
Abstract
Background:
Aberrant motor behavior (AMB) is a neuropsychiatric symptom (NPS) prevalent in Alzheimer’s disease (AD), known to cause great distress to both patients and caregivers. Apolipoprotein E4 (APOE4) is the most important genetic predictor of AD, and it has been associated with high NPS prevalence.
Objective:
To investigate the neuropathological substrates and risk factors associated with AMB in AD patients.
Methods:
Cases with Braak stage I-II and CERAD 0-1 were classified as Low AD (LAD), while Braak stage III-IV and CERAD 2 were grouped as Intermediate AD (IAD). Cases with Braak stage V-VI and CERAD 3 were classified as High AD (HAD) in accordance with NIA-Reagan criteria. All cases were stratified by APOE genotype, yielding No ɛ4 & ɛ4 and ɛ4/ɛ4 groups depending on ɛ4 copy number within APOE. Presence of AMB was assessed using NPI-Q.
Results and Conclusion:
AMB increased in parallel with CERAD and Braak & Braak scores. Hypercholesterolemia, but no other cardiovascular risk factors, was associated with AMB in HAD. AMB prevalence in HAD was significantly increased in the presence of two APOE ɛ4 alleles as compared to No ɛ4 & ɛ4. The relationship between homozygous APOE4 and AMB was strongly associated with the presence of both Lewy bodies and cerebral amyloid angiopathy pathologies in both sexes.
Keywords
INTRODUCTION
Aberrant motor behavior (AMB) is characterized by engagement in repetitive movements, inability to keep still, and irregular pacing [1] among others. As a symptom, AMB has been strongly associated with Alzheimer’s disease (AD) [2, 3], dementia, and its several subtypes [4]. AMB is also one of the twelve neuropsychiatric symptoms (NPS) assessed through the Neuropsychiatric Inventory questionnaire (NPI) [2]. As a symptom, several studies report higher AMB prevalence scores in clinically diagnosed severe AD [3, 5], with an overall 24.3% [6] to 32% prevalence [7]. AMB has also been associated with medium to high levels of caregiver burden and patient distress [8]. The ɛ4 allele of the Apolipoprotein E (APOE) gene is the most important genetic predictor of late onset AD [9]. APOE4 has been associated with several neuropathological and clinical features of AD such as amyloid-β (Aβ) plaque formation, disruption of synaptic plasticity [10, 11], and accelerated dementia in a dose dependent manner [12]. In addition, APOE4 genotype has been repeatedly associated with a higher prevalence of all NPS [13]. Focused studies on depression [14], psychosis, and its subtypes in severe AD have also reported an association with APOE4 [15]. In the aforementioned study, APOE4 effect on psychosis was found to be mediated by the presence of comorbid Lewy body (LB) pathology [15].
Despite its prevalence and distressing effects on AD patients, the underlying mechanisms responsible for AMB are poorly understood. The goal of this study is to investigate the role of AD load and comorbid neuropathological substrates such as LB and cerebrovascular pathology play in the development of AMB. Furthermore, we seek to investigate the relationship between AMB prevalence and genetic and cardiovascular risk factors.
MATERIALS AND METHODS
Data and subject criteria
Data was obtained from the National Alzheimer’s Coordinating Centre (NACC) dataset, which contains clinical and neuropathological data from Alzheimer’s Disease Centers in the United States funded by the National Institute of Aging (NIA). The Uniform Data Set (UDS), the Neuropathological Data Set (NP), as well as the Research Data Dictionary-Genetic Data set (RDD-Gen) were used throughout the study. Demographical and clinical data, including gender and cardiovascular risk factors such as hypertension, hypercholesterolemia, diabetes, and smoking history were obtained from the UDS. AMB presence was assessed using the Neuropsychiatric Inventory, Quick version (NPI-Q), evaluating the presence of motor disturbance within the month prior to a clinical visit. Criteria for motor disturbance within NPI-Q comprises, yet is not limited to, engaging in irregular pacing, repetitive set of movements, and overall inability to keep still.
The NP was used to evaluate AD severity using neuropathological criteria. CERAD scores and Braak & Braak stage were used to assess density of neuritic plaques and neurofibrillary pathology, respectively. NP was also used to gauge the presence of comorbid LB pathology, as determined by positive immunohistochemical staining for alpha-synuclein at any cerebral site. Further LB quantification was not used. Cerebrovascular disease was assessed through the presence of ischemic, hemorrhagic and overall vascular pathology (IHVP), cerebral amyloid angiopathy (CAA: including mild, moderate, and severe CAA), and subcortical arteriosclerotic leukocephalopathy (SAL).
