the group comparisons in terms of participants’ description of how they later remembered the forgotten information should be taken with cautions as, in many instances, participants did not provide any information or the information provided was too vague to understand what the circumstances of the recovery from the lapse were.
From clinical perspective, the most interesting findings emerged when memory failures were further classified into several subcategories within each of the broad category of retrospective, prospective and absent-minded lapses (see Table 5). Our results showed that individuals with aMCI recorded significantly more lapses than controls in the following three subcategories: 1) forgetting appointments, 2) forgetting to carry out regular duties at home, and 3) not remembering well-learned procedures. The finding that individuals with MCI more often forgot about appointments is consistent with the results of the questionnaire studies that compared the performance of individuals with MCI and healthy older adults on the IADLs and included the keeping of appointments as a separate IADL domain (which was not always the case). These studies have consistently shown that individuals with MCI (or their carers) evaluate their functioning in this domain as poorer than healthy older adults, and as the domain that is most frequently affected among the IADL domains measured [77–79] (see also a meta-analysis [11]).
The two other specific types of failures that were experienced significantly more often by individuals with MCI in our study, represent difficulties on routine tasks that had been repeatedly performed by participants in similar circumstances in the past and, at least in case of well-learned procedures, they had been previously completed, by and large, automatically. These lapses thus resulted primarily from a failure of automatic/spontaneous processes in long-term memory. The group differences in this respect is a novel finding that is in accordance with the recently proposed Spontaneous Retrieval Deficit hypothesis [69, 80]. The hypothesis states that spontaneous retrieval from long-term memory is particularly disrupted in aMCI and therefore tasks relying on spontaneous/automatic retrieval should be most effective in discriminating aMCI patients from healthy controls and useful as early cognitive markers of disease. The hypothesis is consistent with the findings from several studies in which group differences were found in prospective memory tasks, relying on spontaneous retrieval [69, 82] and in the frequency of involuntary autobiographical memories [80] (see also [80], for a review of neuroscience data that supports the hypothesis). It is worth noting that the finding that memory failures in simple, routine tasks that rely mostly on automatic memory retrieval may be among those best discriminating individuals with aMCI from normally aging adults, is counterintuitive. Based on the cognitive aging literature [83–85], researchers and clinicians typically look for early cognitive markers of the Alzheimer’s disease in more demanding tasks that require effortful, strategic encoding and retrieval (for a review of currently used cognitive tasks that rely on such processes, see [1, 86]).
The results of more fine-grained analysis of memory failures, which showed significant group differences in forgetting appointments and the inability to perform well-learned procedures may be important clinically for improving the MCI diagnosis, which relies on self- or informant-reported memory problems in everyday life. Although these types of failures were not very frequently reported in the aMCI group, critically, they were totally absent in the diaries kept by healthy older adults. Therefore, when analyzing memory complaints and lapses of older adults in the context of possible cognitive decline, it may be worth paying special attention to these specific types of failures, which are not likely to happen in normally aging adults, especially in the short time frame. Future studies need to examine whether these specific types of failures will distinguish aMCI from other types of MCI and especially if they can predict the individual’s conversion to Alzheimer’s disease.
The present study has also significant methodological implications by showing that a diary of everyday memory failures, when each measurement is clear and brief, can be successfully used in the aMCI groups. First, the percentage of participants with aMCI who were given the diary booklet but did not complete the task of keeping a diary (19%), was not significantly different from the percentage of healthy adults (12%) who did not complete the study. The rest of the MCI participants, although they rated the diary method as more difficult compared to healthy older adults, kept the diary as instructed, with 91% of them keeping the diary every day for 7 days, compared to 95% of participants in the control group. Second, keeping a diary did not have any negative consequences on individuals with aMCI. If anything, their mood was significantly better in Session 2, after keeping a diary for a week, compared to Session 1. In addition, there was a significant tendency among aMCI participants to claim that keeping a diary reduced the number of lapses experienced rather than to claim that it had no effect or increased this number. Third, our findings support the validity of a diary of memory failures by demonstrating that, in some aspects, the diaries provided information about everyday functioning in aMCI that is consistent with the results obtained previously with other methods, such as everyday memory questionnaires (about overall higher frequency of memory failures in MCI) and IADL questionnaires (about forgetting appointments as a failure that very well discriminates MCI from healthy aging). In other aspects, our diaries provided new findings about the contribution of distinct memory abilities and memory processes to the deficits in the performance of complex everyday tasks by individuals with aMCI.
Despite its usefulness, the diary method may pose some challenges, when used with individuals with aMCI, which should be taken into account in future research. As noted before, it may be that when cognitively impaired older adults progress to the more severe end of aMCI diagnosis, an insight into their functional and memory problems diminishes, which would make the diary method less useful. Moreover, the diary method requires participants’ commitment and high levels of compliance, which makes recruitment more challenging in both the aMCI and healthy adult groups. However, many participants were curious about their everyday memory failures and were willing to try the diary method, especially when informed that they could find recording memory lapses useful to them personally. Finally, we do recommend contacting participants every day to remind them about keeping a diary. Many participants found it very helpful when the issue was discussed at the post-diary session.
In conclusion, the findings of this diary study provide novel insights into functional impairments in aMCI and call for more targeted investigation of everyday memory failures that may be of special importance when analyzing older adults’ memory complaints in the context of possible cognitive decline. Thus, our results suggest that when older adults convert from normal aging to pathological cognitive decline (aMCI), their retrospective memory deficits should manifest in increased difficulties in performing retrospective memory-based everyday tasks that require retrieving information from the past and these difficulties should dominate their memory complaints. In contrast, we would not expect them to complain more about forgetting to complete delayed intentions (at least not when they live with their spouses) or about being absent-minded compared to healthy older adults. It is therefore retrospective/episodic memory that should be primarily targeted in neuropsychological interventions to improve the quality of their everyday life. Nevertheless, our results also suggest that certain types of prospective memory failures such as forgetting appointments and regular household tasks (which had been repeatedly completed previously) may be highly symptomatic of aMCI diagnosis and should merit further investigation.
Footnotes
ACKNOWLEDGMENTS
This research was supported by a Marie Sklodowska-Curie Intra-European Fellowship within the 7th European Community Framework Program. We would like to thank all the old age psychiatrists, clinical psychologists, and nurses from EMDASS and SMHT in Hertfordshire for their help in the recruitment process. We are particularly grateful to Kunle Ashaye, Amirtha Pasupathy, Shora Shaheen, Jenny Noero, Edward Smith, Marianne Kreutz, Guney Dillioglu, and Heather Condon for their support throughout the study and invaluable help in reaching our recruitment targets.