
Abstract
Background:
Alzheimer’s disease (AD) and behavioral variant frontotemporal dementia (bvFTD) share cognitive and behavioral symptoms, such as apathy. Social cognition measurements are useful in distinguishing bvFTD from AD, but their accuracies may be affected by apathy.
Objective:
To investigate whether social cognition measurements can distinguish bvFTD from either apathetic or non-apathetic AD patients.
Methods:
Three groups of participants were enrolled in the present study: bvFTD (n = 22), AD (n = 20), and healthy controls (HC, n = 23). The AD group was divided into apathetic (n = 10) and non-apathetic (n = 10). All subjects underwent comprehensive neuropsychological examination, including the short version of the Social and Emotional Assessment (Mini-SEA), which comprises the facial emotion recognition test and the faux-pas recognition test (Faux-Pas Test). Apathy was assessed according to the Starkstein’s Apathy (SA) Scale.
Results:
The bvFTD and AD groups did not differ on global cognitive efficiency and on executive functions. In comparison to the whole AD group, bvFTD displayed lower Faux-Pas Test and Mini-SEA scores. Both AD subgroups, apathetic or non-apathetic, exhibited similar performance on all social cognition measurements. In comparison to either apathetic AD or non-apathetic AD, bvFTD patients underperformed on the Faux-Pas Test and on the Mini-SEA. The area under the curve values for the Mini-SEA total score were 0.87 (bvFTD versus AD), 0.90 (bvFTD versus apathetic AD), and 0.83 (bvFTD versus non-apathetic AD).
Conclusion:
Social cognition tests provide accurate distinction between bvFTD against either apathetic AD or non-apathetic AD. Social cognition measurements did not correlate with apathy severity.
INTRODUCTION
The differential diagnosis between Alzheimer’s disease (AD) and behavioral variant of frontotemporal dementia (bvFTD) is challenging since both AD and bvFTD share several cognitive and behavioral symptoms. Although a subgroup of bvFTD patients may present normal executive performance, executive dysfunction is considered a common feature of bvFTD [1]. Similarly, AD patients may also present executive impairment [2]. On the other hand, while episodic memory deficits are a hallmark of typical AD, nearly half of bvFTD patients can exhibit anterograde amnesia [1, 4].
Apathy may also be a confounding factor [5]. Apathy is defined as the lack of motivation or reduced goal-directed behavior [6]. It comprises a core diagnostic feature of bvFTD [7] and is frequently accompanied by other behavioral symptoms such as disinhibition and impulsivity [8–10]. Moreover, apathy is also the most frequent behavioral symptom in AD [11].
Considering how cognitive and behavioral symptoms may overlap in both bvFTD and AD, the need to find valid markers to differentially diagnose each disease is clear. Social cognition measurements have been proposed as potential markers to distinguish bvFTD from AD clinically [1, 12]. Social cognition refers to a set of different cognitive processes related to perception and interpretation of the social environment [13]. These are required abilities to adapt to different social contexts, like for appropriate interpersonal exchanges [14], which includes multiple skills and social functions such as emotion recognition, empathy, Theory of Mind (ToM), social knowledge, and mentalizing [14, 15].
bvFTD is a prototypical neurodegenerative disorder that affects the “social brain” and is characterized by socially inadequate behavior, including disinhibition and lack of empathy [7]. These behavioral alterations seem to be related to frontotemporal atrophy involving the orbitofrontal cortex, temporal poles, and some other key regions implicated in social cognition [16]. Accordingly, tests related to social cognitive abilities, such as the ToM and emotion recognition tests, have been used to diagnose bvFTD [1, 17–21]. For instance, the short version of the Social and Emotional Assessment (Mini-SEA), composed by a ToM and an emotion recognition tests, can accurately distinguish bvFTD from AD [22].
