
Abstract
Background:
Dementia is the leading cause of dependency and disability among older persons worldwide. There remains, however, limited studies on dementia rates within the Asia-Pacific region, with little data on differences across major Asian ethnic groups.
Objective:
To study the prevalence of cognitive impairment (CI) and dementia in community-dwelling Indians from Singapore and to examine interethnic differences among Chinese, Malays, and Indians.
Methods:
Participants (>60 years) drawn from the Indian component of the multiethnic Epidemiology of Dementia in Singapore (EDIS) study were screened using the locally validated Abbreviated Mental Test and Progressive Forgetfulness Questionnaire. Screen-positive participants underwent further detailed neuropsychological assessments. CI was classified into Cognitive impairment no dementia (CIND)-mild, CIND-moderate, and dementia.
Results:
Of 961 Indian adults, 120 (12.5%) had CIND-mild, 101 (10.5%) CIND-moderate, and 12 (1.2%) dementia. The overall age-standardized prevalence of any CI was 24.6%. The prevalence of any CI increased with age (15.7% in ages 60–64 years to 30.1% in ages≥80 years), and was higher in women than men. Multivariate analysis showed that age, lower education, and hypertension were independently associated with CI. Even after demographic and cardiovascular risk factor adjustment, Indians were more likely to be cognitively impaired compared to Chinese (odds ratio [OR], 95% CI:1.37 [1.01–1.86]) but not Malays (0.89 [0.72–1.10]).
Conclusions:
Among elderly Indians, the overall prevalence of any CI was 24.6%. Despite similar assessment protocols and risk factor adjustments, the prevalence of CI was higher in Indians compared to Chinese but similar to Malays. Further research is needed to unravel other factors that may underlie these ethnic differences.
INTRODUCTION
Dementia is a common age-related brain disease, and the leading cause of dependency and disability among older persons worldwide, with a global societal economic cost of US$ 604 billion [1–3]. An estimated 36 million people were diagnosed with dementia in 2010, a number expected to double every 20 years to 66 million by 2030 and 115 million by 2050 [4]. Asia, in particular, is estimated to have the largest increase in projected number of people with dementia, with its proportion of persons aged≥60 years to rise almost threefold by 2050 [5–7]. This increase is expected to have huge impacts on healthcare systems within Asia, and emphasizes the importance of dementia research within this region.
While there are limited studies on dementia rates within the Asia-pacific region [5, 8], recent focus has shifted to the identification of pre-clinical stages of dementia, cognitive impairment no dementia (CIND), as a potential optimum intervention stage to delay further disease progression [9, 10]. However, data on CIND has been largely performed in Caucasian populations, with a prevalence ranging from 5.1% to 33.3% [11, 12]. Recent studies have reported higher prevalence rates of cognitive impairment in Asians than in Caucasians, but evidence remains equivocal [12–16]. Moreover, it is difficult to make direct comparisons across populations and ethnicities, due to differences in methods of dementia ascertainment, demographics, environmental factors, and a lack of extensive neuropsychological testing [16–18].
The Epidemiology of Dementia in Singapore (EDIS) Study focuses on the prevalence and risk factors of dementia and cognitive impairment in Singapore. The Singapore population, comprises of 74.3% Chinese, 13.3% Malay, and 9.1% Indians [19], and offers a unique opportunity to study three major Asian ethnic groups sharing a common environment. We have previously published data on the Chinese and Malay components of EDIS, reporting an overall prevalence of cognitive impairment/dementia of 15.2% and 25.5%, respectively [16, 18]. Studies on the prevalence of cognitive impairment among Indians in Singapore and across Asia are lacking. Hence in the present study, we focused on the Indian component of the EDIS study and report on the prevalence of cognitive impairment and dementia in this ethnic group. We also examined the ethnic differences between Chinese, Malays, and Indians.
