
Abstract
Alzheimer’s disease (AD)-associated sequence (ADAS) of cultured fecal bacteria was discovered in human gut targeted screening. This study provides important information to expand our current understanding of the structure/activity relationship of ADAS and putative inhibitors/activators that are potentially involved in ADAS appearance/disappearance. The NCBI database analysis revealed that ADAS presents at a large proportion in American Indian Oklahoman (C&A) with a high prevalence of obesity/diabetes and in colorectal cancer (CRC) patients from the US and China. An Oklahoman non-native group (NNI) showed no ADAS. Comparison of two large US populations reveals that ADAS is more frequent in individuals aged ≥66 and in females. Prevalence and levels of fecal metabolites are altered in the C&A and CRC groups versus controls. Biogenic amines (histamine, tryptamine, tyramine, phenylethylamine, cadaverine, putrescine, agmatine, spermidine) that present in food and are produced by gut microbiota are significantly higher in C&A (e.g., histamine/histidine 95-fold) versus NNI (histamine/histidine 16-fold). The majority of these bio-amines are cytotoxic at concentrations found in food. Inositol phosphate signaling implicated in AD is altered in C&A and CRC. Tryptamine stimulated accumulation of inositol phosphate. The seizure-eliciting tryptamine induced cytoplasmic vacuolization and vesiculation with cell fragmentation. Present additions of ADAS-carriers at different ages including infants led to an ADAS-comprising human sample size of 2,830 from 27 studies from four continents (North America, Australia, Asia, Europe). Levels of food-derived monoamine oxidase inhibitors and anti-bacterial compounds, the potential modulators of ADAS-bacteria growth and biogenic amine production, were altered in C&A versus NNI. ADAS is attributable to potentially modifiable risk factors of AD associated diseases.
Keywords
INTRODUCTION
In the previous reports, I analyzed the presence of Alzheimer’s disease (AD) associated human gut bacterial sequence (ADAS) in health and diseases using the National Center for Biotechnology Information (NCBI) sequence databases [1, 2]. More recently (August-October, 2018), the new human gut metagenome Third Party Annotation (TPA) assembly derived from the primary whole genome shotgun (WGS) data set added to the human gut microbiota database [3]. The present study reveals ADAS in the new NCBI additions in human gut metagenomics. The ADAS findings based on the assumption that the biochemical pathway for the tryptamine produced by human gut microbiome and implicated in seizures and neurodegeneration can be targeted in human gut analysis with the usage of newly designed PCR primers. The tryptophan metabolite tryptamine is a dietary biogenic amine (BA) with a dose-dependent cytotoxicity [4, 5]. Tryptamine shows cytotoxicity in cell cultures at the concentrations that can be found in common food, especially fermented food. The human tryptamine content and cytotoxicity are modulated by monoamine oxidases (MAO) and monoamine oxidase inhibitors (MAOI). Elevated concentrations (2-fold) of blood β-carboline alkaloid harmane, a MAO inhibitor, were detected using HPLC in essential tremor cases [6] and in Parkinson’s disease (PD) in the study of 113 PD cases and 101 controls [7]. These data correlate with a tryptamine ability to induce tremor potentiated by MAOI pretreatment [8] and with the data on elevated (3.3-fold) urine tryptamine in PD [9]. Moreover, tryptamine is able to form β-carboline in reaction with metabolites such as peruvic acid [10]. Therefore the ADAS discovery in human gut microbiome [1] is originated from the studies of tryptamine-induced neurodegeneration in cell culture and mice [11, 12]. The PCR primers for analysis of DNA from human stool samples of AD patients and controls were designed to target the metabolic pathway that predictably related to tryptamine production in bacteria. The previous and present NCBI database analyses reveal the sequence of the resulted PCR product (ADAS) in associated diseases thus expanding our understanding of human pathophysiology. The frequent presence of ADAS in Oklahoma American Indian Cheyenne and Arapaho (C&A) population with a high prevalence of type 2 diabetes (T2DM, 50%) and overweight/obesity (∼93%); and in the populations of colorectal cancer (CRC) patients of the US and China was recently reported [2]. The seven potentially modifiable risk factors have consistent evidence of an association with the AD: T2DM, midlife hypertension, midlife obesity, physical inactivity, depression, smoking, and low educational attainment [13]. Here, the population-based fecal metabolites levels and the detectability percentage (prevalence % as a fraction above the detection limit) in C&A, in the non-native Oklahoma individuals (NNI) [14, 15], in CRC patients, and controls (Washington, DC) [16] were analyzed. The analyses of dietary MAOI exemplify this approach: MAO-A and MAO-B was found to be potently and reversibly inhibited by common natural isoflavones, genistein (more potent than the standard deprenyl) [17]. Genistein accounts for <2% of the isoflavone content of the soybean, soy proteins, and most Western soy foods including soy infant formulas [18]. Here, the fecal genistein was detected in six (4 adults and 2 children) of 23 NNI (20 adults and 3 children) with prevalence of 26% in the total population or 20% in the adult population and in 13 of 35 C&A adults (prevalence 37%). However, the mean level of detectable genistein was lower in C&A than in NNI. Genistein contents varied among the participants (4053–248115 units) with a highest level detected in the sample with a highest tryptamine level. The drugs (antidepressants) and food-derived MAOI can potentiate the tryptamine and other BA toxicity in human. Tryptamine inhibits tRNA aminoacylation of a vital protein biosynthesis enzyme tryptophanyl-tRNA synthetase (TrpRS) leading to tryptophanyl-tRNAtrp deficiency [4]. A subject who presented with early developmental delays, motor weakness, and intellectual disability and who was considered during several years as having a non-progressive encephalopathy, had mitochondrial TrpRS (mtTrpRS) deficiency. The two pathogenic variants were detected in the mtTrpRS gene WARS2 [19]. The cumulative effect of the mtTrpRS deficiency with drug valproate, a MAO A/B inhibitor [20] led to severe hepatopathy and neurological deterioration [19]. It was recently revealed that TrpRS plays an important role in high-affinity tryptophan uptake into human cells [21]. Tryptamine-treatment led to TrpRS deficiency concomitant with manifestations of neurodegeneration [12], while TrpRS hyperphosphorylation [22] and overexpression [23, 24] correlate with malignancy. Inhibition of human TrpRS expression by TrpRS-specific siRNAs decreased while TrpRS overexpression increased tryptophan uptake into the cells. Notably, the TrpRS-mediated uptake system had more than hundred-fold higher affinity for tryptophan than the known L amino acid transporter; had the promoted uptake of low tryptophan concentrations, and also very high tryptophan selectivity [21].
In order to gain more insight into the role of ADAS, the present population-based study focuses on meta-analysis of fecal metabolites associated with the presence of ADAS as a potentially modifiable risk factor of Alzheimer’s disease associated diseases.
MATERIAL AND METHODS
Statistical analyses
Statistical analysis of ADAS detection [1] was performed with Prism 7.02 software (GraphPad, San Diego, CA). Data was expressed as mean±standard deviation (SD). The groups were compared using unpaired two tailed t test. p-values <0.05 were considered significant. The initial abundance profiles of metabolites from fecal metabolomics were compared between the NNI (male/female = 14/9) and C&A (male/female = 14/24) sample groups using the non-parametric Kruskal-Wallis tests, in which p < 0.05 indicated a significant difference. The significantly different metabolites were visualized in boxplot [14]. Here, the statistical analysis of metabolites was conducted using unpaired two-tailed p value parametric (Gaussian distribution) linear regression “do not assume equal” SD t test with Welch’s correction (Welch’s test) and F test to compare variances using software GraphPad Prism version 8.1.1 (330). The differences between NNI and C&A considered significantly different at p < 0.05. The outliers were identified and removed from some evaluations using GraphPad Prism 8.1.1. Taking into account that metabolites are undetectable in some human samples, the prevalence (%) of detectable fecal metabolites of interest in C&A, NNI, CRC casesm and controls is estimated here. “Undetectable” metabolite is defined as present at the lower level than the minimum of detection by fecal metabolomics [14, 16]. The prevalence percentage for identification of the direct or inversed association between C&A and CRC populations based on analysis of ∼150 metabolites. The present metabolomic meta-analyses focus on analysis of both the level and prevalence of metabolites in fecal samples from groups with a frequent ADAS occurrence (C&A and CRC versus corresponding controls). The meaningful data on prevalence of metabolites were not analyzed in the original study of C&A versus NNI [14]. Moreover, the metabolites with a prevalence that essentially lower than 100% were excluded from statistical analysis. The special interest of the present analysis are fecal metabolites with 1) activity toward MAO, 2) food-derived anti-microbial activity, 3) activity linked to tryptamine pathway, 4) bioactive metabolites altered in C&A, obesity, T2DM, and cancer, and 5) metabolites resulted from tRNA aminoacylation activity/protein biosynthesis.
Electron microscopy
Tryptamine treatment and electron microscopy of bovine kidney cells MDBK, human neuronal cells of SH-SY5Y subline, and of mice were described earlier in detail [4, 11].
RESULTS AND DISCUSSION
The ADAS prevalence: Updated NCBI database
ADAS was searched with Basic Local Alignment Search Tool (BLAST) in healthy and diseased populations of different continents [1, 2]. The untargeted human gut metagenomics and metabolomics of AD patients are not available. Here the new data was added (Table 1) to the previously reported ADAS prevalence in the 1,246 participants from 17 human gut metagenomics studies [2].
