
Abstract
Background:
The environment of patients with Alzheimer’s disease and related disorders (ADRD) intensifies the consequences of cognitive impairment and exacerbates behavioral problems if inappropriate or, conversely, mitigate these problems if its design is tailored to the needs of these persons.
Objective:
We evaluate the impacts of hospitalization and of a specific healing garden on self-consciousness which represent a central impairment in ADRD. The self-consciousness questionnaire (SCQ), validated for its assessment at mild to moderate phases of the disease, explores the dimensions of personal identity, awareness of cognitive deficiencies, self-assessment of affective state, awareness of body representation, prospective memory, capacity for introspection, and moral judgments.
Methods:
After having verified, by means of a preliminary study, its feasibility to the more advanced stages of the disease, this questionnaire allowed assessment of the impact of the environment by comparing, in routine care, patients hospitalized in a cognitive-behavioral unit who solely remain indoors with others who use the Art, Memory and Life healing garden.
Results:
A significant decrease in SCQ due to an increase in anosognosia during hospitalization was observed in the group that remained indoors. For the group using the garden, a positive effect on overall SCQ score was observed, as a result of a significant improvement in body representation as the driving parameter.
Conclusion:
Factors that are grounded in the hypotheses that spearheaded its conception, such as sensory enrichment, familiarity, contact with nature, scaffolding role for cognitive functions, supportive effect for social interactions, and the “Nancy hypotheses of beauty”, thus contribute to their validation.
INTRODUCTION
Particularly frequent, Alzheimer’s disease and related disorders (ADRD) ultimately lead to a severe loss of autonomy related to cognitive and psycho-behavioral disorders. This leads to the institutionalization of a large number of affected individuals in nursing homes for dependent elderly persons (Etablissements d’Hébergement pour Personnes Âgées Dépendantes, EHPAD). As a result, these individuals are confronted with the risk of being cut off from the ‘normal’ outside world both by their cognitive disorders and their institutional confinement.
Self-consciousness (SC), or reflective consciousness [1], proper to humans and a few great apes [2], allows the subject to be the object of his consciousness [3, 4]. SC is inseparable from memory through which the identity of each individual is constructed and maintained. It features many facets [5 –7]: for the subject, it is the consciousness of his or her perceptions, of his or her body, the cognition of his or her own projects [3], the subject’s judgment on his or her own thoughts and actions, and the subject’s self-knowledge through his or her autobiographical memory [8 –11]. SC is also expressed through our relationship with others. Becoming aware of the existence of this Other, distinct from oneself, allows strengthening one’s individual identity and therefore SC. A neural network, e.g., medial prefrontal cortex, precuneus, temporoparietal junction, and temporal lobe, involved in the elaboration and consolidation of the sense of identity has been described as the brain map of the Self. The prefrontal regions are believed to coordinate the representations of the Self and the Other, contributing to social cognition [12].
Impairments in SC are considered a major characteristic during ADRD [4]: daily clinical experience testifies to the frequency of the anosognosia or non-awareness of the disorders, present in 23% to 75% cases according to different studies. Likewise, the inability to recognize oneself in the mirror at the advanced stages results from the alteration of the residual capacities to acquire new semantic knowledge regarding the Self. According to Moghrabi, Braun, and Morris, even though the patient can still refer to his or her premorbid self (petrified self), he or she no longer modifies his or her reflection of Self; thus, while self-maintenance persists, the integration of new experiences involving self-adjustment is altered [13]. Cohen-Mansfield et al. identified modifications of four types of role-identity during AD: the professional role which is the most impaired, the family role which is best preserved, while the impairment of role identities of leisure activities and of personal attributes is intermediate [14, 15]. The Self’s sense of identity is correlated with the severity of the disorders as assessed by the Mini-Mental State Examination (MMSE) score. Gil et al. further validated a self-consciousness questionnaire (SCQ) adapted to its assessment in Alzheimer’s disease and frontotemporal dementia [4 , 16]. These authors suggested that SC disturbances likely fall into the default network, namely the posterior cingulate cortex, orbital and medial prefrontal cortex, and angular gyrus, involved in self-oriented tasks and social cognition. In Alzheimer’s disease, this rather involves a defective addressing of information by the altered posterior cortical areas toward the medial prefrontal cortex whereas the behavioral variant of frontotemporal dementia likely results from a direct impairment of the latter [16].
However, the benefits of non-pharmacological approaches on SC, such as music therapy, have been demonstrated during AD using the SCQ [17].
The link between nature and health has been well recognized since antiquity, at a time when the temples of Asclepios surrounded patients with nature, music, and art in order to promote their healing [17]. The benefits of nature on health apply to the prevention and alleviation of symptoms of stress and anxiety as well as in various diseases [18 –27]. The use of healing gardens is currently being developed in France in various healthcare and medico-social establishments, particularly since the impetus given by the 2008-2012 Alzheimer’s Plan. The term ‘garden’ corresponds to an enclosed green space, according to the Latin origin hortus conclusus designed by and for man. This garden becomes therapeutic when it becomes an aid to the process of care, is integrated in the project of a nursing team, and is adapted to the needs of the individuals who use the healing garden, whether they be patients or residents, family members, or healthcare team [28].
Several theories have attempted to explain this link between nature and health: 1) Wilson’s theory of biophilia is based on the innate attraction of human beings to other living organisms and generally to nature [19, 29]; 2) Ulrich’s theory of stress reduction, according to which the presence of natural elements aids the recovery process during stressful events [25]; and 3) Kaplan and Kaplan’s theory in which the presence of natural elements captures involuntary attention and allows the restoration of directed attention [27].
While the benefits of using healing gardens have been demonstrated, particularly on psycho-behavioral disorders and the affective state during ADRD [29, 30], no study has yet examined the effect of hospitalization conditions on SC. The present study aimed to focus on the impact of providing patients with neurodegenerative disease access to a healing garden during their hospitalization. Given the number of affected individuals living in institutions with available green spaces which could be developed into healing gardens on the one hand and the importance of alterations in SC during ADRD on the other, it is our belief that this particular domain deserves to be explored. We present herein an exploratory study comprised of two phases:
The preliminary study was carried out in routine care; patients and their care providers were informed of the study by the physician in charge of the CBU and their consent was requested. The JAZ SELF study received a favorable opinion from the Ethics Committee of the CHRU Nancy on June 26, 2016.
MATERIAL AND METHODS
Art Memory and Life
The Art, Memory and Life garden created at the Paul Spillmann Center of the University Hospital of Nancy, for individuals with progressive neurocognitive diseases, brings together nature, art, and regional culture [31 –38]. The garden encompasses a total area of 4000 m2 and is directly accessible from the day room of the CBU unit. The garden is surrounded by buildings on three sides and a gate with a view of the city on the fourth. Access is restricted to patients and visitors to the center. Maintenance is provided by the green spaces department of the CHRU which collaborated with the pilot group during its design and development in 2008-2010. The region’s climate is continental with cool winters and frequent rain. The garden is oriented facing south with the building to the north; it is both sunny and shaded owing to the presence of numerous old trees that are planted within. Patients do not have to leave the care center during their stay to go into the garden. The garden can be accessed directly from the day room of the CBU unit, thereby allowing patients to enjoy or have activities outside. Patients can use the garden as they please, which is very similar to the conditions in a nursing home, while providing them with a maximum of autonomy. Patients can walk in the garden, admire the plants and numerous works of art that have been added, use the benches to contemplate the garden or hold conversations; tables are judiciously arranged allowing them to put their personal objects, a magazine, or have an available beverage in case of hot weather. The flowers can be touched and cut to make a small bouquet; the sculptures are accessible and intended to be touched and explored owing to their surface texture specifically designed for tactile exploration. Patients can receive their loved ones of all ages in the garden. Planters with small-sized strawberry plants as well as aromatic and scented plants are installed in the garden, all of which can be observed, watered, or their fruit tasted by the patients. Patients can view the Galileo thermometer indicating the temperature as well as the insect hotel. They can receive their friends and relatives without time or schedule constraints and can go into the garden with them as often as they desire. Visits of young children are preferably allowed in the garden. Patients can have their meal or snack in the garden whenever they wish to do so, weather permitting.