METHODS
Study design and study population
EDIS Study participants, aged 60–90 years, were drawn from the Singapore Epidemiology of Eye Disease (SEED) study, a population-based study among Chinese (Singapore Chinese Eye Study [SCES]), Malays (Singapore Malay Eye Study [SiMES-2]), and Indians (Singapore Indian Eye Study [SINDI-2]), details of which have been reported in detail elsewhere [20]. SINDI-2 participants formed the baseline for the Indian component of EDIS study, and were assessed from 2013 to 2015.
The EDIS Study comprises of two main phases, which have been described in detail for the Chinese and Malay components previously [16, 18]. Briefly, the first phase of the EDIS study involved a cognitive screen of all SINDI-2 Indian participants aged≥60 years (n = 1,128), comprising of the Abbreviated Mental Test (AMT), and a self-report of Progressive Forgetfulness questionnaire (PFQ) [21, 22]. Screen positives were defined as AMT score≤6 among those with≤6 years of formal education, or≤8 among those with > 6 years of formal education, or persons for whom the care-giver reported progressive forgetfulness. Those who were screen-negative were considered to be not cognitively impaired.
The second phase of the EDIS study involved only screen-positive participants, who were invited to undergo further neuropsychological assessment and brain magnetic resonance imaging (MRI). Figure 1 provides a summary of participant numbers and screening criteria of the two EDIS phases. Ethics approval for the EDIS study (protocol number EDS512) was obtained from the Singapore Eye Research Institute (SERI), and National Healthcare Group Domain-Specific Review Board (DSRB). The study is conducted in accordance with the declaration of Helsinki. Written informed consent was obtained in the preferred language of the participants prior to their recruitment into the study.
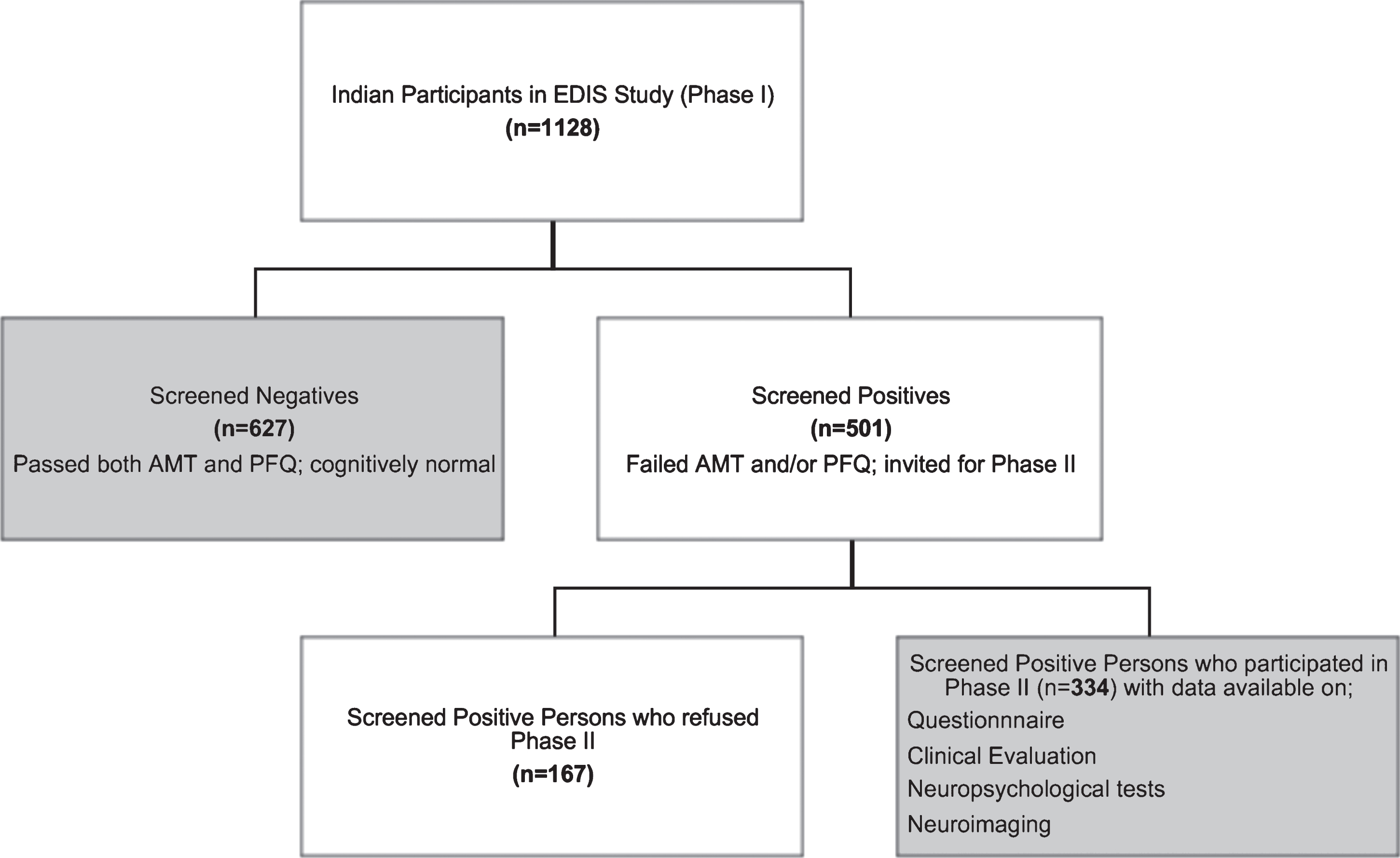
