
Abstract
Behavioral and cognitive variables predicting behavioral frontotemporal dementia (bvFTD) versus primary psychiatric disorders mimicking bvFTD (phenocopy syndrome: bvFTD-PS) were studied. Forty-one probable/definite bvFTD and 16 bvFTD-PS patients were evaluated with cognitive battery, Neuropsychiatric Inventory, and Stereotypic and Ritualistic Behavior-revised questionnaires. Twenty-seven healthy subjects served as control. Severity of cognitive impairment/behavioral symptoms and profile of cognitive deficits were similar, with bvFTD-PS showing impaired executive abilities and memory. However, phonemic fluency was impaired only in bvFTD (p < 0.001). Depression was worse in bvFTD-PS, while apathy, disinhibition, and dietary changes characterized bvFTD. Phonemic fluency and depression accounted for the best predictive diagnostic model. A structured psychiatric screening of bvFTD mimickers may often yield a psychiatric diagnosis with predominant depressive symptoms and therefore a potentially treatable condition.
INTRODUCTION
Phenocopy syndrome of behavioral frontotemporal dementia (bvFTD-PS) is a condition sharing the clinical characteristics of neurodegenerative bvFTD. Patients with phenocopy may be diagnosed as possible bvFTD according to Rascovsky criteria, with early presentation of personality changes, loss of empathy, and executive deficits [1, 2]. However, they have no evidence of frontotemporal atrophy or glucose hypometabolism, and do not develop functional impairment over 1-2 years [2]. Most patients with bvFTD-PS will receive a diagnosis of primary psychiatric disorder: bipolar spectrum disorder, unipolar depression, personality or anxiety disorders [3]. In few cases, phenocopy patients present a benign form of bvFTD with long lasting preservation of functional performance and minimal brain atrophic/metabolic changes [2]. A recent systematic review on this topic summarizes the main clinical differences of these two conditions and underlines the open issue whether bvFTD-PS is a separate entity or belongs to the bvFTD-spectrum [4]. Although the differential diagnosis is challenging, accurate identification of bvFTD-PS is crucial since it implies different therapeutic and prognostic choices [3]. Diagnosis of bvFTD-PS implies costly investigations (often both MRI and PET) and a wait-and-see approach with follow-up assessments documenting stability or even improvement of functional abilities, a main determinant of non-neurodegenerative condition. Few studies have been carried out to determine whether bvFTD-PS could be distinguished from bvFTD at first assessments on a clinical ground. bvFTD-PS has been described with lower compulsivity and more severe depressive symptoms; cognitive differences, mainly in the executive domain, were not consistently detected [2, 5].
We investigated behavioral and cognitive profiles of psychiatric bvFTD-PS and bvFTD patients, aiming at identifying which variables could be predictors of bvFTD-PS diagnosis.
METHODS
Eighty-four subjects were recruited and divided in three groups: 41 with probable/definite bvFTD, 16 with bvFTD-PS, and 27 age-matched healthy controls (HC). Patients were recruited at the outpatient memory clinic at the Department of Neurosciences in Padua (Italy) between 2011 and 2018. Initial inclusion criteria were a diagnosis of possible bvFTD [1], Mini-Mental State Examination (MMSE) score ≥15/30 and severity of language deficit or behavioral disturbances not interfering with the neuropsychological assessment. Exclusion criteria were the presence of a previous diagnosis of primary psychiatric disorders assessed with review of medical charts or through the National Health system database, systemic or brain diseases responsible of behavioral/cognitive alterations, a past history of head injury and diagnosis of other neurodegenerative diseases. HC subjects were recruited from participants of programs of community based social engaging activities among subjects with MMSE ≥27/30.