The nucleotide sequence identity (87–100%) to ADAS as a population-attributable risk of Alzheimer’s associated diseases: an analysis of population-based data on age, geographic location, ethnicity, and health status. The NNI control for C&A contained no ADAS, the C&A contained 87% /88% (1 female and 1 male) and 100% (2 females) nucleotide identity to ADAS, Of the C&A population, the 5 individuals are ≥66 years old; the NNI population includes no individuals ≥66. Of the ADAS-comprising human sample size of 2,830 from 27 studies across four continents, the 100% ADAS identity was revealed in only 8 individuals of the entire database. The Boston male study HPFS of aged population of ≥66 and the dbGaP male and female study of 18–40 years old contained 87% /88% ADAS identity. The dbGaP sampling includes an approximately equal number of males and females; the 87% /88% ADAS identity was revealed in 3 females and 1 male in dbGaP. Thus, the 87% /88% ADAS identity is 3.3 times more frequent in females than in males from the healthy population of ages 18–40 of MO/TX, USA
*ADAS revealed in one individual of the population examined. †age: control 36–82 (SD = 11), CRC 31–89 (SD = 13.6), no statistically significant difference in age between control and CRC. **182 samples from 33 individuals, ADAS was in one of seven samples from one individual at different time points.
In the recently updated NCBI database (August-October 2018), the 14 samples with 89% identity to ADAS were revealed in Danish, Spanish, and Swedish individuals in the MetaHIT study of 760 European samples [25]. These samples collected from healthy individuals, participants with obesity, and patients with Crohn’s disease (CD) and ulcerative colitis (UC) were combined in the pangenomic study of the European population. The total prevalence of ADAS is 1.84% in the pangenomic 760 MetaHIT metagenomes of the European population. In the Spanish study (study MetaHIT-MGS), ADAS was found in one CD patient and one UC patient detected in the project PRJEB25962, in addition to four CD and three UC patients of the European study PRJEB28245. The CD and UC are types of inflammatory bowel disease (IBD). Irritable bowel syndrome (IBS) is associated with an increased risk of AD and non-Alzheimer’s dementia in patients older than 50 years in both male and female in the Chinese nationwide population-based study [26]. IBD and IBS are chronic conditions that affect the gut and are typically diagnosed in young people. IBD and IBS express overlapping symptoms such as belly pain and diarrhea. Moreover, as treatments for inflammation in IBD have become more effective, it is now apparent that ∼1 in 3 patients with IBD in remission from inflammation still have persistent abnormalities of sensation, motility, and gut microbiota, which might cause IBS-like symptoms [27]. Damage of the mucus layer is suggested as the possible shared critical common cause for both IBD and IBS [28]. Intestinal barrier dysfunction characterizes both IBS [29] and IBD [30].
In the Japanese study, the 106 participants [age: 32±11, BMI: 22±2.7 (mean±S.D.), 19–60 years old, male:female = 64:42] were recruited by Azabu University (Japan) from 2010 to 2013 [31]. The ADAS at 88% nucleotide identity was detected in seven of 106 individuals (total 6.6%): in 4 males (6.25% of males) and 3 females (7.14% of females) of ages 19–50. Among them, fecal samples were longitudinally collected multiple times at different time points. A total of 168 fecal samples were collected from the 106 individuals. In the ADAS + seven participants, this sequence was detectable in one of two; one of two; two of four; two of six; one of six; one of one; and one of one samples. The recent study described the increasing trends in AD prevalence in Japan [32] as 1.5% in 1985, 1.4% in 1992, 2.4% in 1998, 3.9% in 2005, and 7.2% in 2012 (p for trend <0.01). Japanese mortality due to CRC is also on the rise [33].
In a longitudinal analysis (DIABIMMUNE study) of the developing gut microbiome in infants from Finland, Estonia, and Russian Karelia (http://www.diabimmune.org/), ADAS was detected in one infant from Finland. The number of children included in this study (BioProject: PRJEB26925) was 74 from each country or 222 total. Inclusion criteria are positive cord blood testing for HLA DR-DQ alleles conferring increased risk for autoimmunity.
In the separate case-control study (California, USA) of 49 pregnant women (age 18 years or older), 15 women delivered preterm [34]. 89% identity to ADAS was revealed in the preterm group that included combined samples of 11 individuals.
A comprehensive metagenomic study of the fecal microbiomes from the 23 traveler’s diarrhea (TD) patients and seven healthy travelers was performed, all of which tested negative for the known etiologic agents of TD in standard tests [35, 36]. Samples were collected from adults participating in studies who had traveled from the US to Mexico, India, or Guatemala. The 88% identity to ADAS was determined in one patient with TD of unknown cause and none in the healthy travelers. The ADAS-comprising bacteria was isolated from the fecal sample of the traveler. The TD can be caused by enterotoxigenic Escherichia coli, other pathogenic gram-negative pathogens, norovirus, and some parasites. Nevertheless, standard diagnostic methods fail to identify pathogens in more than 30% of TD patients.
The new additions (WGS data set: PRJNA305507) are from the gut metagenomics study of athletes-cyclists aged 19–49 (median age 33) conducted by Jackson Laboratory (CT, USA) [37]. All participants spent a minimum of 6 h exercising per week. The 88% nucleotide sequence identity to ADAS was detected in one athlete of 33 participants (182 samples collected at different time points). Moreover, ADAS was detected in one sample out of seven fecal samples self-collected at different time points by this athlete. It seems that this ADAS-sample was not the last collected sample. The lack of ADAS in six of seven samples can be explained by regular physical activity of the athlete. The highest estimated population-attributable risk (PAR) of AD was for physical inactivity in the USA (21.0%), Europe (20.3%), and the UK (21.8%) [13]. In the human gut microbiota study, the athletes had relative increases in pathways, such as amino acid and antibiotic biosynthesis and carbohydrate metabolism [38].
In the China study, an ankylosing spondylitis (AS) patient (BioProject: PRJEB26158) contained ADAS at 100% nucleotide identity. The one sample of 32 AS patients led to two AS patients with 100% identity to ADAS with one from the BioProject: PRJEB24527. Patients with AS are at increased risk of developing IBD [39].
In the Boston follow-up study (USA) of male health professionals [3, 41] over age 65 (aged 40–75 years at enrollment, 1986), the ADAS containing sequences (87–88% ADAS nucleotide identity) were detected in 28 individuals (32 different samples) of 308 participants (9.09%) in human gut metagenome/whole genome shotgun sequence analysis (stool collection of 2012). Each sample was divided and the handling conducted using different techniques in this study (https://sites.sph.harvard.edu/hpfs/). The Health Professionals Follow-Up Study (HPFS) began in 1986. The purpose of the study is to evaluate a series of hypotheses about men’s health relating nutritional factors link to the incidence of serious illnesses, such as cancer, heart disease, and other vascular diseases. Patients diagnosed with the non-metastatic colorectal cancer (1986–2012) [42] and persons with self-reported subjective cognitive function [43, 44] are among the HPFS. Note, the age of participants at enrolment (1986) was 40–75 and became 66–101 at the time of stool sample collection (2012); the NCBI gut microbiome sequences was uploaded on 22–24 October 2018. One in 10 people age 65 and older (10%) has AD. Almost two-thirds of Americans with AD are women. Therefore, the ADAS detectability in the Boston study correlates well with AD estimations (https://www.alz.org/alzheimers-dementia/facts-figures). In the previous study [2], the four stool samples with 87% nucleotide identity (equal to 97% amino acid identity) to ADAS were found in the NCBI dataset of 300 males and females of 18–40 years old (1.3%) from the control healthy population of Houston, TX and St. Louis, MO (Table 1). This population-based control set (dbGaP study) of the Human Microbiome Project (HMP) addresses whether individuals share a core microbiome. Therefore, the Boston group of 66 and older showed higher ADAS prevalence (9.09%) than the younger USA mixed male and female group of 18–40 years old (1.3%), the younger Japanese group of age 32±11 (6.6%), and the European 760 MetaHIT pangenomic group (1.84%). The dbGaP sampling includes an approximately equal number of males and females. The 87/88% ADAS identity was revealed in the 3 females and 1 male in dbGaP. Thus, the 87/88% ADAS identity is 3.3 times more frequent in females (2%) than in males (0.6%) in the healthy population of age 18–40 in MO/TX, USA. In the Boston male group of ≥66, the frequency of 87/88% ADAS is 15.15-fold higher than in male group of 18–40 from TX/MO, USA.
Human gut metagenomics of 24 healthy human subjects (22 and 38 years of age) was conducted by University of Nebraska (Bioproject PRJNA324129) with the primary objective to determine acceptability and safety of Bifidobacterium longum subsp. longum AH1206 at a daily dose of 1010 cells [45]. ADAS was determined in samples collected at pre-treatment (baseline), after probiotic consumption, and around 200 days after consumption in one individual. Therefore, the B. longum AN1206 bacteria showed no impact on the ADAS presence in one of 24 individuals.
In the Chinese study of 10 pairs of infant twins, the gut DNA sequence of one twin showed 88% nucleotide/96% amino acid identity to ADAS [46].
Summarizing, the present additions of ADAS with cases of CD and UC (760 individuals, Europe); preterm birth (49 pregnant women, CA, USA); traveler’s diarrhea of unknown cause (30 individuals - patients and controls); health professionals of Boston metropolitan area (308 participants, USA); three-countries study (222 infants, North Europe); healthy individuals (106 adults, Japan); athlete-cyclist (33 participants, USA); healthy human subjects consumed Bifidobacterium (24 individuals, Nebraska, USA); Chinese case/control study of ankylosing spondylitis (32 AS patients); and Chinese infant twins study (20 participants) led to ADAS-comprising human sample size of 1,246 in the previous report [2] with 1,584 in the present report = 2,830 from 27 studies of four continents including North America (US and Canada), Australia, Asia (China and Japan), and Europe. The Table 1 shows a prevalence of sequence identity (87–100%) to ADAS as a population-attributable risk (PAR) of Alzheimer’s associated diseases.
In oral microbiome of saliva and dental samples, a 55% of amino acid identity to ADAS was detected in four (no correlation with disease) out of 266 individuals of Chinese study (controls and rheumatoid arthritis patients aged 23–74 years) [47] and no significant identity to ADAS was detected in oral cavity in the US study dbGaP in the NCBI dataset of 300 males and females of 18–40 years old from the control healthy population of Houston, TX and St. Louis, MO (PRJNA48479). Therefore, no ADAS was revealed in human oral microbiome of at least 566 individuals from two continents.