Flowchart of participants in the Indian component of the EDIS study. Boxes shaded in grey reflect the composition of our total baseline (n = 961).
Cognitive assessment
An extensive neuropsychological battery (previously validated in Singaporean elderly [23]) was administered to screen-positive participants in their preferred language, to fully determine their cognitive status. This battery comprised of seven (five non-memory and two memory) domain specific tests, namely (a) Executive Function, (b) Attention, (c) Language, (d) Visuomotor Speed, (e) Visuoconstruction, (f) Verbal Memory, and (g) Visual Memory. A modified 15-item Geriatric Depression Scale (GDS) was also administered to all persons [24]. Details on the battery have been reported previously [16, 18].
Diagnosis of CIND was based on impairment in at least one of the above domain of the neuropsychological test battery and no functional loss [25]. CIND was classified into mild when≤2 domains were impaired, and moderate when > 2 domains were impaired [26]. The diagnosis of dementia was made according to DSM-IV criteria, while dementia subtypes were defined in accordance with internationally accepted criteria: NINDS-ARDRA for Alzheimer’s disease and NINDS-AIREN for vascular dementia [27, 28].
Demographic and cardiovascular risk factor assessment
A detailed questionnaire was administered via personal interview to collect basic demographic information (age, gender, education, ethnicity, smoking, and socio-economic status) and medical history (including medications). Reported medical history of hypertension, hyperlipidemia, and diabetes mellitus was subsequently verified by medical records. A total of 20 ml of blood was drawn in the fasting state for blood tests that included glucose/glycated hemoglobin and lipid levels. Physical examination included height and weight. Systolic and diastolic blood pressures were measured twice using a digital automatic blood pressure monitor (OMRON-HEM 7203, Japan), five minutes apart, and the mean of the two readings was taken.