During their hospital stay, the patients did not leave the CBU at all and the patients in the G–group (see definition in the Subjects sub-section below) specifically did not go into the garden.
The methodology for creating the garden has already been published elsewhere [32]: creation of a core pilot group, organization of an accredited regional symposium; preliminary survey with an association of family caregivers of persons with AD in order to collect their observations on the behavior of patients in gardens and their expectations; a second survey in 63 nursing homes in order to list experiences, facilities and uses of their green spaces, creation of an extended work group, systematic analysis of the existing green space or garden, systematic pre-, per- and post-occupancy surveys to collect needs, wishes, expectations and satisfaction of the users of the garden: patients, visitors and professionals alike.
General design recommendations for a healing garden intended for persons treated for ADRD were applied: Avoid glare phenomena because of eye diseases associated with age-related degeneration, which can induce withdrawal and refusal to go out to the garden; a gradual transition zone in terms of lighting from inside the building to the garden along with non-reflective flooring or walkways are recommended. Compliance with hospital standards: hygiene (no standing water for example), accessibility for persons with reduced mobility. Clearly visible signs indicating access to the garden as well as from the garden back inside. Security: fences and locked gates to the outside world, while allowing free access to the garden for the patients. Careful design facilitating orientation and path finding: looped pathway with no dead ends while naturally returning patients to nurses, thus playing a reassuring role and encouraging the discovery of the various spaces, landmarks; space for social activities and for privacy and being with family. Foster a sense of security relative to behavioral and emotional aspects of the disease; it is best to avoid large empty spaces or ambiguous or distressing elements. Views: window view attracting residents from indoors to the outdoors, staff surveillance; distant views from the garden to the outside thus connecting people with the surrounding landscape and life in the city. Furnishings: well-adapted furniture, lighting, raised planting beds to allow for gardening while being seated and for horticultural therapy. Conscious choice of plants: area offering shadow, a great variety of nontoxic plants including scented plants, many of them familiar to the patients, but also including some unusual species, distinct with strong colors. Presence of water. Symbolic cues evoking common cultural references.
The principles underlying the creation of the garden combine a neuropsychological and artistic approach to the design. The latter includes a detailed analysis based on the desired impacts: 1) solicitation of the longest preserved cognitive capacities, 2) support for the most impaired capacities, and 3) soothing of psycho-behavioral disorders. These features are presented in the Supplementary Material as well as in the previously published study [33].
The designing of the Art, Memory and Life garden is based on two hypotheses (H): Hypothesis H1 according to which the therapeutic potential of a garden intended for those with ADRD can be optimized by an artistic design and artwork integrating the neuropsychological, social and cultural specificities of its users. Both dimensions of nature and art synergistically combine their effects in the garden, the latter of which can be summarized by the equation 1 + 1 > 2. Hypothesis H1 encompasses the cognitive (H1.1), psycho-behavioral (H1.2), and interaction (H1.3) levels. Hypothesis H2 postulates that hypothesis H1 is based on a common factor between nature and art which is the notion of beauty [33]. This garden, comprising a sensory-rich environment, illustrates cultural invariants and regional socio-cultural references through the integration of works of art specifically designed and adapted to the surrounding architectural setting; this approach shows respect for the person, as a cultural being, without reducing the latter to his or her illness. The garden is in stark contrast with the neutral and sanitized atmosphere of the interior of a hospital department, is propitious to social interactions, and proves to be a valuable interface conducive to the opening of the structure to the outside world. By the same token, it contributes to restoring the status of ‘citizen’ and more broadly of ‘subject’ to those treated in this setting [31]. This prototype garden is the framework and research platform of the JAZ research program [JAZ for the French term Jardin AlZheimer (Alzheimer’s Garden)] which aims to assess its impact on persons with ADRD, their relatives, and the caregivers who practice there. The JAZ program includes studies analyzing 1) the specific effects of spatial organization and 2) the vegetation and artistic elements of the garden on cognitive and emotional capacities, as well as 3) impact assessment of the garden in daily practice at the Cognitive Behavioral Unit for persons with ADRD, their relatives and the professionals who practice there [32–35 , 39].
The present study is based on the hypotheses developed and detailed in a previous publication [33], and in particular on the overall hypothesis of a specific effect of this garden in its totality, the latter constituting a central aspect of the study. The effects of using the garden on SC are notably compared with the results obtained by Arroyo et al. [17]. using musicotherapy, another non-pharmacological approach, and demonstrate the different impacts of these two approaches on SC.
Subjects
The non-inclusion criteria were common to both study phases: 1) patients having already been hospitalized at the Paul Spillmann Center and who already knew the garden, 2) a severe language impairment, 3) severe comprehension impairment with a < 1/3 success result on the three-step instruction of the MMSE [40]. The characteristics of the patients were recorded: gender, age, socio-cultural level divided into three levels (1: no studies certificate, 2: studies until high school, 3: studies continued beyond high school). Table 1 summarizes the main characteristics of the subjects of the two phases of the study.
Preliminary study: characteristics of the study groups
SCL, socio-cultural level; MMSE, Mini-Mental State Examination; FAB, Frontal Assessment Battery; NPI, Neuro Psychiatric Inventory; MT86-1α, Montreal-Toulouse Protocol 86 module 1α; GDS, Geriatric Depression Scale; SCQ, Self Consciousness Questionnaire (percentage of incorrect answers). JAZ SELF study characteristics of the G+/G-groups: G+: patients who used the healing garden, G- patients who did not use the healing garden (Means ± standard deviation). Comparison of the JAZ SELF G-/G+ groups at T0 (Chi-square test or Fisher’s exact test for qualitative variables and Wilcoxon test for quantitative variables).
Preliminary phase
Inclusion criteria were: patients hospitalized at the Paul Spillmann Center, diagnosed with Alzheimer’s disease according to the NINCDS-ADRDA criteria [41].
This exploratory study was conducted in 20 subjects.
JAZ SELF Study
Inclusion criteria were: patients hospitalized at the Paul Spillmann Center UCC between May 2016 and March 2017, diagnosed with dementia syndrome according to DSM-5 criteria [42].
Therapeutic optimization was carried out in the same manner for all patients in the G+ and G–group (see group definitions below) according to the recommendations for good geriatric practices at entry.
The life habits of the subjects with regard to gardens, from their childhood to today, were noted and the help of the family was solicited to confirm the autobiographical data. Thirty-four patients participated in this study, allocated as follows:
This duration was chosen in reference to the duration of exposure to familiar music of individuals with AD selected in the Arroyo study aimed at assessing changes in SC by the SCQ using this approach [17]. This could involve a passive use (sitting outside and contemplating the garden, etc.) or active use of the garden (walks, usual activities in the garden, etc.). Patients went to the garden, either alone or with their family or health care team. However, if before reaching the 12 h threshold, an interval of seven consecutive days without having been in the garden was found, the cumulative time was reset to zero.