Population-based analysis of metabolomics attributable to ADAS presence: Binding and kinetics for tryptamine, MAO, MAOI, and TrpRS
Prevalence of tryptamine is higher in C&A and CRC versus controls (Supplementary Table 1). MAO-A and MAO-B contribute to the catabolism of BA including tryptamine. MAO, a mitochondrial enzyme, oxidizes BA to generate hydrogen peroxide, a major source of oxidative stress. Both MAOs are composed of an flavin adenine dinucleotide (FAD)-binding domain [48]. The influence of inhibitors such as pirlindole (pyrazinocarbazole) on the redox co-factor FAD is a key factor in the MAO inhibition. The data suggest that FAD is a preferred substrate and an inhibitor, suppressing the activities of bacterial NAD(P)H:flavin oxidoreductase at low NADH concentrations [49]. Prevalence of FAD is directly associated with CRC and inversely associated with C&A (Supplementary Table 1). Nevertheless, the FAD level is significantly higher in C&A than in NNI [14]. Here, the FAD is 1.49-fold higher (Fig. 1) in C&A than in NNI (t test p value 0.0032**, F test p value 0.0108*). Therefore, the FAD level would not limit the MAO activity in a majority of C&A individuals. However, levels of many BA are higher in C&A versus NNI (Fig. 1). The magnitude of TrpRS inhibition by tryptamine in vivo depends on kinetic parameters of TrpRS inhibition and MAO oxidizing activity toward tryptamine. Chronic administration (s.c. via Alzet osmotic minipumps) of MAOI antidepressant drugs (daily doses: tranylcypromine.HCl, 0.5 and 1.0 mg kg–1; phenelzine sulfate, 5 and 10 mg kg–1, each for 28 days; clorgyline.HCl, 1.0 mg kg–1; (–)-deprenyl.HCl, 1.0 mg kg–1, each for 14 days) to rats resulted in decreases in [3H]tryptamine binding site density in brain cortical membranes [50]. The tryptamine MAO Km [51] and TrpRS Ki values support that tryptamine inhibition of TrpRS can be more efficient than tryptamine oxidation by MAO especially in the presence of MAOI. Taking an initial symmetrical dimeric TrpRS protein the two dissociation constants (KD) for tryptophan at pH 8; 25 C are respectively K1 = 2.0±0.5μM and K2 = 10±4μM. They are respectively K1 = 1±0.25μM and K2 = 20±8μM if one considers a sequenced binding of the two tryptophan molecules [52]. The bovine pancreatic TrpRS Ki for tryptamine is 6×10–7 M or 0.6μM [4]. In medial frontal cortex of human brain the [14C]tryptamine binding was at the KD value of 5μM [53]. In bovine liver MAO B, tryptamine was ‘partially immobilized’ with a KD of 39μM and 2.2 moles bound per enzyme dimer [54]. These estimations may indicate that tryptamine has higher binding affinity to TrpRS than to MAO assuming that the smaller KD values correspond to the greater binding affinity of the ligand for its target. To determine the stability of tryptamine for potential TrpRS inhibition in vivo it is important to estimate the rates for tryptamine as TrpRS inhibitor and as MAO substrate. In vivo, the E. coli codon GAA was found to be translated with a rate of 21.6 codons/s whereas codon GAG was translated 3.4-fold slower (6.4 codons/s) [55]. Kinetic measurements indicated that the half-life for tryptamine ranges from 0.28 min (16 s in rat brain) to 1.6 min (96 s in rat spinal cord) [53]. In rabbits, radiolabeled iodinated [131I]tryptamine rapidly entered the brain (olfactory bulb and olfactory peduncle) and was completely excreted in the urine 20 min after injection in the marginal ear vein [56]. Thus, tryptamine can lead to Trp codon translation blockage even without MOAI. Unexpectedly, radiolabeled N,N-dimethyltryptamine (DMT) remained in the rabbit brain for at least 7 d after injection. DMT is a potent hallucinogen and an endogenous agonist for the sigma-1 receptor [57]. DMT is a direct metabolite of tryptamine. The DMT degradation by MAO is inhibited by β-carbolines, the reversible MAOI [58]. A significant acceleration in the slope of cognitive decline occurs following an episode of delirium in AD patients [59]. The rate of polypeptide chain elongation in prokaryotes is 4–10 times faster than in eukaryotic cells [60]. On that account, the tryptamine-induced TrpRS-dependent blockage of Trp codon translation may be more pronounced in prokaryotes than in eukaryotes. Tryptamine can lead to dysbiosis in the gut by killing tryptamine-sensitive bacteria.

The population-based statistical analysis of the fecal metabolites for NNI and C&A: correlation of gut metabolites with ADAS occurrence. The metabolomics crude data for NNI and C&A are derived from the Oklahoma study [14]. The 23 NNI (20 adults and 3 children) and 35 C&A adults are included in Oklahoma metabolomic study and all available data for all subjects from this study are analyzed here. The comparison of fecal metabolites from C&A containing 87% and 100% nucleotide identity to ADAS was with the NNI group of no ADAS. Here, the mean data with SD is presented in the graphs built with software GraphPad Prism 8. The outliners identified with this software usage are shown in parenthesis. Panel H shows comparison of the total 81 peptides with the tryptamine (T) level in NNI and C&A. The tryptamine high level correlates with a low level of the total peptides; T high samples (NO1 and NO13) versus T-low (NO2) and non-detectable (ND) tryptamine (NO7 and NO15) of the NNI group.
The MAO enzymes are proteins localized mainly on the outer membranes of mitochondria [61, 62]. Thus, MAO may not present in the cytoplasm in large amounts sufficient to prevent inhibition of the cytoplasmic protein biosynthesis by BA. Nevertheless, the BA can be degraded by MAO on mitochondria and after MAO biosynthesis on the cytoplasmic ribosomes since MAO is encoded by nuclear genes. The genes controlling the expression of MAO A and MAO B are located on the human X chromosome [63]. Semicarbazide-sensitive amine oxidase (SSAO), widely distributed in highly vascularized mammalian tissues, metabolizes endogenous and xenobiotic aromatic and aliphatic monoamines. Widespread SSAO distribution was observed in all tissues except the thyroid gland and endocrine pancreas, which were devoid of specific SSAO immunoreactivity. In most tissues, SSAO immunoreactivity appeared to be bound to the cytoplasmic membrane [64].
Portal hypertension, circulatory anastomosis, liver bypass, diversion of portal flow of intestinal blood to the systemic circulation, collateral vessels (varices), and fistula
In the previous report, we discussed the possible anatomical routes for tryptamine from the gut microbiome to systemic circulation avoiding degradation by MAO [2]. Here, more detailed analysis of anatomical predispositions suggested for the gut microbiome-produced BA distribution in human organs. Biogenic amines can escape from the MAO-catalyzed degradation in liver by the liver bypass due to the circulatory anastomosis such as portacaval anastomosis. Portacaval anastomosis is a veno-venous anastomosis between a vein of the portal circulation and a vein of the systemic circulation, which allows blood to bypass the liver in patients with portal hypertension, often resulting in hemorrhoids, esophageal varices, or caput medusae. Portosystemic collateral pathways (also called varices) develop spontaneously via dilation of pre-existing anastomoses between the portal and systemic venous systems. Hypertension is produced by biogenic amines tryptamine, tyramine, and phenylethylamine [65–68]. Tryptamine produced vasoconstrictor and vasodilator responses in rat-isolated perfused mesentery vasculature [69]. Histamine produces the hepatic portal vasoconstriction at 0.5–1μg (causes rise in vascular resistance) and the hepatic arterial vasodilation at 50–100 ng [70]. Histamine injection (10 ml in a dilution of 1μg/ml) via the cannulated portal vein significantly raised the portal pressure (mean 2.25-fold, p < 0.001) in ten normal volunteers [71]. Angiographic study showed that histamine induced intrahepatic portal vasoconstriction in the normal controls. A similar change was obtained in the schistosomal group (parasitic flatworms hepatic fibrosis), particularly on the periportal neovascular formation [71]. In patients with hepatosplenic schistosomiasis (8 patients) and controls (7 volunteers), standing heart rate was 60–110 versus 68–74 beats min–1; systolic 105–150 versus 100–120 mm Hg and diastolic blood pressure - 60–90 versus 60–80 mm Hg, respectively [72]. Study of cardiac dysfunction in cirrhotic portal hypertension revealed that left ventricular diastolic dysfunction is commonly associated with advancement of hepatic dysfunction while systolic function is maintained till advanced hepatic failure [73]. Cirrhosis with portal hypertension is associated with increased heart rate.
Tryptamine, infused intravenously in man (4 patients of the National Institute of Mental Health Addiction Research Center, Lexington, KY, USA), facilitates the patellar reflex, dilates pupils and elevates blood pressure (maximal difference between infusion and pre-infusion data for diastolic blood pressure was ∼45 mm of Hg). It also causes changes in vision and hearing, as well as nausea, vomiting, dizziness, sweating, and heaviness of body [74]. The tryptamine infusion rates varied from 0.025 to 0.364 mg/kg/min, and periods of time varied from 2 to 7.5 min. The total amounts of tryptamine administered during an experimental day ranged from 23 to 277 mg. Maximal rates and times of infusion were determined by the patient’s ability to tolerate the infusion. The control tryptamine excretion in the urine was found to be 0.1 mg/24 h. For the Austrian population, the fresh/cooked fish, preserved fish, cheese, raw sausage, condiments, sauerkraut and fermented tofu maximum tolerable levels were 1,650, 3,200, 2,840, 4,800, 14,120, 1,740, and 2,400 mg kg–1, respectively. For beer, the maximum tolerable limit of 65 mg kg–1 included an uncertainty factor of 10 [75]. A tryptamine dose without effect of 8 mg kg–1 body weight day–1 was derived from literature data. In rats, the i.v. administration of tryptamine (20 mg/kg) induced clonic seizure [76]. Tryptamine-induced (40 mg/kg, administered via the tail vein) clonus of the forepaws was observed in 100% of the animals (20 rats) [77]. Tryptamine-induced clonic seizures are studied at the dose 40 mg/kg in rats (bilateral clonic seizures of the forepaws were observed for a period of 5 min after tryptamine intravenous injection [78]. In our study, convulsions were induced in Balb/c mice by intravenous injections of tryptamine at dose 40 mg/kg of weight [11]. Increase of urine tryptamine from ≤120μg/24 h (normal) to 900μg/24 h in the patient was demonstrated during MAO inhibition [79].