It remains uncertain whether the diagnostic accuracy of social cognition tests depends on the degree of apathy, since some abilities involved in interpersonal interaction (e.g., empathy) are affected by apathetic symptoms [23]. Due to this reason, it is important to analyze how apathy influences social cognition as some of its aspects are not automatically processed [5, 23], and motivational elements may play an important role in processing social relevant stimuli. Moreover, some apathetic features may overlap with social cognition deficits, such as loss of empathy and affective ToM deficits.
From a clinical perspective, it is not clear whether social cognition tasks can differentiate bvFTD from apathetic AD patients. We addressed this question by comparing the diagnostic accuracy of the Mini-SEA and its subtests to distinguish bvFTD from either apathetic or non-apathetic AD. Additionally, we also examined whether social cognition tests’ and apathy scale’ scores correlated. Previous data have shown that executive tests correlate with apathy severity [5]. However, whether apathy and social cognition present any relationship still remains unclear. Considering that ToM and emotion recognition abilities rely on brain structures that are severely affected in bvFTD, we hypothesized that social cognition tests hold optimal differential diagnostic accuracy between bvFTD and AD despite patient’s degree of apathy.
METHODS
This study was conducted at the University Hospital from the Universidade Federal de Minas Gerais (UFMG - Belo Horizonte, Brazil) and was approved by the local Ethics Committee. All participants or their legal representatives provided written informed consent. The present study is part of a large project on Social Cognition in bvFTD and other neurodegenerative diseases, and involves clinical, cognitive, and neuroimaging data. The main goal of this project is to investigate cognitive markers that may assist bvFTD differentiation from other disorders. We decided, retrospectively, to compare the diagnostic accuracy of social cognition measurements in differentiating bvFTD from either apathetic or non-apathetic AD.
Three groups of participants were enrolled in the present study: bvFTD patients (n = 22), patients with AD (n = 20), and healthy controls (HC, n = 23). The bvFTD patients were included according to the consensual diagnostic criteria for probable bvFTD [7]. All of them had a history of behavioral alterations including progressive impairment in personality and in social conduct. Patients with AD were selected according to the National Institute of Aging-Alzheimer’s Association diagnostic criteria [24, 25] and had a typical history of progressive episodic memory deficits.
All participants underwent careful clinical evaluation by experienced neurologists and psychiatrists in order to avoid the inclusion of patients with reversible causes of dementia and/or with psychiatric conditions that may confound with AD or with bvFTD. None of the participants fulfilled criteria for major depressive disorder according to the Diagnostic and Statistical Manual of Mental Disorders (DSM–5) [26].
Structural and/or functional neuroimaging was performed in all bvFTD and AD patients. Atrophy and/or impaired cerebral perfusion with frontotemporal or medial temporal predominance in bvFTD patients or in AD patients, respectively, was observed. We did not include patients that displayed marked vascular lesions on brain MRI (Fazekas scale higher than 1). To improve diagnostic accuracy, we followed all patients for at least 24 months and confirmed that their clinical follow-up matched their baseline diagnosis. Lastly, the HC group did not present any cognitive complaint and had no clinical history of either a neurologic or a psychiatric disorder.
Information regarding cerebrospinal fluid (CSF) AD biomarkers (total Tau, Tau phosphorylated at threonine 181 [P-Tau] and Aβ42) was available for 10/22 bvFTD and for 12/20 AD patients. CSF samples were collected by lumbar puncture and biomarkers were measured with a double-sandwich enzyme-linked immunosorbent assay (ELISA) method (Innogenetics, Gent, Belgium), as described elsewhere [27]. CSF AD biomarker profile was based upon the Innotest Amyloid Tau Index (IATI, calculated as Aβ42/(240 + 1.18×Tau)). When available, AD patients had pathological IATI score (<1), while bvFTD had normal CSF biomarker profile (IATI > 1).