Indeed, it is not possible to prohibit access to the garden when the weather conditions are favorable. The view of the garden from the living area where other patients are present motivates these patients to go to the garden and they do not accept that this access be refused to them. Such prohibited access could favor a risk of onset of behavioral disorders of the patients of the unit. In a previous study, we observed that patients treated at the CBU walked for a mean duration of 11±12 min/day when going out to the garden [36].
Method
Assessments common to both study phases
Assessment of SC using the SCQ [4]: A systematized SCQ was created by Gil et al., exploring seven aspects of SC [4, 7] (cf Supplementary Material): personal identity, anosognosia, self-assessment of affective state, body representation, prospective memory, capacity for introspection, and moral judgments. In both mild-to-moderate Alzheimer’s disease and in the temporal variant of frontotemporal dementia, this scale has enabled demonstrating heterogeneous and distinct alterations in SC [4, 16]. In addition, this questionnaire is suited for evaluating the benefits of music therapy on the SC of patients with AD [17]. Help of the patients’ entourage was solicited in order to confirm the autobiographical data. Comprised of fourteen simple questions directly asked to the patient by the person responsible for each study (preliminary phase and JAZ SELF study), the questionnaire addresses the daily life of patients as much as possible. The maximum total score is thus 14.
Assessment of cognitive and behavioral status: MMSE: Folstein’s Mini-Mental Status Examination with a maximum scale of 30 [40]; Geriatric Depression Scale (mini-GDS with 4 items) with a maximum scale of 4 [43]; Rapid Frontal Assessment battery (FAB) with a maximum scale of 18 [44]; Neuro Psychiatric Inventory nursing home (NPI-NH) behavioral disturbance scale with a maximum scale of 144 [45].
Assessments specific to JAZ SELF
Neuropsychological assessment. In addition to the above scales, the Montreal-Toulouse Protocol 86 (MT86 Aphasia Battery, module 1α) [46] was performed.
Assessment of SC. The study comprised two time intervals T0 and T1, at which SC was assessed using the SCQ: T0, within the first 48 h of admission, before any visit to the healing garden; and T1, after a minimum cumulative of 12 h in the garden over the span of two weeks for group G+ and after two weeks for group G–not using the garden.
Primary endpoint. The primary endpoint, which is the total score on the SCQ, was compared in groups G+ and G–: before and after using the garden.
Statistical analyses
Analyses were performed on the characteristics of the data, described as percentages for the qualitative variables and means and standard deviations for the quantitative variables. The parametric and non-parametric tests used included the Chi-square test or Fisher’s exact test for qualitative variables and the Student and Wilcoxon tests for quantitative variables. Comparisons of quantitative variables for both time intervals were performed using the Wilcoxon signed rank test for paired samples. Spearman coefficients were calculated to assess the association between the SC score and the MMSE, FAB, NPI-NH, mini GDS, and MT86-1α scales. The threshold of significance was set at 5%. Statistical analyses were performed with the SAS version 9.2 software package for the exploratory study and version 9.4 for JAZ SELF.
RESULTS
Preliminary phase
Socio-demographic characteristics
Socio-demographic characteristics are summarized in Table 1. The average age of the subjects was 81.8±6.6 years, the majority of whom were female (65%), along with only 15% of subjects from a relatively low sociocultural level (SCL 1). Patients were hospitalized predominantly for behavioral disorders related to the disease (55%).
Neuropsychological assessments
Patients exhibited a pronounced overall cognitive impairment (mean MMSE at 11.0±5.3) with a patent dysexecutive syndrome (mean FAB score 5.3±3.3) and significant psycho-behavioral disorders (mean NPI-NH 23.9±14.4); a depressive mood was noted in 65% of cases (mini GDS > 0) (Table 1).
Self-consciousness questionnaire (SCQ)
All patients, despite their impairments, were able to answer the questionnaire. The overall SCQ score was markedly low: 6.9±2.6 (maximum score of 14). The results by items and by dimension of the SCQ questionnaire are illustrated in Figs. 1 and 2 respectively:
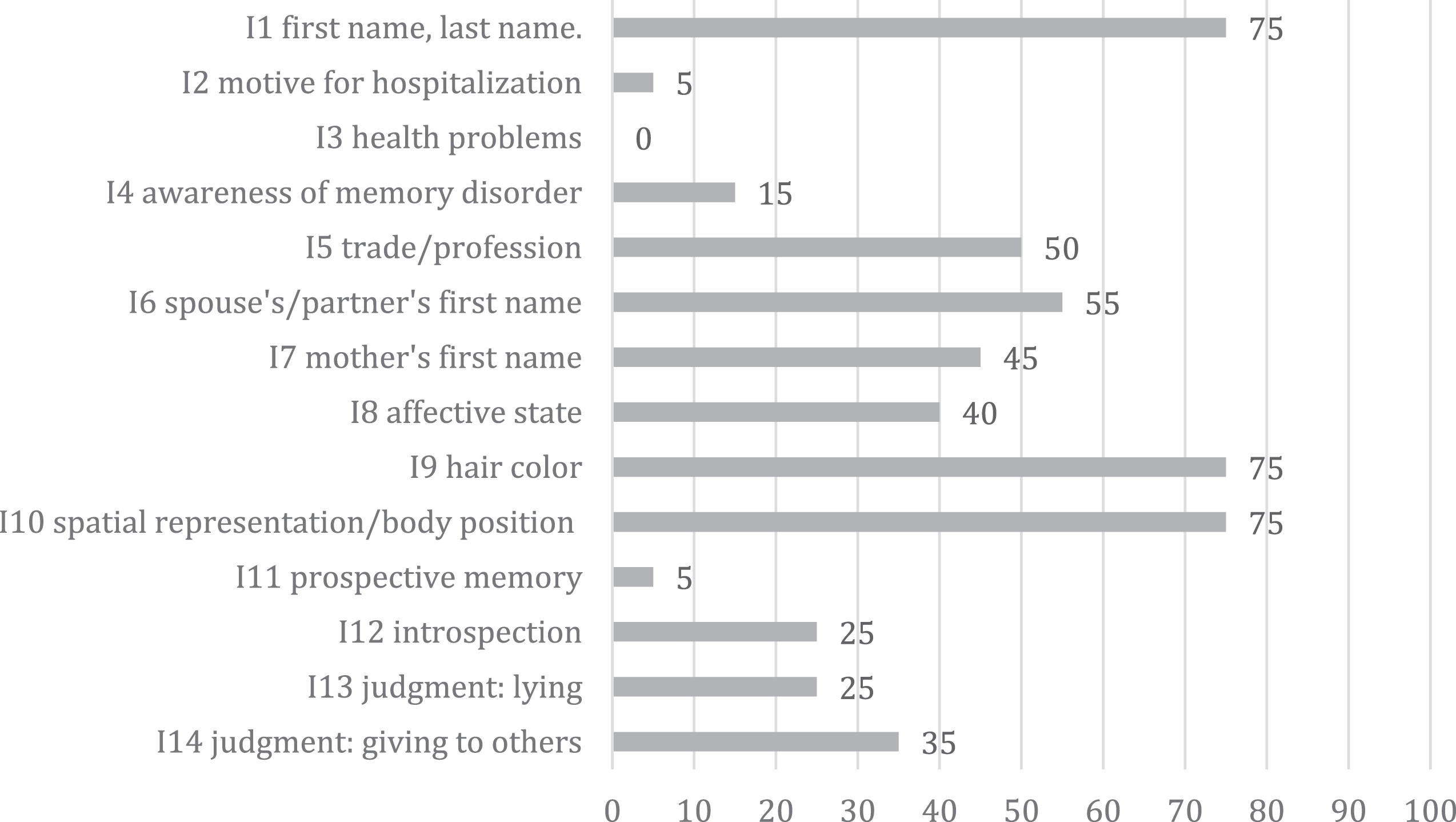
Preliminary phase (20 subjects): Percentage of correct responses to the 14 SCQ items.
