
Abstract
Background:
Subjective memory complaints (SMC) are a risk factor for Alzheimer’s disease.
Objective:
We aimed to explore the association between SMC and regional amyloid-β (Aβ) deposition in mild cognitive impairment (MCI).
Methods:
Sixty-eight individuals with MCI were recruited. [18F]Florbetaben PET scans were performed. T1-weighted 3D volumes were also acquired for co-registration with PET and for defining the regions of interest (ROI). Two step exploratory partial correlation analyses between SMC and Aβ deposition were performed with covariates of age, sex, education, and depression. Furthermore, for the priori ROI that had the most significant partial correlation, we investigated the correlation between the SMC and regional Aβ burden using a multiple linear regression model controlling for depression, age, sex, and education.
Results:
Significant positive correlations between the SMC and Aβ burden was found in the medial temporal ROI (first step) and in the left parahippocampus ROI (second step). In the priori left parahippocampus, we found significant correlation between the SMC and Aβ burden (R2 = 0.473, p = 0.014).
Conclusions:
Our study suggested that the SMC was associated with amyloid accumulation, especially in the left parahippocampus, in individuals with MCI.
INTRODUCTION
Mild cognitive impairment (MCI) is a transitional phase between normal aging and clinical probable Alzheimer’s disease (AD). MCI shows annual conversion rates to probable AD of around 10–15% per year, but the rates drops to 1-2% in normal elderly people [1]. It has been reported that MCI with high amyloid retention had an 82% conversion rate to AD during a 3-year follow-up [2].
Subjective memory complaints (SMC) is a self-perception of memory performance decline, which usually occurs at the preclinical stage of AD. Although one previous study reports that as many as 62% of individuals who experience cognitive decline do not report SMC [3], some individuals with MCI also have SMC, which could be the driving cause for MCI patients to visit memory clinics.
Until now, most SMC studies for individuals with the preclinical stage of AD, such as cognitively normal elderly, indicate that the SMC is associated with AD biomarkers, such as cerebrospinal fluid [4] and positron emission tomography (PET) imaging of amyloid-β (Aβ) [5–11] and tau [10], entorhinal/hippocampal volumes [12, 13], or reduction in cerebral metabolic rates of glucose [14–16] and with clinical progression [17, 18].
However, association between SMC in MCI and AD biomarkers is not clear. Therefore, we hypothesized the presence of a significant positive association between SMC and Aβ burden in the AD-related cerebral region for participants with MCI. We investigated the exploratory correlation and a fitting regression model between SMC and Aβ burden in the regions of interest (ROI) with PET co-registered using magnetic resonance imaging (MRI).
METHODS
Participants
Sixty-eight individuals with MCI were recruited from the community and from Dementia Clinic, Chosun University Hospital, Gwangju, South Korea from May 2017 to April 2018. All subjects were fully informed about study participation, and written informed consents obtained. All participants were examined by a clinical interview, which included the assessment of the Clinical Dementia Rating (CDR) [19]. The participants received a CDR score of 0.5 and met the Petersen’s criteria [20]: 1) memory complaint corroborated by an informant; 2) objective memory impairment of age, education, and sex; 3) essentially preserved general cognitive function; 4) largely intact functional activities; 5) not demented. For criterion (2), a z-score performance for at least one of attention, memory, language, visuospatial function, and frontal/executive cognitive function tests included in the Seoul Neuropsychological Screening Battery (SNSB) was below -1.5 according to the respective age-, education-, and sex- specific norms.
The exclusion criteria included any current serious medical, psychiatric, or neurological disorder affecting the cognitive function, evidence of focal brain lesions on MRI including lacunae and white matter hyperintensities of grade 2 or more on Fazeka scale [21], presence of severe behavioral or communication difficulties, or a current use of psychoactive medication.
The Institutional Review Board of Chosun University Hospital approved the study protocol (CHOSUN 2016-12-011-003) and written informed consents were obtained from all study subjects
Clinical and neuropsychological assessment
All the participants were examined by a clinical interview. Their medical history, including stroke or family history of dementia, was also assessed. Clinical diagnosis including CDR scores was made after reviewing all the available information in consensus case conferences. SMC were assessed using 14 items of the subjective memory complaints questionnaire (SMCQ) [22]. Subjective depressive symptoms were assessed using 30 items of the Geriatric Depressive Scale (GDS) [23]. Both these tests were self-administered.
