
Abstract
Background:
Type 2 diabetes (T2D) is associated with an increased risk of cognitive impairment and dementia with poorly understood underlying mechanisms.
Objective:
We examined the role of blood pressure (BP), aortic stiffness, and hemodynamics in this association.
Methods:
Cross-sectional sample of late middle-aged twins discordant for T2D from the Australian Twin Registry. Measurements included neuropsychological battery and brain MRI including arterial spin labelling (ASL) to measure cerebral perfusion. Mobil-o-Graph devices were used to non-invasively obtain 24-hour BP, aortic stiffness, and hemodynamic measures. Using mixed modelling, we studied associations of T2D with cognition, MRI measures, BP, aortic stiffness, and hemodynamics.
Results:
There were 23 twin pairs with mean age 63.7 (SD = 6.1) years. T2D (β=–0.45, p < 0.001) and age (β=–0.05, p = 0.022) were independently associated with poorer attention but not with memory or perceptual speed. T2D was associated with reduced nocturnal central systolic BP dipping (β=–3.79, p = 0.027), but not with BP, aortic stiffness, cerebral perfusion, or other hemodynamic measures. There was a statistically significant interaction between T2D and central systolic BP dipping in predicting attention scores (both p < 0.05 for the interaction term) whereby there was a positive association between BP dipping and attention scores in those with T2D, but not in those without T2D.
Conclusion:
We found an association between T2D and reduced nocturnal central systolic dipping, but not with any other measures of BP, stiffness or hemodynamic measures. Further study of the role of nocturnal central BP dipping in the association between T2D and cognitive impairment may help identify potential mechanisms.
Keywords
INTRODUCTION
Type 2 diabetes mellitus (T2D) is associated with an increased risk of dementia [1], but the mechanisms underlying this association are poorly understood. T2D is associated with hypertension and central (aortic) and peripheral artery disease [2]. Prior evidence suggests that blood pressure (BP) modifies the risk of dementia in those with T2D [3–6], but the mechanisms underlying this are not clear.
T2D and hypertension are associated with aortic stiffness [2, 7] which may result in excessive systolic pulsatile pressures damaging the blood-brain barrier [8], potentially leading to neuronal injury cell death [7, 9]. Furthermore, stiffening of the aorta seen in T2D and hypertension affects aortic (central) hemodynamics, and specifically reduces reservoir function of the aorta [10], which refers to the ability of the aorta to act as a reservoir, enabling it to maintain an even flow of blood to the peripheral circulation even during diastolic filling [11]. Impaired reservoir function could thus result in reduced cerebral perfusion, due to reduced flow during diastole. In addition, the loss of a cushioning effect by the aorta may lead to the peripheral transmission of the high pressures generated during cardiac systole, and thus may further damage the blood-brain barrier [8].
Another hemodynamic variable, nocturnal BP dipping, has been linked to the presence of cognitive impairment [12, 13]. In normal adult human physiology, both systolic BP (SBP) and diastolic BP (DBP) drop 10 to 20% during sleep [13]. In T2D, this nocturnal BP dipping is reduced or absent [14, 15], resulting in a greater risk of cardiovascular events [13]. An association between reduced dipping and cognitive impairment may occur through exposure of the cerebral microvasculature to higher pulsatile flow for longer periods of time.
To our knowledge, the relationships between BP, aortic stiffness, central hemodynamics, and BP dipping on brain perfusion, structure, and function have not been studied in the context of T2D. We aimed to study these relationships in a sample of twins discordant for T2D. We hypothesized that T2D would be associated with increased BP and aortic stiffness, poorer aortic reservoir function, and reduced nocturnal BP dipping, and that these associations would mediate or modify the association between T2D and brain health (cognition, brain perfusion, and structure).
METHODS
Sample
The sample was derived from the Australian Twin Registry (ATR), a national registry of over 30,000 volunteer twins. To be eligible, twin pairs had to be discordant for T2D, aged≥50 years, with one twin having T2D confirmed by a physician and validated with fasting glucose level≥7.0 mmol/L (≥126 mg/dL), and their co-twin without T2D having a fasting glucose level of < 7.0 mmol/L (<126 mg/dL). Exclusion criteria were a history of significant neurological disease (seizures, dementia, Parkinson’s disease, severe head trauma), those with insufficient English language ability for cognitive testing, or contraindication to magnetic resonance imaging (MRI). The sampling frame consisted of 90 twin pairs identified as being discordant for T2D, some of whom had participated in our previous study of brain activation [16]. Those twin pairs with T2D discordance were mailed an invitation to participate in the study. Zygosity was ascertained using standard responses to questions shown to have 95% accuracy for that purpose [17]. This study was approved by the Monash University Human Research Ethics Committee and the Monash Health Human Research Ethics Committee.