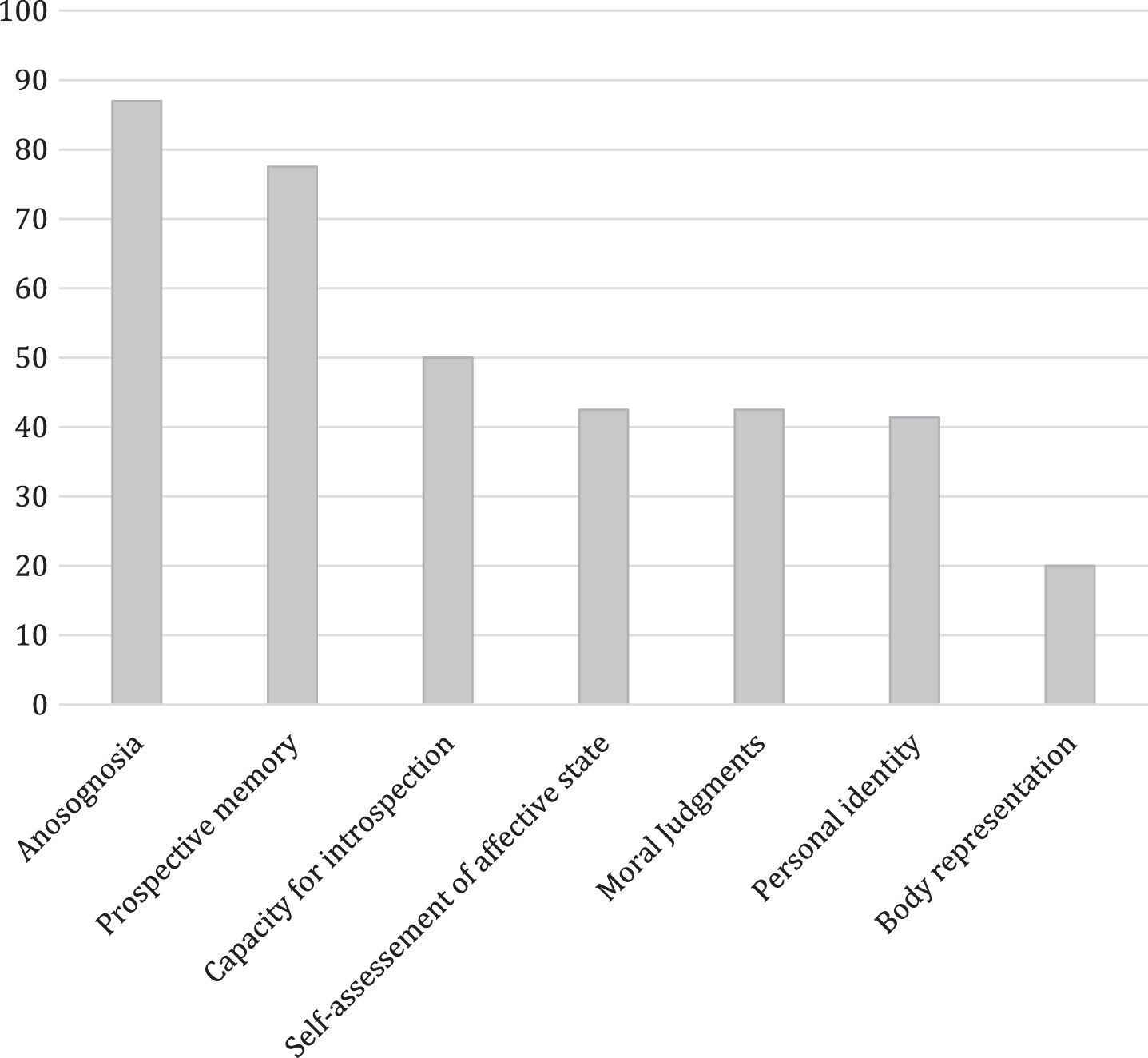
Preliminary study (20 subjects): Percentage of incorrect answers by dimension of the SCQ questionnaire. Anosognosia (items 2 + 3 + 4), Prospective memory (item 11), Capacity of introspection (item 14), Self-assessment of affective state (item 8), Moral judgments (items 13 + 14), Personal identity (items 1 + 5 + 6 + 7), Body representation (items 9 + 10).
Anosognosia (items 2–4): The maximum score for the reason for hospitalization was obtained in only 1 patient. The answer on the state of health was never correct or complete, only 15% of the patients acknowledged having memory problems/disorders on item 4.
Prospective memory (item 11): This was massively disrupted with 95% of wrong answers.
Capacity of introspection (item 12): Only 25% of patients maintained an introspective capacity and responded correctly, by justifying their choice, to the question regarding any desired changes in past life.
Self-assessment of affective state (item 8): A majority (60%) of patients were unable to recognize and express their affects.
Moral judgments (items 13 and 14): For the moral value of the truth, only 25% of answers were correct; for the second judgment dealing with mutual aid, the answer was slightly more often correct (35%).
Personal identity (items 1, 5–7): The question regarding the last name and first name of the patient had 75% correct answers, the score was never nil; half of the subjects correctly recalled the trade/profession they practiced; the first name of the spouse was answered correctly in 55% of cases, that of the mother in 45% of cases.
Body representation (items 9 and 10): The success rate for body image questions (being blond/brown, sitting or lying) was identical to that for last name and first name questions (75%). Of note, only 2 patients specified having white hair, the other responses referring to past hair color.
In summary, the percentage of wrong answers shows that the anosognosia (87%) and prospective memory (77.5%) appeared to be the most affected domains, while personal identity (41.4%) and body representation (20%) were the best preserved, with impairment in moral judgments being of the same intensity as that of the self-assessment of affective state.
In the studied group, the SCQ was not associated with either age or gender, but was significantly correlated with overall cognitive efficiency (MMSE), executive functions (FAB), and psycho-behavioral disorders (NPI-NH), but not with the presence of a depressive mood (mini GDS) as illustrated in Table 2.
Preliminary study: Correlations (Spearman coefficient) between SCQ, neuropsychological assessments (MMSE, FAB) psycho-behavioral disorder score (NPI-NH) and depressive mood score (mini GDS); rs = Spearman rank correlation coefficient and p-value for the association between the two variables. See Table 1 for abbreviations
Our study shows that the SCQ exhibited good relevance for the assessment of SC at moderate to moderately severe stages of Alzheimer’s disease. Results also revealed an elective impairment profile with the most significant impairments observed for anosognosia, prospective memory, and introspection and a relative preservation of body representation, identity, and affective state.