The RDD-Gen was used to confirm patient’s genetic background. The number of ɛ4 alleles within APOE gene was used to classify cases according to their APOE4 genotype.
Cases with other primary etiological diagnoses such as traumatic brain injury, CNS neoplasm, Down syndrome, Huntington’s disease, progressive supranuclear palsy, corticobasal degeneration, prion disease, and frontotemporal dementia with or without amyotrophic lateral sclerosis were excluded. Cases with Braak & Braak stage I & II and CERAD 1 and 0 were classified as Low AD pathological load (LAD), while Braak stage III & IV and CERAD 2 cases were classified as Intermediate AD pathological load (IAD), and cases with Braak stage V & VI and CERAD 3 were classified as High AD load (HAD), in accordance with NIA-Reagan criteria [16]. Cases with incongruent CERAD and Braak & Braak scores were excluded. Regarding APOE ɛ4 status, cases were classified as No ɛ4, presence of one (ɛ4) or two copies (ɛ4/ɛ4) of the ɛ4 allele; cases with unassessed APOE4 genotype were also excluded.
Statistical analysis
Statistical analysis was performed using SPSS 23.0 software. Unadjusted logistic regression models were used to assess the relationship between AD pathological loads, gender, APOE4 genotype, preliminary associations, comorbid neuropathological substrates, and AMB. Logistic regression results were reported as odds ratio (OR) with associated 95% confidence intervals (CI), as well as p-value. One-way ANOVA was used for direct comparisons between continuous data such as preliminary neuropathological associations coupled with risk estimate. Results were reported as p value, followed by OR with associated 95% CI. All statistical analyses were conducted using an α= 0.05 significance.
RESULTS
Subject demographics
We assessed AMB prevalence in an initial sample of 2,959 cases in the NACC NP dataset. Cases were then classified using CERAD and Braak & Braak scores as described [16], yielding 831 LAD, 584 IAD, and 1,544 HAD cases. Because of the scarcity of ɛ4/ɛ4 subjects, the LAD and IAD subsets were grouped into a Low to Intermediate AD group (LIAD). After excluding those with unassessed APOE4 genotype, we identified 1,218 LIAD and 1,333 HAD cases. Further information regarding the demographic and clinical characteristics of LIAD and HAD groups can be found in Table 1.
Demographic and clinical characteristics
Aberrant motor behavior across CERAD, Braak & Braak scores, and overall AD load
First, we assessed the prevalence of AMB in relation to AD pathology load, separately for plaques and neurofibrillary pathology, and then jointly. AMB prevalence significantly increased with CERAD scores (p = 0.001, Fig. 1A). CERAD 3 and CERAD 2 cases were significantly more likely to report present AMB compared to CERAD 0 (OR = 3.928, 95% CI 2.897–5.326, p = 0.001; OR = 2.433, 95% CI 1.724–3.433, p = 0.01, respectively). AMB prevalence increased along Braak & Braak stages as well (p = 0.001, Fig. 1B), with Braak VI being significantly more likely to report AMB than Braak 0 (OR = 2.268, 95% CI 1.349–3.813, p = 0.002). Interestingly, Braak II was significantly less likely to report AMB than Braak 0 (OR = 0.520, 95% CI 0.282–0.958, p = 0.036). As seen in Fig. 1B, those 19 Braak 0 cases reported present AMB in an off-trend fashion, with their primary diagnosis being Lewy body disease (26.3%) and cognitive impairment with unknown cause (26.3%).
