
Abstract
Background:
The efficacy and safety of glycogen synthase kinase 3 (GSK-3) inhibitors in patients with Alzheimer’s disease (AD) is unknown.
Objective:
A systematic review and meta-analysis of randomized controlled trials (RCTs) to test GSK-3 inhibitors on AD patients.
Methods:
We included RCTs of GSK-3 inhibitors in AD patients and subjects with mild cognitive impairment (MCI), using cognitive function scores as a primary measure.
Results:
Five RCTs (three RCTs using lithium and two RCTs using tideglusib) with 568 patients were included. There was no significant difference in cognitive function scores between the GSK-3 inhibitors and placebo groups [standardized mean difference (SMD) = –0.25, p = 0.11, I2 = 55% ]. However, significant heterogeneity remained. A sensitivity analysis revealed that the lithium subgroup was more effective on cognitive function scores than placebo for AD and MCI (lithium subgroup: SMD = –0.41, p = 0.04; tideglusib subgroup: SMD = –0.02, p = 0.89). Moreover, a meta-regression analysis showed that the effect size of GSK-3 inhibitors on cognitive function scores was associated with study duration (coefficient, –0.0116). For safety outcomes, tideglusib was associated with a higher incidence of increased aspartate aminotransferase than placebo. There were no significant differences in other secondary outcomes between treatments.
Conclusion:
Our results suggested that GSK-3 inhibitors were ineffective in treating AD and MCI; however, several studies included in the present meta-analysis were small, and future studies using a larger sample size are needed.
INTRODUCTION
Alzheimer’s disease (AD) is a neurodegenerative disease characterized by the progressive loss of cognitive function and neurobehavioral symptoms; it is the most common cause of dementia [1]. Approved treatments for AD, including cholinesterase inhibitors (donepezil, galantamine, and rivastigmine) and an N-methyl-D-aspartate receptor antagonist (memantine), temporarily alleviate symptoms, but their effects are limited. Therefore, new therapeutic drugs need to be developed [2, 3].
A recent study identified glycogen synthase kinase 3 (GSK-3) as a potential therapeutic target for AD [4]. GSK-3, which is a multitasking serine/threonine protein kinase, is the major kinase responsible for phosphorylating the tau protein [5]. GSK-3 overexpression produces tau hyperphosphorylation and neurodegeneration in transgenic mice [6]. In addition, recent studies have suggested that GSK-3 overactivity is associated with increased amyloid-β production, local plaque-associated microglial-mediated inflammatory responses, and memory impairment [7]. Moreover, GSK-3 inhibition reduced tau phosphorylation and amyloid-β prediction in in vitro and in vivo studies [5, 7–9].
Recently, two types of GSK-3 inhibitors, lithium and tideglusib, were tested in patients with AD [10–14]. A recent meta-analysis of three randomized controlled trials (RCTs) suggested that lithium was superior to placebo in improving cognitive function in patients with AD and in subjects with mild cognitive impairment (MCI) [15]. However, tideglusib showed no significant difference between treatments for mild-to-moderate AD in two phase II studies [13, 14].
These discrepant results may be due to the small sample sizes in the trials and/or study design differences. Therefore, we conducted a systematic review and meta-analysis to clarify the efficacy and safety of GSK-3 inhibitors for AD treatment.
MATERIALS AND METHODS
This systematic review and meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA checklist, Supplementary Material 1) [16] and was registered with the International Prospective Register of Systematic Reviews (PROSPERO, available in the public domain at http://www.crd.york.ac.uk/PROSPERO/. CRD42019118804).
Search strategy and inclusion criteria
We included only RCTs on the GSK-3 inhibitor treatment in patients with AD or subjects with MCI. To identify relevant studies, two authors (S.M. and H.T.) independently searched the MEDLINE, Cochrane Library, and Scopus databases, without language restrictions, from the date of these databases’ inception to April 2, 2019, using the following search strategy: ("Alzheimer Disease”[Mesh] OR “Alzheimer disease” OR “Alzheimer’s disease” OR “mild cognitive impairment”) AND ("Glycogen Synthase Kinase 3"[Mesh] OR “Glycogen Synthase Kinase 3” OR “GSK-3” OR “Lithium” OR “Tideglusib”) AND (“randomized” OR “randomly” OR “random”). They also searched ClinicalTrials.gov (http://clinicaltrials.gov/), the ISRCTN registry (https://www.isrctn.com/), and the International Clinical Trials Registry Platform (http://www.who.int/ictrp/en/) websites to ensure comprehensive inclusion of RCTs and to minimize the possibility of publication bias. They independently assessed the inclusion/exclusion criteria and selected the relevant studies. References to included articles and reviews also were searched for citations of additional relevant published and unpublished studies, including conference abstracts.