JAZ SELF
Socio-demographic characteristics
Table 1 summarizes the main characteristics of the JAZ SELF patients. There were no significant differences between the two groups, G+ and G–, in terms of age, gender, education level, history, treatment, disease duration, or etiology of the dementia. At admission, only visual disorders were significantly more frequent in the G + versus G–groups (100% versus 72.2%, p = 0.05). In both groups, walking autonomy was equivalent, with 10 patients walking without technical aids, 1 with a cane in group G–and 1 in group G+, 3 with a walker in group G–and 1 in group G+, and 4 patients using wheelchairs in each group.
Neuropsychological assessments
At T0: When adjusting the relationship between exposure and score for gender, the effects of healing garden exposure before, after, and during score evolution remained unchanged and no association between gender and score variables was observed in the model (p = 0.91).
There was no significant difference between the G+ and G–groups in terms of neuropsychological assessments MMSE, FAB, MT86-1α, mini-GDS, NPI-NH, and in SCQ scores (Table 1). For the group as a whole, and for group G+ and G–, the SCQ was not correlated with MMSE, frontal functions assessment using FAB, or language assessment using the MT86-1α (Table 3).
JAZ SELF study: Correlations (Spearman coefficient) between the SCQ score and neuropsychological assessments (MMSE, FAB, MT86-1α) in the entire group and in groups G+ and G–at T0 and T1. rs = Spearman rank correlation coefficient and p-value for the association between the two variables
No significant difference was observed in either mean total SCQ scores between the G+ and G–groups or between the scores for the different components of the SCQ (Table 1). The SC profiles were similar between the two groups. The most altered aspects of SC were prospective memory, moral judgments, and anosognosia, while the least disrupted aspects were affective state, identity, and body representation.
At T1: The comparison of the total SCQ score in the G–and G+ groups revealed a significant difference: G+(n = 16, T1 SCQ = 10.41 [6.49 –11.75]) versus G–(n = 18; SCQ = 7.95 6.00–9.16]), p = 0.0079.
At T1 compared to T0 (Table 4, Figs. 3 –5): The MMSE, MT86-1α, and mini-GDS scores did not show significant variations between T0 and T1, both in the G–group and G+ group. On the other hand, there was a significant decrease in total NPI-NH score between the assessments at T0 and T1, in both groups (G+ 37 versus 19 after exposure to the garden, and G–29.5 versus 15 during the reassessment). The mean improvement in NPI-NH between T1 and T0 in group G–was –11.8 points and –15.3 points between T1 and T0 in the G+ group. Comparison of the evolution of the scores between T1 and T0 in groups G + and G–showed no significant difference in NPI-NH improvement between the two groups.
JAZ SELF study: SCQ scores of groups G–and G+ and comparison of mean SCQ scores in groups G–(grey columns) and G+ (white columns) at T0 and T1
For SCQ scores (the primary endpoint of the study), a significant decrease in mean total SCQ score between T0 and T1 was observed in the G–group, and associated with an increase in anosognosia score (Figs. 3 and 4), with no significant difference for the other components of the SCQ between the two assessments (Table 4).

JAZ SELF study: Comparison of the total SCQ scores in groups G+ and G–at T0 and T1.
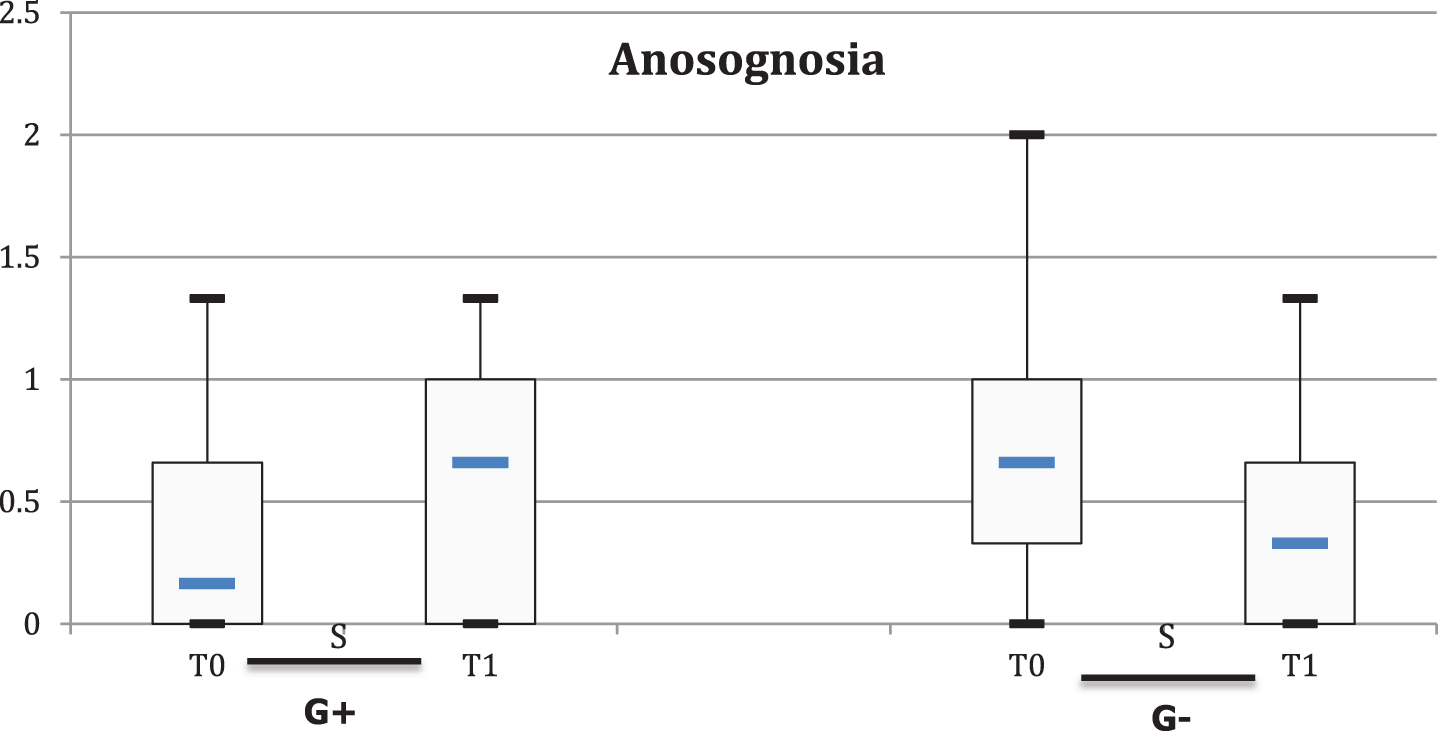
JAZ SELF study: Comparison of the anosognosia score in the G+ and G–groups at T0 and T1.
For SCQ scores in the G+ group, on the other hand, a significant improvement in total SCQ score between T0 and T1 was observed (Fig. 3). The improvement was significant for body representation (Fig. 5), while no significant difference was noted for the six other aspects of the SCQ at T1 versus T0 (Table 4).

JAZ SELF study: Comparison of the body representation scores in G+ and G–groups at T0 and T1.
DISCUSSION
Preliminary study
The SCQ was found to be applicable to all AD subjects in the present study despite the severity of cognitive and psycho-behavioral disorders. These subjects predominantly presented a depressed mood (65%) in keeping with the study of Al Aloucy and Roudier [46]. While the overall SCQ score indicated a severe impairment in SC, this score was never nil, thus confirming the accuracy and interest of this test even in severe stages of AD. The SCQ score was not correlated with the patients’ socio-cultural level. It was, however, correlated with the scores of various neuropsychological tests used herein: MMSE, FAB, NPI-NH, mini GDS. The domains of SC were affected in a heterogeneous and specific manner within the studied group: awareness of disorders (anosognosia; 87%) and prospective memory (77.5%) were those most impacted by AD at this stage of severity. These impairments are logically greater than those generally observed in the mild to moderate stages of the disease, respectively 68.9% for anosognosia and 40% for prospective memory [4].