Hemodynamic measures
Hemodynamic measures were collected using the Mobil-o-Graph device which incorporates a standard oscillometric cuff BP device, as well as estimation of central aortic BP by pressure waveform analysis [18, 19], a method with an accuracy for estimating central systolic BP within 3 mmHg (SD 6 mmHg) [20]. This device has been specifically validated in those with T2D by comparing to invasive methods [20]. The cuff was applied to the left arm for 24 hours and participants were advised to continue their usual daily activities. The device was configured to record brachial mean arterial pressure (MAP) and pulse waveform every 15 minutes during daytime, and every 30 minutes at night.
Pressure waveform analysis was used to derive central SBP, central DBP, estimated aortic pulse wave velocity (PWV), and the augmentation index. Central pulse pressure (PP) was also derived by subtracting central DBP from central SBP. The augmentation index (augmentation pressure adjusted for pulse pressure) is considered to be a measure of the total effect of wave reflection [21, 22] and reflects arterial stiffness in addition to other factors such as branching and tapering of the arteries, and body size [22]. Augmentation index has previously been associated with cardiovascular events, myocardial hypertrophy, heart failure, and mortality [22, 23].
Aortic reservoir function [reservoir pressure (pReservoir) and excess pressure (pExcess)] was measured using the algorithm developed by Parker [10]. Reservoir pressure is defined as the pressure required to fill the aortic reservoir, whereas pExcess is defined as the pressure difference when the reservoir pressure is subtracted from the overall pressure waveform, and represents excess work performed by the left ventricle during systole [28].
The degree of nocturnal dipping of central and peripheral SBP was calculated as a percentage of mean BP reduction at night time (0100 to 0600 hours) compared with daytime (1000 to 2100 hours) and expressed as a percentage.
Diastolic dipping was calculated in the same manner. These time periods were chosen to maximize the likelihood that a participant would be asleep at the time of night measurements, and awake during times of day measurement, regardless of personal lifestyle.
MRI acquisition
MRI scans were obtained using a single 3T Siemens Magnetom Skyra scanner (Siemens, Erlangen, Germany). The following structural imaging sequences and parameters were used: T1: repetition time (TR) = 1900 ms, echo time (TE) = 2.43 ms, flip angle = 9°, field of view (FOV) = 240 mm, 192×192 matrix, and slice thickness = 0.6 mm; Fluid attenuated inversion recovery (FLAIR): TR = 9000 ms, TE = 81 ms, flip angle = 150°, FOV = 220 mm, acquisition matrix 320x217, and slice thickness = 4 mm. We used pulsed arterial spin labelling (PASL) to measure cerebral perfusion using QUIPSS II (quantitative imaging of perfusion using a single subtraction) with parameters: TR = 2500 ms, TE = 11 ms, FOV = 192 mm, matrix 64x64, tag thickness 10 cm, proximal slice gap 22.1 mm, bolus duration = 700 ms, inversion time = 1800 ms, and slice thickness = 6 mm. QUIPSS II is a PASL based technique designed to make the sequence less prone to transit-time error [24].
Image processing
Tissue classification was performed using FreeSurfer 5.3 to derive brain volumes and white matter hyperintensity (WMH volume). FreeSurfer removes non-brain tissue using a hybrid deformation procedure [25]. It performs automated Talairach transformation, segmentation of the subcortical white matter and deep gray matter volumetric structures [26], intensity normalization [27], tessellation of the gray matter white matter boundary, automated topology correction [28, 29], and surface deformation following intensity gradients to optimally place the gray/white and gray/cerebrospinal fluid borders at the location of the greatest shift in signal intensity [30–32].