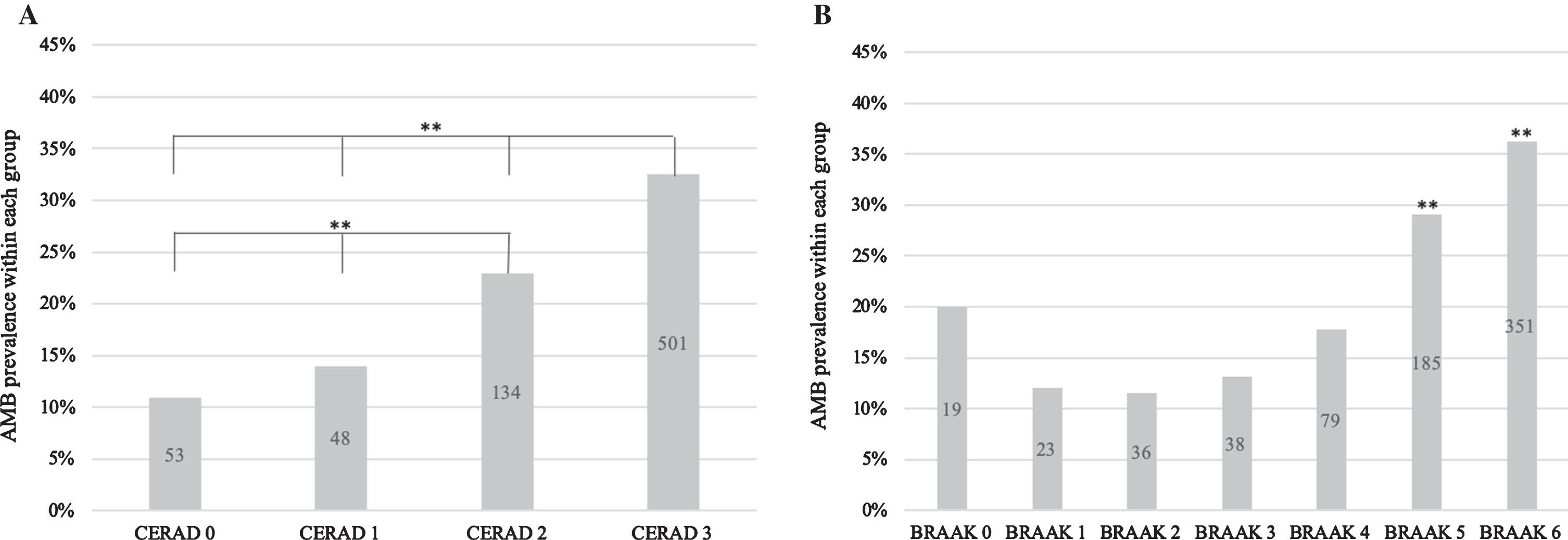
AMB prevalence increases across neuropathological substrates. Each column represents % of cases with present AMB in each pathological substrate group. Logistic regression was used to assess AMB prevalence differences between groups. Number of cases within group reflected in each bar. **p = 0.001, *p < 0.050. AMB prevalence increases across (A) CERAD scores and (B) Braak & Braak stages (except Braak 0).
AMB significantly increased across AD load (p = 0.001, Fig. 2), with HAD being significantly higher than LAD (OR = 3.473, 95% CI 2.748–4.386, p = 0.001). AMB differences between IAD and LAD were also significant (OR = 2.152, 95% CI 1.621–2.858, p = 0.001). Throughout AD load, gender did not influence AMB prevalence, as females were not more likely to report AMB compared to males (OR = 0.878, 95% CI 0.742–1.039, p = 0.129).

AMB prevalence increases significantly across AD pathological load. Each column represents percent of cases with present AMB in each AD load group. AMB prevalence differences were assessed with an unadjusted logistic regression model using LAD as an indicator. Number of cases within group reflected in each bar. **p = 0.001.
APOE4 genotype is associated with AMB in HAD but not in LIAD load
APOE4 genotype did not significantly influence AMB within LIAD (p = 0.120, Table 3). Compared to No ɛ4, ɛ4/ɛ4 cases were not significantly more likely to report AMB in LIAD (OR = 1.356, 95% CI 0.583–3.153, p = 0.480). Only 7 cases homozygous for APOE ɛ4 genotype reported present AMB in LIAD, and thus we did not perform any further analysis in the LIAD group.
Regression analysis of the relationship between AMB prevalence and AD neuropathological load
Table representing the relationship between AD pathological load, separately and jointly, and AMB prevalence. Predictors referred to presence of neuritic plaques (CERAD score), neurofibrillary pathology (Braak & Braak score), or joint AD pathological load (LAD-HAD). Numerical values within each column represent Odds Ratio with associated 95% Confidence Interval (95% CI) and p value. The relationship between AD neuropathological load and AMB was assessed in an unadjusted logistic regression model.
Regression analysis of the relationship between APOE4 genotype and presence of AMB in LIAD and High AD load
Table representing the relationship between APOE4 genotype and AMB prevalence in different AD pathological loads. Predictors referred to the presence of one (ɛ4) or two (ɛ4/ɛ4) copies of the ɛ4 allele of the APOE gene in cases with Low to Intermediate AD load (LIAD) or High AD load (HAD). Numerical values within each column represent Odds Ratio with associated 95% Confidence Interval (95% CI) and p value. The relationship between APOE4 genotype and AMB prevalence was assessed in an unadjusted logistic regression model.
In HAD, APOE4 genotype did influence AMB prevalence (p = 0.001, Table 3). Compared to No ɛ4 only, ɛ4/ɛ4 cases were significantly more likely to report AMB in HAD.