Comprehensive neuropsychological assessment was performed using the SNSB II [24], which covers five cognitive domains. The attention domain was assessed by a forward and backward digit span test. The language domain was assessed by a shortened form of the Korean version of the Boston Naming Test (BNT: 15-item version, Form A). The visuospatial domain was assessed by the copying test from the Rey Complex Figure Test (RCFT). The memory domain was assessed by six measures including the Seoul Verbal Learning Test (SVLT) immediate recall (SVLTirl), SVLT 20-min delayed recall (SVLTdrl), SVLT yes-no recognition (SVLTrcg), RCFT immediate recall (RCFTirl), RCFT 20-mne delayed recall (RCFTdrl), and RCFT yes-no recognition (RCFTrcg). The frontal/executive domain was assessed by category fluency tests (animal and supermarket lists), Stroop test (Stroop_W: word reading, and Stroop_CW: color naming in color-word incongruent condition), and Trail Making Tests A and B. The global cognition was assessed by Mini-Mental State Examination.
Image acquisition
T1-weighted 3D volumes were acquired (3T, SIEMENS AVANTO) for co-registration with PET and to define the ROI. Additionally, fluid-attenuated inversion recovery images were also obtained for white matter hyperintensity reading.
PET scans were performed using a PET/CT scanner (Discovery ST PET/CT, GE) with a field of view of 250 mm, providing 3.3 mm thickness and 256×256 matrix size. The brain 3D acquisition mode was used. Images were reconstructed from the data and corrected for tissue attenuation of 511-keV gamma radiation photons. After [18F]Florbetaben injection, subjects were made to wait for 90 min, and 47-slice images were acquired over 20 min. The injected dose was 300 MBq.
Image analysis
T1-weighted magnetic resonance (MR) images were co-registered to the 90–110 min [18F]Florbetaben PET images using Statistical Parametric Mapping (SPM) 12. Co-registered MR images were segmented into grey matter (GM), white matter (WM), and cerebrospinal fluid. A GM-specific 120-region digital atlas using automated anatomical labeling [25] in native PET space was created for each participant. The individual native-space brain atlases were used to acquire regional values for the PET data. SPM 12 (Wellcome Trust Centre for Neuroimaging) software-based on MATLAB (The MathWorks, Inc.) was used to create summed PET images.
[18F]Florbetaben images were co-registered and re-sliced to their individual T1 reference image. All T1 reference images were segmented into GM and WM tissue classes using the unified segmentation algorithm of SPM12. The resultant probabilistic GM density map for each participant had a threshold of 0.5 applied to it, and a binary GM mask was created (0, no tissue, and 1, tissue with a > 50% probability of belonging to GM). The inverse nonlinear transformation parameter file from the segmentation algorithm of SPM12 was used to warp a simplified digital probabilistic atlas, consisting of 120 cortical and subcortical regions, into each participant’s native T1 space. These atlases were multiplied by the corresponding binary GM mask, which generated a GM-specific digital atlas for each participant. Raw, co-registered, and re-sliced PET and MRI data for each participant were sampled using the same individual digital atlases created previously. Mean regional standardized uptake value ratios (SUVRs) were measured for each atlas region using this method. Regional [18F]Florbetaben SUVRs were acquired by dividing each atlas region by mean value of the reference which have both cerebellar hemisphere except vermis as normalization area. Mean cortical Aβ burden was expressed as the average SUVR of the area-weighted mean of the frontal, medial temporal, lateral temporal, lateral parietal, posterior cingulate-precuneus, basal ganglia, and occipital regions [26], which were also the defined ROIs for the exploratory first step partial correlation analyses. In the present study, [18F]Florbetaben SUVR was also considered a dichotomous variable (amyloid positive or negative). Participants were classified as amyloid positive when the mean cortical SUVR was≥1.20. This threshold calculation process are as follows. We first selected four threshold SUVRs of 1.1, 1.2, 1.3, and 1.4 for amyloid positivity. And we compared numbers of amyloid positive/negative MCI subjects by four different thresholds with those by visual rating using brain amyloid plaque load (BAPL) which two experts of nuclear medicine scored. Finally, we defined the threshold of 1.2 with highest reliability (Cronbach’s alpha = 0.71).