ASL and FLAIR images were first aligned with the T1-weighted using the co-registration facility in the Statistical Parametric Mapping (SPM12) software, Wellcome Trust Centre for Neuroimaging. Co-registration between ASL and T1 is needed to calculate mean signal for each lobe, whereas co-registration between FLAIR and T1 is required to identify WMH. Global cerebral blood flow (CBF, in ml/min/100 g brain tissue) was estimated from the ASL images using BASIL (Bayesian Inference for Arterial Spin Labelling) [33] from the FSL package. A nonlinear transformation to standard MNI space was estimated using the SPM12 unified segmentation procedure applied to the T1-weighted images and used to transform CBF images to standard space for voxel-wise statistics. A lobe-based parcellation was also produced and mean CBF was computed for each lobe using the FreeSurfer output (https://surfer.nmr.harvard.edu/fswiki/CorticalParcellation).
Cognitive measures
Cognitive tests were conducted to examine several domains of cognitive function. These included the Hopkins Verbal Learning Test (verbal memory) [34], Rey-Osterrieth Complex Figure Test copy (visuospatial, perceptual function, organization) and delay (visual memory) [34], and components of the Cambridge Neuropsychological Test Automated Test Battery (CANTAB) including paired associate learning (PAL, episodic memory, and learning), and simple reaction time (SRT, speed) [35]. Also included were components from the Wechsler Memory Scale 3rd version (WMS-III) including mental control (maintaining mental set), digit span forwards (simple attention) and backwards (working memory) [36]. The National Adult Reading Test (NART) was conducted to assess premorbid intelligence [37].
Other measurements
Demographic information and medical history including cardiovascular factors (hypertension, hyperlipidemia, stroke, coronary artery disease), diabetes complications, medication use, and age of diabetes onset were recorded using a standardized, structured questionnaire. Height, weight, waist and hip circumference were measured. Two readings were taken for each measurement, and if there was a difference of 2 cm or more between these two readings, a third was performed, and the average of the measurements was used. Body mass index (BMI) and waist-hip ratio (WHR) were then calculated. Blood samples were analyzed for fasting glucose, HbA1c, and insulin levels. A Beckman Coulter DXC800 Analyzer was used to determine glucose concentration using oxygen rate method utilizing a glucose oxygen electrode (Beckman Coulter, Inc, Indianapolis, IN, USA) and HbA1c was measured using an ADAMS ARKRAY Glycohemoglobin Analyzer HA8160 (ARKRAY, Inc, Kyoto, Japan). Serum insulin levels were measured using the immune-enzymatic Access/DXI Ultrasensitive Insulin assay (Beckman Coulter, Inc, Indianapolis, IN, USA) and insulin resistance was calculated using the Homeostatic Model Assessment (HOMA2) method [38].
Statistical analyses
Similar to our previous work [39], neuropsychological test scores were subjected to data reduction using confirmatory factor analysis, yielding three factors. Based on loading of tests, the factors represented the cognitive domains of attention, memory, and perceptual speed (Supplementary Table 1). Factor scores were developed for individuals in each factor using Thomson’s method [40], which were then used in subsequent analyses.
McNemar’s test and paired t-tests were used to compare categorical and continuous characteristics between discordant twin pairs. Linear mixed level modelling was used to examine the relationships between T2D, hemodynamic variables, and brain variables. In these models, a unique twin pair identification code was entered as a random effect, so that the model incorporated both within-pair comparisons and between-pair comparisons and allowed the incorporation of covariates such as age and sex, along with primary variables of interest (T2D, BP, and hemodynamic measures) into the model.
To examine whether BP and hemodynamic measures mediated the associations detected between T2D and the brain outcomes (perfusion, brain structure, cognition), we added terms for hemodynamic measures that were associated with T2D into the models relating T2DM to relevant outcomes, adjusting for age and sex. As with our previous work [41], if the hemodynamic measure introduced substantially attenuated the β coefficient for T2DM and the coefficient of the brain outcome measure remained unchanged from its unadjusted value without T2D in the model, it was to be considered a potential mediator. Two-way interactions were also planned using a test of significance of product terms to assess effect modification. Standard regression diagnostics were conducted to assess the adequacy of models. A p value of < 0.05 was used as a threshold for statistical significance. Stata statistical package software (version 13.0, StataCorp, College Station, TX, USA) was used for these analyses.
