
Abstract
Background:
Cognitive disorders in old age have a serious impact on the health and social aspects of patients and their families.
Objective:
The scope of this paper is to explore the role of cobalamin and folate that has been linked to cognitive decline, not only as a deficiency state depending on malnutrition, but also a determinant in cognitive impairment.
Methods:
A 6-year observational, retrospective study was conducted by collecting the routine blood analyses and cognitive screening scores of patients aged 60 years or older, followed at our Centre for the Diagnosis and Treatment of Cognitive Disorders.
Results:
In a linear regression with a multi-vitamin model, higher folate concentrations were correlated with better cognitive performances through MMSE score, even after correction for sex, age, and years of education (beta = 0.144, p = 0.001). Estimated MMSE marginal means for folate versus homocysteine showed that folate deficiency was associated with worse cognitive performances, with a more severe cognitive impairment when hyperhomocysteinemia was present.
Conclusion:
The assessment of B-vitamin status among elderly adults can contribute to an economic and practical approach to the prevention and management of cognitive decline. Future studies focused to define optimal vitamin status are warranted.
Keywords
INTRODUCTION
With the increase in longevity, there has also been an increase in the geriatric population. The consequent increase in cognitive disorders requires urgent understanding of the underlying mechanisms and modifiable causes in order to bring about the actuation of preventive measures [1]. Every 20 years, the number of individuals with dementia doubles [2]. In the 2010 World Alzheimer Report, the economic impact of dementia seems to exceed that of both cancer and cardiovascular disease expenditures combined [3].
Dementia is a multifactorial disease, with genetic and environmental etiology [4]. Among environmental factors, vitamin B12 (Cbl) and folate deficiencies have been proposed as indications for preventive practices [5, 6]. Low Cbl and folate concentrations are the primary determinants for the increase in homocysteine (HCY) levels.
The existence of an association between total blood HCY and B-vitamin concentrations with cognitive deficit was proposed [7–9].
Although, not without criticism [10], hyperhomocysteinemia has been linked to cardiovascular diseases [11], but it also seems to be linked to dementia as an independent risk factor [12]. Elevated HCY levels can act through oxidative stress against endothelial and neural cells [13, 14].
It seems that in the adult brain, the dominant function of folate metabolism is probably the recycling of HCY and the supply of methyl groups for purine and pyrimidine synthesis [15].
Vascular dementia, Alzheimer’s disease (AD), and, more in general, cognitive impairment are associated with high concentrations of total plasma HCY, as highlighted by many prospective and cross-sectional studies [8, 16–19]. Nevertheless, it was also postulated that the rise in HCY is a secondary phenomenon in vascular dementia and AD in older people with cognitive symptoms [20].
High concentration of HCY, together with low concentration of Cbl, are also frequent among patients with early signs of Parkinson’s disease and correlates with the progression of the disease and the worsening of cognition [21].
Unfortunately, B-vitamin as treatment for lowering total HCY levels gave inconsistent results in cognitive recovery, as shown in randomized controlled trials, although this may depend on heterogeneity of the studies [22, 23]. In contrast, vitamin B12 intervention to asymptomatic elderly subjects with low serum Cbl, ameliorated peripheral nerve conductivity while there was no improvement among participants with high serum folate [24]. So, it seems that treatment of non-genetic risk factors in preclinical stage of dementia is crucial, before it can manifest with its major symptoms [25, 26]. Victor Herbert suggested that Cbl deficiency is a gradually progressive disorder, in a continuum from asymptomatic vitamin depletion to clinical deficiency [27]. He defined a model of sub-clinical signs of deficiency with corresponding blood levels, including HCY, in which he showed that the anemic manifestation of Cbl deficiency could proceed to irreversible neuropathologic modifications [28]. Neuropsychiatric symptoms in Cbl deficient subjects are common and precede hematological manifestations in up to 50% of patients [29].