All participants underwent a comprehensive neuropsychological assessment that included the Mini-Mental State Examination (MMSE) [28], the Figure Memory Test from the Brief Cognitive Screening Battery (BCSB) for visual episodic memory [29], the Frontal Assessment Battery (FAB) [30] for executive functions, Digit Span for working memory, and verbal fluency (letters FAS and animals in one minute) [31]. We used the Apathy Scale (AS) to assess apathy symptoms [32, 33]. AS scores range from 0 to 42, whereas higher scores indicate greater severity of apathetic symptoms. AS was completed by patients’ caregivers (bvFTD and AD groups), while HC answered the AS as a self-report questionnaire. Scores greater than 14 indicate clinically relevant apathy [33].
Social cognition assessment
The short version of the Social and Emotional Assessment (Mini-SEA) [34] was applied to all participants. This battery is composed by a ToM (Faux-Pas) test and a Facial Emotion Recognition Test (FERT).
The Faux-Pas Recognition Test (hereafter named as Faux-Pas Test) is composed by 10 previously published stories [35], five of which described a “faux-pas” situation (which is characterized by saying something inappropriate without realization) and five stories without faux-pas. The test is comprised of two steps [18]. In the first step, the participant is asked to listen to the story while also being provided a written copy of it. In the second step, the participant is asked questions about the story. Participants are allowed to refer to the written copy of the story when answering the questions in order to control for memory deficits.
Stories with “faux-pas” are scored out of 6. There are six questions for the stories with “faux-pas”. The first question asks about whether there was a faux-pas, e.g., “Did anyone say something he/she shouldn’t have said? Did anyone say something awkward?” If the participant answers “Yes”, there are five follow-up questions related to the elements of the faux-pas: attribution (who committed the faux-pas), identification (describe the faux-pas situation), knowledge (understanding details of the faux-pas), intentionality (why did he/she did commit the faux-pas), and empathy (how the person was feeling). One point is attributed for each correct answer (n = 6), totalizing 6 points. If the participant answers “No” to the first question, follow-up questions are not asked and a total score of 0 is attributed to the participant. Finally, two control questions about the participant’s comprehension of the story are also asked.
Stories with no “faux-pas” are scored out of 2. Two points are attributed to the participant if he/she answers “No” to the first question “Did anyone say something he/she shouldn’t have said? Did anyone say something awkward?”. There are also two controls questions checking the understanding of the story.
In sum, stories with “faux-pas” are scored out of 6, while stories without “faux-pas” are scored out of 2. The total score on the Faux-Pas Test (maximum of 40) is calculated by adding both subscores obtained from stories with “faux-pas” (five stories×6 points = 30) and the subscores obtained on stories without “faux-pas” (five stories×2 points = 10). The scores on the control questions are not considered for the total score on the Faux-Pas Test.
Previous studies that investigated the diagnostic accuracy of the Faux-pas test for differentiating bvFTD from AD [18, 34] only considered its total score. In the light of the development of more specific cognitive markers for bvFTD, it might be important to verify which ToM subcomponent is the most accurate in distinguishing bvFTD from AD. Here, we assessed whether bvFTD and AD differed on these subcomponents of the Faux-pas Test. Considering that bvFTD patients have major deficits on affective ToM [36–40], we hypothesized that intentionality and empathy subscores would be the most discriminative.
The FERT is composed of 35 images from Ekman’s database [41], representing seven different facial emotional expressions (happiness, sadness, fear, disgust, surprise, anger, and neutral). Participants are required to choose one facial emotion to each one of the presented images. During the test, each emotion is presented five times, by five different images [42]. During all the procedure, emotions are written down on labels and are shown to participants in order to avoid impaired performance due to memory deficits. Participants then choose what emotion each presented image resembles. The final score (out of 35) represents the number of facial emotions correctly identified. We report results for the overall FERT score and each emotion subscore. Previous data have shown that bvFTD perform worse than AD in specific emotions, especially anger and disgust [43].
Finally, the total score on the Faux-Pas Test is converted to a score out of 15, as previously described [18]. The total score on the FERT is also converted to a score out of 15. The total Mini-SEA score (/30) is calculated by adding the FERT (/15) and Faux-Pas Test (/15) scores, as described elsewhere [34]. Lower scores indicate higher degree of impairment.