(OR = 2.124, 95% CI 1.504–2.998, p = 0.001, Table 3). ɛ4 cases were also more likely to report present AMB compared to No ɛ4 (OR = 1.377, 95% CI 1.065–1.781, p = 0.015).
APOE ɛ4/ɛ4 is associated with AMB in HAD cases
We then performed a regression analysis of the relationship between the presence of two copies of ɛ4 in APOE4 and AMB prevalence in HAD. ɛ4/ɛ4 cases were more likely to report AMB when analyzed against one ɛ4 copy only (OR = 1.542, 95% CI 1.111–2.140, p = 0.010, Table 3) and No ɛ4 & ɛ4 (OR = 1.769, 95% CI 1.297–2.411, p = 0.001; Fig. 3, 1.a). Given these results, the impact of APOE ɛ4 allele on AMB prevalence was further assessed by grouping HAD cases into No ɛ4 & ɛ4 and ɛ4 homozygous (ɛ4/ɛ4) groups. ɛ4/ɛ4 was more likely to report present AMB in both females (OR = 1.923, 95% CI 1.175–3.149, p = 0.009; Table 4, Fig. 3, 1.b) and males (OR = 1.653, 95% CI 1.108–2.465, p = 0.014; Table 4, Fig. 3, 1.c) compared to No ɛ4 & ɛ4 in HAD.
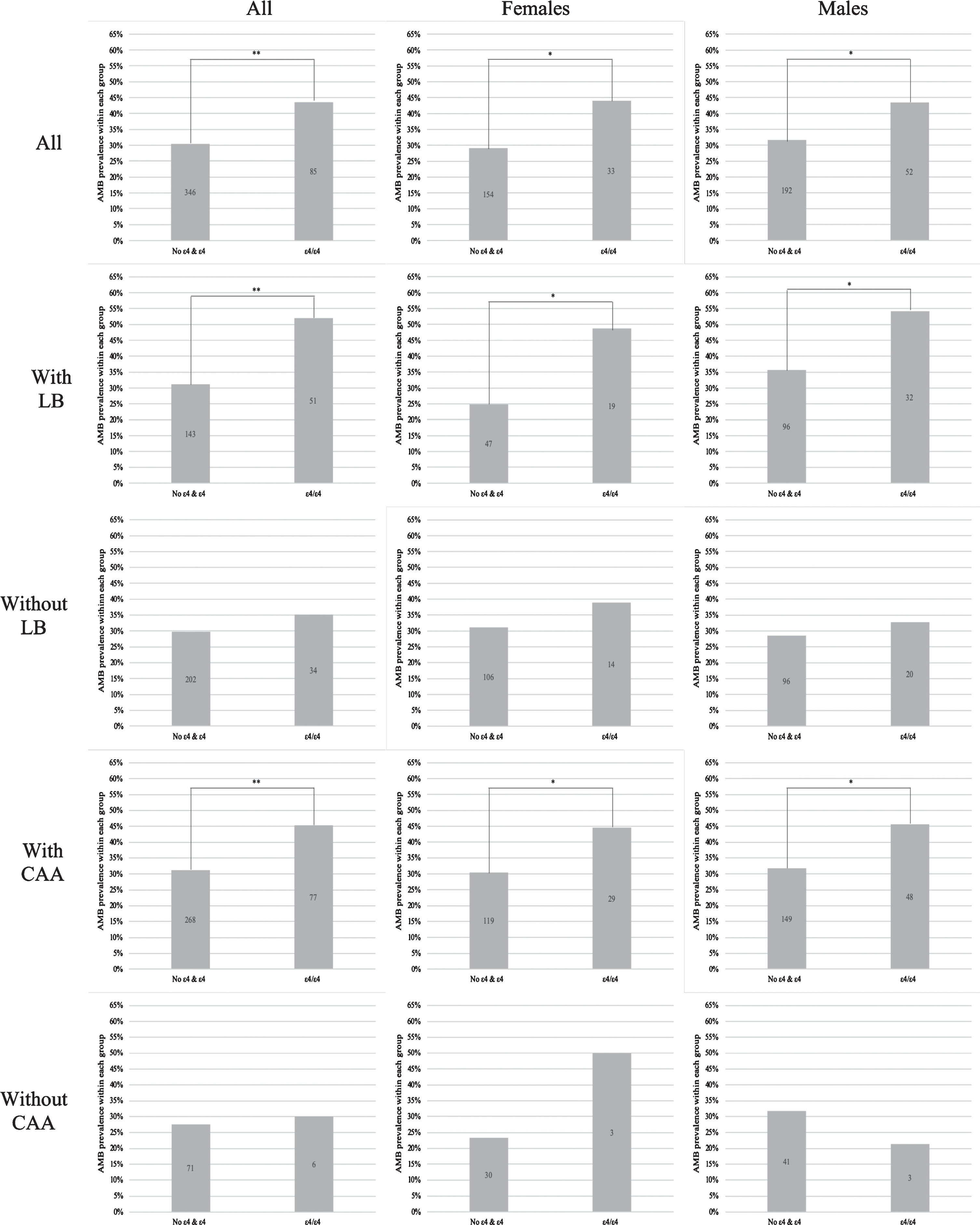
APOE ɛ4/ɛ4 significantly increases AMB prevalence in the presence of individual neuropathological substrates in both genders in HAD. Each column represents percent of cases with present AMB according to its APOE4 genotype-HAD group. AMB prevalence differences were assessed with an unadjusted logistic regression model using No ɛ4 & ɛ4 as an indicator. Number of cases within group reflected in each bar. First row represents all HAD cases, 2nd row represents HAD cases with comorbid LB, 3rd row represents HAD cases with absent LB, 4th row represents HAD cases with comorbid CAA, and 5th row represents HAD cases with absent CAA. Column A represents both females and males, column B represents females only, and column C represents males only. Each individual graph is labeled as Figure 5 number.letter, with number referring to row and letter referring to column. **p = 0.001, *p < 0.050.
Regression analysis of the relationship between APOE ɛ4/ɛ4 genotype and presence of AMB with comorbid neuropathological substrates in HAD
Table representing the impact of Lewy bodies (LB) and cerebral amyloid angiopathy (CAA) as separate comorbid neuropathological substrates on the relationship between APOE4 and AMB in HAD. Predictors referred to presence of two (ɛ4/ɛ4) copies of the ɛ4 allele of the APOE gene in HAD cases with or without LB, as well as with or without CCA. Numerical values within each column represent Odds Ratio with associated 95% Confidence Interval (95% CI) and p value. The relationship between APOE4 genotype and AMB prevalence was assessed in an unadjusted logistic regression model.