The occurrence of chronic Cbl and folate deficiency among the European elderly population has been confirmed [30, 31]. This deficiency status among older people depends presumably more on common atrophic gastritis, with its higher prevalence with aging, than on poor dietary intake [32–34]. Even if the development of cognitive impairment is a multifactorial phenomenon, there are recurrent causes like age, hyperhomocysteinemia, and hypertension. Xu and colleagues, after a pooled analysis of 6,310 subjects from 13 cohort studies classified the association between increased total serum HCY and AD as a Grade I evidence [35].
The association was also significant for MTHFR polymorphism in a meta-analysis with Mendelian randomization with 9,397 subjects from 34 studies [36]. In the VITACOG randomized trial on elderly people, a combination of B-vitamins slowed cognitive decline and brain atrophy only among participants with serum HCY levels above 11 μmol/L [37, 38].
HCY might influence cognition through non-mutually exclusive, multiple mechanisms: impaired methylation, oxidative stress, apoptosis, antagonistic action to NMDA receptors, formation of neurofibrillary tangles and senile plaques [39–42]. As with HCY that might act as a vasculotoxic and neurotoxic factor, the accumulation of methylmalonic acid (MMA) caused by B-vitamin deficiency, can cause abnormal incorporation of fatty acids in the neuronal membrane with consequent neuropsychiatric symptoms [29, 43].
The literature highlights the importance of B-vitamins for brain functions. Moreover, even if folate and Cbl shortage are well defined, a worldwide challenge is to identify from more population-based data valid cutoffs for the subclinical deficiency, which is more widely spread than clinically evident deficiency [44, 45]. Although interventions to ameliorate cognitive symptoms in the elderly are of great importance, prevention would be the best approach. To better understand the role of commonly used blood markers during routine screening in health centers, we explored the association between some B-vitamin serum markers and common cognitive tests, in patients with suspected cognitive impairment, followed at a public, dedicated outpatient clinic. Our aim was to find key, commonly available markers and their cut-off points, that discriminate the consequences of the early-onset nutritional deficiencies, related to cognitive impairment, in order to identify early markers that can promote the development of supplementation programs for prevention.
MATERIALS AND METHODS
Study design and participants
This observational, retrospective study was conducted on 6 years of consecutive records (between June 2012 and May 2018) at the Northern District of the Local Health Unit of Treviso (Italy). Patients included in the study were enrolled from the elderly individuals accessing for the first time the center for diagnosis and treatment of cognitive disorders during the reference period. All patients were living at home.
Inclusion criteria
We enrolled 700 patients who consulted the specialist center for the first time. We excluded individuals: younger than 60 years; taking B-vitamin supplementation; treated with acetylcholinesterase inhibitors or memantine; affected by diseases that influence cognitive status (i.e., thyroid dysfunctions, brain trauma, psychiatric disorders), apart from individuals with vascular alterations of the white matter at the neuroimaging. Accordingly, we excluded 131 subjects.
Assessments
Routine blood analyses performed on admission were collected (hemoglobin, mean corpuscular volume, platelet count, and some markers for B-vitamin status, i.e., Cbl, folate, and HCY), together with clinical condition and the presence of clinical and pharmacological risk factors (gastric surgery, chronic kidney disease, alcoholism, psoriasis, hypothyroidism, L-DOPA, anticonvulsants, metformin, and antacid use).
Serum Cbl and folate detection were performed by Immulite 2000 immunoassay system (Siemens), through solid-phase competitive chemiluminescence enzyme immunoassay. Plasma HCY detection was performed by Cobas c702 chemistry analyzer (Roche), through a two-step assay (reduction of HCY forms and enzymatic conversion) using specific reagents (Axis-Shield). The protocols were executed according to the manufacturer’s specifications.
By considering that there is no consensus on how to define B-vitamin status, patients were categorized by applying different cut-offs found in the literature. Specifically, for Cbl, a cut-off of 148 pmol/L (equivalent to 200 pg/mL), commonly used to describe Cbl deficiency [46], was used, while a cut-off of 360 pmol/L (equivalent to 488 pg/mL), proposed by Herrmann to better discriminate functional vitamin shortage in critical conditions [47], was used. Three different cut-offs (2.2, 3, and 4 ng/mL) were used for folate deficiency [46, 49]. Finally, the cut-offs used for HCY were 15 and 12 μmol/L [46, 51].