According to the Mayo Clinic, hemorrhoids are very common. Nearly three out of four adults will have hemorrhoids from time to time. Rectal varices and their relationship to hemorrhoids presented in patients with portal hypertension [80]. Elevated venous portal pressure is an important factor in patients having severe hemorrhoidal bleeding [81]. Portal systemic encephalopathy is a neuropsychiatric disorder that occurs secondary to chronic liver disease. The vein most affected is the portal vein, which contributes 75% of the blood to the liver. To eliminate the high pressure in the portal vein caused by the reduced blood flow, the portal vein develops collateral vessels that bypass the liver and drain directly into the inferior vena cava. Almost any vein in the abdomen may serve as a potential collateral channel to the systemic circulation [82]. Although varices of the gastroesophageal axis are most often the cause of clinical concern in patients with portal hypertension, varices in other locations have been frequently reported [83]. Swollen portasystemic collateral vessels have been found in the duodenum, small bowel, and colon, at intestinal anastomoses and stomas, on the abdominal wall, and in the rectum at the so-called hemorrhoidal plexus [80]. When blood is not cleared, or when hepatic functioning fails, toxins accumulate in the circulation and affect the central nervous system [84]. The normal hepatic venous pressure gradient (HVPG) value is between 1 to 5 mmHg. Pressure higher than this defines the presence of portal hypertension, regardless of clinical evidence [85]. The portal hypertension (defined as HVPG ≥10 mmHg) marks the progression to a stage of clinical complications. Diagnosed cirrhosis and portal hypertension might regress after removing the etiological factor causing disease [86]. In the patient with senile dementia and no evidences of portal hypertension, a meso-caval shunt was found in the right lower abdomen. Superior mesenteric arteriography revealed a shunt flowing into the inferior vena cava via the right gonadal vein. The shunt was closed by balloon, and dementia-like symptoms improved [87]. The brain lesions of patients with chronic portal-systemic venous shunts were much the same regardless of the presence or absence of primary liver disease. Alzheimer-type abnormality of astrocytes and areas of spongy degeneration (multiple vacuoles) were found [88]. An autopsy case of portal systemic encephalopathy and senile dementia of the Alzheimer-type coexisting was described [89]. A heterogeneous distribution for the tryptamine binding site was observed in hippocampus⪢frontal cortex = caudate nucleus > temporal cortex = cerebellum. When comparing [3H]tryptamine binding site densities in control brain tissue with that in brain tissue from patients with hepatic encephalopathy (HE), significant decreases in densities were observed in the frontal cortex (by 56%, p < 0.001), hippocampus (by 43%, p < 0.001), and caudate nucleus (by 41%, p < 0.01) of the HE group. Binding site affinities were within normal limits. The findings of decreased densities of [3H]tryptamine binding sites taken in conjunction with reports of increased cerebrospinal fluid and brain tryptamine concentrations in HE suggest a pathogenic role for this neuroactive amine in HE resulting from chronic liver failure [90]. Congenital portosystemic venous shunts are rare vascular anomalies resulting in diversion of portal flow to the systemic circulation. They allow intestinal blood to reach the systemic circulation bypassing the liver, resulting in a variety of symptoms and complications in the longer term, although asymptomatic cases, discovered incidentally on imaging, are not uncommon [91]. The BA produced by gut microbes can avoid degradation in liver by spreading through the gastrointestinal fistula, which can be formed due to paraproctitis [92]; inflammatory bowel diseases, such as Crohn’s disease [93]; diverticulitis [94]; abscess [95]; or spontaneously [96]. In three-dimensional (3D) cell culture, the vascular anastomosis occurs between sprouts formed by angiogenesis and tubes formed by vasculogenesis [97]. Vasculogenesis is the process of new blood vessel formation during embryonic development of the cardiovascular system whereas angiogenesis is the process by which new blood vessels take shape from existing blood vessels by “sprouting” of endothelial cells.
In our studies, the cytotoxic concentrations of tryptamine stimulated the angiogenesis in hippocampus of mouse brain [98] and outgrowth of neuronal processes with neurodifferentiation in human cell culture [12]. The endothelial cell tube formation and sprouting are dependent on two essential processes in angiogenesis, endothelial cell migration and differentiation, while the synergistic inhibition of endothelial cell proliferation, tube formation, and sprouting can be induced by cytotoxins [99]. In the 3D collagen gel culture, we demonstrated that tryptamine (5μg/ml or 30μM; 25 and 100μg/ml, bell-shaped concentration-dependence with optimum at 25μg/ml or 0.15 mM) potentiates the capillary-like tube formation by human umbilical vein endothelial cells (HUVEC) when cultured in the presence of hepatocyte growth factor (HGF) and vascular endothelial growth factor (VEGF)-165 at 100 ng/ml each (data not shown). Tryptamine itself had no direct effects on the processes of angiogenesis in this procedure. The VEGF isoform VEGF-A(165) and HGF stimulate mitogen-activated protein kinases and focal adhesion kinase. This study demonstrated that under angiogenic conditions, combining VEGF-A with HGF can promote neovascularization by enhancing intracellular signaling [100]. Similar to tryptamine [12], histamine induces neural stem cell proliferation and neuronal differentiation [101]. Data showed that another BA histamine (0.1, 1, 10μM) itself was absent of direct effects on the processes of angiogenesis, including the proliferation, migration, and tube formation of endothelial cells. Nevertheless, it could concentration-dependently enhance basic fibroblast growth factor (bFGF)-induced angiogenesis as well as production of VEGF from endothelial cells [102].
Nonalcoholic fatty liver disease (NAFLD) is a major cause of liver disease worldwide. Global prevalence of NAFLD is 25.24% with highest prevalence in the Middle East and South America and lowest in Africa. Metabolic comorbidities associated with NAFLD included obesity, T2DM, hyperlipidemia, hypertension, and metabolic syndrome [103]. There is evidence that portal venous pressure may begin to rise in the earliest stages of NAFLD when fibrosis is far less advanced or absent [104]. The presence of ADAS was earlier reported in fecal samples of NAFLD patients with obesity [2]. Idiopathic portal hypertension is characterized by a long-standing presinusoidal portal hypertension of unknown etiology in adults. Some unidentified agent(s) affect(s) the intrahepatic small portal veins or portal tracts [105]. A France 2008-13 nationwide retrospective cohort study concluded that alcohol use disorders were a major risk factor for onset of all types of dementia, and especially early-onset dementia [106], while alcohol is a neurotoxin inducing liver and brain damage [107].
Prevalence of fecal metabolites in C&A and CRC
ADAS was found in 4 of 35 C&A individuals [2], while in the gut metagenomics of 23 control rural Oklahoma non-native individuals [15], no ADAS was detected by BLAST analysis of the BioProject Sequence Read Archive (SRA) PRJEB13051.
Approximately one third of CRC patients had at least one comorbidity, with cardiovascular disease and T2DM being most common [108]. CRC is the second most common cancer among American Indians. Comparing the epidemiological data on CRC and AD, it was found that CRC and AD have similar epidemiologic feature; both diseases correlate with high prevalence of constipation [109]. This correlation supports a role of gastrointestinal conditions in the pathogenesis of AD.
The detectability as a prevalence of fecal metabolites are varied among participants. In many if not most metabolomics, statistical analyses are conducted for the metabolites with a high prevalence close to 100%, while the metabolites of lower prevalence are frequently unnoticed. However, the prevalence (%) as a fraction above the detection limit can be instrumental in the analysis of comparatively rare samples. Here the prevalence of 132 fecal metabolites are compared between C&A and CRC with a special focus on the food-derived metabolites with MAOI activities, anti-microbial activities, tryptamine pathway, metabolites reflecting protein biosynthesis/proteolysis/tRNA aminoacylation, known signaling molecules, cytotoxic metabolites, and disease-related compounds. In this study, prevalence (%) as a fraction above the detection limit correlates directly or inversely C&A conditions and CRC in a number of fecal metabolites including tryptamine and short peptides. The data on metabolites prevalence presented in Supplementary Table 1, while Fig. 2 demonstrates the possible interactions between fecal metabolites in C&A and CRC. The fecal peptide profiles indicate that both increased protein degradation/proteolysis (higher peptide prevalence) and impaired tRNA aminoacylation (lower peptide prevalence) characterize gut microbiome of C&A and CRC populations in comparison with NNI and controls, similar to findings on short peptides in the blood of AD patients [98].