Patients underwent a diagnostic work-up including a multidisciplinary assessment with neurologist and psychiatrist, brain MRI/CT (n = 55/2) and FDG-PET (n = 57), genetic testing for pathogenic mutations associated with FTD. Follow-up assessments were available in all patients for a minimum of sixteen months (bvFTD; mean 33±13, range 5–16 months; bvFTD-PS: 35±12, range 16–49 months). After the diagnostic work-up, patients received a diagnosis of bvFTD: 35 probable and 6 definite (5 c9orf72 and 1 progranulin mutations) [1], or bvFTD-PS (n = 17) following the definition by Kipps and collaborators (lack of functional decline and normal neuroimaging) [2]. As regard as FDG-PET findings, PET scans were evaluated by a nuclear medicine expert, aware of the working hypothesis of frontal lobe syndrome. PET scans of patients classified with bvFTD were clearly unambiguous, showing predominantly dorso-lateral, ventro-lateral, and mesial frontal lobe involvement. In two patients, the glucose hypometabolism was located in the bilateral temporal poles. In 4 cases, fronto-parietal hypometabolism was associated with detection of gene mutations (c9orf72).
In the bvFTD-PS group, brain PET-FDG study was clearly unremarkable in 11/16 cases. In the other 6 patients, a mild/doubtful hypometabolism was found restricted to part of the anterior cingulate cortex (n = 3), in the superior temporal gyrus (n = 1), and in the temporo-parietal regions (n = 2). Although these PET scans were qualitative evaluated in the normal range of variation, a regional semiquantitative analysis of FDG-SUV values was run and compared data with those of a reference normal population. In all cases, the individual regional metabolism was within 2 standard deviations from normal distribution. Although subtle changes were found, we classified this pattern of glucose metabolism as normal.
Patients with diagnosis of suspected bvFTD-PS underwent psychiatric evaluation to determine if a DSM-5 diagnosis was achievable guided by the Mini-International Neuropsychiatric Interview [6]. bvFTD-PS patients received the following psychiatric diagnoses: bipolar disorder (BD) (n = 8:6 type II and 2 type I), unipolar depressive disorder (n = 2), temperamental traits/personality disorder (n = 4:3 cluster B and 1 cluster A), generalized anxiety disorder (n = 2), no psychiatric diagnosis identified (n = 1). The patient without a diagnosis of primary psychiatric disease carried a diagnosis of bvFTD-PS (no functional impairment, no cognitive decline in a follow-up of three year, and normal MRI and brain glucose metabolism) but was excluded from the study to maintain the diagnostic homogeneity of the other 16 bvFTD-PS patients, which represented our final sample.
Behavioral disorders were assessed with the Neuropsychiatric Inventory (NPI) questionnaire. Stereotypies and repetitive behaviors were evaluated with the Stereotypic and Ritualistic Behavior-revised (SRB-r), a questionnaire on frequency and severity of simple motor stereotypies, verbal stereotypies, verbal perseverations, clock watching, counting, hoarding, routines/rituals, fixed leisure activities, and recurrent eating behaviors [7].
The neuropsychological assessment included: MMSE, digit cancellation test [8], and Trail Making Test A (TMT-A) for visual attention; digit span forward and backward for short-term and working memory; prose memory test [9], and Rey Auditory Verbal Learning Test (RAVLT) for episodic memory [10]; verbal fluency for lexical access and executive functioning [9]; Frontal Assessment Battery (FAB) for executive functions [11]; clock drawing test for visual-constructional abilities; Rey-Osterrieth Complex Figure (ROCF) for the assessment of visual-constructional abilities (copy) and long-term visual-spatial memory (delayed recall) [12]. HC underwent a shorter cognitive evaluation, including digit span forward and backward, TMT-A, clock test, verbal and semantic fluency, and RAVLT.
Data were analyzed with the IBM Statistical Package for Social Science (SPSS 22.0). ANOVA was run to compare the performances of bvFTD, bvFTD-PS, and HC, while Student t-test was used to compare bvFTD and bvFTD-PS.
Backward stepwise logistic regressions were used in order to predict the probability that an observation falls into bvFTD or bvFTD-PS categories based on behavioral and cognitive measures.
Local ethics committee approved the study. All participants gave written informed consent.