All patients were evaluated by a neurologist, using the Mini-Mental State Examination (MMSE), a screening tool for cognitive impairment in elderly adults. The MMSE consists of a variety of questions, and ordinarily can be administered in 5–10 minutes. The questions explore seven cognitive domains or functions: Orientation to time and place (10 points); Registration of three words (3 points); Attention and calculation (5 points); Recall of three words (3 points); Language (8 points); and Visual construction (1 point). The maximum score is 30. A score of 23 or lower is indicative of cognitive impairment, more precisely a score of 23-18 is considered as a mild, and a score 17-0 as a severe grade of cognitive impairment. Since its creation, the MMSE has been validated and extensively used in both clinical practice and research [52–54]. We also evaluated the individual years of education of the sample.
Neuroimaging data from CT scan or MRI were available for a subgroup of patients.
All measurements were performed once, on admission. Although the global assessment of the patients involved a number of examiners, each single analysis was performed by the same examiner. In particular, the MMSE was performed by one neurologist (B.L), and was always performed in the same dedicated place, unfamiliar to the patient, and with only the patient and examiner present. Data analyses were conducted in a single laboratory and under standardized conditions.
Data collection was performed anonymously. Written informed consent of the participants was collected according to the respective regulation for retrospective studies. The study was conducted in accordance with the Helsinki Declaration and approved for clinical trials by the local ethics committees of Treviso and Belluno (Veneto, Italy, 533/CE Marca, 09.17.2018).
Statistical analysis
Summary statistics were calculated for all variables. The normality of plasma biomarker levels for B-vitamin status (Cbl, folate, and HCY) was checked by Kolmogorov-Smirnov tests and log-transformations were applied. The chi-square test was adopted for categorical data. For continuous data, to carry out the assessment of the differences between two, or more than two independent groups of patients, the two-tailed t-test or ANOVA, were performed, respectively.
Linear regression models were estimated to test the association of each log-transformed B-vitamin status biomarker (Cbl, folate, and HCY) with the MMSE score (‘Single vitamin models’), with adjustment for sex, age and years of education. A linear regression model with all the three log-transformed B-vitamin status biomarkers was estimated (‘Multi-vitamin model’), with adjustment for sex, age and years of education. Finally, interaction effects were accounted for.
All p values were two-tailed, with a significance level of 0.05. No multiple testing correction was applied due to the exploratory nature of the study. Analyses were performed by SPSS 22.0 for Windows.
By focusing on the Multivitamin model, the sample size of 569 achieved 100% power to detect a percentage of explained variance of 8.3% attributed to the 3 markers (Cbl, Folate, HCY) using the F-test with a significance level of 0.05. The variables tested were adjusted for age, sex and years of education with an additional percentage of explained variance of 16.4%. The power calculation was performed by using PASS 11 Professional.
RESULTS
A total of 569 patients, 226 male and 343 female (mean age 78.8, SD 6.6, range 60–96), were eligible for the study. Mean years of education was 6.0 with a median of 5.0 (range 0–21). The description of the markers for B-vitamin status is given in Table 1.
Markers for B-vitamin status (n = 569)
By considering the MMSE score, the mean score was 22.63 (SD 5.57), while the categorization showed that 52.5% of patients fell in the range of normal cognitive status (score 30-24), 29.2% resulted affected by a mild (score 23-18), and 18.3% by a severe grade of cognitive impairment (score 17-0).
The neuroimaging data, available for 510 patients (89.6%), showed vascular encephalopathy (VE), consisting in focal and/or diffuse vascular alterations of brain density, in 80.2%; brain atrophy without vascular alterations of the white matter (BA) in 11.0%; only 8.8% were normal.
Mean Hb, MCV, and platelets values fell within the normal range (13.62, SD 1.36 g/dL; 93.19, SD 5.10 fL; 240.81, SD 72.10 103/fL, respectively).