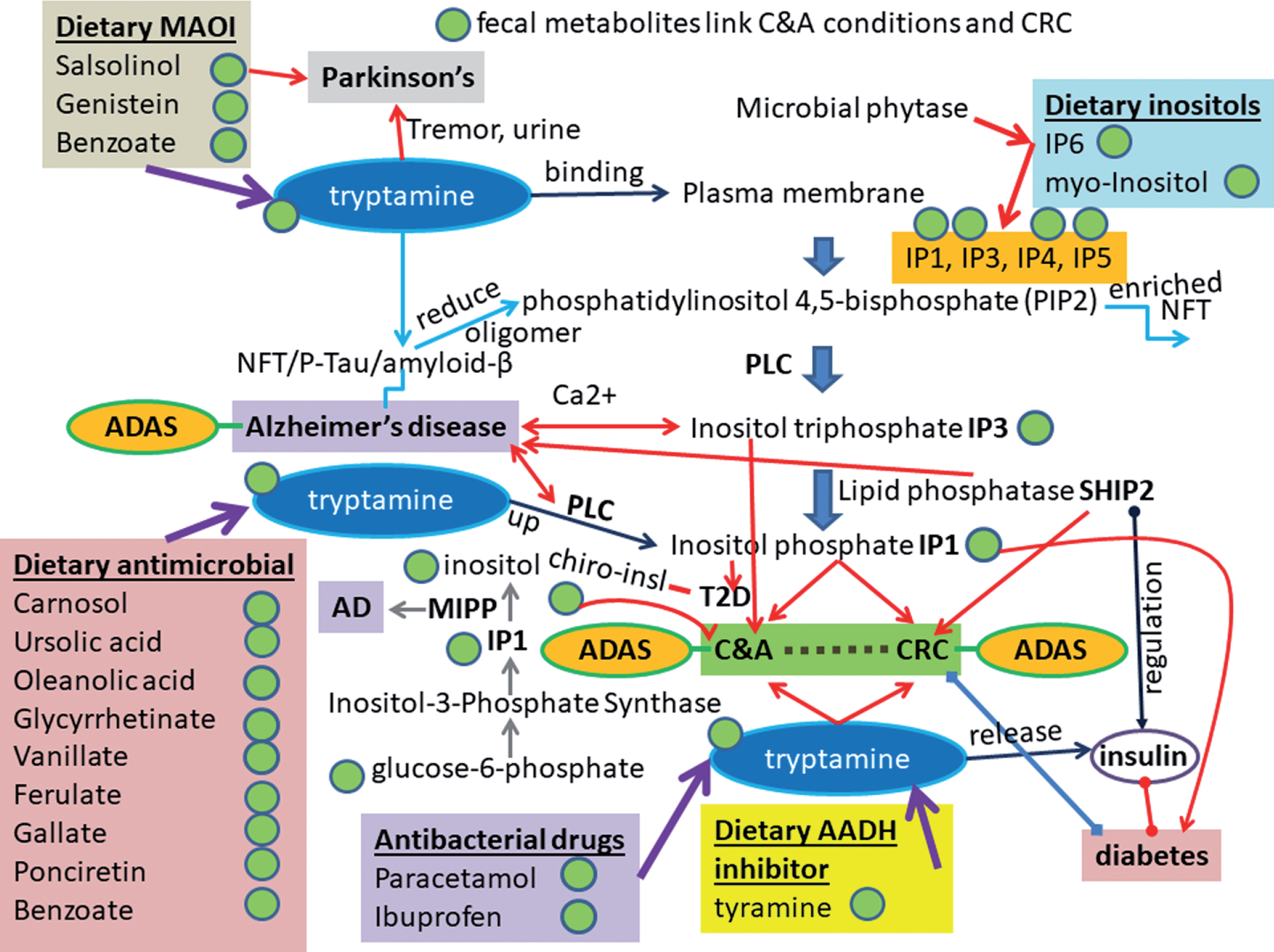
A metabolic link between CRC, medical conditions prevailing in C&A, and diet. The scheme shows the interactions between the fecal metabolites in the (ADAS+) populations. The gut metabolites are altered in ADAS-containing C&A [14] and CRC [16]. The associated medical conditions (diabetes, Parkinson’s disease, and AD) and dietary metabolites present in the scheme are discussed in the Results and Discussion. Abbreviations are in the text.
Fecal tryptamine increase correlates with tryptamine-induced morphological features in cells and mouse brain
Increase in tryptamine prevalence correlates with elevation of the soy product MAOI genistein in human gut of both C&A and CRC compared to controls. Tryptamine treatment induce formation of tangles of twisted filaments in the bovine kidney cells MDBK (15–20 nm thick), in human neuronal cells SH-SY5Y subline and in mouse brain (Fig. 3 A–C) resembling neurofibrillary tangles (NFTs) of paired helical filaments that characterize AD patients and other neurodegenerative diseases. The tryptamine cytotoxic effect visualized as cytoplasmic vacuolization or vacuolation of “spongy degeneration” type (Fig. 3B). The vacuolation seems to be a distinct form of cell death, which is different from the conventional lytic and apoptotic modes. Another way of cell death related to tryptamine effect is vesicularization or vesiculation—the formation of vesicles accompanied with neuronal cell fragmentation (Fig. 3B). The abundant vesicularization and neuronal fragmentation was also observed in AD brain [12]. The twisted filaments are visible in cytoplasm and in mitochondria lacking mitochondrial cristae in tryptamine-treated neuronal cells (Fig. 3B). Importantly, the decreased levels of platelet distribution width, red blood cell, hematocrit, hemoglobin, lymphocyte, and basophil revealed in the peripheral blood cells of AD patients compared with normal controls [110]. The blood cells deficiency can be caused by cytotoxic compounds such as tryptamine circulated in the peripheral blood and/or present in the blood cell forming tissues such as bone marrow, the lymph nodes, and spleen of AD patients.
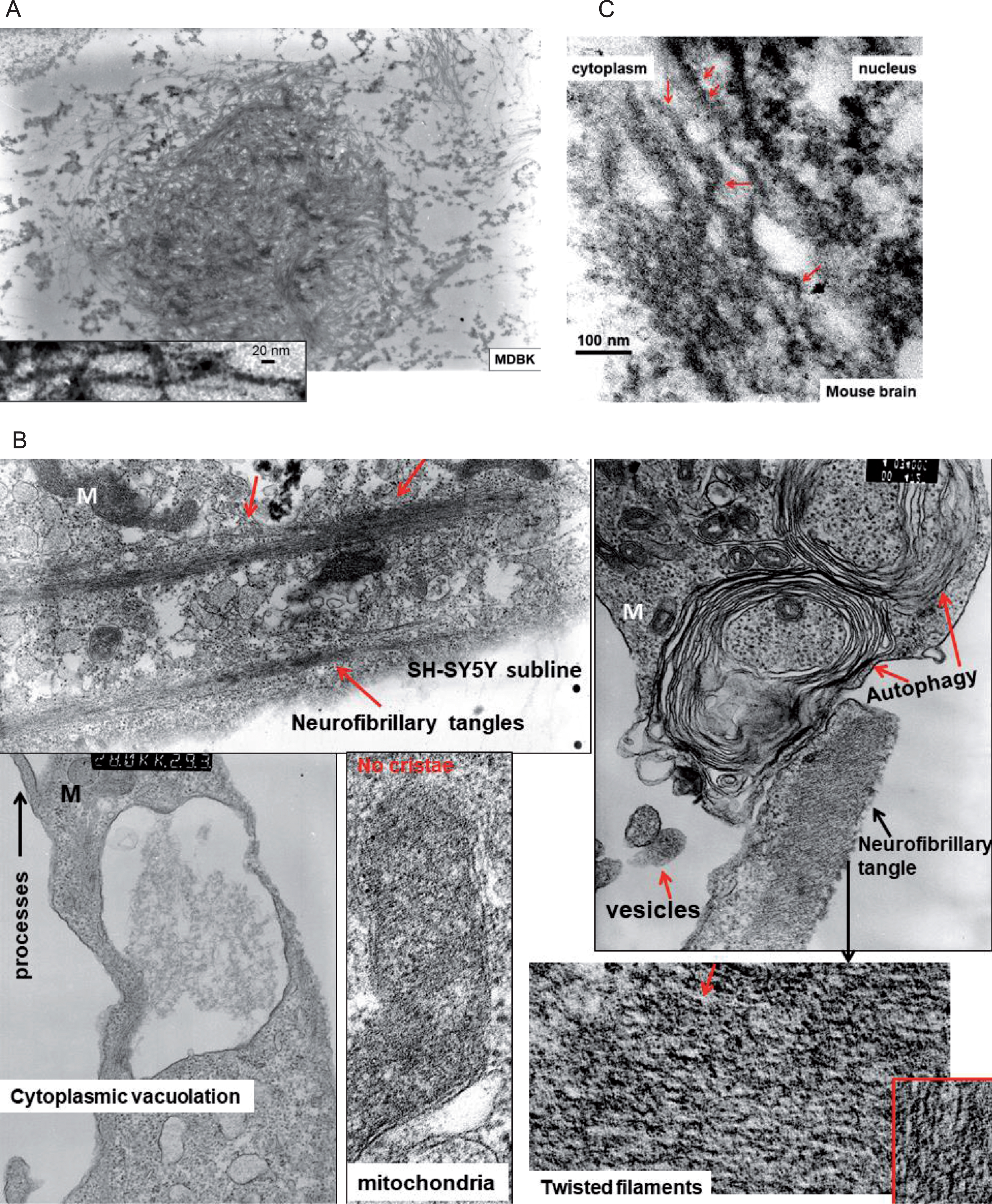
Electron microscopy of tryptamine-treated bovine kidney (A), human neuronal (B) cells, and mouse brain (C). A) Tangle of twisted filaments (15–20 nm thick) in detergent-pretreated MDBK cells. B) The twisted filaments are visible in mitochondria lacking mitochondrial cristae. M, mitochondria. Blue arrow shows TrpRS-immunopositive twisted filaments revealed with immune-gold particles of 10 nm. The monoclonal antibodies AT8 occasionally show rare P-tau positive twisted (helical) filaments. The visible here dramatic cytoplasmic vacuolation in the tryptamine-treated cells probably occur due to overproduction of hydrogen peroxide (H2O2), the reactive oxygen species (ROS). Tryptamine degradation produces H2O2. Morphological characteristics of cell death induced by H2O2 include DNA fragmentation, increased vacuolization, and nuclear condensation. The control cells and mice showed no manifestations of degeneration similar to those visible in tryptamine-treated cells and animals. The treatment of cells and animals and anti-TrpRS antibodies described earlier in details [4, 11, 277].