The degree of non-awareness of the disorders or anosognosia in patients with AD varies according to different studies [47 –50]. This condition deprives the patient of a concordance with judgment of the Other and hence alters the possibility of dialogue with the latter. The severe impairment of this domain in the current study, associated with the presence of behavioral disorders, confirms the cleavage between the reality of Self and that perceived by others. Analysis of the items in this domain (item 2–reason for hospitalization, item 3–health problems, item 4–memory disorders) shows that, even when they admit to having memory problems (15%), patients do not integrate the latter as ‘health problems’ or as the cause of their hospitalization, thus confirming the dissociation [37] between recognition of disorders and appraisal of their impact in everyday life.
Prospective memory presented a degradation parallel to that of the global cognitive state. Alterations in chronological benchmarks and in the notion of duration of activities of daily living during AD have already been established [51 –54]. Intentionality weakens, in which the component of projection into the future, in the very short or medium term, escapes cognitive control [55]. The patient remains suspended in a moment of time, somewhere on the abscissa between the past as remembered or imagined and a vague present.
Introspection was also disrupted and reflects the difficulty in taking a critical, outside look at one’s own journey. This difficulty in detaching oneself from the current self is explained by a lack of interior mobility called ‘petrified self’ [13], but also likely by the limitation in working memory capacities and executive functions.
The awareness of one’s affective state was also deficient, although the score was nonetheless better than that of introspection, suggesting an easier access to one’s own affects than the capacity to distance oneself from SC.
Moral judgments in this group were more impaired than in patients with a lighter form of AD reported by Gil et al. [4]. Although the responses regarding moral judgments were progressively less nuanced in parallel with the evolution of AD, they remained correct in 40% of these patients, adequate to the social and moral norms as semantic knowledge and relatively less vulnerable to the evolution of the disease. The observation of higher scores on the self-help item than that obtained on the value of truth may surprisingly evoke a certain sparing of the process pertaining to the theory of the mind as well as a residual capacity for empathy.
Identity (41.4%): last name, first name of self and loved ones, and Body representation (20%): morphological characteristics, positioning and mobilization in space, were better preserved than the other domains, although less impaired (11.10%) than in the study by Gil et al. (6.67%) [4]. The persistence of SC according to these dimensions may again be explained by the semantic nature of the stored memories [56]. The high and identical scores of correct answers (75%) thus confer to this knowledge an element of pillars of Self, as evoked by the philosopher John Searle (1997): “Since the very beginning, since the earliest experience of perception and action, the body is central to our consciousness. My conscious experience of my own body as an object in space and time, an experience that is in fact built in my brain, is the basic element that runs through all our conscious experiences ... all consciousness begins with the experience of the body, through the image of the body” (quoted by Colman [57]).
In comparison of SCQ results obtained at the mild to moderate stages by Gil et al. [4] and the moderately severe to severe stages of AD obtained herein, we found the same profile of SC impairment: Body representation, Identity, Affective State, and Introspection were the least disrupted aspects, while Prospective Memory, Moral Judgments, and Anosognosia were the most altered domains.
Except for anosognosia and moral judgments, which were already noticeably altered as early as in the mild to moderate stages of the disease in the group of the preliminary phase, all the other domains of SC saw their percentage of incorrect answers increase to over two-fold in the more advanced stages of the disease, reflecting the progressive nature of the impairment of SC in parallel with the evolution of AD. The two founding domains of SC, which were initially the least affected, namely identity and body representation, were those that best resisted the progression of the disease.
JAZ SELF
General analysis
The two groups of patients, G+ and G–, did not differ in terms of their socio-demographic characteristics and disorders. At T0, the SCQ score was significantly and equally altered in both groups. These results are concordant with the results of the preliminary phase as well as with studies which showed an overall impairment of the SCQ in Alzheimer’s disease [4 , 13–15], but also with the evolutive pattern described above, whereby the heterogeneous alterations were predominant for prospective memory and anosognosia, while the least altered aspects were identity, body representation and introspection. This confirms the results obtained in the preliminary phase while differing from those reported in subjects with mild to moderate Alzheimer’s disease. Regarding the effect of the garden, our group of patients hospitalized in CBU presented more severe impairments than the group of ambulatory patients exposed to familiar music in the Arroyo et al. study: SCQ total score 8.6±3.4 for the G–group and 7.5±2.9 for the G+ group herein, compared to 10.11 (±2.44) for the unfamiliar music control group and 10.17 (±2.1) for the familiar music group in the Arroyo et al. study [17].
In the context of the study, there were no differences in baseline scores, i.e., before the use of the garden, between the exposed and non-exposed groups. On the other hand, a significant difference in scores was observed between the groups after the use of the garden, concomitant with a significantly different evolution of the before-after score between the two groups.
Effect of hospitalization
The destabilizing effect of hospitalization and the confrontation with an unfamiliar environment for individuals with ADRD is a common clinical observation. Our study is the first to analyze this effect via an assessment of the SC score during hospitalization. In the present study, a significant decrease in global SCQ score linked to an increase in anosognosia during CBU hospitalization was observed in group G–.
Effect of the provision of a therapeutic garden during hospitalization
A positive effect on the overall SCQ score was indeed observed in the G+ group with a significant improvement in the body representation domain. The garden as a whole represents a full-fledged environment different from the interior of the unit, capable not only of counterbalancing the deleterious effects of hospitalization on SC, but also of producing specific effects. From a qualitative standpoint, the different evolution profiles of the components of the SCQ observed both after an intervention in music therapy in the Gil et al. study and herein after using the garden argues in favor of the possibility of specific modulations of SC through different non-pharmacological approaches. Lastly, in the G+ group, the effect on SC of patients with ADRD can be considered as residual since the T1 assessment was conducted after a period of a few hours to a few days and not solely during or just after the visit of the garden.
Effect of the sensory dimension
In patients who did not go to the garden, there was a significant decline in SC during the stay at the CBU between T0 and T1. This effect was driven by the worsening of anosognosia for the G–subjects. Hence, the stay for patients who remain inside, even in an adapted environment such as that of a CBU, is not conducive to maintaining the sense of self. The question of the role of the relative adaptation to cognitive impairments of units such as CBUs thus remains unanswered: is anosognosia aggravated by this less restrictive environment than that of conventional units? Are the rhythms of life ’à la carte’ and ergonomics less ‘confrontational’ to the subject’s difficulties thus leading to less awareness and more anosognosia? Or is it rather a non-contextual intrinsic deterioration? In any event, this increase in anosognosia does not appear conducive to facilitating the subsequent return to the usual non-adapted living space.
In contrast, the use of the healing garden allowed a notable improvement in the SC of patients in the G+ group hospitalized in the CBU, who benefited from the same care as those in the G–group but used the garden, with a stabilization of anosognosia. Moreover, in a most noteworthy manner, this improvement in SC was not merely a reverse mirror of the alteration noted in group G–: in addition to stabilization of the anosognosia, a significant improvement in body representation was also observed in the G+ subjects while not found in the G–group.