Risk factors were defined and assessed using standardized criteria. Hypertension was defined as systolic blood pressure≥140 mmHg and/or diastolic blood pressure≥90 mmHg or use of anti-hypertensive medication. Diabetes mellitus was defined as glycated hemoglobin≥6.5% or on anti-diabetic medication. Hyperlipidemia was defined as total cholesterol levels≥4.14 mmol/L (as per National Cholesterol Education Programme (NCEP) Adult Treatment Panel (ATP) III Guidelines) [29], or on anti-cholesterol/lipid medication. Education was categorized into≤6 years and > 6 years of Primary education. Smoking was categorized into non-smokers and smokers (past and current smokers). Alcohol consumption was categorized into current drinkers and non-drinkers. A low income was defined as a monthly income less than 2000 Singapore dollars per household. Housing was categorized into≤2 room public housing flats and≥3 room flat/condominium/private estates. Body mass index (BMI) was calculated as body weight (in kilograms) divided by the square of the height (in meters).
Genome-wide genotyping was performed using the Illumina Human610-Quad BeadChip with the 1000 Genomes (phase 1, version 3) reference panel used for imputation as described previously [16]. For persons with available genetic data, imputed data on two single nucleotide polymorphisms (SNP) [rs429358 and rs7412] was used to define apolipoprotein E (APOE) status.
Statistical analysis
Characteristics of study participants who agreed to participate in phase II were compared to those who refused phase II, using χ2 statistic for proportions of categorical variables, and a student t test for continuous variables. The Mann-Whitney U test was performed if a continuous variable (age) was not normally distributed. The baseline characteristics of SINDI-1 participants who returned for SINDI-2 follow up were also compared against those who did not return for follow up.
Crude and age-adjusted prevalence of cognitive impairment and dementia were computed for the whole cohort, and within strata of age and gender. Age-standardized rates were computed using the world standard population [25], and 95% confidence intervals (CI) were calculated assuming that the prevalence counts were Poisson distributed.
Multiple logistic regression models were used to examine the relationships between risk factors (demographic, cardiovascular, and genetic) and cognitive impairment/dementia. Model I included age, gender, and education. In Model II, all risk factors (age, gender, education, income, housing, diabetes mellitus, hyperlipidemia, hypertension, smoking, and BMI) were included in the same model to examine the independent associations of the risk factors with cognition. Odds ratio (OR) were reported with 95% CI and a p value of < 0.05 was considered statistically significant.
To explain potential interethnic differences in the prevalence of cognitive impairment/dementia, Analysis of Covariance (ANCOVA) was performed (with adjustment for age and gender) to investigate differences in the prevalence of associated risk factors across ethnicities. Post-hoc analyses with Bonferroni-correction were then used to determine the specific differences between individual ethnic groups. Finally, logistic regression models were used to determine the independent effects of ethnicity on the prevalence of any cognitive impairment, after adjustment for the above risk factors. All statistical analyses were performed using Stata 14.1 (StataCorp, College Station, TX).
RESULTS
A total of 1,128 Indian persons from SINDI-2 aged 60 years and above [Median: 68 years] underwent cognitive screening (AMT and PFQ) and hence participated in the EDIS Study. Of these 1,128 persons, 627 were screened negative and 501 participants were screened positive. 334 of the screen-positive persons agreed to participate in phase II, and the remaining 167 non-participants were excluded, leaving a total of 961 persons (627 screen-negatives and 334 screen-positives) available for the analysis (median age; 67.5 years). Table 1 presents the characteristics of all persons who participated at phase I, as well as a comparison between participants and non-participants at phase II. Compared with those who did not participate in phase II, those who participated were younger (mean age 68 years), more often men, had a higher education and income, were less likely to have hypertension and hyperlipidemia, and were more likely to smoke/have smoked. Supplementary Table 1 presents the baseline characteristics of the 1,128 persons from SINDI-1 who eventually participated at SINDI-2 in the EDIS study, compared to SINDI-1 participants who did not participate in SINDI-2 and hence in EDIS. Non-participants were older, less educated, and with lower socioeconomic status.
Characteristics of the Indians who participated in the Epidemiology of Dementia in Singapore (EDIS) Study at SINDI-2
*p values represents differences in the risk factors among participants and non-participants at phase I. BMI, body mass index.