RESULTS
Demographic and clinical characteristics are summarized in Table 1. The bvFTD-PS and bvFTD groups were comparable for age, sex distribution, education level, age of onset of behavioral disturbances, symptoms duration, and degree of cognitive impairment (mean MMSE score: bvFTD-PS: 25.38±2.47, bvFTD: 23.93±3.96; p = 0.88). The HC group had higher mean age (72.5±3.7 years, p < 0.001), mean MMSE score (29.4±0.9; p < 0.001), and education level (15.4±3 years, p < 0.001) with respect to patients’ groups.
Demographic and clinical characteristics of the patients and healthy controls
p*, comparison between bvFTD and bvFTD-PS. bvFTD, behavioral variant frontotemporal dementia; bvFTD-PS, phenocopy syndrome of behavioral variant frontotemporal dementia; HC, healthy controls; MMSE, Mini-Mental State Examination.
Mean NPI and SRB-r total scores were not significantly different between groups (mean NPI-total score = bvFTD-PS: 23.88±14.35, bvFTD: 32.9±17.86; p = 0.079; mean SRB-r-total score = bvFTD-PS: 8.94±10.02, bvFTD: 15.94±14.19; p = 0.083) (Table 2). However, the bvFTD-PS group showed higher mean score for NPI-depression (p = 0.005), while bvFTD had higher mean scores for NPI-apathy (p = 0.02), NPI-disinhibition (p = 0.019), and NPI-dietary changes (p = 0.001) items. Moreover, the bvFTD group also showed more severe compulsive/repetitive behaviors at SRB-r eating and obsessive counting items (Table 1).
Comparison of NPI and SRB-r mean scores between bvFTD and bvFTD-PS
NPI, Neuropsychiatry Inventory questionnaire; SRB-r, Stereotypic and Ritualistic Behavior–revised questionnaire.
Cognitive tests scores and statistical differences corrected for MMSE scores are reported in Table 3. Both bvFTD-PS and bvFTD groups performed worse than HC subjects in tests assessing semantic fluency, episodic verbal memory, and visual-constructive abilities. bvFTD patients performed worse than bvFTD-PS in phonemic fluency, semantic fluency, immediate and delayed prose memory, and visuospatial memory. Deficits of executive functions and frontal lobe abilities were similar.
Distribution of cognitive variables between bvFTD, bvFTD-PS, and healthy controls (HC)
In the ANOVA, the following symbols are used: *significant differences (p < 0.001) between bvFTD and controls. §significant differences (p < 0.05) between bvFTD-PS and controls. For multiple comparisons (i.e., ANOVAs with the healthy control group) Bonferroni correction was applied in order to avoid Type I error. TMT-A, Trial Making Test; RAVLT, Rey Auditory Verbal Learning Test; ROCF, Rey-Osterrieth Complex Figure.
The differences emerged in the latter paragraph (see also Table 3) were further tested by using a logistic regression. The variables that were significantly different when comparing the two clinical groups were used as predictors. The analysis of significant behavioral variables showed that depression predicted the diagnosis of bvFTD-PS (OR = 0.67, p < 0.01), while apathy (OR = 1.27, p < 0.05) and dietary changes (OR = 1.29, p < 0.05) predicted the diagnosis of bvFTD. These predicting variables explained 51% of the variance (Nagelkerke R2, χ2 = 23.02, p < 0.001) with 80.4% of cases correctly classified. As for cognitive variables, worse verbal phonemic fluency predicted the diagnosis of bvFTD (OR = 0.91, p < 0.05), explaining 66% of the variance (Nagelkerke R2, χ2 = 15.21, p < 0.001) and correctly classifying 82.5% of cases.
The higher accuracy in discriminating between bvFTD-PS and bvFTD was obtained considering phonemic verbal fluency scores and depression severity (AUC: 0.80, CI: 0.66–0.94; AUC: 0.71, CI: 0.56–0.87, respectively; p < 0.05) (Fig. 1).