In order to avoid circular reasoning, the results of the Mini-SEA were not considered for diagnostic purposes. The clinical diagnosis of the different groups (bvFTD, AD, and controls) was established regardless of the Mini-SEA.
Definition of AD subgroups
The AD group was subdivided into two subgroups according to the AS score. Given that scores greater than 14 indicate clinically relevant degrees of apathy [33], two AD subgroups were defined as: non-apathetic AD (score≤14) and apathetic AD (score > 14) subgroups. It was not possible to subdivide the bvFTD group by this same procedure because only one bvFTD patient was clinically classified as non-apathetic.
Statistical analyses
All statistical analyses were performed using the software SPSS 22 (SPSS Inc., Chicago, Illinois). Descriptive statistics were used to characterize groups. Shapiro-Wilk test and visual inspection of histograms determined whether variables were under a normal distribution. Variables that were not normally distributed were analyzed by non-parametric tests. Non-parametric Kruskal-Wallis test was used to compare variables across the three groups of participants. When suitable, the Mann-Whitney U-test was employed to perform two-by-two group comparisons. To measure the effect size, we calculated the value of Cohen’s d using the z-values obtained in the comparisons. Correlation analyses (Spearman’s test) were conducted in order to evaluate the effects of apathy on social cognition measurements (Faux-Pas Test total score, FERT total score, and Mini-SEA total score). We adopted Bonferroni’s correction for multiple comparisons and for multiple correlations and the level of significance (α) was finally set at 0.002.
We used binary logistic regression to investigate the diagnostic accuracy of social cognition measurements. Logarithmic transformation of the Mini-SEA total score was set as the covariate, while diagnosis was considered to be the dependent variable. The diagnostic accuracy of social cognition tests was also investigated by the Receiver Operating Characteristics (ROC) curve analyses, in which the area under the curve (AUC) was defined as a measurement of the overall performance of each test (within 95% confidence interval). Finally, we assessed whether the AUC values for each test were statistically different using a nonparametric method for independent samples (Hanley & McNeil’s method).
RESULTS
Table 1 presents demographical and clinical data of the participants. The three groups (HC, bvFTD, and AD) did not differ in terms of age, sex distribution, and educational level. Disease duration was also not statistically different between bvFTD and AD.
Demographical data for the study population (mean±standard deviation)
aSignificant difference compared to bvFTD. AD, Alzheimer’s disease; bvFTD, behavioral variant frontotemporal dementia; NA, not applicable.
HC performed significantly better than patients (bvFTD and AD) in almost all standard cognitive tests (Table 2). HC also performed better than patients on the Faux-Pas Test (total score), as well as in all of its subcomponents (detection, attribution, identification, knowledge, intentionality, and empathy). In comparison to patients (bvFTD and AD), HC displayed higher total FERT score as well as on sadness, disgust, and neutral subscores. HC and clinical groups (bvFTD and AD) did not display significant differences on happiness, anger, surprise, and fear FERT subscores. The Mini-SEA total score was significantly higher in HC than it was in clinical groups (bvFTD and AD).
Neuropsychological results (mean±standard deviation)
AD, Alzheimer’s disease; bvFTD, behavioral variant frontotemporal dementia; FMT, Figure Memory Test. aSignificant difference compared to Controls. NSNon-significant compared to bvFTD.
There were no significant differences between bvFTD and AD groups on the MMSE, FAB, categorical fluency (animals), FAS, Digit Span, and BCSB Figure Memory tests. bvFTD patients performed worse than AD patients on the Faux-Pas Test-total score (p < 0.0001, d = 1.58), as well in all of its subcomponents, except for intentionality. In addition, bvFTD and AD patients did not differ on the comprehension (control) task from the Faux-Pas Test. Compared to AD, bvFTD did not differ on FERT total score and on its subcomponents’ scores. The Mini-SEA overall score was significantly lower in the bvFTD group than in the AD group (p < 0.0001, d = 1.58). bvFTD patients also scored higher than AD individuals on the Apathy Scale (p < 0.0001, d = 1.12).