Food-derived fecal metabolites
Here the population-based data on prevalence (Table 2) and levels (Fig. 1) analyzed for food-derived fecal metabolites that include toxins, MAOI, antimicrobial compounds, biogenic amines, and other health-related metabolites. The C&A participants had significantly higher fecal erythritol level (1.87-fold, F test p value <0.0001****) than the NNI population. Participants with adiposity gain had significantly higher blood erythritol, a pentose-phosphate pathway metabolite [111]. It is widely used as sweetener in calorie-reduced food [112]. Erythritol may contribute to association between food and obesity. Food additive erythritol is significantly associated with incident T2DM [113]. Prevalence and level of fecal 2,4,6-trihydroxybenzoate are higher in NNI compared to C&A. In the clinical trial [114], the 2,4,6-trihydroxybenzoate significantly increased by 1.75-fold in the volunteers group consumed cranberry juice versus a placebo group suggesting that this may be a potential biomarker of consumption for cranberry juice. The 2,4,6-trihydroxybenzoate was not found in the cranberry beverage or blood plasma, but was detected in urine (https://www.fasebj.org/doi/abs/10.1096/fasebj.29.1_supplement.249.2).
2,4,6-trihydroxybenzoate is a product of oxidative degradation of quercetin[284]. In this table, the filled pink cells (color shading) represent positive associations and filled green cells represent inverse association between C&A and CRC.
Prevalence of food-derived MAOI genistein is higher in C&A (1.42-fold) and lower in CRC (1.2-fold) than in controls. The detectible genistein levels varied in both groups: in NNI (8,335–248,115 units) and C&A (4,053–141,578 units). In the NNI fecal samples, the highest tryptamine level corresponds to the highest genistein level in agreement with the genistein MAOI activity [115]. The difference in the genistein detectable levels was NNI/C&A = 2.3-fold (F test p value 0.0061).
Prevalence of food-derived [116] fecal metabolite neurotoxin (R)-salsolinol implicated in PD [117] is higher in C&A compared to NNI (difference in the level C&A/NNI = 4.25-fold, F test p value 0.0044) and lower in CRC than in controls. The dopamine-derived salsolinol derivatives determined as endogenous MAOI [118]. Salsolinol presents in Port wine and dried banana [119].
Prevalence of phytanate is higher in C&A and CRC than in controls. The level of food-derived phytanate is 1.58-fold higher in C&A than in NNI (t test p value 0.02*, F test p value 0.001**). Elevated amounts of phytanate was revealed in cases of multi-neuronal degeneration, hepatosplenomegaly, and adrenocortical insufficiency [120]. Phytanic acid induced neurotoxicity in an animal study [121]. Studies elucidated that the toxic activity of phytanic acid is mediated by multiple mitochondrial dysfunctions, generation of ROS, and Ca2+ deregulation via the Inositol P3–Ca2+ signaling pathway in glial cells [122]. Phytanic acid is a conjugate acid of a phytanate. It derives from a hydride of a phytane. Phytanic acid and phytanate are used as synonyms. Prevalence of phytol, a metabolic precursor of phytanic acid [123] is 100% in both C&A and NNI and is lower in CRC than in control group. The level of phytol is 1.8-fold higher (statistically significant p value <0.0001) in NNI than in C&A.
Prevalence of antimicrobial dietary component Carnosol is higher in NNI than in C&A. Prevalence of antimicrobial dietary components ursolic acid (163,729–3,076,120 units; levels: NNI/C&A = 1.46-fold, p value 0.0004) and oleanolic acid [124] (detected level NNI/C&A = 2.18-fold, p value 0.0395) is considerably lower in C&A and CRC compared to controls. Prevalence of glycyrrhetinate, the antibacterial compound of the plant Licorice [125] used in food, is lower in C&A than in NNI (NNI/C&A level 1.87-fold, p value 0.0002). Prevalence of a rare fecal ponciretin (occurred in the trifoliate orange) with anti-Helicobacter pylori activity [126] is lower in C&A and CRC compared to controls. The xylitol level is higher in NNI (NNI/C&A = 7.35-fold, F test < 0.0001). The sugar alcohol xylitol inhibits the growth of some bacterial species including Streptococcus mutans. It is used as a food additive to prevent caries [127]. Doses of xylitol as low as 0.15 g/kg-BW in dogs can result in life-threatening hypoglycemia and acute liver failure [128]. Xylulose is also higher in NNI (NNI/C&A = 1.6-fold, t test p value 0.02; 2 outliners in each group determined and removed using GraphPad Prism 8 software). The biotransformation from xylitol to L-xylulose by xylitol 4-dehydrogenase was studied intensively [129]. The lower prevalence of the plant-derived metabolites correlates with the C&A characteristics of high rates of processed food consumption and low fresh fruit and vegetable consumption. Concentrations of the antimicrobial dietary compounds varied among participants. These compounds can modify a gut microbial tryptophan metabolism in a dose-dependent manner.
Okra plants (used as food) colonization with Alcaligenes faecalis bacterial endophytes induced the plant defense response that can contribute to the biocontrol activity toward pathogenic fungus [130]. Assessment of chemotactic and biofilm formation potential toward individual phenolic acids revealed that different strains of Alcaligenes faecalis are maximally attracted toward 1μM shikimic acid or 1 mM vanillic acid (4-hydroxy-3-methoxybenzoic acid; flavoring agent) or 1 mM ferulic acid, thereby the phenolic acid components are responsible for attracting the endophytic A. faecalis isolates [131]. Human infections due to Alcaligenes faecalis are very rare [132, 133]. Food components vanillic acid [134], ferulic acid and gallic acid [135] exerted antibacterial activity. Prevalence of vanillate (level NNI/C&A = 1.14-fold, p value 0.006), ferulate (no significant difference in level NNI/C&A), and gallate (level NNI/C&A = 4.4-fold, p value <0.0001) are altered in C&A and CRC compared to controls (Table 2, Fig. 1). Gallic acid occurs in a great number of fruits and vegetables. The food compound plant sterol sitostanol is higher in C&A (C&A/NNI = 1.257-fold, F test p value 0.0155, 1 outliner removed) and lower in CRC compared to control. The food compound daidzein prevalence is higher while level is lower in C&A compared to NNI. Prevalence and level of β-hydroxypyruvate (OH-pyr) identified as a potential mediator of T2DM [136] is higher in C&A and CRC. OH-pyr can be biosynthesized from pyruvic acid and L-serine through the action of the enzyme serine—pyruvate aminotransferase. OH-per can be found in a number of foodstuffs such as root vegetables, cascade huckleberry, chervil, and common salsify. In C&A, prevalence of trans-4-hydroxyproline, which present in processed meat is higher (1.4-fold), but the level is lower than in NNI (NNI/C&A = 1.3-fold, F test p value 0.0002). Lower plasma trans-4-hydroxyproline and methionine sulfoxide levels are associated with insulin dysregulation in horses [137]. Methionine sulfoxide level is lower in C&A than in NNI (NNI/C&A = 1.2-fold, F test p value 0.0311). Thermal treatment of milk and milk products leads to protein oxidation, mainly the formation of methionine sulfoxide [138]. Prevalence and level of diaminopimelate are higher in C&A and CRC compared to controls (C&A/NNI = 1.72-fold F test p value 0.0160. Diaminopimelic acid (DAP) is an amino acid, representing an epsilon-carboxy derivative of lysine. DAP is a characteristic of cell walls of some bacteria. Prevalence of pyridoxine (vitamin B6) is higher in C&A and CRC versus controls. The level of vitamin B6 is higher in C&A than NNI (1.62-fold, p values t test 0.03*, F test <0.0001****). Tryptamine is produced by the aid of the vitamin B6-dependent enzymatic reaction. The enzyme employs a pyridoxal 5’ phosphate (PLP) co-factor similar to many amino acid decarboxylases. Pyridoxine induced cell death in a concentration-dependent way [139]. The food-derived pipecolate (metabolite of essential amino acid lysine) [140] is elevated in pyridoxine-dependent epilepsy and in C&A compared to NNI (C&A/NNI = 1.37-fold t test p value 0.0303). Another lysine metabolite, the food-produced 2-aminoadipate [141], is elevated in C&A (C&A/NNI = 1.46 t test p value 0.0413). Aminoadipic acid inhibits the production of kynurenic acid, a tryptophan metabolite in brain tissue slices [142].
Biogenic amines (BA), GABA, and amino acids from food and gut microbiome: Decarboxylase activity
Although no significant difference in fecal tryptophan detected between NNI and C&A (NNI/C&A = 1.088-fold, t test p value 0.5445), the decarboxylated tryptophan metabolite tryptamine is higher in C&A (C&A/NNI = 3.73-fold, cleaned data minus definitive 5 outliners, rout Q = 0.1%, identified and removed by GraphPad Prism 8 software; p values t test 0.0031**, F test <0.0001****). Tryptamine metabolite indoleacetate formed via MAO oxidation activity is slightly higher in NNI (NNI/C&A = 1.06-fold, F test p value 0.0239*). Altogether, the data indicate that the tryptamine conversion to IAA in gut can be inhibited in C&A group by MOAI and also by inhibitors of diamine oxidase (DAO), such as copper amine oxidase, which is active toward BA including tryptamine as a substrate [143]. Tryptamine also inhibits irreversibly this enzyme under anaerobic conditions in a manner of substrate inhibition.
In total, 74 BA-producing or BA-degrading strains were isolated from the human gut [144]. The human fecal bacteria Alcaligenes faecalis that presents in environment is able to utilize phenylethylamine, tyramine, and tryptamine as both carbon and nitrogen sources via activity of aromatic amine dehydrogenase (AADH). The quinone prosthetic group of AADH is tryptophan tryptophylquinone [145]. While MAO degrading BA present in both eukaryotes and prokaryotes, the AADH have been found only in bacteria. The inhibitors of AADH enzymatic activity can increase BA levels. Tyramine exerts the substrate inhibition activity toward AADH. Notably, the dietary/microbial tyramine is significantly higher in C&A than in NNI. Thus, tyramine can potentially protect tryptamine from the AADH-catalyzed utilization. AADH was inhibited irreversibly by hydrazine, phenylhydrazine, hydroxylamine, semicarbazide, and aminoguanidine while reversibly by isonicotinic acid hydrazide (isoniazid) and isonicotinic acid 2-isopropyl hydrazide (iproniazid) [146].