16.9% of patients had a Cbl level below 148 pmol/L, and 71.1% fell in the range 148–360 pmol/L, which identifies the “grey zone” where functional deficiency (if MMA detection is not available) can be present. Considering both situations (clinical and functional deficiency, below the cut-off of 360 pmol/L) the total percentage was 88%. Using the lowest cut-off, the deficiency of folate was present in 6.3% of patients. This percentage increased to 19.5% by using 3 ng/mL as cut-off, and to 40.4% with the highest cut-off. Using the highest and more frequently used cut-off of 15 μmol/L, 55.9% (n = 318) of patients had hyperhomocysteinemia, while the other cut-off of 12 μmol/L raised this percentage to 81.4% (n = 463).
By using the aforementioned cut-offs, the association between B-vitamin status deficiency and hyperhomocysteinemia and age showed an increase with age for all markers, with the exception of the 148 pmol/L Cbl cut-off which had the highest deficiency for the 60–64 age range. The comparison did not reach statistical significance for Cbl (for neither cut-off), nor for the lowest folate cut-off (Table 2).
Prevalence of Cbl and folate deficiency and hyperhomocysteinemia for age ranges
The comparison of the prevalence of B-vitamin status deficiency between males and females was not significant.
Regarding the clinical and pharmacological risk factors that can influence B-vitamin deficit and hyperhomocysteinemia, 43.8% of participants had Cbl risk factors (gastric resection, alcoholism, psoriasis, anticonvulsant, metformin, and antacid use), 1.6% folate risk factors (alcoholism, psoriasis, anticonvulsants use) and 16.5% HCY risk factors (chronic kidney disease, hypothyroidism, L-DOPA and anticonvulsant use) (Table 3). B-vitamin deficiency and hyperhomocysteinemia were not associated with the presence of the aforementioned risk factors (Chi-square tests, p > 0.05).
Prevalence of the clinical and pharmacological risk factors for B-vitamin deficit and hyperhomocysteinemia (n = 569)
The comparison of the prevalence of B-vitamin status deficiency and hyperhomocysteinemia among MMSE categories showed an increase for all markers depending on cognitive impairment and reached statistical significance for all cut-offs for folate and HCY, and only for the 360 pmol/L cut-off for Cbl (Table 4).
Cbl and folate deficiency and hyperhomocysteinemia by cut-off levels and cognitive impairment category (MMSE) prevalence (n = 569)
By considering neuroimaging results (normal, VE, BA) and B-vitamin status, only HCY resulted significantly associated (<12 deficiency: 71.1%, 84.6%, 62.5%, p < 0.001; <15 deficiency: 33.3%, 57.9%, 44.6%, p = 0.002, respectively).
Linear regression models with each log-transformed B-vitamin status biomarker as an independent variable and the MMSE score as a dependent one (‘Single vitamin models’) showed that higher levels of folate were significantly correlated to a lower cognitive impairment (Beta = 0.178 with p < 0.001), while higher HCY concentrations were significantly correlated to a higher cognitive impairment (Beta = –0.149 with p < 0.001) (Table 5).
Linear regression models with MMSE score as the dependent variable and each log-transformed marker for B-vitamin status as the independent variable, together with sex, age and years of education as confounders (n = 569)
In the ‘Multi-vitamin model’, estimating the association between the three biomarkers and the MMSE score, HCY lost its significance (Beta = 0.076 with p = 0.092). Higher folate concentrations confirmed to be correlated with better cognitive performances (Beta = 0.144 with p = 0.001) (Table 6). All models were adjusted for sex, age and years of education.
Linear regression model with MMSE score as the dependent variable and all log-transformed markers for B-vitamin status as independent variables, together with sex, age and years of education as confounders (n = 569)
Finally, when interaction terms were introduced, only the effect between HCY and folate resulted significant (Beta = 0.536 with p = 0.016). As shown in Fig. 1, estimated MMSE marginal means for the highest folate cut-off (4 ng/mL) versus HCY (on the left HCY cut-off of 15 μmol/L, on the right HCY cut-off of 12 μmol/L) put in evidence that folate deficiency was associated with worse cognitive performances and, more remarkable, that the cognitive impairment became more severe when hyperhomocysteinemia was present.