RESULTS
Sample
Of the 90 twin pairs approached between April 2015 and May 2016, there were 10 pairs in which at least one twin did not respond, 45 pairs in which at least one twin declined to participate, and 9 pairs who agreed to participate but were unable to meet the logistical requirements to attend all study assessments. Thus 26/90 pairs (11 pairs from our previous sample and 15 new pairs) were enrolled and underwent all measurements, a recruitment rate of 32%. Two pairs were subsequently excluded because both twins in both pairs were found to have T2D based on fasting glucose levels. A further pair was excluded due to failure of one of the twins to attend assessment, leaving 23 pairs (12 dizygotic pairs, 11 monozygotic pairs) with data available for analysis.
The mean age of the sample was 63.7 years (SD 6.1), with mean duration of T2D of 10.7 years (SD 11) in affected individuals (Table 1). Compared with their unaffected co-twins, those with T2D had a significantly greater HbA1c, fasting glucose, BMI, and WHR, were more likely to report of a history of hyperlipidemia and myocardial infarction, and more likely to be on BP lowering medications, and oral hypoglycemic agents (all p < 0.05). All individuals without T2D had fasting glucose < 7.0 mmol/L but eight of these individuals had a fasting glucose > 5.5 mmol/L, consistent with impaired glucose tolerance. Central SBP dipping was the only detectable difference in hemodynamic variables (using paired comparisons; Table 2).
Sample characteristics
p-values derived using paired t-tests or McNemar’s test.
Blood pressure, aortic stiffness, and hemodynamic measures using paired t tests
SD, standard deviation, SBP, systolic blood pressure, DBP, diastolic blood pressure, BP, blood pressure, PP, pulse pressure.
Associations between T2D and hemodynamic measures
T2D was negatively associated with nocturnal dipping of central SBP in univariable analysis (β=–3.96, 95% CI –7.28 to –0.65, p = 0.019) and following adjustment for age and sex (β=–3.79, 95% CI –7.15 to –0.42, p = 0.027; Table 3). Sex was not associated with nocturnal central SBP dipping. There were no other detectable associations between T2D and other BP, stiffness, hemodynamic measures, or with global cerebral perfusion (Table 3). In a sub-group analysis by zygosity, the association between T2D and nocturnal dipping of SBP was stronger among dizygotic pairs (β=–4.88, p = 0.006) than among monozygotic pairs β=–2.96, p = 0.34). Otherwise, the associations for other hemodynamic variables by zygosity were not different in magnitude compared with the whole sample.
Associations between T2D and hemodynamic measures
SBP, systolic blood pressure, DBP, diastolic blood pressure, PP, pulse pressure.
Associations between T2D and cognition
T2D was associated with poorer attention scores (β=–0.45, 95% CI –0.68 to 0.21, p < 0.001) independent of age and sex, but not with memory (β=–0.31, 95% CI –0.68 to 0.056, p = 0.10) or perceptual speed (β=–0.20 95% CI –0.52 to 0.12, p = 0.22). Addition of education level into these models did not change the associations, which were similar in magnitude in both monozygotic and dizygotic subgroups.
Associations between hemodynamic measures and cerebral perfusion
Adjusting for age and sex, there was a negative association between peak excess pressure and global CBF (β=–0.78, 95% CI –0.15 to 0.03, p = 0.043) and between central SBP and global CBF (β=–0.19, 95% CI –0.44 to 0.05, p = 0.013; Table 4). There were no detectable associations between any of the other BP, hemodynamic, or stiffness variables and cerebral perfusion.
Associations between hemodynamic measures and global cerebral perfusion
SBP, systolic blood pressure, DBP, diastolic blood pressure, BP, blood pressure, PP, pulse pressure.
Associations of hemodynamic measures with cognition and brain structure
Higher aortic reservoir pressure (β= 0.02, 95% CI 0.01 to 0.04, p = 0.01) was associated with better attention score, wider central pulse pressure was associated with better memory score (β= 0.02, 95% CI 0.01 to 0.05, p = 0.02), and wider peripheral PP was associated with poorer perceptual speed (β=–0.03, 95% CI –0.05 to –0.01, p = 0.03), independent of age and sex (Supplementary Table 2). We were unable to detect any other associations between other central or peripheral hemodynamic variables and cognition. Wider peripheral PP was associated with lower total brain volume (β=–2108, 95% CI –3822 to –395, p = 0.016,
Moderation and interactions
There was a statistically significant interaction between T2D and nocturnal dipping of central SBP in predicting attention scores (β= 0.031, 95% CI 0.0066 to 0.055, p = 0.013 for the interaction term) whereby in those with T2D, reduced nocturnal BP dipping was associated with poorer attention scores but not in those without T2D (Fig. 1). There was also a similar interaction between T2D and dipping of peripheral SBP in predicting attention scores (β= 0.034, 95% CI 0.0065 to 0.061, p = 0.015 for the interaction term) whereby there was a positive association between BP dipping and attention scores in those with T2D, but not in those without T2D. However, no other interactions were detected between T2D and hemodynamic variables in predicting cognitive domain scores.