Similarly, AD subgroups (apathetic and non-apathetic) did not differ on age, sex, and disease duration. There were no differences between AD subgroups regarding standard cognitive measurements and social cognition tests.
There were no significant differences between bvFTD and non-apathetic AD subgroup for age, sex, and disease duration, and for all standard cognitive measurements. As expected, bvFTD patients scored higher than non-apathetic AD subgroup on AS (p < 0.0001, d = 2.24). In comparison to non-apathetic AD subgroup, bvFTD performed significantly worse on the Faux-Pas Test (total score) (Fig. 1B) (p < 0.0001, d = 1.63), detection (p < 0.002, d = 1.44), knowledge (p < 0.0001, d = 1.74), and empathy (p < 0.002, d = 1.3), but not on intentionality, attribution, and identification. There was no difference between bvFTD and non-apathetic AD groups on the Faux-Pas Test comprehension (control) task. Also, bvFTD and non-apathetic AD subgroup did not differ on FERT total score and on any of its subcomponents’ scores (Fig. 1 C). The bvFTD group scored significantly lower (p < 0.002, d = 1.45) than the non-apathetic AD group on the Mini-SEA test (Fig. 1A).
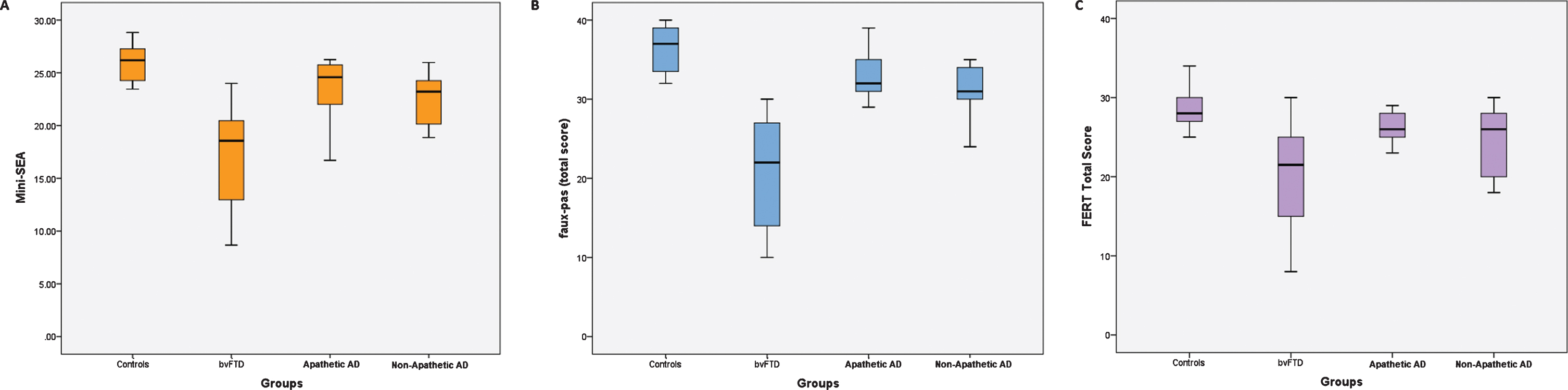
Distribution of Social cognition scores (median, quartile and range) in behavioral variant frontotemporal dementia (bvFTD) and in the subgroups of Alzheimer’s disease (AD) according to their apathy status (apathetic or non-apathetic AD). A) Performance of groups at the short version of the Social and Emotional Assessment (Mini-SEA). B) Performance of groups at the faux-pas test (total score). C) Performance of groups at the facial emotion recognition test (FERT - total score).