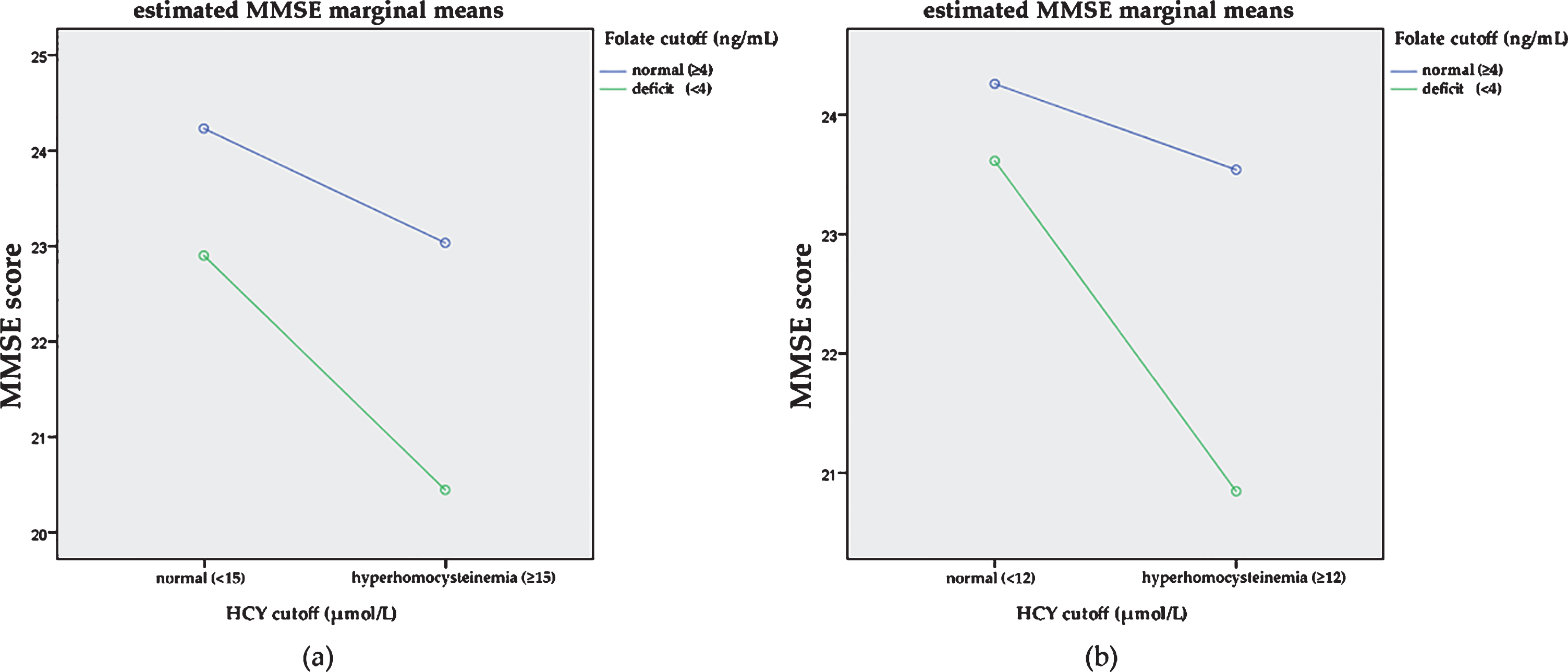
Estimated MMSE marginal means for the highest folate cut-off (4 ng/mL) versus HCY: (a) HCY cut-off of 15 μmol/L; (b) HCY cut-off of 12 μmol/L.
DISCUSSION
The screening for vitamin B12 and folate deficiency in elderly patients with cognitive disorders is already a recommended procedure in The American Psychiatric Association Practice Guidelines for the Psychiatric Evaluation of Adults [55]. Folate and Cbl deficiency could enhance cerebral atrophy and dementia risk among elderly because they are the major determinants of total HCY increase [56–58].
In 2017, an international consensus analyzed clinical studies that manipulated nutritional risk factors and stated that for the development of dementia, AD, and cognitive decline in the elderly, high concentration of total HCY is a modifiable risk factor, even in case of moderate hyperhomocysteinemia (>11 μmol/L), very common at this age [59]. These conclusions, even if further trials are needed to define interventional conditions, are of major public health significance.