Data synthesis and outcome measures
The primary outcome was the change in cognitive function scores from baseline to the last available follow-up. Cognitive function scores were derived from the Alzheimer’s Disease Assessment Scale-cognitive subscale (ADAS-cog) [17] and the Mini-Mental State Examination (MMSE) [18]. The following secondary outcomes were also assessed: Neuropsychiatric Inventory (NPI12) [19] total scores, word fluency test [20], discontinuation due to all-cause, discontinuation due to adverse events, incidence of individual adverse events, and biomarkers in cerebrospinal fluid (CSF) [P-tau 181, total tau (T-tau), and amyloid-β 42 (Aβ42)]. When multiple intervention groups of GSK-3 inhibitors (e.g., 1000 mg/day of tideglusib and 500 mg/day of tideglusib) were present in a study, all intervention groups were combined into one group. The selected trials’ methodologic quality was assessed according to the risk-of-bias criteria in the Cochrane Handbook for Systematic Reviews of Interventions (version 5.2.0; Cochrane Collaboration, available in the public domain at http://training.cochrane.org/handbook).
Data extraction
Two authors (S.M. and H.T.) independently extracted data from the included studies. Where possible, an intention-to-treat or a full analysis set population was used. When such data were unavailable, the per protocol analysis results were extracted from each study. When data required for the meta-analysis were missing, investigators or the pharma sponsors of the relevant study were contacted and asked to provide unpublished data.
Meta-analysis methods
The meta-analysis was conducted using Review Manager software (version 5.3 for Windows; Cochrane Collaboration, available in the public domain at http://tech.cochrane.org/revman). A random effects model was selected for this meta-analysis because of its potential heterogeneity across studies. Dichotomous outcomes were presented as risk ratios (RRs) with 95% confidence intervals (CIs). When the random effects model showed significant differences between groups, the number needed to harm (NNH) was calculated. The NNH values were derived from the risk difference (RD) using the following formula: NNH = 1/RD. Continuous outcomes were analyzed using the mean difference (MD) or, when different studies used different scales, the standardized mean difference (SMD). Lower MMSE and word fluency test scores indicated more impairment, or more severe symptoms; thus, the algebraic sign of the numerical scores was reversed for these scales. Study heterogeneity was assessed using the I2 statistic, with I2≥50% reflecting considerable heterogeneity [21]. In cases with I2≥50% for the primary outcome measure, we conducted sensitivity analyses to determine the reasons for heterogeneity. We examined the following confounding factors: type of drug (lithium versus tideglusib), severity of disease (mild-to-moderate AD versus MCI), and study duration (≤26 weeks or >26 weeks). A meta-regression analysis was performed to evaluate the association between the results of the meta-analysis on cognitive function scores and certain modulators (patient age and study duration) using Comprehensive Meta-Analysis software, version 3 (Biostat, Inc., Englewood, NJ, USA). Funnel plots were examined visually to assess publication bias in primary outcomes when >10 studies were included [21].
RESULTS
Study characteristics
Of the 234 articles obtained from our literature search, 63 were excluded because they were duplicates, 158 were excluded after a review of the abstract or title, and eight were excluded after a review of the full text (two non-RCTs, five review articles, and one study protocol). No further studies were added from the clinical trials registration. Five RCTs that tested GSK-3 inhibitors for AD and MCI were accepted for the current meta-analysis [10–14] (Supplementary Material 2).
Two studies assessed the effects of lithium on AD [10, 11], one study assessed the effect of lithium on amnestic MCI [12], and two studies assessed the effect of tideglusib on AD [13]. Four studies were double-blind RCTs [11–14] and one was a single-blind RCT [10] (Table 1). The study duration of the included studies was 34.6 weeks, and the mean patient age was 72.5 years. One study included four arms (Lovestone 2015 study of 1000 mg of tideglusib once a day, 1000 mg of tideglusib every other day, 500 mg of tideglusib once a day, and placebo) [14], and two studies included two arms [10–13]. One study was supported by funding from AstraZeneca [10], and two studies were supported by funding from Noscira SA [13, 14].