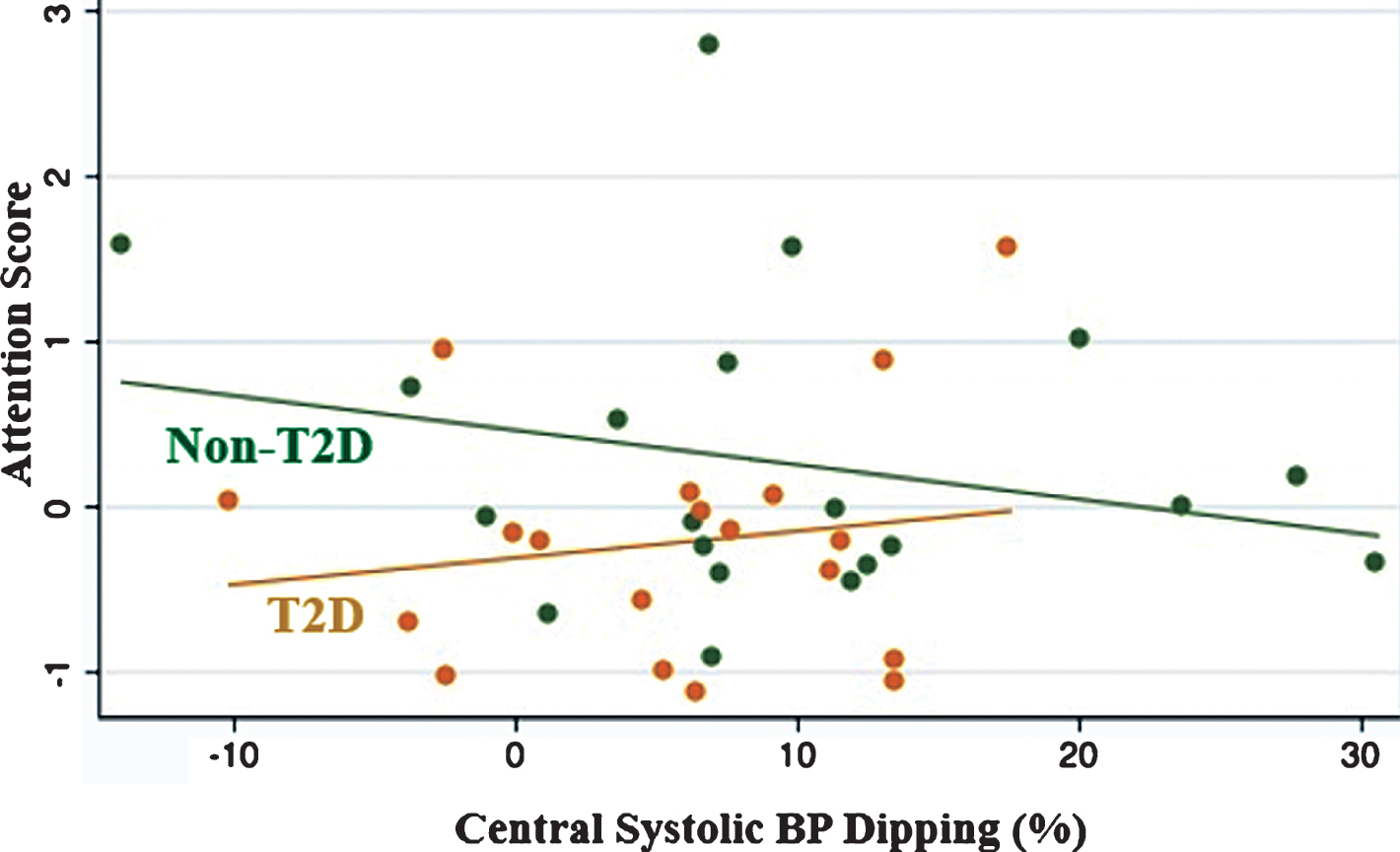
Interaction between T2D and central systolic dipping in explaining attention scores.