Indeed, the standardized indoor hospital setting is patently poor in sensory stimulation and is detrimental for elderly people with severe neurocognitive disorders who often suffer from visual (cataract, glaucoma, etc.), hearing (presbyacusis), proprioceptive, and/or olfactory deafferentations. These individuals are thus particularly sensitive to an environment which features low sensory levels [58], ultimately generating a sensory habituation phenomena with consequences similar to those observed during sensory deprivation experiments [59]: asthenia, anxiety, depressive mood, psycho-behavioral disorders, and alterations in body representation and position in space [58 –60].
In contrast, thoughtful and systematized sensory enrichment, which is one of the design principles of the Art, Memory and Life garden, can represent an effective means to counteract these phenomena by simultaneously combining a plethora of various stimuli: olfactory (odoriferous plants), visual (wide range of colors of plants and works of art), natural elements (light, the sky), flow of water, tasting (fruit trees and shrubs) as well as proprioceptive stimuli (varieties of materials to touch: earth, plants, furniture, works art, the wind, fresh air, etc., as well as those provided by the various surfaces offered for walking—paved paths, compacted pathways, wooden walkways, lawn, etc.). We were able to show in a previous preliminary study, during reminiscence workshops with patients at the CBU, that the evocative power of a memory is not only triggered by the surrounding stimulus itself but is also dependent on the intensity of the sensory richness of the theme material [61]. Given that the sensory component of material presented on photographs was not experienced or felt but rather represented, this implies a semantic access. Thus, semantic knowledge of a sensory nature (acquired very early in development) would thus appear to remain an operative channel for memory activation, even in the advanced stages of Alzheimer’s disease.
The concomitant contemplative, sensory and proprioceptive experiences during walks in the garden probably help patients regain the awareness of their body representation and the position of their body in space. In developmental psychology, it is acknowledged that “From the moment of birth, perceptual experiences uniquely and exclusively specify one’s self, as opposed to the other physical bodies of the environment. These are polysensory experiences that generally include a proprioceptive experience that is the modality of excellence of self-perception” [62]. In the course of neurodegenerative diseases, the alteration profile in SC appears to follow a pattern that is the reverse of its acquisition. However, our results further suggest the possibility that, even in the presence of visual disturbances, the deleterious effects of hospitalization on SC may be partly counteracted by the use of the Art, Memory and Life healing garden. Thus, “the sense of an ecological self, the sense of the body as a differentiated entity, both situated and active in the environment” [62] would appear to remain mobilizable in this favorable and specifically adapted environment.
Effect of the dimension of nature
However, a garden is not merely a provider of sensory-rich stimuli. The role of contact with nature must also be considered and is seemingly superior to an artificial sensory-rich environment. Indeed, Goto et al. [63] showed that, in patients with severe dementia syndrome, the presence of an interior Japanese garden brought more benefits than that of a multisensory Snoezelen room with a 10% decrease in heart rate indicating a decrease in stress. Unlike the Snoezelen sessions, contemplation of the garden always maintained the patients awake and none wished to end the session, with some patients even asking to prolong the session. In front of the garden, they expressed more recollections than in the Snoezelen room. Another notable observation was that, when this temporary garden was removed, some patients questioned the caregivers as to the reason for its disappearance, thus testifying their interest for the latter and a certain capacity for remembrance.
Effects of the dimension of familiarity
Our study, as in the study of Arroyo-Anllo et al. [17], compared the exposure to familiar or unfamiliar stimuli: in the case of music in the latter study, a significant worsening of anosognosia was observed at three months with the non-familiar music. In our study, this deterioration occurred much more rapidly, i.e., as early as 2 weeks in group G–, with patients being at a more advanced stage of the disease on the one hand and immersed 24/24 in an unfamiliar hospital environment on the other. Conversely, exposure to familiar music allowed stabilization of anosognosia, as also allowed by the use of the Art, Memory and Life garden in our study. These two studies thus converge to emphasize the importance of the nature of sensory stimulation: only those that are personalized and familiar, such as the Art, Memory and Life garden, allow a stabilization of anosognosia. In contrast, both the unfamiliar music and the lack of exposure to a familiar natural outdoor space featuring regional socio-cultural references proved to be ineffective, and even disturbing for an unfamiliar interior environment without access to the garden. During their lifetime, most patients in the G–/G+ group lived in a house with a garden (81.3% of patients during childhood, 62.5% during adulthood). The majority of patients were from the countryside (75% lived there as children and 68.8% live there today). The comparison of these two studies thus evokes the existence of two factors influencing the anosognosia axis of SC, namely the sensory dimension and the familiarity dimension.
Effect on cognitive functions
We have already previously emphasized the role of the garden as a mediator and catalyst of communication between patients, relatives, and caregivers [34]. In the present study, in both groups at times T0 and T1, there was a significant correlation between the SCQ and the MT86-1α scores: SC is a metacognition function that borrows on the instrumental function of language; it is on this reasoning that Morin contends that ‘inner speech’ is one of the most important cognitive processes involved in acquiring information on the Self [64]. According to Morin, SC, that is “becoming the object of one’s own attention”, is in fact tantamount to “talking to oneself about oneself”. Language provides humans with a directory enabling to describe the Self and thereby represents a privileged mode of access to SC [65]. According to our results, SC is more influenced by language than by the overall cognitive efficiency explored by the MMSE.
The relationship with autobiographical memory should also be considered. Autobiographical, episodic, and semantic memories provide a foundation for a sense of identity and of continuity over time and play a crucial role in SC. The results of Piolino et al. on the effectiveness of multisensory interaction on autobiographical memory which predominates over the semantic component through the REMau program (autobiographical REMiniscence) weave a link between self-awareness, sensory enrichment provided by the garden, and autobiographical memory [66]. The activation of episodic memory, particularly via semantic memory, has been observed in the Art, Memory and Life garden [34]. Access to specific recollection facilitated by the presence of perceptual-sensory indices very similar to the encoding situation leads to the revivification of autobiographical memories [66]. The use of gardens induces recollections, reminds patients of episodic memories of moments spent in other gardens, but also activates their semantic knowledge in relation to the world of gardens. Indeed, in addition to the universal character of the experience of nature, the presence of works of art and regional cultural references [32–34 , 61] (also sources of memories), of emulation of autobiographical memory and identity, revives the coherence of the Self and mobilizes SC [67].
Effect on psycho-behavioral disorders
In both the G–and G+ groups, psycho-behavioral disorders significantly decreased during the stay at the CBU as assessed by the NPI-NH scale. However, the evolution of the SCQ score was not correlated with that of the psycho-behavioral disorders. The attenuation of these symptoms cannot therefore solely account for the favorable evolution of SC only observed in the G+ group [68].
Effect of social interactions
The role of gardens in mediating social relations has already been established [18]. In the case of the Art, Memory and Life garden, this was the first observation of the healthcare teams. The exchanges between patients, families, and/or care teams are thus facilitated. Indeed, the world of gardens and nature represent a familiar and shared canvas for all to draw upon for interaction and communication [34]. Nevertheless, SC also features a social facet: indeed, consciousness is expressed in our relationship with others, and our rapport to others is an essential counterpoint to self-awareness. The hypothesis of a role of improved social relations through the garden on the favorable evolution of SC in the G+ group can thus be envisaged, although cannot be proven given that the ‘richness of social relations’ variable during the visits to the garden was not evaluated.