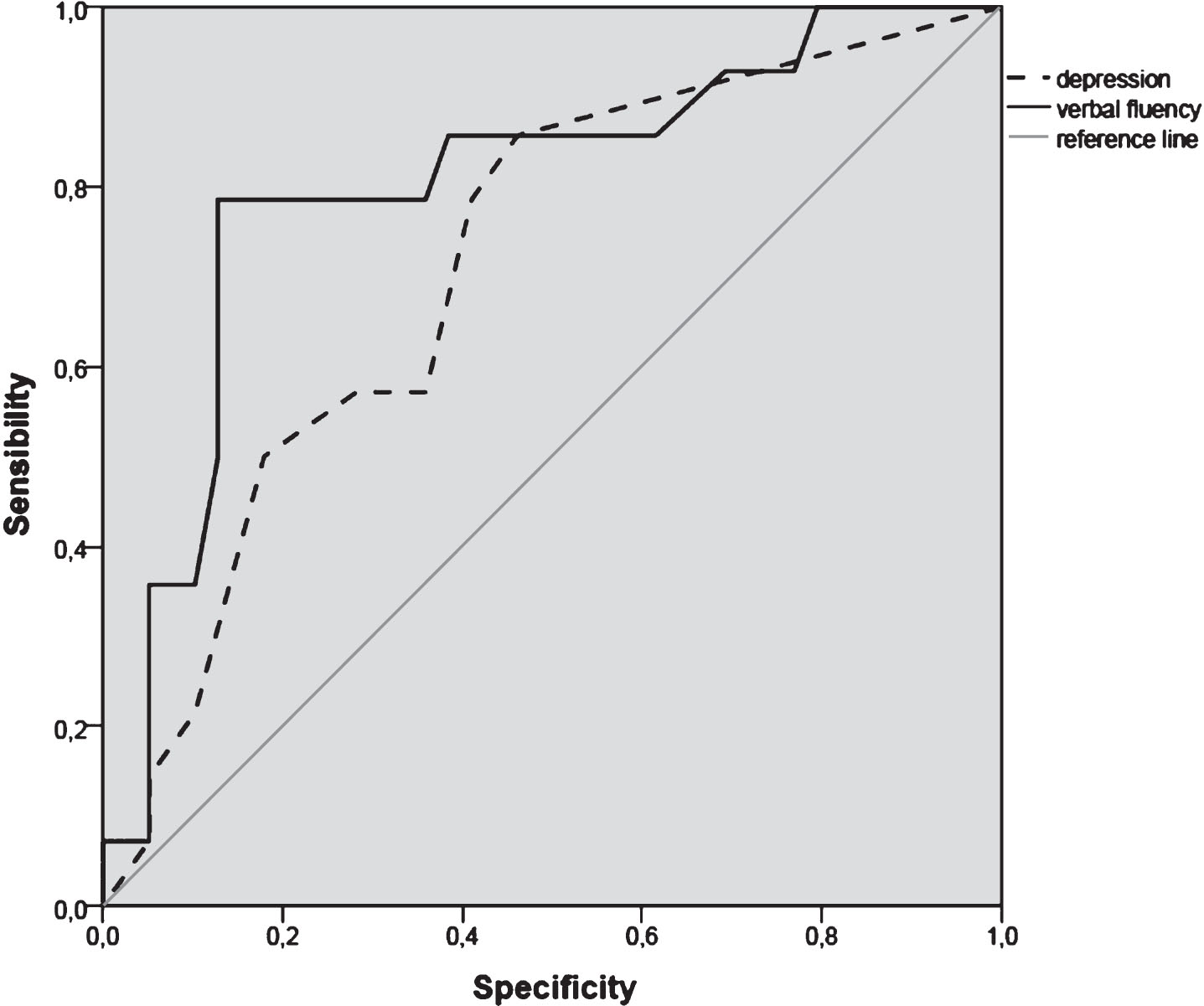
ROC curves of variables predicting bvFTD-PS versus bvFTD. Dot line represents accuracy of phonemic verbal fluency (AUC 0.80), and continue line represents the accuracy of depression (AUC 0.71).