Statistical analysis
All analyses were performed using SPSS Version 22.0 (Statistical Package for the Social Sciences, IBM, Armonk, New York). The demographic and clinical data from the two groups (amyloid positive and amyloid negative) were compared by unpaired t-test. To compare proportions and categorical data, the χ2 test was applied. Exploratory first step partial correlations between the SMCQ score and the Aβ burden were performed with covariates of age, sex, education, and a GDS score for 7 lobar ROIs including frontal, medial temporal, lateral temporal, lateral parietal, posterior cingulate-precuneus, occipital, and basal ganglia. We included age, sex, and education as covariates because they are well-known risk factors for AD dementia. Even though the participants did not report clinically significant depression, we included the GDS as a covariate because it was significantly associated with the SMC. We performed second step partial correlation analyses for the sub-ROIs of the ROI which had a significant partial correlation. Finally, we defined a priori ROI, which was the most significant ROI in the second step partial correlation analysis and performed a multiple linear regression analysis with SMC as a dependent variable and the regional amyloid burden, GDS, age, sex, and education as independent variables. For correlation analyses, the p-value was adjusted by dividing it with the number of ROIs according to Bonferroni correction for multiple comparisons. A p-value of less than 0.05 was considered statistically significant in the multiple linear regression analysis.
RESULTS
Participants
Participants with MCI who showed amyloid positivity did not show statistically significant differences in terms of age, sex, education, SMC, GDS, and neuropsychological tests compared to those who showed amyloid negativity (Table 1). However, significant difference was observed in the lobar and mean cortical amyloid burden (p = 0.001 and p < 0.001) (Supplementary Table 1).
Demographic and neuropsychological test performance for mild cognitive impairment subjects by amyloid positivity
Values (except gender and CDR) represent means (SD). Neuropsychological data presented as group mean z-scores based on age-, education-, and gender specific normative information (standard deviation). *Significant at p < 0.05 for unpaired T-tests. CDR, Global score of Clinical Dementia Rating; SMC, Subjective Memory Complaints Score; GDS, Geriatric Depression Scale Score; MMSE, Mini-Mental Status Examination; DSF, Digit Span Forward; DSB, Digit Span Backward; BNT, Boston Naming Test (15 item); RCFT copy, Rey Complex Figure Test copy score; SVLTirl, Seoul Verbal Learning Test, immediate recall score; SVLTdrl, SVLT, delayed recall score; SVLTrcg, SVLT, recognition score; RCFTirl, RCFT, immediate recall score; RCFTdrl, RCFT, delayed recall score; RCFTrcg, RCFT, recognition score; Fluency_A, Fluency score for animal; Fluency_S, Fluency score for supermarket list; TMT, Trail Making Test.
Correlation between SMC and amyloid deposition
First step exploratory partial correlation analyses between SMC and Aβ burden for 7 cerebral lobar ROIs showed that only the medial temporal ROI had significant correlation (r = 0.338, p = 0.006) (Table 2). Second step partial correlation analyses were performed between SMC and amyloid burden for the 6 medial temporal sub-ROIs, including left hippocampus, right hippocampus, left parahippocampus, right parahippocampus, left amygdala, and right amygdala. We found significant correlations in the left parahippocampus (r = 0.353, p = 0.004) and right amygdala (r = 0.339, p = 0.006) (Table 3). We defined the left parahippocampus as the priori ROI, which showed the most significant correlation. Furthermore, dividing two groups by amyloid positivity, we found more significant correlation in the amyloid positive MCI group than all MCI group (r = 0.565, p = 0.003) (Supplementary Table 2) but no significant correlation in the amyloid negative group (Supplementary Table 3) between SMC and left parahippocampal amyloid burden. Supplementary Table 4 shows medial temporal sub-regions mean cortical amyloid burden for MCI subjects by amyloid positivity. Supplementary Table 5 demonstrated lobar and mean cortical amyloid burden for amyloid positive MCI subjects by SMC positivity (Subjects were classified as SMC positive when the SMCQ score was≥6).