Hypercholesterolemia is the only vascular risk factor or lesion directly associated with AMB in HAD
Prevalence of vascular lesions or risk factors in cases with AMB was then investigated. No direct significant associations were found between AMB and IHVP (p = 0.603, OR = 1.285, 95% CI 0.499–3.307), CAA (p = 0.065, OR = 1.317, 95% CI 0.982–1.765), and SAL (p = 0.733, OR = 1.059, 95% CI 0.761–1.474) in HAD. Hypercholesterolemia was the only cardiovascular risk factor significantly associated with AMB in HAD (p = 0.035, OR = 1.279, 95% CI 1.017–1.607). AMB prevalence did not significantly differ in cases with hypertension (p = 0.506, OR = 0.927, 95% CI 0.741–1.159), diabetes (p = 0.968, OR = 1.007, 95% CI 0.704–1.442), or past smoking history (p = 0.618, OR = 1.021, 95% CI 0.942–1.106) in HAD.
In HAD, APOE ɛ4/ɛ4 is associated with AMB in cases with LB pathology in both sexes
LB pathology was not directly associated with higher AMB prevalence in HAD (p = 0.091, OR = 1.222, 95% CI 0.969–1.541). However, LB pathology was significantly associated with APOE ɛ4 allele’s copy number in HAD (p = 0.006), with homozygous APOE4 being significantly more likely to report present LB (OR = 1.704, 95% CI 1.220–2.378, p = 0.002). Therefore, APOE4 effect on AMB was re-assessed upon stratification by LB. In HAD cases with comorbid LB, the presence of ɛ4/ɛ4 in APOE significantly influenced AMB prevalence when analyzed against No ɛ4 & ɛ4 (OR = 2.390, 95% CI 1.535–3.722, p = 0.001; Table 4, Fig. 3, 2.a). This association was maintained when females (OR = 2.870, 95% CI 1.412–5.834, p = 0.004; Fig. 3, 2.b) and males (OR = 2.136, 95% CI 1.208–3.775, p = 0.009; Fig. 3, 2.c) were analyzed separately.
In the absence of LB, AMB prevalence differences between ɛ4/ɛ4 and No ɛ4 & ɛ4 were not significant (OR = 1.269, 95% CI 0.810–1.987, p = 0.298; Table 4, Fig. 3, 3.a). The association remained non-significant in both females (OR = 1.405, 95% CI 0.692–2.852, p = 0.347; Fig. 3, 3.b) and males (OR = 1.225, 95% CI 0.683–2.197, p = 0.497; Fig. 3, 3.c).