Characteristics of included randomized controlled trials
AD, Alzheimer disease: ADAS-cog, Alzheimer’s Disease Assessment Scale-cognitive subscale: ADCS-ADL, Alzheimer’s Disease Cooperative Study–Activities of Daily Living: AEs, adverse events: Aβ, amyloid-β: CDR-SB, Clinical Dementia Rating-Sum of Boxes score: CGI-C, Clinical Global Impressions of Change: CSF, cerebrospinal fluid: DBRCT, double-blind randomized controlled trial: DRS, Delayed Recall Score: DSM-IV-TR, Diagnostic and Statistical Manual of Mental Disorders-4th edition-text revision: EQ-5D, EuroQol 5-dimensional: FRS, Figure Recall Score: GDS, Geriatric Depression Scale: GSK, glycogen synthase kinase: ITT, intention to treat: MCI, mild cognitive impairment: MMSE, Mini-Mental State Examination: n, number of patients: NINCDS-ADRDA, National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association: NPI, Neuropsychiatric Inventory: NR, not report: PLA, placebo: PP, per protocol: P-tau, phosphorylated tau: QD, once a day: QOD, every other day: SBRCT, single-blind randomized controlled trial: SD, standard deviation: SLN, Sequence of Letters and Numbers score: TID, tideglusib: TMT, Trial Making Test: T-tau, total tau: WF, word fluency: y, years.
The methodologic quality of the included studies was evaluated according to the Cochrane risk-of-bias criteria (Supplementary Material 3). Three studies did not mention the randomization method [11–13]. Furthermore, four studies did not mention the method of allocation concealment [10–13]. One study was not blinded to the investigators [10], and two studies used a per protocol analysis [10, 11].
Results of the meta-analysis
Efficacy outcomes
No significant difference between the GSK-3 inhibitors and placebo groups were found in cognitive function scores (SMD = –0.25, 95% CI = –0.56–0.06, p = 0.11, I2 = 55%; N = 5, n = 527; Fig. 1) or secondary outcomes (NPI12 and word fluency test; Supplementary Material 4).
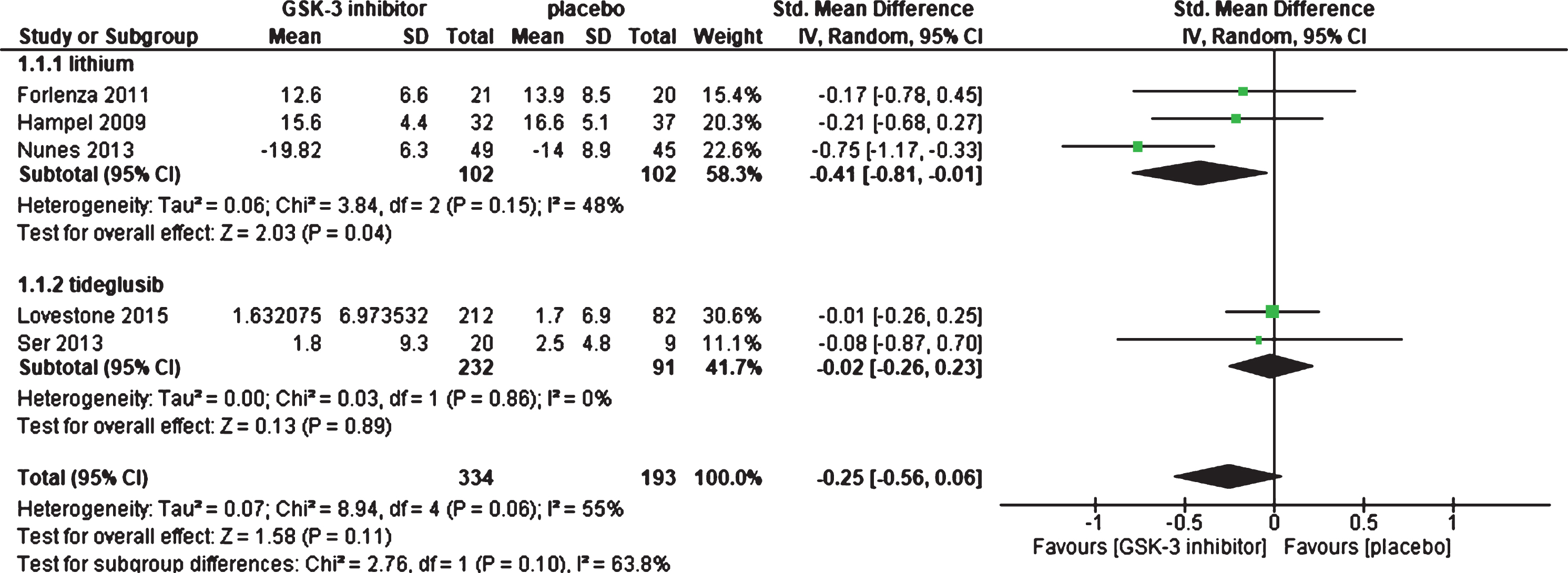
Forest plot of cognitive function scores.