Among 961 persons, a total of 233 (24.3%) participants were diagnosed with any cognitive impairment, of whom 120 (12.5%) had CIND-mild, 101 (10.5%) had CIND-moderate, and 12 (1.2%) were diagnosed with dementia. Of these 12 dementia cases, 9 (0.94%) were classified as Alzheimer’s disease, 1 with vascular dementia (0.1%), and 2 (0.2%) with mixed dementia. Due to the low numbers of dementia cases, CIND-moderate and dementia were grouped together for subsequent analyses. The crude prevalence of any cognitive impairment in the population was 24.3%, with an age-standardized prevalence rate of 24.6% (95% CI: 22.0–27.5). The age-standardized prevalence of CIND-mild was 11.7% (95% CI: 9.8–13.8), and that of CIND-moderate/dementia was 12.9% (95% CI: 10.9–15.3).
Figure 2a shows the prevalence of any cognitive impairment, CIND mild, and CIND moderate/dementia per five-years age strata, Overall, the prevalence of any cognitive impairment increased with age from 15.7% in those aged 60–64 years, to 30.1% in 80-years and above. This trend was particularly observed in the CIND moderate/dementia group (from 5% in 60–64 years to 27.7% in≥80 years). In terms of gender differences, Fig. 2b shows a higher prevalence of any cognitive impairment in women compared to men, which increases with increasing age: 33.8% versus 29.6% in 70–74 years, and 37.9% versus 22.1% in≥80- years.
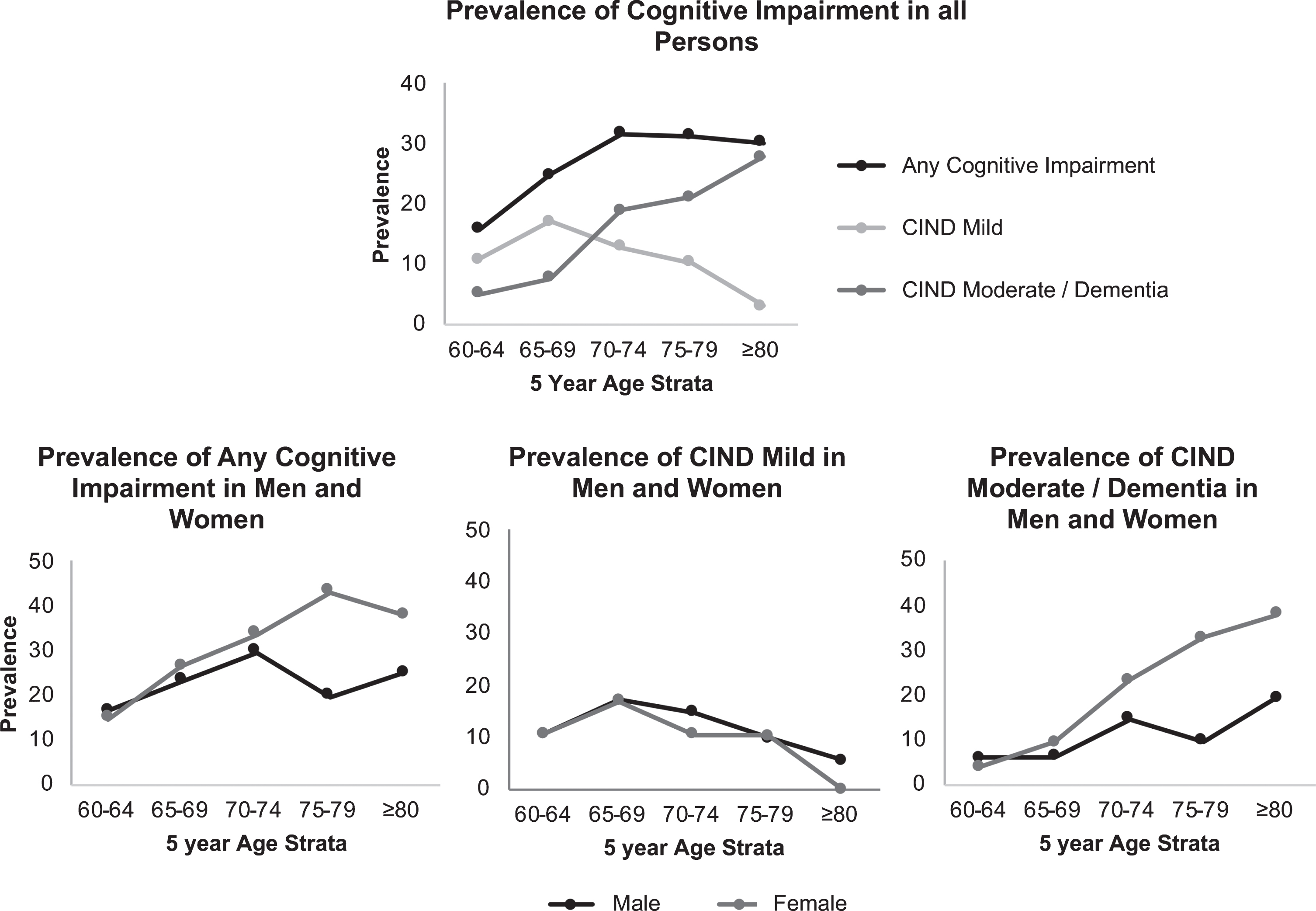
Prevalence of cognitive impairment and dementia, stratified by 5 years age strata.
Table 2 shows that in the fully adjusted model age, education, and the presence of hypertension showed a significant association with cognitive impairment (CIND-moderate/dementia) in Indians. Gender was associated with cognitive impairment in (Model I), but became attenuated after adjustment for all confounders in Model II. None of the risk factors were significantly associated with CIND-mild. Genetic data was only available for a subset of our participants (n = 736 (77%)). Nonetheless, the effect estimates in our multivariable models (Model I and Model II) did not change when performed on this subset.