There were no significant differences between bvFTD and apathetic AD subgroup for age, sex, and disease duration, and for all standard cognitive measurements. Importantly, bvFTD and apathetic AD did not differ on AS score. bvFTD performed significantly worse than the apathetic AD subgroup on the Faux-Pas Test (total score) (Fig. 1B) (p < 0.0001, d = 1.51), and empathy (p < 0.001, d = 1.28), but not for detection, intentionality, knowledge, attribution, and identification subcomponents. bvFTD and apathetic AD patients did not differ on the comprehension (control) task from the Faux-Pas Test. Compared to apathetic AD subgroup, bvFTD did not differ on FERT total score and on any of its subscores (Fig. 1C). The bvFTD group scored significantly lower on the Mini-SEA as compared to the apathetic AD group (Fig. 1A) (p < 0.0001, d = 1.68).
Data for the apathy scale and for the social cognition assessment (mean±standard deviation)
AD, Alzheimer’s disease; bvFTD, behavioral variant frontotemporal dementia; Faux-Pas Test, Faux-pas Recognition Test; Mini-SEA, Short version of Social and Emotional Assessment. aSignificant difference compared to Controls; bSignificant difference compared to bvFTD; cSignificant difference compared to Apathetic AD.
Correlation analyses
We further investigated whether there was a correlation (Spearman’s test) between AS score and cognitive measurements (MMSE, FAB, FAS, FERT total score, Faux-Pas Test Total Score, and Mini-SEA score) for each clinical group (bvFTD, AD) separately. There were no significant correlations between AS score and any cognitive measurements for both groups (Supplementary Table 1).
Accuracy of the Mini-SEA to distinguish apathetic-AD or non-apathetic AD from bvFTD
We investigated the diagnostic accuracy of social cognition measurements via binary logistic regression analyses. Logistic regression using Mini-SEA score calculated bvFTD versus AD, bvFTD versus apathetic AD, and bvFTD versus non-apathetic AD accuracies to be 78.6%, 84.4%, and 81.3%, respectively.
ROC curves were employed to investigate the individual accuracy of social cognition measurements (Fig. 2, Supplementary Table 2). The AUC values for the FERT total score were 0.77 (bvFTD versus AD), 0.82 (bvFTD versus apathetic AD), and 0.71 (bvFTD versus non-apathetic AD) and were not statistically different (Hanley & McNeil’s method). The AUC values for the Faux-Pas Test total score were 0.91 (bvFTD versus AD), 0.91 (bvFTD versus apathetic AD), and 0.90 (bvFTD versus non-apathetic AD), and, once again, were not statistically different. Finally, the AUC values for the Mini-SEA total score were 0.87 (bvFTD versus AD), 0.90 (bvFTD versus apathetic AD), and 0.83 (bvFTD versus non-apathetic AD), and were not statistically different.
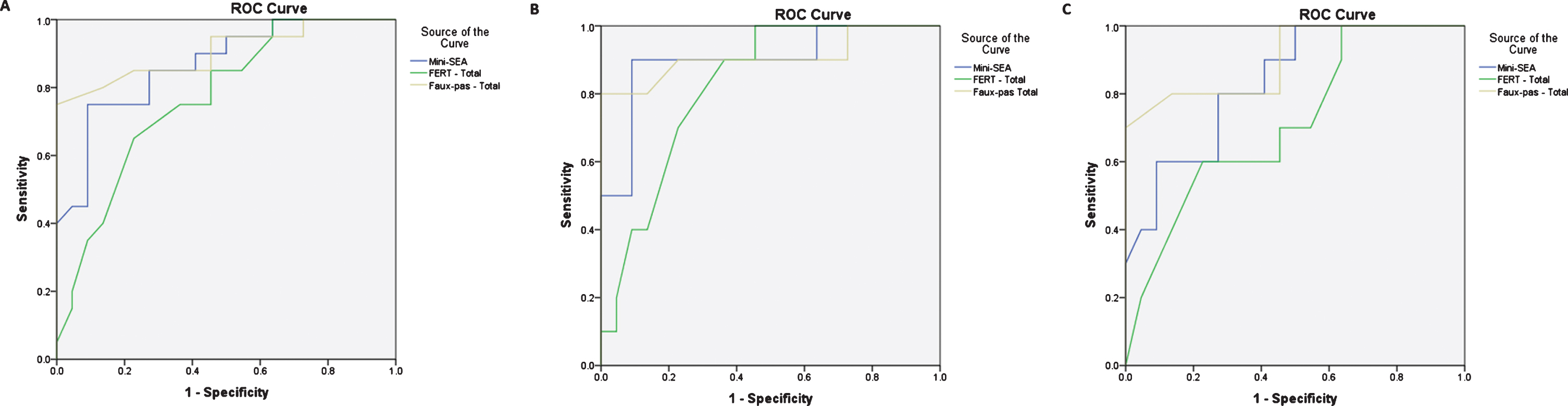
Receiver Operator Characteristic (ROC) curve for the faux-pas test (upper curve), the short version of the Social and Emotional Assessment (mini-SEA - middle curve) and the facial emotion recognition test (FERT – (lower curve) for the diagnostic distinction between: A) behavioral variant frontotemporal dementia (bvFTD) and Alzheimer’s disease (AD); B) bvFTD versus apathetic AD; and C) bvFTD versus non-apathetic AD.