We detected considerable heterogeneity in the cognitive function scores (I2 = 55%). Therefore, we performed three sensitivity analyses to identify the confounding factors affecting these scores (Table 2). When divided according to the type of drug (lithium or tideglusib subgroups), the significant heterogeneity disappeared in both subgroups; moreover, there was a significant effect of the lithium subgroup (lithium subgroup: SMD, –0.41; 95% CI, –0.81 to –0.01; p = 0.04, I2 = 48%; N = 3, n = 204; tideglusib subgroup: SMD, –0.0.; 95% CI, –0.26–0.23; p = 0.89, I2 = 0%; N = 2, n = 323; test for subgroup differences, I2 = 63.8%, p = 0.1; Table 2). When divided according to the study duration (≤26 weeks or >26 weeks), the significant heterogeneity disappeared in the ≤26 weeks subgroup; however, significant heterogeneity remained in the >26 weeks subgroup (≤26 weeks subgroup: SMD, –0.06, 95% CI, –0.27–0.16, p = 0.61, I2 = 0%; N = 3, n = 392; >26 weeks subgroup: SMD, –0.51; 95% CI, –1.07–0.06; p = 0.08, I2 = 58%; N = 2, n = 135; test for subgroup differences, I2 = 52.5%, p = 0.15; Table 2).
Sensitivity analysis (glycogen synthase kinase 3 inhibitors for cognitive function scores)
CI, confidence interval; N, number of studies; n, number of patients; na, not applicable; SMD, standardized mean difference.
The meta-regression analysis showed that the GSK-3 inhibitors effect with respect to cognitive function scores was associated with the study duration (coefficient = –0.0116, 95% CI = –0.0223 to –0.0009, p = 0.0336; Table 3; Supplementary Material 5).
Meta-regression analysis (glycogen synthase kinase 3 inhibitors for cognitive function scores)
No significant differences in the CSF biomarkers (P-tau 181, T-tau, and Aβ42) were found between the GSK-3 inhibitors and placebo groups (Supplementary Material 4).
Safety outcomes
There was no significant difference in discontinuation due to all-cause or adverse events between the GSK-3 inhibitors and placebo groups (Supplementary Material 4). In addition, there was no significantly higher rate of at least one adverse event in the GSK-3 inhibitors compared to the placebo groups (Supplementary Material 4). With respect to individual adverse events, the tideglusib subgroup was associated with a higher incidence of increased aspartate aminotransferase compared to the placebo group (RR = 4.26, NNH = not significant; Supplementary Material 4).
DISCUSSION
Our meta-analysis results showed that GSK-3 inhibitors effect did not improve cognitive function scores, NPI12 scores, or word fluency test for patients with AD and subjects with MCI.