DISCUSSION
In this discordant twin sample, we found that T2D was associated with reduced nocturnal BP dipping, but not other hemodynamic measures. We also detected a modifying effect of nocturnal SBP dipping on the association between T2D and attentional ability, raising interesting speculation about underlying biological explanations and the potential for impaired nocturnal BP dipping as a mediator of cognitive dysfunction in T2D. Additionally, we identified associations of some BP and hemodynamic measures with cognition and total brain volume, and associations of excess pressure and central SBP with cerebral perfusion.
One interesting finding in our study was the interaction between T2D and nocturnal SBP dipping in predicting cognition, specifically attentional ability. T2D is known to be associated with reduced nocturnal dipping [14, 15]. One explanation for impaired dipping in T2D may be the presence of co-existent sleep apnea, which is known to be associated with nocturnal hypertension [14]. However, we were unable to investigate this issue as we did not have measures of sleep apnea. Alternatively, reduction in dipping may be the result of increased sympathetic nervous system activation during sleep [42], but salt sensitivity, reduced renal salt excretion, corticosteroid levels, leptin, insulin resistance, and endothelial dysfunction all may have a role [43]. Reduced nocturnal BP dipping has been associated with poorer cognition previously in people without T2D [44–46], but to our knowledge, not in the context of T2D. Others have previously raised the possibility that impaired dipping could be mechanistically related to target organ damage, including the brain [13]. It could be hypothesized that reduced nocturnal BP dipping is indicative of microvascular dysfunction, which could lead to impaired blood-brain barrier function, neuronal damage, and reduced cognition over time. T2D is also associated with microvascular dysfunction and thus may amplify the effect of impaired dipping on cognition. This interaction between nocturnal BP dipping and T2D on cognition and deserves exploration and replication in future larger and longitudinal studies. An interesting finding in sub-group analysis by zygosity showed a stronger relationship between T2D and nocturnal dipping among dizygotic pairs than among monozygotic pairs. Although this raises speculation that genes may have a strong contribution to this association, these findings must be regarded as hypothesis-generating given the small size of the subgroups. Similarly, the lack of differences by zygosity in analyses of T2D against other hemodynamic variables or cognition may also be due to the small subgroup samples.
Apart from the interaction between T2D and nocturnal BP dipping, we did not uncover associations of T2D with other hemodynamic variables. This is in contrast to several studies of T2D in which central BP and aortic stiffness were examined [15, 47–49]. In a sample of 37 people with T2D (mean age 63 years), compared to 37 people without T2D (mean age 52 years), we previously reported that T2D was associated with higher central and peripheral SBP, as well as higher excess and reservoir pressure [15]. Similarly, Cakar et al., found that in 20 people with T2D (mean age 40 years) compared to 17 healthy controls (mean age 48 years), those with T2D had increased aortic PWV, and central and brachial BP [48]. Kozakova et al. similarly found that aortic PWV, carotid artery BP, and LV mass were higher in those with T2D (n = 125) compared to healthy volunteers (n = 101, whole sample mean age 57.5 years) [49] However, Scott et al. found that there was no difference in central BP between 73 people with T2D and 73 healthy volunteers at rest (mean age 53.5 years), but that those with T2D were more likely to have an exaggerated central BP response to aerobic exercise [47].
There are several possible reasons why we did not detect similar associations between T2D and BP, aortic stiffness, and hemodynamic measures. The method we utilized is a validated non-invasive cuff-based method to measure central BP and the aforementioned studies incorporated a similar method [48], or a tonometric method [15, 49]; methods found to be similar when compared to oscillometry [19]. Furthermore, such methods have been specifically validated by comparing to invasive methods in those with T2D [50]. Although it is not possible to validate ambulatory methods against invasive methods, ambulatory central BP has been shown to outperform conventional ambulatory BP [51]. Therefore, the validity of these measurements does not likely explain the lack of associations observed. However, one exception is that the Mobil-o-Graph may underestimate PWV compared with carotid-femoral waveform assessment, the gold standard technique [52]. A potential explanation for our inability to detect associations between T2D and BP and hemodynamic measures may be the effective use of BP reducing medications (mean defined daily dose of antihypertensive medication in T2D group = 1.9 compared to 0.8 in control, p = 0.002), and the relatively tight glycemic control (mean HbA1c = 7.1% in T2D group) in a high proportion of our sample with T2D, thus minimizing any disease-related differences in BP. Finally, the relatively small size of our sample may have also further reduced our chances of uncovering associations, even though our discordant twin study design provides tight control of important confounders.