DISCUSSION
Apathy is often a confounding factor in the differential diagnosis of dementia. Apathy turns the clinical distinction between bvFTD and AD difficult as it is a common symptom in both diseases [5]. Moreover, apathy can modulate the performance of cognitive tests, thus challenging the diagnostic accuracy of cognitive markers of neurodegenerative diseases. Our study found that social cognition tests (especially the Faux-Pas Test) can provide accurate distinction between bvFTD against either apathetic AD or non-apathetic AD. Interestingly, social cognition measurements did not correlate with apathy severity as assessed by AS, suggesting that these measurements are independent.
Here, we confirmed Mini-SEA’s differential diagnostic accuracy in a sample of AD and bvFTD patients matched for age, sex, education, MMSE, and executive function scores. To the best of our knowledge, this is the first investigation on Mini-SEA’s diagnostic accuracy in a non-European population. It is worth emphasizing that cultural background is a critical issue in the development of social cognition tests, as the performance relies on social norms that are often related to cultural factors [44]. We demonstrated that the Mini-SEA sensitivity/specificity still remains reliable when diagnosing bvFTD in populations from different backgrounds as those reported in previous studies [34, 45]. Therefore, the Mini-SEA may also be a valuable tool to assess social cognition deficits in culturally diverse populations affected by bvFTD.
Besides confirming Mini-SEA’s diagnostic accuracy, the present study also provides a new perspective on its clinical accuracy in distinguishing bvFTD from either apathetic and non-apathetic AD patients. The Faux-Pas Test demonstrated to have a better diagnostic accuracy than the FERT and Mini-SEA to clinically differentiate bvFTD versus AD. In comparison to other ToM measurements, such as the Reading the Mind in the Eyes and false-belief tests, the Faux-Pas Test is known to provide better diagnostic distinction between bvFTD and AD [12]. We also showed that the Faux-Pas Test provides accurate distinction between bvFTD and either apathetic and non-apathetic AD patients. Another interesting finding is that empathy score was the most discrepant subcomponent from the Faux-Pas Test in all group comparisons (bvFTD versus AD, bvFTD versus non-apathetic AD, and bvFTD versus apathetic AD). This finding may indicate that this subcomponent is related to specific social cognition processes that are affected in bvFTD. These results may be relevant for the development of novel neuropsychological tools for bvFTD clinical diagnosis.
On the contrary, we did not find significant differences between bvFTD and AD patients on the FERT and on any of its subcomponents. Previous studies found that bvFTD patients underperform on recognizing facial emotional expressions, especially those expressing negative emotions [43]. Here, bvFTD scored lower than AD patients on the FERT and on most of its subcomponents, but none reached statistical significance. The small number of patients and the strict statistical correction adopted in this study may explain these unexpected findings.