The Art, Memory and Life healing garden, as expressed in hypothesis H1 of its conception, thus appears as a source of benefit in all three aspects developed in this hypothesis, namely cognition, psycho-behavioral disorders, and social interactions, all of which are able to mobilize SC and help improve the sense of identity [33].
Hypothesis H2, on the other hand, postulates that hypothesis H1 is based on a common factor between nature and art, i.e., the notion of beauty [69, 70]. Since ancient times, beauty has been linked to the notion of good according to the Greek maxim, καλος και αγαθος, and to the stereotype ‘Beauty is Good’. The study of the neural bases of the perception of beauty has established a correlation with the activity of the medial orbitofrontal cortex, irrespective of the origin of the experience of beauty. This area, located in close proximity to the medial prefrontal cortex which plays a key role in SC, may therefore be activated by the experience of beauty, whether as a result of listening to familiar music or via the Art, Memory and Life healing garden where nature and works of art are thoughtfully combined for this purpose. This hypothesis is supported by the observation of similar orbitofrontal cortex activations during attractiveness judgment tasks performed on photographs of faces along with moral judgments of hypothetical actions presented in the form of sentences as in the SCQ [71]. These distinct eco-psychosocial approaches, i.e., exposure to familiar music and the Art, memory and Life garden, both demonstrate positive effects on SC. Music as well as the Art, Memory and Life garden are potential sources of emotion, namely that of beauty. Both summon a familiar experience of interaction with the outside world, by experiencing a sense of beauty and thus promoting the resurgence of SC during ADRD. Beyond this global observation, familiar music and the garden respectively call upon different cognitive domains: body perception in the case of the garden since this environment allows the subject to interact actively through his or her motricity and to activate his or her procedural memory. For music it is more about personal identity, affective state, awareness of body representation, and moral judgments. Unfortunately, the difference in severity of the groups of patients with ADRD studied in both instances precludes concluding to a superior effect of one approach over the other. On the other hand, their combined association could eventually be considered for a stronger overall effect on anosognosia and enhance the solicitation of specific dimensions of SC.
Study limitations
This study addresses the use of the garden as a whole: given that this exploratory phase intended to ascertain the feasibility of studying the impacts of the garden on SC, we did not specifically study variables such as sunshine and activity practiced in the garden, in particular walking. These points warrant future investigation.
The small size of these studies is one of their limitations resulting in low statistical power. There was also no randomization. Being an observational study, the initial characteristics of the two groups were compared, with no differences observed between groups.
Patients who were not exposed to the garden did not leave the center. Therefore, it is not possible to attribute the entire observed effects to the use of the garden alone, since the unexposed patients should have been offered an exit other than to the therapeutic garden and under the same climatic conditions as the exposed group. However, the design of the therapeutic garden may suggest that the differences observed can be reasonably attributed, even if only partially, to this therapeutic tool. While we are unable to distinguish the individual effect of each design element on SC, exposure to the Art, Memory and Life garden should be considered in its totality; however, an analysis of each element and its potential impact is presented in the Supplementary Material.
Conclusion
Our exploratory study revealed that SC can still be explored in the advanced stages of Alzheimer’s disease and that perceptible areas of SC are preserved: to quote the campaign slogan of the France Alzheimer Association, persons with the disease can “have (AD) and (still) be here”. Such approach, inscribed in the patient-family-caregiver interrelationship, can thus contribute by a change in our view of these individuals. The SCQ also provides an appropriate tool to assess, even at these stages of the disease, the benefits of eco-psycho-social approaches on SC. Accordingly, SC was found significantly improved in the group of patients with ADRD through the Art, Memory and Life healing garden. This improvement, moreover, does not appear to result from the simple alleviation of psycho-behavioral disorders, but rather fostered through 1) sensory enrichment and the physical contact with nature, as well as 2) the dimension of contact with the living—as claimed by Wilson in the theory of biophilia [19]—provided by the garden, 3) the familiar character of this environment, 4) its scaffolding role in communication in autobiographical, episodic and semantic memory, and finally 5) its supportive effect on social interactions. Clearly observed for individuals in the advanced stages of the evolutive course of ADRD, the benefits of the garden were already apparent after two weeks of use and appeared to have a residual effect. The significant improvement observed at the level of the overall SC score is essentially driven by the restoration of body awareness, which distinguishes the latter from the reported effect on SC when listening to familiar music. Factors that can explain these benefits of the Art, Memory and Life garden on SCs are grounded in the hypotheses that spearheaded its conception and thus contribute to their validation. The sense of beauty experienced both through music as well as through the artistic dimension of a garden, can constitute a common well for patients with ADRD to draw upon to maintain their full status of genuine ‘person’. For patients living in an institutional setting, benefiting from a healing garden that meets evidence-based design principles allows reconnecting with the real world as well as maintaining ‘a focus on life’, which is an essential component of SC as described by Bergson [72].
Footnotes
ACKNOWLEDGMENTS
We would like to give a special thanks to all the patients who took part in the JAZ SELF study. We thank Pierre Pothier for his thorough translation. We thank the cross functional team of the Art, Memory and Life garden for their continuous efforts and their dedication to the vision to enhance people’s life: Hervé Bardot, Dabia Berge, Yohan Bernard, Anne Bernot, Philippe Bertrand, Dominique Capelli, Anne Chahine, Léa Chatauret, Dorothé Dhouib, Edith Clément, Jean Jacques Cœur, Laetitia Demarche, Hervé Denis, Céline Dagrenat, Olivia Deschamps, Pierre Didierjean, Marcel Dossmann, Bernard Dupont, Nicolas Fescharek, Daniel Fivet, Danièle François, Jean Pierre Frigerio, Thierry Galmiche, Pascale Gerardin, Frédéric Grosse, Eric Haubrugge, Bernd Heep, Christian Hermann, Christel Jacob, Valerie Jurin, Klemenz Kuhl, Klaus Heymann, Patrick Hennebert, Nathalie Keil, David Kozon, Michèle Jacques, Virginie Labat, Catherine Lamouille, Philippe Ledogar, Philippe Lefèvre, Michel Leturcq, Joelle Lighezzolo Alnot, Luc Mangel, Guy Marchal, Rémi Marchioni, Jean Francois Millard, Véronique Millet, Emeline Nassau, Willi Paffrath, Benoit Pericard, Michel Parrache, Christophe Petitjean, Pierre Pothier, Lise Pottier, Odile Pottier Mouton, Aline Rahnema, Yvan Renaud, Wolfgang Rink, Liliane Roux, Emilie Royant, Dominique Schondorf, Medhi Siaghy, Emanuelle Skoor, Laure Soulon, Alexandra Tesorini, Laurence Verger, Christine Vauthier, Philippe Vigouroux, Catherine Waechter, and the schools Berufliche Schule des Landkreises Marburg Biendkopf in Kirchain and Lycée Polyvalent des métiers de l’énergie et du Bâtiment Emmanuel Héré de Laxou.
The Art, Memory and lLfe garden was supported by the CHRU de Nancy, Université de Lorraine, Opération Plus de vie, Ville de Nancy, Communauté urbaine du Grand Nancy, Conseil départemental de Meurthe et Moselle, Région Lorraine, Fondation Médéric Alzheimer, Lions, ANALA, Lions Lunéville, Lions national, Club Rotary Nancy, Association Alzheimer 54, Association Jardins et Santé, Fondation Lemarchand, Fondation des Parcs et Jardins de France, Association des Chefs de service CHRU Nancy, Association JAZ Pairespective.