Correlations between Subjective Memory Complaints and amyloid burden for 7 cerebral regions of interest (ROIs)a
*indicate significant by Bonferroni correction (p < 0.007 = (0.05)/7). aEffects of age, gender, education, and Geriatric Depression Scale score were removed.
Correlations between Subjective Memory Complaints and amyloid burden for 6 medial temporal regions of interest (ROIs)a
*indicate significant by Bonferroni correction (p < 0.0083 = 0.05/6). aEffects of age, gender, education, and Geriatric Depression Scale score were removed.
Regression model between SMC and amyloid deposition
We found significant fitting regression model between SMC and left parahippocampus amyloid burden with adjusted GDS (R2 = 0.473, p = 0.014) (Table 4) (Fig. 1).
Results of regression model analysis between Subjective Memory Complaints and left parahippocampus amyloid burden with covariates of GDS, age, gender, and education
Model R2 = 0.473. Model F (2, 65) = 29.186, p < 0.001. GDS, Geriatric Depression Scale; Ab, amyloid burden.
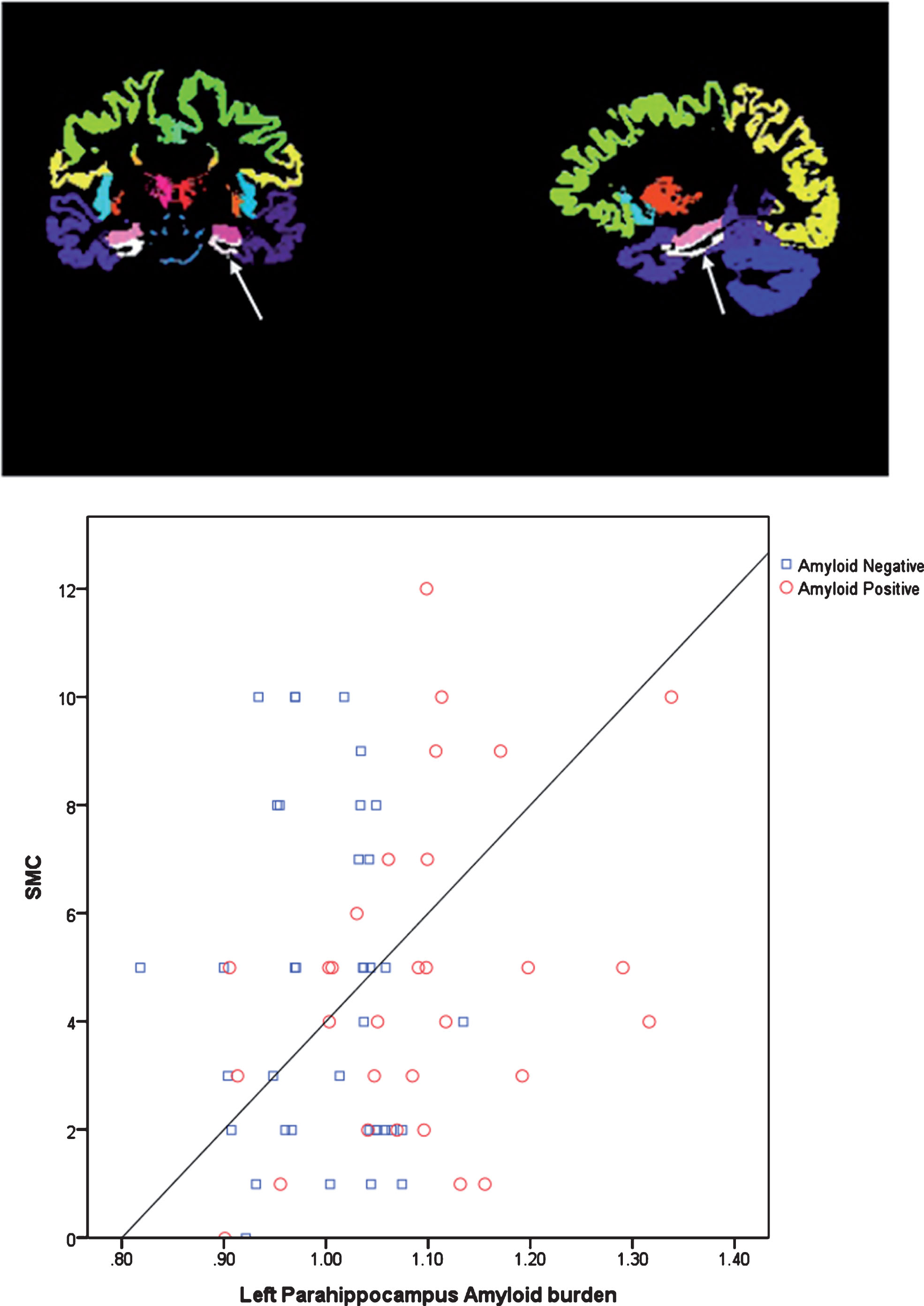
Scatterplot between Subjective Memory Complaints (SMC) and left parahippocampus amyloid burden by amyloid positivity. White arrows indicate region of interest of left parahippocampus.