DISCUSSION
Degree of cognitive impairment, profile of cognitive deficits, and severity of behavioral symptoms were similar in psychiatric bvFTD-PS and bvFTD. However, poor phonemic fluency, memory deficits, and typical behavioral features, i.e., apathy, disinhibition, and changes in dietary habits, were most frequent and severe in bvFTD. On the other hand, depression was worse in the bvFTD-PS group. Verbal fluency and depression could be used as predictors of the diagnosis of bvFTD-PS versus bvFTD.
Only a few studies compared neuropsychological and behavioral variables of bvFTD-PS and bvFTD. Vijverberg et al. studied the behavioral and cognitive variables predicting bvFTD versus late-onset primary psychiatric disorders presenting as bvFTD mimickers [5]. Patients with psychiatric disorders were predominantly male, had fewer stereotypies, and more severe depressive symptoms. These results replicated a previous study of the same group showing that male sex, low stereotypies, and severe depression explained 49% of the variance and correctly classified 82.1% of late-onset psychiatric patients [5, 13]. Similar results were also described by Hornberger et al., which found that presence of current depression was prevalent in the non-progressive form of possible bvFTD, while stereotypic speech was prevalent in the bvFTD [14]. We confirmed that less stereotypies and more frequent and severe depressive symptoms are typical of bvFTD-PS. In addition, we found that apathy, disinhibition, and specific compulsive features (dietary compulsive behavior and repetitive counting) were more specific of bvFTD. These findings are in line with some items in the recently proposed checklist aimed at identifying from clinical history bvFTD patients from patients with psychiatric late-onset frontal lobe syndrome [15]. The most informative questions include presence of repetitive behaviors, change in food habits, and language impairment.
Few and heterogeneous results have been published on cognitive predictors of bvFTD-PS versus bvFTD. Kipps described non-significant differences between the two groups [16]. Vijverberg et al. found that performances on frontal lobe tests, verbal fluency, memory and visual spatial abilities were similar in bvFTD-PS and bvFTD [5]. On the other hand, Hornberger et al. found a spared performance of executive tasks in phenocopies as opposed to predominant executive deficits with relative sparing of memory and visuospatial functions in bvFTD [17].
We did not confirm these previous findings showing an impairment of executive functions and episodic verbal memory in bvFTD-PS compared to controls, and also finding a few specific differences between bvFTD-PS and bvFTD which may help in the differential diagnosis.
Different types of bvFTD-PS patients across studies may in part explain these differences. In our study, the inclusion criteria for phenocopy syndrome required the diagnosis of possible bvFTD, including the presence of dysexecutive syndrome, in patients without a previous diagnosis of primary psychiatric disorders. Finally, the type of psychiatric diagnosis was unbalanced toward the spectrum of affective disorder, possibly characterizing the cognitive profile of this group.
The limitations of the study are the relatively small sample size for the bvFTD-PS group, the lack of neuropathological diagnosis for bvFTD-PS, the shorter cognitive evaluation, and absent behavioral assessment for the HC group. In addition, more specific cognitive markers of bvFTD, such as social cognition, were not considered. The strengths of our study are the possibility to compare the cognitive variables with normal controls, the long follow-up assessment, and the selection of a bvFTD-PS group with frontal lobe syndrome and new diagnosis of late-onset psychiatric disorder. This type of bvFTD phenocopy represents the most challenging set of patients entering in the differential diagnosis with bvFTD. In conclusion, results from this study suggest that 1) language impairment, mainly deficit of phonemic fluency, and compulsive behaviors/changes of dietary habits point toward a diagnosis of bvFTD; 2) a structured psychiatric screening of bvFTD-PS yields a psychiatric diagnosis in the vast majority of cases, mainly with depressive symptoms and potentially treatable diseases; and 3) a combination of poor phonemic fluency and high depressive symptoms yielded the best model toward a diagnosis of bvFTD respect to its psychiatric phenocopy syndrome.