Association between risk factors and cognitive impairment in Indians expressed as odds ratios (OR) with 95% confidence interval (CI)
aModel I: includes age, gender, education, and each associated factor separately. bModel II: includes age, gender, education, income, housing, diabetes mellitus, hyperlipidemia, hypertension, smoking, and BMI. cAnalysis performed on a subsample of participants (n = 736) with genetic data available for the APOE ɛ4 carrier. CIND, cognitive impairment no dementia; BMI, body mass index; APOE ɛ4, apolipoprotein E.
Upon comparison to previously published data from the Malay and Chinese, the age-adjusted prevalence of any cognitive impairment among Indians (24.6%) was similar to that in Malays (25.5%), but higher than Chinese (15.2%) (p < 0.001). Table 3 presents the prevalence of demographic, cardiovascular, and genetic risk factors, across the ethnic groups. Compared to Chinese, both Indians and Malays had a higher frequency of cardiovascular risk factors, and lower socioeconomic status. Of the three ethnic groups, Indians had the worst cardiovascular risk profiles while Malays had the poorest socioeconomic status.
Risk factors across different ethnicities
cIndicates whether group mean was significantly different compared with Chinese. mIndicates whether group mean was significantly different compared with Malays. *p values adjusted for age and gender based on post-hoc analysis (p < 0.05, with Bonferroni correction) using Analysis of Covariance (ANCOVA). BMI, body mass index; APOE ɛ4, apolipoprotein E.
Table 4 shows the association between ethnicity and cognitive impairment in Chinese and Indians. Adjustment for cardiovascular risk factors in particular, attenuated the relationship between ethnicity and cognitive impairment (from (OR:1.88, 95% CI,1.51–2.25) to (OR:1.41 95% CI,1.08–1.85)). After adjustment for all risk factors, the prevalence of any cognitive impairment in Indians still remained significantly higher compared to Chinese (OR:1.37,95% CI:1.01–1.86). A similar association was likewise observed between the Malays and Chinese (OR: 1.80,95% CI:1.27–2.56), while no significant differences were observed between Indians and Malays (OR: 1.12,95% CI:0.86–1.45).