There were few associations between BP, aortic stiffness, and hemodynamics and cognition in our study. Higher reservoir pressure was associated with higher attention score, and wider central PP was associated with higher memory score, whilst wider peripheral PP was associated with poorer perceptual speed score. Regarding the association between reservoir pressure and attention, Climie et al. previously studied a sample of people with T2D and healthy controls, and found that higher excess pressure, but not reservoir pressure, was associated with lower grey matter volume in people with T2D [15]. There have been no other studies examining the role of excess pressure or reservoir pressure in cognitive impairment in T2D. The aortic pressure waveform can be divided into excess pressure and reservoir pressure with excess pressure representing excess work performed by the left ventricle, whereas reservoir pressure indicates the pressure required to fill the physiologic reservoir [53]. Therefore, a higher reservoir pressure, as opposed to excess pressure, may be indicative of more efficient reservoir function. Such efficient reservoir physiology might represent reduced arterial stiffness, which could adversely affect the brain. Therefore, this may explain the association seen between reservoir pressure and attention. Surprisingly, wider central PP was associated with higher memory score in our study. Although PP is considered a marker of arterial stiffness, the gold standard measure is PWV [54], which was not associated with memory score in our study.
Except for an inverse association between peripheral PP and total brain volume, we did not find any associations between other measures of aortic stiffness, central hemodynamics, or BP dipping with total or regional brain volumes. We did however find that higher central SBP and higher excess pressure were associated with lower cerebral perfusion, but neither were associated with T2D in our sample. Hence, we were unable to establish mediation. Detailed studies of the links between central hemodynamics and cerebral perfusion or brain structure are lacking. The relationship between aortic stiffness and cerebral perfusion has been examined previously in only two studies, and none in the context of T2D. In one study, athletes had lower PWV and greater occipitoparietal blood flow, as assessed by ASL, than sedentary individuals and there was a statistically significant correlation between PWV and occipitoparietal blood flow [55]. In another study, people with T1D (mean age 46 years, n = 51) were compared to those without T1D (mean age 44 years, n = 34) [56]. In that study, T1D was associated with lesser grey and white matter volume and greater CBF, while both PWV and CBF were independently associated with white matter volume in those with T1D only [56]. Associations between PWV and CBF were not examined [56].
The strengths of our study are its discordant twin pair design, careful phenotyping of T2D, and comprehensive measures of BP, hemodynamics, cognition, and structural imaging. One limitation is our relatively small sample size, and another is that our T2D sample had relatively well-controlled T2D and were more likely to be on protective therapies than those without T2D, thus restricting our ability to detect small effects. This limitation is somewhat offset by the potential increased sensitivity of this study design to detect small effects. It is also recognized that a person who has a co-twin with T2D is at a high risk of developing T2D in the future and therefore may not be considered to be a true “control”. Indeed, some participants without T2D had fasting glucose levels consistent with pre-diabetes which has the potential to reduce our ability to detect within-pair differences. However, this may be considered a strength as it allows for isolation of the effect of T2D from other factors associated with T2D such as impaired fasting glucose, hypertension, and obesity, and early age lifestyle exposures. Furthermore, we did not apply a correction for multiple hypotheses, which increases the likelihood of false positive results. However, our hypotheses were pre-specified. Additionally, this is a cross-sectional study which is susceptible to potential information bias such as that which can result from self-reporting questionnaires, and furthermore causation cannot be inferred in any associations found. Finally, our recruitment rate was only 32%, and many of the included twins had participated in our twin previous study [16], which may have caused sampling bias, since such individuals may differ from the remaining eligible study sample in characteristics such as health literacy and participation.
Conclusions
The potential role of nocturnal central BP dipping in explaining the association between T2D and cognitive dysfunction requires further confirmation in larger, longitudinal studies, with exploration of potential underlying mechanisms such as sleep apnea.