An increase in polyamines cadaverine (C&A/NNI = 7.8-fold t test p value 0.0002) and N-acetyl-cadaverine (C&A/NNI = 5-fold t test p value 0.0006) is significant in C&A compared to NNI. Lysine decarboxylase is an enzyme that converts lysine to cadaverine. N-acetylcadaverine has been found to be a metabolite of several bacteria species. The polyamine putrescine is also elevated in C&A (C&A/NNI = 2.9-fold F test p value <0.0001). N-acetylputrescine prevalence and level are elevated in C&A (C&A/NNI = 2.7-fold F test p value 0.0017). The biogenic amines putrescine and cadaverine show in vitro cytotoxicity at concentrations that can be found in foods [147]. A level of polyamine spermidine is elevated in C&A (C&A/NNI = 1.55-fold, f test p value <0.0001), while its prevalence is lower in C&A and CRC compared to controls. Spermidine exhibits anti-inflammatory properties [148]. The three low pH inducible amino acid decarboxylases specific for arginine, lysine, and ornithine were annotated in the bacterial genome [149]. It has been extensively demonstrated that the transcription of genes of many decarboxylase clusters are induced by low pH [150]. Tyramine biosynthesis is transcriptionally induced at low pH in human gut bacteria Enterococcus faecalis [151]. The histidine decarboxylase gene cluster of Morganella morganii DSM30146(T) was sequenced, and four open reading frames, named hdcT1, hdc, hdcT2, and hisRS, were identified. Two putative histidine/histamine antiporters (hdcT1 and hdcT2) were located upstream and downstream the hdc gene, codifying a pyridoxal-P dependent histidine decarboxylase, and followed by hisRS gene encoding a histidyl-tRNA synthetase [152]. The hdc and hisRS genes were highly induced under acidic and histidine-rich conditions. The food-borne biogenic amine histamine, a decarboxylated histidine is significantly higher in C&A than in NNI (C&A/NNI - 5.2-fold t test p value 0.0167) while the level of essential amino acid histidine is 1.14-fold lower in C&A than NNI (F test p value 0.02). In NNI, ratio histamine/histidine = 16-fold (F test p value <0.0001) whereas in C&A, the ratio histamine/histidine = 95-fold (t test p value 0.0031; F test p value <0.0001). Histamine is one of the few central nervous system neurotransmitters found to cause consistent blood-brain barrier opening [153]. Histidine is transported across the blood-brain barrier by its transporter, but histamine, a singly charged cation, can hardly penetrate the blood-brain barrier [154]. Pretreatment of mice, rats, and guinea pigs with inhibitors of histamine methylation, followed by systemic injection of 14C-histamine, results in a significant increase in brain 14C-histamine relative to controls [155]. Prevalence of N-acetyl-1-methylhistidine is 1.6-fold higher in C&A versus NNI. The two genes within the his operon implicated in histidine biosynthesis, trpR and hisB, were required for rice pathogen Xanthomonas virulence and bacterial growth in planta [156]. In Lactobacillus, the histamine-producing pathway encoded on an unstable plasmid [157]. Histamine at the concentration 16μM significantly inhibited protein biosynthesis in the rat liver microsomal fraction with aminoacyl-tRNA synthetases [158]. Tyramine level is 4-fold higher in C&A than in NNI [2] (t test p value 0.0194*; F test p value <0.0001****). Tyramine and histamine were toxic for intestinal cell cultures at concentrations commonly found in biogenic amines-rich food [159]. Moreover, the dietary biogenic amines tyramine and histamine show synergistic toxicity toward intestinal cells in cultures [160]. The cytotoxic histidinol, a histidine precursor, inhibits histidyl-tRNA synthetase. In addition to inhibiting protein synthesis, L-histidinol acts as an intracellular histamine antagonist [161, 162]. Human gut bacteria strains convert dietary histidine into histamine [163]. Bacterium that produces histamine utilizes histidine as its sole energy source, and it could play a role in bovine and equine laminitis [164]. This histamine-producing bacterium was isolated from the feces of cattle fed grain and the cecum of a horse. Histamine-secreting microbes are increased in the gut of adult asthma patients [165]. Histamine level in cattle rumen fluid increased from 0.013 mM (control) to 3.23 mM following soybean meal (at 48 h during in vitro rumen fermentation) [166]. Imidazole propionate as a microbially produced histidine-derived metabolite present at higher concentrations in subjects with versus without T2DM [167]. The imidazole propionate is lower (1.967-fold, F test p value 0.0002***) in C&A versus NNI. The prevalence (1.45-fold) and the level (1.85-fold, t test p value 0.0074) of histidine catabolite formiminoglutamate is lower in C&A versus NNI. A dietary biogenic amine agmatine is a decarboxylated arginine elevated in C&A and CRC (prevalence C&A/NNI = 1.4-fold or 60% /43%, level C&A/NNI = 2.06-fold F test p value 0.016). In targeted plasma metabolomics, the amino acids histidine, arginine, and glutamine are lower in schizophrenic patients than in controls [168]. The fecal arginine is lower 1.677-fold in C&A compared to NNI (t test p value 0.0334*, F test p value 0.012*). The mean lysine is 1.32-fold lower in C&A compared NNI (unpaired t test p value 0.0559). Methionine is 1.3-fold lower in C&A than in NNI (Welch’s t test p value 0.0184*). Cysteine is higher 1.52-fold in C&A than in NNI (t test p value 0.0113*). Taurine is derived from cysteine. Taurine prevalence and level are higher in C&A than in NNI (C&A/NNI 3.76-fold in t test, p value 0.0213*, F test p value 0.0011**). In this pathway, cysteine sulfinic acid is decarboxylated to taurine precursor. Although the aged or diseased brain might benefit from taurine food supplementation, it appears that adolescents are not likely to benefit from supplementation and may, in fact, suffer ill effects from chronic ingestion of high doses [169]. A previous study [2] showed the increase of biogenic amine phenylethylamine (PEA) in C&A versus NNI. The PEA abundant in fermented foods [170] is cytotoxic for some cells [171]. PEA is an inhibitor of bacterial phenylalanyl-tRNA synthetase [172]. PEA elevates mood and favors aggression [173]. The ratio cadaverine/Lys for NNI is 0.79 (t test p value <0.0001****), while the ratio cadaverine/Lys is 8.15 for C&A (t test p value 0.0001***, F test p value <0.0001****). The cadaverine/Lys ratio is 10.3-fold higher for C&A than for NNI. Cadaverine is a decarboxylation product of lysine and a competitive inhibitor of lysine binding to its lysyl-tRNA synthetase (LysRS) [174, 175]. The Km for lysine is 23.6±2μM and Ki for cadaverine is 77±8μM in ATP-PP, exchange reaction of LysRS from Bacillus stearothermophilus. Thus, the 8-fold molar excess of cadaverine over lysine in C&A can result in LysRS inhibition. Increased metabolites such as methionine sulfoxide, 3-methoxy-anthranilate, cadaverine, guanine, and histamine were observed by widely targeted metabolomics of postmortem cerebrospinal fluid from the AD subjects [176]. Fluor 555-cadaverine exudes into most tissues, but normally is excluded from the central nervous system, the vasculature of which is protected with the blood-brain barrier [177]. The metabolic link of histidine to tryptophan was demonstrated in Neurospora crassa, in which the starvation of tryptophan mutants for tryptophan resulted in the de-repression of tryptophan, histidine, and arginine biosynthetic enzymes [178]. Ornithine level is 1.32-fold lower in C&A compared to NNI (F test p value 0.0199*). Ornithine is a non-proteinogenic amino acid. Ornithine via the action of ornithine decarboxylase is the starting point for the synthesis of polyamines such as putrescine. The mean level value of gamma-aminobutyrate (GABA) synthesized from glutamate via the enzyme glutamate decarboxylase with pyridoxal phosphate (the active form of vitamin B6) as a cofactor is 1.8-fold higher in C&A compared to NNI (t test p value 0.1605; F test p value <0.0001****) while glutamate is 1.18-fold lower in C&A than in NNI (t test p value 0.0203*, F test 0.2835). Data suggest that GABA and glutamate play an important role in the etiology of pain and depression [179]. GABA and cadaverine inhibit LysRS and GABA inhibits in vivo growth of Bacillus subtilis strains [180]. Level of essential amino acid valine is 1.36-fold lower in C&A versus NNI (t test p value 0.0114*, F test p value 0.0178*). The level of norvaline is also lower in C&A versus NNI (1.28-fold, F test p value 0.0015**). The misincorporation of a non-proteinogenic amino acid norvaline found in E. coli strain on 10% of all measured leucine residues under microaerobic conditions [181]. The level of essential amino acid isoleucine is 1.25-fold lower in C&A versus NNI (t test p value 0.0294*). The level of essential amino acid threonine is 1.39-fold lower in C&A versus NNI (t test p value 0.0002***). The level of allo-threonine is 1.43-fold lower in C&A versus NNI (p values t test 0.0342*, F test 0.0109*). Allo-threonine found in immunogenic tetra-peptide of the Mycobacterium avium [182]. The level of essential amino acid phenylalanine is 1.25-fold lower in C&A versus NNI (t test p value 0.0341*, one outliner removed). The level of essential amino acid leucine is not significantly different in C&A versus NNI (NNI/C&A = 1.2-fold, t test p value 0.0838). Thus, the essential amino acids (Met, Ileu, His, Val, Thr, Phe, Lys) excluding leucine and tryptophan are statistically lower in C&A versus NNI. The semi-essential amino acid tyrosine is 1.2-fold lower in C&A versus NNI (statistically non-significant, t test p value 0.0808). The nonessential amino acids are significantly lower in C&A versus NNI: proline is 1.4-fold (t test p value 0.0059**), glycine - 1.295-fold (t test p value 0.0288*), and alanine - 1.278-fold (t test p value 0.0253*). The nonessential amino acids glutamine (1.07-fold, t test p value 0.67), asparagine (1.21-fold, t test p value 0.3860) and serine (1.13-fold, t test p value 0.3358) are non-significantly lower in C&A versus NNI. The non-essential amino acid aspartate showed non-significantly higher level in C&A versus NNI (NNI/C&A = 1.009, t test p value 0.9490). Significant decrease was observed with AD progression for asparagine, methionine, histidine in the serum samples [183]. Therefore, the only one proteinogenic amino acid cysteine (Cys) was significantly higher in C&A versus NNI (Fig. 1, Table 3).