DISCUSSION
In the present study, we reported positive association between SMC and Aβ burden in the left parahippocampus in participants with MCI. This association was prominent in the amyloid positive MCI group. Our result suggests that for individuals with MCI, increasing SMC could be associated with Aβ accumulation in the left parahippocampus.
Studies have reported the association between SMC and Aβ burden [5–11]. However, they included only the cognitively normal older individuals and assessed the global or lobar ROI Aβ burden. A recent study for clinically healthy older adults reported the association between SMC and entorhinal cortical tauopathy, and between SMC and Aβ deposition in the frontal or cingulate cortex [10]. Entorhinal cortex is the anterior portion of parahippocampus. It is the earliest cortical involvement in the progression of AD tau pathology [27]. In contrast, our findings showed that the greater left parahippocampus Aβ deposition is associated with increasing SMCQ score in individuals with MCI. Interestingly, although both the studies demonstrated AD-related pathology in the same ROI of parahippocampus, the former found an association between tauopathy and SMC in cognitively normal elderly individuals. The present study reported an association between Aβ deposition and SMC in individuals with MCI. These observations are in line with neuropathology literature reporting the number of plaques and neurofibrillary tangles in the entorhinal cortex is inversely related to poor memory function [28]. These findings could also suggest a potential temporal sequence of two different AD pathologies in the parahippocampus related to self-perception of cognitive worsening; correlation of SMC with tauopathy in cognitively normal individuals and with Aβ deposition in individuals with MCI. However, these cross-sectional findings should be supported by a longitudinal study. Results of longitudinal studies have demonstrated that SMC can predict clinical progression [17, 18]. It has also been suggested that the SMC progression is most pronounced among Aβ positive individuals [12].
The present study used two self-report scales of SMC and GDS. The findings about the association between left hemisphere of parahippocampus and the self-recognition scores were consistent, with a previous report suggesting that the left hemisphere has a role of an interpreter in self-recognition [29].
To overcome the limitations of the ROI method such as many regions of brain being left unexplored, the present study applied two-step partial correlation analyses. The left parahippocampus was selected as the priori ROI for the association of Aβ deposition with SMC.
We believe that this might be the first study to demonstrate a significant association model between SMC and amyloid burden in the left parahippocampus in participants with MCI.
Some limitations of the present study should be discussed. The study had cross-sectional design. The results need to be supported with longitudinal follow-ups to confirm the correlation between SMC and AD pathology. A longitudinal study has reported five times greater rate of progression to MCI or AD in cognitively normal Aβ positive individuals with higher subjective memory decline (SMD) than in those with lower SMD [12]. Another study reported that higher baseline subjective cognitive complaints predicted more rapid cognitive decline among individuals with elevated amyloid [17]. In the present study, we included only participants with MCI. However, future studies need to include individuals across the categories of cognitively normal, MCI, and mild AD dementia.
The results of the present study suggested that SMC could be associated with amyloid accumulation, especially in the left parahippocampus, in individuals with MCI.