Effect of risk factors on the difference in Prevalence of any cognitive impairment in Indians compared to Malays and Chinese
Model I: includes age, gender. Model II: Age, gender, education, housing, income, alcohol and smoking. Model III: Age, gender, diabetes, hypertension, hyperlipidemia and BMI. Model IV: Age, gender, education, housing, income, alcohol, smoking, diabetes, hypertension, hyperlipidemia and BMI.
DISCUSSION
In this study, we report that among Indian participants, the overall prevalence of any cognitive impairment was 24.6%, including 1.2% of dementia. The major risk factors of cognitive impairment were age, education, and hypertension. Furthermore, under a similar protocol of recruitment, neurological assessment, and adjustment for known demographic and cardiovascular risk factors, the prevalence of cognitive impairment in Indians was similar to Malays, but nearly 1.5 times higher than Chinese.
To better compare and extrapolate the present findings beyond the Singapore population, Fig. 3 summarizes the reported rates of cognitive impairment from other ethnicities in comparison to data from EDIS. The prevalence rates for Chinese, Malays, and Indians fall within the upper ranges for Caucasian populations (5.1% to 33.3%) [11, 12]. However, the prevalence of cognitive impairment in Indians in the current study is higher than the data from India, which report rates from 3.5% in Himachal Pradesh to 14.9% in Kolkata [14, 30]. It must be noted that the comparison of our findings with other studies is challenging due to methodological issues, most particularly differences in the criteria and assessments used to define cognitive impairment. In particular, the studies in India relied purely on either the Hindi Mental State Examination, or modified Mini-Mental State Examinations, in comparison to the extensive neuropsychological assessment used in diagnosis of cognitive impairment and dementia for the present study. With data suggesting that the prevalence of dementia cases in India will double by 2025 [6], the findings from our study may have implications on healthcare systems and societies beyond Singapore.

Reported prevalencea of cognitive impairment in other populations/ethnic groupsb, based on previous studies. aData for EDIS Chinese, Malay, and Indian studies are using individual prevalence and associated confidence intervals for each study. bThe number of studies per ethnic group is reported in numbers on top of the respective box and whisker plot.
This study found a higher prevalence of cognitive impairment in women than men, especially in those aged≥70 years. Such gender disparity has been observed across multiple studies, largely explained by disparities in education, survival rates, and an increased susceptibility to cerebral small vessel disease in post-menopausal elderly women [15, 31]. Education and hypertension were also found to be independently associated with cognitive impairment in Indians. The observed effect of education is in line with the cognitive reserve hypothesis [32], while a high cardiovascular risk profile is known to increase susceptibility to cognitive impairment via various vascular mechanisms such as vascular fragility, arteriolosclerosis, and endothelial dysfunction [33, 34]. Nonetheless, hypertension and education represent modifiable risk factors, which if targeted, may reduce the development of cognitive impairment.
There still remains a paucity of data regarding interethnic differences using standardized population-based sampling and methods of case ascertainment. Of those that exist, many focused only on dementia, without investigating pre-clinical stages of cognitive impairment [17]. This study showed that Indian elderly have an age-standardized prevalence of cognitive impairment similar to Malays, but higher than Chinese. Previous Singaporean studies have also shown higher risk of dementia in Indians and Malays (OR: 1.92 and 2.32, respectively) compared to Chinese [35]. Similarly, international studies conducted by the 10/66 Dementia Research Group using standardized methods of cognitive assessment, found prevalence rates of cognitive impairment in India (4.3%) to be higher than in China (0.8%), even after age, gender, and education adjustment [36]. It is further reported that the prevalence of cardiovascular risk factors is higher in Indians and Malays compared to Chinese, in addition to differences in socioeconomic risk factors (especially education and income). Indeed, after adjusting for these risk factors (in particular cardiovascular risk factors), the effects of ethnicity were attenuated, but still remained significant. This suggests that these ethnic differences in cognitive impairment are largely, but not fully, explained by differences in demographic and cardiovascular risk factors.