In HAD, APOE ɛ4/ɛ4 is associated with AMB in cases with CAA in both sexes
APOE4 genotype was not significantly associated with either IHVP or SAL in HAD (p = 0.113 and p = 0.555, respectively). In contrast, ɛ4 copy number in APOE was significantly associated with CAA in HAD (p = 0.001), with homozygous APOE4 being significantly more likely to report CAA (OR = 4.212, 95% CI 2.556–6.940, p = 0.001). The association between APOE4 and AMB was then re-assessed upon stratification by CAA. In the presence of comorbid CAA, ɛ4/ɛ4 in APOE significantly influenced AMB prevalence when analyzed against No ɛ4 & ɛ4 (OR = 1.826, 95% CI 1.306–2.552, p = 0.001; Table 4, Fig. 3, 4.a). This association was maintained in both females (OR = 1.835, 95% CI 1.075–3.131, p = 0.026; Fig. 3, 4.b) and males (OR = 1.809, 95% CI 1.176–2.781, p = 0.007; Fig. 3, 4.c).
In the absence of CAA, we found no significant differences in AMB prevalence based on APOE4 genotype (OR = 0.811, 95% CI 0.417–3.052, p = 0.811; Table 4, Fig. 3, 5.a). This relationship remained non-significant in both females (OR = 3.300, 95 % CI 0.633–17.211, p = 0.157; Fig. 3, 5.b) and males (OR = 0.585, 95% CI 0.155–2.212, p = 0.430; Fig. 3, 5.c).
In HAD, APOE ɛ4/ɛ4 is associated with AMB in cases with concurrent CAA and LB only
Given our previous results on the relationship between APOE4 and both LB and CAA, the association between APOE4 and AMB was re-assessed upon double stratification by CAA and LB. In cases with presence of both LB and CAA, AMB prevalence in ɛ4/ɛ4 was significantly greater than in No ɛ4 & ɛ4 (OR = 2.681, 95% CI 1.663–4.322, p = 0.001; Table 5, Fig. 4.a). We found no significant differences in AMB prevalence between ɛ4/ɛ4 and No ɛ4 & ɛ4 in HAD cases with comorbid LB but absent CAA (OR = 0.800, 95% CI 0.147–4.368, p = 0.797; Fig. 4.b). The same trend was found in cases with absent LB but present CAA (OR = 1.226, 95% CI 0.754–1.993, p = 0.412; Fig. 4.c), as well as cases with both LB and CAA absent (OR = 1.366, 95% CI 0.399–4.670, p = 0.619; Fig. 4.d).
Regression analysis of the relationship between APOE ɛ4/ɛ4 genotype and presence of AMB with concurrent LB and CAA pathology in HAD
Table representing the effect of Lewy bodies (LB) and cerebral amyloid angiopathy (CAA) as concurrent neuropathological substrates on the relationship between APOE4 and AMB in HAD. Predictors referred to presence of two (ɛ4/ɛ4) copies of the ɛ4 allele of the APOE gene in HAD cases with or without LB, as well as with or without CCA. Numerical values within each column represent Odds Ratio with associated 95% Confidence Interval (95% CI) and p value. The relationship between APOE4 genotype and AMB prevalence was assessed in an unadjusted logistic regression model.