Heterogeneity of cut-offs for normal status is presently a problem in need of further study [58, 61]. In a recent review of Allen and coworkers on vitamin B-12, deficient, depleted, and normal cutoffs at different ages were proposed but the authors highlighted the importance of multiple markers use for better prevention of clinical outcomes of B-vitamin deficiency [44].
Vogiatzoglou and colleagues explored plasma MMA and HCY measurements in a large population including elderly adults (71–74 years) in the Norwegian Hordaland Homocysteine Study, and assessed that a replete vitamin B12 status can be found with vitamin B12 levels ≥400 pmol/L [62].
In our patients, mean Cbl concentration was above 148 pmol/L cut-off, but fell in the range of risk of functional deficiency of 148–360 pmol/L. Mean folate concentration was above all cut-offs, while HCY was hyperhomocysteinemic for all cut-offs considered.
Cognitive impairment was present in 47.5% of the study sample, as displayed by a low MMSE score for mild and severe grade of impairment in 29.2% and 18.3% of the sample, respectively.
Moreover, only 8.8% of patient with neuroimaging data showed no functional issues of VE or BA. These aspects point out the prevalence of brain damage of the sample.
Cbl, folate, and HCY are routine markers used in neurogeriatric healthcare. But their interpretation depends on the cut-off applied. A minor percentage of patients displayed deficiency of Cbl and folate at lower cut-offs, but at the higher value, prevalence of Cbl deficiency reversed (16.9% versus 88.0%, respectively), with 71.1% of patients falling in the “grey zone” of possible functional deficiency. A gradual increase in folate deficiency prevalence was observed from 6.3% to 40.4%, with the increase of cut-off value. Two different values for HCY cut-off were used with the rise of deficiency from 55.9% to 81.4% of patients using 15 or 12 μmol/L cut-off values, respectively. Taking into account the prevalence of cognitive issues, less stringent cut-offs for blood markers could better describe an association with cognitive impairment. Moreover, stratification for age showed that the deficiency prevalence trend was significant only for HCY and for 3 ng/mL and 4 ng/mL folate cut-offs. In our sample, no trend was statistically significant for Cbl; moreover, no association among sex and markers emerged.
Linear regression models explored the effect of marker concentrations and sex, age, and years of education as confounders on the MMSE score. ‘Single vitamin models’ showed that higher folate levels were significantly correlated to a lower cognitive impairment, while higher HCY concentrations were significantly correlated with a higher cognitive impairment. In the ‘Multi-vitamin model’, only higher folate concentrations confirmed to be significantly correlated with better cognitive performances. Moreover, sex was not correlated with MMSE score, while age and education were negatively and positively correlated with MMSE score, respectively, in both single-vitamin and multi-vitamin models.
It is still a matter of debate, whether hyperhomocysteinemia is only a marker or one of the direct causes of cognitive impairment, which include B-vitamin deficiency [63–65]. Interestingly, prospective studies have shown an association between hyperhomocysteinemia and cognitive outcomes, even after B-vitamin status adjustment [64]. The VITACOG B-vitamin supplementation trial evidenced decreased total homocysteinemia, and reduced brain atrophy and cognitive decline [66]. In the preliminary sample of the Treviso Dementia (TREDEM) retrospective cohort study, associations were found between low folate concentrations and cortical-subcortical atrophy, as well as between hyperhomocysteinemia and severe cortical-subcortical and hippocampal atrophy [67]. The gradual rise of HCY levels is an important factor in the concentration-effect relationship, as shown in an Italian prospective study, in which an increase of total HCY >15.0 μmol/L from baseline in healthy elderly was responsible for a 5-fold higher incidence of dementia, when compared with subjects with an increase of <10.1 μmol/L [68]. Similar results were found by the OPTIMA study, but with a greater cognitive decline in patients with AD, over a range of total HCY between 10.0 and 18.0 μmol/L [69]. A key role could be represented by the variation of individual HCY concentration. In fact, in 1,670 Norwegian elderly people, the mean memory test score was lower in subjects with an increase of up to 8 μmol/L in total HCY, over a 6-year period, when compared to those with no variation or decreased by up to 6 μmol/L, over the same period [70].