However, our meta-analysis results of the cognitive function scores displayed significant heterogeneity which, according to the sensitivity analysis, likely resulted from the study duration and type of drug. In the meta-regression analysis of study duration, there was a negative correlation between cognitive function scores and study duration. This sensitivity analysis result suggests that a long study duration may be more effective for patients with AD and subjects with MCI than a short study duration. In the sensitivity analysis based on the drug type, the lithium subgroup had less deterioration in cognitive function scores than the placebo groups without considerable heterogeneity. According to the results of a recent meta-analysis that examined the effectiveness and safety of cholinesterase inhibitors for AD, the effect size of cholinesterase inhibitors on cognitive functions scores was small (SMD = –0.38) and that of lithium was similar (SMD = –0.41) [22, 23]. These results suggest that lithium might be effective for AD patients and subjects with MCI. By contrast, there were no significant difference between the tideglusib subgroup and the placebo group. The discrepancy between the lithium and tideglusib subgroups can be potentially explained by the following reasons: 1) The RCTs of tideglusib had a shorter study duration than the RCTs of lithium (mean study duration: lithium = 42.3 weeks, tideglusib = 23 weeks). Because AD is a slow, progressive neurodegenerative disease, studies with longer intervention periods may be more effective than those with shorter intervention periods. 2) Differences between lithium and tideglusib action mechanisms may have influenced the results. Tideglusib irreversibly inhibits GSK-3 but does not block the whole enzyme in the cell [24]. In addition, tideglusib has shown to induce neuroprotection and attenuate the production of proinflammatory cytokines and activation of astrocytes and microglial cells in rat [25]. On the other hand, recent animal studies have suggested that lithium is not only a non-competitive inhibiter of GSK-3, but it also provides neuroprotection through anti-inflammatory effects on toll-like receptor 4, increasing neurogenesis, cell survival, and long-term potentiation via CREB-dependent transcription of brain-derived neurotrophic factor and prevention of long-term depression by inhibition of over-active metabotropic glutamate receptor-dependent synaptic transmission [26]. In addition, lithium is effective in the management of manic, depressive, and maintenance phases of bipolar disorder treatment.
There were no significant differences in CSF biomarkers (P-tau, T-tau, and Aβ42) between the GSK3-β inhibitor and placebo treatment groups for patients with AD and subjects with MCI. One of the reasons for these results might be the small sample size. We included only two RCTs (GSK3-β inhibitor group: 48 patients, placebo group: 54 patients) [10, 12] in the current meta-analysis of CSF biomarkers. Furthermore, these results might have been caused by the heterogeneities in study duration, drug dosages, and the stage of disease in each study in this meta-analysis. In a 10-week study by Hampel and colleagues [10], lithium was titrated to target serum levels of 0.5–0.8 mmol/l, and non-significant CSF biomarker changes were identified in patients with AD. However, in a 12-month study by Forlenza and colleagues [12], lithium was titrated to target serum levels of 0.25–0.5 mmol/l, and a significant decrease in CSF concentrations of P-tau was identified in subjects with MCI.
When assessing safety outcomes, our meta-analysis suggested that GSK-3 inhibitors were well tolerated except for increased aspartate aminotransferase levels with tideglusib treatment. However, our meta-analysis included only five RCTs with 568 patients and had a short study duration (mean duration 34.6 weeks). In addition, lithium has a high risk of toxicity due to the narrow therapeutic window and is reportedly associated with an increased risk of reduced urinary concentrating ability, hypothyroidism, hyperparathyroidism, and weight gain [27, 28]. Therefore, further studies with a longer duration and larger sample size are required to reach definitive safety outcome conclusions.
Several study limitations should be addressed. The meta-regression analyses were conducted using only five studies; therefore, the results of these analyses may be false positives. In addition, because a funnel plot is generally only used when >10 studies are included in the meta-analysis, this plot was not used to explore potential publication bias. Second, there is a possibility that the mechanism other than the GSK-3 inhibitory action of lithium may influence our results. Third, three of the included studies were industry sponsored, which tend to show more favorable efficacy results than those sponsored by other sources [29]; therefore, a sponsorship bias may exist in our results. Finally, since all study durations were short (mean duration 34.6 weeks), we could not determine GSK-3 inhibitors’ long-term efficacy and safety for AD patients based on our results.
In conclusion, our meta-analysis suggested that GSK-3 inhibitors were ineffective in treating AD and MCI; however, several studies included in the present meta-analysis were small, and future studies using a larger sample size are needed.
DISCLOSURE STATEMENT
Authors’ disclosure available online (https://www.j-alz.com/manuscript-disclosures/19-0256r1).