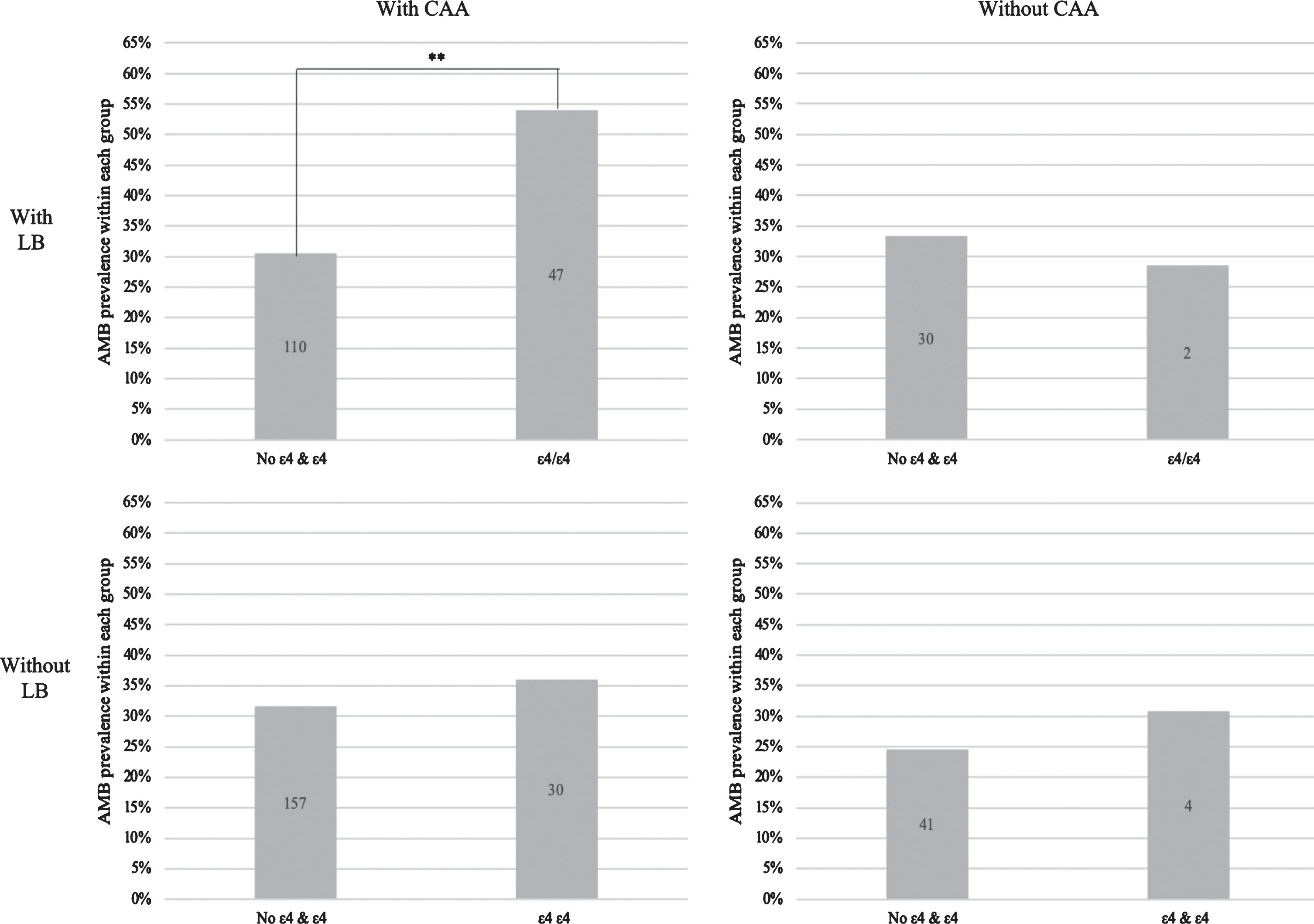
APOE ɛ4/ɛ4 is associated with higher AMB prevalence only in cases with comorbid LB and CAA pathology in HAD. Each column represents percent of cases with present AMB according to its APOE4 genotype-HAD group. AMB prevalence differences were assessed with an unadjusted logistic regression model using No ɛ4 & ɛ4 as an indicator. Number of cases within group reflected within each bar. (a) The presence of two copies of ɛ4 within APOE is significantly associated with AMB prevalence in HAD cases with comorbid LB and CAA (top, left). The presence of two copies of APOE ɛ4 does is not significantly associated with higher AMB prevalence in HAD cases with (b) present LB but absent CAA (top, right), (c) absent LB but present CAA (bottom, left), and (d) absent LB and CAA pathology (bottom, right). **p = 0.001.
DISCUSSION
We found AMB prevalence to significantly increase along with AD pathological load. These results are consistent with others reporting an association between AMB and neurofibrillary pathology [17], although that study focused on AMB with comorbid agitation. Neurofibrillary tangle burden has also been linked to other NPS such as apathy [18] and psychosis [19]. We found SAL not significantly associated with either AMB or APOE genotype, unlike the findings of a study focused on psychosis [20]. However, there is mixed evidence regarding the relationships between specific NPS and white matter rarefaction in AD [21, 22]. In High AD, the ɛ4 allele of the APOE gene significantly influenced AMB prevalence in a strong recessive pattern. The literature offers mixed evidence regarding the role of APOE4 role in NPS development, with several studies reporting a non-significant [23], mixed [16], and a significant relationship between them [17]. This discrepancy could be explained by the reliance on clinical AD characterization [16, 23], whereas our study used neuropathological postmortem analysis. Interestingly, the relationship between NPS and APOE has mostly been assessed in APOE ɛ4 carriers [17]. However, we found the association between homozygous APOE4 and AMB to be significant when analyzed against cases with no copies of ɛ4, as well as cases with one copy of ɛ4, and both no copies and one copy together. These results agree with others reporting a specific APOE4 recessive effect in delusions [24] and anxiety prevalence [25] in AD.