Our results may thus suggest the additional role of genetics and culturally mediated lifestyle factors, such as diet, physical activity, and even social involvement on cognitive functioning as also recently laid by WHO [31, 38]. The “Latent Early-life Associated Regulation” [LEARn] Model, for example, emphasizes the role of environmental, lifestyle, and intrinsic factors in addition to genetic factors to explain the development of dementia [39]. Some studies have also highlighted links between migrant status and cognitive functioning, with migration proposed to underlie several contributory factors to cognitive impairment such as lack of social support, environmental changes, and psychological stress [40, 41]. This may contribute the higher rates of cognitive impairment in Indians (but not indigenous Malays), with a substantial proportion of elderly Indians classified as first generation immigrants (born outside Singapore) [42]. Additional indicators of mental health such as differential depression rates in Indians and Malays [43] may also play a contributory role in compromising cognitive functioning [44]. However, reverse causality cannot be ruled out when it comes to these social, mental, and physical lifestyle components, as neuropathology may begin decades before, and have an effect on lifestyle, before actual symptomatic diagnosis [37]. The APOE ɛ4 allele is the most widely accepted genetic risk factor associated with Alzheimer’s disease [45–47], though its association with cognitive function is reported to vary across ethnic groups and populations [48]. In addition, findings on whether it is a risk factor for the pre-clinical stages of dementia, such as mild cognitive impairment or CIND in particular, have been inconsistent [45]. In this study, however, the APOE4 allele had a minimal role on cognitive functioning, exerting no significant effect in our multivariable models.
The strengths of this study include the drawing of EDIS participants from a population-based study, the use of extensive neuropsychological tests to assess cognitive impairment, and standardized procedures in the collection of participant data. Limitations of our study include: firstly, phase I participants were recruited from the SINDI-2 study, a follow-up cohort from the original baseline SINDI-1 cohort. Persons who presented at SINDI-2 are more likely to be survivors and less cognitively impaired resulting in selection bias. Furthermore, 33.3% of screen-positive persons did not participate in phase II. Non-participants excluded from both phases were generally older, less educated, and with lower socioeconomic and cardiovascular profiles. The exclusion of these two groups of persons with worse risk profiles for cognitive impairment may have led to an underestimation of the prevalence of cognitive impairment and dementia in the Singapore population. However, despite this potential underestimation, a significant ethnic difference between Indians and Chinese was still found. Secondly, due to the small number of dementia cases, it was not possible to study dementia separately, or examine the different subtypes of dementia in further detail. Lastly, the cross-sectional design does not allow temporal inferences on associations between risk factors and cognitive impairment.
In conclusion, among elderly Indians, the overall prevalence of any cognitive impairment is 24.6%, including 1.2% of dementia, similar to the rates reported in Malays previously. However, even with a similar protocol of recruitment, assessment, and adjustments for known demographic, cardiovascular, and genetic risk factors, the prevalence of cognitive impairment remained higher in Indians compared to Chinese. Further research is still required to unravel other (potentially modifiable) factors that may underlie these ethnic differences in the occurrence of cognitive impairment and dementia.
Footnotes
ACKNOWLEDGMENTS
This work is supported by the National Medical Research Council (NMRC), Singapore (NMRC/CG/NUHS/2010 [Grant no: R-184-006-184-511]) and (NMRC/CSA/038/2013).
Funders had no role in study design; collection, analysis and interpretation of the data; in the writing of the report; and in the decision to submit the paper for publication.