Cases of reversible dementia with Cbl therapy are very rare [71]. However, among participants with mild cognitive impairment at baseline in the VITA cohort study, cobalamin or folate users were protected from progression to dementia [72]. Taking into account the costs for the cures and their efficacy, screening for hyperhomocysteinemia and the consequent intervention with B-vitamin supplements could be a beneficial approach [73].
In our study, the loss of significance for the correlation between HCY and MMSE in the ‘Multi-vitamin model’, adjusted for sex, age and years of education, may suggest that the role of folate may act in part through HCY mechanisms. Our population sample had a large prevalence of Cbl functional deficiency, as expressed by Cbl values from 148 pmol/L to 360 pmol/L and by HCY values. A population with a significant percentage of Cbl replete individuals could show a better correlation between vitamin and cognition. Conversely, a significant folate correlation with MMSE may suggest a role of folate that is independent of HCY. The highest prevalence of folate deficiency (40.4%) was achieved using the 4 ng/mL cut-off.
The analysis of marginal mean interactions showed a stronger interdependence of HCY levels with MMSE among individuals with folate levels below the 4 ng/mL cut-off. Lower scores, in the case of hyperhomocysteinemia, were more evident with folate deficiency. This phenomenon was more evident with the less stringent cut-off considered for hyperhomocysteinemia estimation (12 μmol/L). Taking into account our sample population, hyperhomocysteinemia increased from 55.9% to 81.4%, by changing the HCY cut-off from 15 to 12 μmol/L. If we consider the 15 μmol/L cut-off, 140 individuals have normal levels of folate (cut-off: 4 ng/mL) and 178 show folate deficits. In the case of the 12 μmol/L cut-off, 246 individuals have normal folate levels and 217 folate deficits. So, the use of wider cut-offs could indicate a better correlation with cognitive impairment and might be more adequate for an elderly population.
This study was conducted on a large sample of subjects, for whom data on Cbl, HCY, and folate concentrations and on cognitive impairment assessed by a standardized instrument (MMSE) were available. Moreover, neuroimaging results cover a wide portion of the sample.
Among its possible limitations, the sample was selected for cognitive issues with high prevalence of vitamin B shortage, as defined by the wider cut-offs. Moreover, patients followed by a center for the diagnosis and treatment of cognitive disorders are on average people with non-cognitive problems or mild brain damage, while patients affected by severe levels of impairment, seek health services less frequently. This could influence the association between vitamin status and cognitive status. Moreover, more specific markers like MMA and holotranscobalamin II could disentangle the vitamin B status, even though these markers are not routinely adopted.
Conclusions
From our study, we suggest what is already known in the available literature, namely that folate deficiency is associated with worse cognitive performances. But, given the design of our observational study, we cannot establish a causative relationship. We also suggest that the co-presence of hyperhomocysteinemia could represents a detrimental factor. However, it needs well designed clinical trials to confirm that prevention of hyperhomocysteinemia and folate deficiency could prevent cognitive dysfunctions.
With respect to other studies, we found no clear, direct association between cognitive impairment and vitamin B12 status: it could be that the latter may act indirectly, by raising HCY levels, or that the study’s sample characteristics do not permit finding this correlation.
Although the assessment of vitamin status among elderly adults followed in geriatric neurology health centers can contribute to an economic and practical approach to the prevention and management of cognitive decline, nevertheless the detection of a high incidence of non-optimal B-vitamin status does not imply that cognitively impaired elderly people can benefit from its normalization: the results from interventional supplementation for cognitively impaired elderly adults are in fact conflicting and do not univocally address the effectiveness of supplementation. B-vitamin deficiencies can develop and progress throughout life from an earlier adult age and therefore could lead to cognitive damage only in the advanced years. New clinical trials performed in the preclinical phases of B-vitamin deficiency could highlight the importance of maintaining a lifelong optimal B-vitamin status.