We found LB pathology significantly associated with high AMB prevalence in homozygous APOE4 cases, thus agreeing with others on the importance of comorbid LB in the association between APOE4 genotype and NPS prevalence [26]. However, LB development has been associated with multiple genetic variants [27], and so the association between APOE4 and AMB might not be entirely mediated by LB. This observation is supported by our own findings on CAA, which was found to be significantly associated with a homozygous APOE4 effect on AMB. Although APOE4 has been extensively associated with CAA in AD [28, 29], the relationship between CAA and NPS is not understood. Up to date, CAA has only been associated with psychosis in AD [30], as well as being reported in a clinical case with a patient presenting psychosis and depression [31]. To our knowledge, our study is the first one reporting CAA presence as an additional pathological feature possibly mediating the association between APOE4 genotype and any NPS development.
Most importantly, our results suggest that the proven association between APOE4 and NPS is possibly influenced by several pathological substrates. A strong association between APOE4 homozygosity and AMB prevalence was only reported in the presence of both LB and CAA. If either of those pathological substrates was absent, differences in AMB prevalence became non-significant. High CAA prevalence has been previously associated with Lewy body disease [32] and Lewy body variant of AD [33]; however, no studies have focused on the functional consequences of CAA and LB comorbidity. To our knowledge, our study is the first one reporting comorbid LB and CAA as a pathological substrate possibly mediating the association between APOE4 homozygosity and any AD-related clinical outcome.
However, there are limitations to our study. The use of NIA-Reagan criteria to characterize High AD load could also be considered a limitation, for we excluded cases with discordant CERAD and Braak scores. The use of NPI-Q is also limiting in that it only considers a standardized recording of AMB within the last clinical visit, and thus data on AMB course was not reported. Additionally, presence of AMB was dependent on caregiver input, leaving room for possible confounds. It should also be noted that the NACC database is a voluntary sample set, and thus it might not be representative of the entire population suffering from AD. In summary, we demonstrate that AMB prevalence significantly increases with AD load, and that APOE4 genotype influenced AMB in a recessive pattern. This association was only found in the presence of concurrent LB and CAA pathology in both sexes, supporting the existence of multiple pathological substrates possibly mediating the association between APOE4 genotype and AMB prevalence. Further research is needed to clarify whether comorbid CAA and LB pathology influence other clinical manifestations of the disease.
Footnotes
ACKNOWLEDGMENTS
The NACC database is funded by NIA/NIH Grant U01 AG016976. NACC data are contributed by the NIA-funded ADCs: P30 AG019610 (PI Eric Reiman, MD), P30 AG013846 (PI Neil Kowall, MD), P50 AG008702 (PI Scott Small, MD), P50 AG025688 (PI Allan Levey, MD, PhD), P50 AG047266 (PI Todd Golde, MD, PhD), P30 AG010133 (PI Andrew Saykin, PsyD), P50 AG005146 (PI Marilyn Albert, PhD), P50 AG005134 (PI Bradley Hyman, MD, PhD), P50 AG016574 (PI Ronald Petersen, MD, PhD), P50 AG005138 (PI Mary Sano, PhD), P30 AG008051 (PI Steven Ferris, PhD), P30 AG013854 (PI M. Marsel Mesulam, MD), P30 AG008017 (PI Jeffrey Kaye, MD), P30 AG010161 (PI David Bennet, MD), P50 AG047366 (PI Victor Henderson, MD, MS), P30 AG010129 (PI Charles DeCarli, MD), P50 AG016573 (PI Frank LaFerla, PhD), P50 AG016570 (PI Marie-Francoise Chesselet, MD, PhD), P50 AG005131 (PI Douglas Galasko, MD), P50 AG023501 (PI Bruce Miller, MD), P30 AG035982 (PI Russel Swerdlow, MD), P30 AG028383 (PI Linda Van Eldik, PhD), P30 AG010124 (PI John Trojanowski, MD, PhD), P50 AG005133 (PI Oscar Lopez, MD), P50 AG005142 (PI Helena Chui, MD), P30 AG012300 (PI Roger Rosenberg, MD), P50 AG005136 (PI Thomas Montine, MD, PhD), P50 AG033514 (PI Sanjay Asthana, MD, FRCP), P50 AG005681 (PI John Morris, MD) and P50 AG047270 (PI Stephen Strittmatter, MD, PhD).