Previous studies have shown conflicting results regarding potential correlations between apathy measurements and cognitive performance in dementia. While some studies found that apathy severity correlates with executive dysfunction in AD [46] or bvFTD [47], others did not [48, 49]. In line with the latter studies, we did not find any correlation between apathy scores and executive tests in any clinical group (bvFTD or AD). Few studies have investigated the correlations between apathy and social cognition measurements in bvFTD [6, 50]. Eslinger and colleagues [47] reported that a false-belief (ToM) test and empathy scales negatively correlated with the Apathy Evaluation Scale [51]. There was no correlation between AS and social cognition tasks (FERT, Faux-Pas Test, and Mini-SEA) in our bvFTD sample. Differences on apathy measurements and social cognition assessments may account for these discrepant findings. Future research should further explore how apathy and social cognition correlate.
We must acknowledge the limitations of the present study. It would have been of value to include a subgroup of non-apathetic bvFTD patients. Actually, only one bvFTD patient in our group did not have clinically meaningful apathy. Some studies recognize two subtypes of behavioral presentations of bvFTD: patients with orbitofrontal/ventromedial involvement presenting predominant “disinhibited” symptoms, and patients with cingulate involvement manifesting an “apathetic” profile [52]. However, apathy and disinhibition usually co-occur in bvFTD [8–10] and “primary severe disinhibition” is uncommon [10], which makes it difficult to recruit a group of non-apathetic bvFTD.
Moreover, similarly to previous studies on the field [18, 53], the lack of an objective scale to assess depressive symptoms is a caveat, as depression and apathy share similar clinical features. The psychometric limitations of the AS must also be acknowledged [54]. However, it must be emphasized that: 1) all participants underwent careful clinical assessment in order to exclude depression as the cause of cognitive and/or behavioral impairment and none of them fulfilled criteria for major depressive disorder; and 2) compared to bvFTD, patients with depression underperform on the Mini-SEA, with performance similar to healthy controls [34].
An additional limitation is that neuropathological diagnostic confirmation was not available. We adopted consensual criteria and evaluated the CSF biomarkers whenever available, thus reducing the likelihood of misdiagnosis. Moreover, we followed all patients for 24 months and confirmed that the disease course matched the baseline diagnosis. Another limitation is that we did not use a multidimensional evaluation of apathy, assessing its cognitive, affective/emotional, and motor components separately. Recent data showed that bvFTD and AD patients have different phenomenological manifestations of apathy, with bvFTD patients presenting more affective apathy [37–39]. Future research may clarify the relations between social cognition deficits and specific dimensions of apathy across neurodegenerative diseases.
Finally, the small number of patients is also a major limiting factor, especially regarding the small sample of AD patients in both subgroups (apathetic and non-apathetic), thus challenging the interpretation of the results. Still, effect size analyses (Cohen’s d) support the interpretation of results. More studies including larger groups of patients as well as a more detailed investigation of apathy and its different aspects are needed.
Despite these limitations, we provide evidence to confirm the diagnostic accuracy of the Mini-SEA for the differential diagnosis of bvFTD versus AD in a population from different cultural backgrounds than those reported in previous studies. We also demonstrated that social cognition measurements, especially the Faux-Pas Test, may provide accurate diagnostic distinction between bvFTD and either apathetic or non-apathetic AD patients. Considering the cognitive and behavioral overlap between bvFTD and AD, these findings may aid distinguishing these conditions in the clinical setting.
Footnotes
ACKNOWLEDGMENTS
We thank the patients and their families for their contribution to this study.
We are grateful to Dr. Aurélie Funkiewiez (Paris, France) and to Dr. Maxime Bertoux (Lille, France) for their scientific collaboration on social cognition investigation in neurodegenerative diseases.
This study was funded by Conselho Nacional de Pesquisa Científica (CNPq), Brazil: Grant 402853/2012. ALT, LCS, MSY and PC are supported by the Brazilian National Council for Scientific and Technological Development (CNPq – Bolsa de Produtividade em Pesquisa). MVBM is supported by FAPEMIG (bolsa de iniciação científica).