Notably, plasma total concentrations of the sulphur amino acid Cys are linearly associated with fat mass in large population studies. Animal and cellular experiments support the concept that Cys may be obesogenic [184]. The PLP-dependent cysteine sulfinic acid decarboxylase catalyzes the decarboxylation of L-aspartate, 3-sulfino-L-alanine (cysteine sulfinic acid), and L-cysteate to beta-alanine, hypotaurine, and taurine, respectively. The expression of cysteine sulfinate decarboxylase of seawater Pacific oyster was upregulated hundreds of times in response to low salinity in salinity stress experiments [185]. Aromatic L-amino acid decarboxylase (AADC) activity in the intestinal mucosa of old rats was higher than in adult rats. High salt diet increased the AADC activity in adult rats, but not in old rats [186]. The biogenic amines tyramine, histamine, putrescine, cadaverine, and agmatine increased during the salt-ripening process of anchovies [187]. The highest BA values were found in the batch where initial microbial load was highest, especially for enterobacteria and enterococci. The presence of NaCl led to an upregulation of histidine decarboxylase gene in the bacterial strain grown on skim milk [150]. The BA were reduced during salted fish fermentation by starter bacterial culture of Bacillus polymyxa possessing amine degrading activity [188]. The disease-linked homocysteine, a protein amino acid in humans [189] is higher in C&A versus NNI (1.5-fold, p values t test 0.0268*, F test <0.0001****). Homocysteine is suggested for the risk prediction of cognitive impairment among ischemic stroke patients with elevated blood pressure [190]. Prevalence of N-formylmethionine (fMet), a derivative of the amino acid methionine in which a formyl group has been added to the amino group for initiation of protein synthesis in bacteria, mitochondria and chloroplasts is lower in C&A (80%) versus NNI (100%) and no difference is in CRC versus NNI (98%). The fMet level is non-significantly lower in C&A versus NNI (1.135-fold, t test p value 0.4512). A lowest content for proteinogenic amino acids is revealed here for histidine in C&A. In the Chinese study, dietary histidine was significantly lower in overweight (p < 0.05) and obese (p < 0.01) participants of both sexes [191]. As many as one-third of mutations in a gene result in the corresponding enzyme having an increased Michaelis constant, or K(m), (decreased binding affinity) for a coenzyme, resulting in a lower rate of reaction. The defective enzymes can be remedied or ameliorated by the administration of high doses of the vitamin component of the corresponding coenzyme, which at least partially restores enzymatic activity [192]. The amino acid decarboxylases are enzymes that use a PLP cofactor, the active form of vitamin B6. Plausibly the 1.62-fold increase in vitamin B6 in C&A versus NNI is linked to coordinated increase in decarboxylase enzymatic activities toward the PLP-dependent production of biogenic amines from corresponding amino acids. Over 80% of the histidine and 95% of the tyrosine had been converted into histamine and tyramine in cheese by day 60. Substrate (amino acids) depletion played an important role in the rate of biogenic amine buildup, becoming a limiting factor in the case of some amino acids. Tryptamine reached 0.4 mg/g of cheese during 240 days of ripening and storage [193].
The secreted protein diamine oxidase (DAO) has a slow turnover. This, together with the efficacy of the homeostatic regulation of the polyamines via the interconversion reactions and by transport pathways, renders a role of DAO in the regulation of polyamine concentrations unlikely [194]. Histamine intolerance is a disorder attributed to the deficiency in the enzyme DAO, which degrades histamine. In patients with episodic migraine treated with DAO supplement, the mean headache durations of 6.14 (±3.06) and 4.76 (±2.68) h were registered before and after treatment, respectively [195].
Administration of BA (putrescine, cadaverine, tryptamine, β-phenylethylamine, spermine, and histamine) to 15 weaned Saanen (goat) kids (2 months old; 11.6±1.4 kg body weight) for 14 days (1.4 g per day of amines by oral administration or 122 mg/kg per day) had a negative effect on the histological characteristics of rumen, abomasum, liver, pancreas, duodenum, jejunum, and distal ileum [196]. If intestinal concentrations of these amines exceed the capacity of gut wall amine oxidizing enzymes, they will be absorbed causing stress to intermediary metabolism with detrimental effects on health and growth performance. Mitotic figures in intestinal glands appeared more common than normal following oral administration of BA. The entire alimentary tract of the treated animals (goats) showed evident signs of inflammation and epithelial shedding. Pathological epithelial cell shedding occurs in many intestinal diseases. The cell loss from the villus exceeds the regenerative capacity of the crypts, due to epithelial injury to one or both components [197]. Shedding of intestinal epithelial cells (IEC) from the epithelial monolayer may cause transient gaps or microerosions in the epithelial barrier, resulting in increased intestinal permeability. The pathological IEC shedding has been observed in mouse models of inflammation and human intestinal conditions such as IBD. Inflammatory infiltrates were present in numerous areas of the rumen musculature following direct oral administration of BA. In the liver inflammatory foci containing eosinophilic granulocytes were often observed in the parenchyma. In the pancreas, the islets of Langerhans endocrine cells appear swollen. The islets contained sometimes cells of abnormally small size. The exocrine pancreas also appeared disorganized [196]. Cell swelling is an early change in most types of acute cell damage. The increased intestinal permeability or “leaky gut” was revealed in AD [198]. Increased concentrations of fecal calprotectin indicate a disturbed intestinal barrier function in AD patients. Fecal calprotectin may be a marker for subclinical intestinal inflammation [199].
Proliferation of mammary epithelial cells was stimulated at low concentrations, while at high concentrations it was inhibited by BA cadaverine, putrescine, spermine, spermidine, and β-phenylethylamine [200]. In other words, the BA tested had both proliferative and cytotoxic effects similar to our findings for tryptamine [12].
Effect of biogenic amines on activity of aminoacyl-tRNA synthetases (ARS) and protein biosynthesis
Tryptamine inhibits TrpRS [98]. Histamine at the concentration 16μM significantly inhibited protein biosynthesis in the rat liver microsomal fraction with the presence of aminoacyl-tRNA synthetases [158]. Cadaverine is a decarboxylation product of lysine and a competitive inhibitor of lysine binding to its lysyl-tRNA synthetase (LysRS) [174, 175]. Phenylethylamine (PEA) is an inhibitor of bacterial phenylalanyl-tRNA synthetase [172].
Biogenic polyamine spermine stimulates activities of microbial argynyl-tRNA synthetase [201] as well as bacterial [202] and rat-liver isoleucyl-tRNA synthetase [203] but inhibits tyrosyl-tRNA synthetase from Drosophila [204]. In the study of Holler (Lawrence Berkeley Laboratory, University of California, Berkeley), isoleucyl-tRNA synthetase of Escherichia coli is inhibited by spermine [205]. Spermine produced from putrescine, which is produced in the cytoplasm of cells by decarboxylation of a non-protein amino acid ornithine.
Disease-related bioactive metabolites
The level and prevalence of deuteroporphyrin IX described as a fecal porphyrin in patients with endemic chronic arsenic poisoning (http://www.hmdb.ca/metabolites/HMDB0000579) are higher in C&A compared to NNI (C&A/NNI level = 1.96-fold, F test p value 0.0009).
Glycolithocholate sulfate, an urinary marker of liver diseases [206], showed a lower prevalence in C&A (no significant difference in NNI/C&A level) and CRC compared to controls. The urinary glycolithocholate 3-sulfate was markedly increased in hepatitis B-induced cirrhotic patients compared with healthy controls [207].
Prevalence of 1-methylimidazoleacetate is higher in C&A than in NNI with no statistically significant difference in levels. Increase of this histidine metabolite in blood is associated with mortality related to cerebral malaria encephalopathy due to infection with Plasmodium falciparum [208].
Prevalence of 3-ureidopropionate (pyrimidine, uracil-containing metabolite) is increased in both C&A (no significant difference in the levels of C&A versus NNI) and CRC. This metabolite predicted mortality in cirrhosis [209].
The 103 subjects with cirrhosis had measured glomerular filtration rate, which was strongly associated with erythronate. The erythronate level (100% prevalence in C&A and NNI) is significantly higher in C&A than in NNI (1.46-fold, t test p value 0.006**). High fecal erythronate is associated with Enterobacteriaceae predominated in CRC [210].
The prevalence of bile acid metabolite glycocholate is lower in CRC and C&A and significantly higher in fecal samples of individuals with Crohn’s disease (CD) in the twin study [211]. ADAS presents in this CD group. The glycocholate level is 1.9-fold higher (F test p value <0.0001) in C&A compared to NNI. Glycocholate was suggested as a biomarker of cholangiocarcinoma, a bile duct cancer [212] and of obesity [213]. Bile acids are important endocrine signaling molecules, modulating glucose homeostasis through activation of cell surface and nuclear receptors. Bile acid metabolism including glycocholate is altered in T2DM [214]. Median fecal glycocholate excretion is 111,000 for NNI and 213,000 for C&A with the highest values in individuals with T2DM/obesity. A number of bile metabolites are altered in C&A and CRC in comparison with NNI and controls (Supplementary Table 1).
For the 2-hydroxybutyrate (AHB) prevalence is NNI/73.9% versus C&A/62.85%; the levels C&A/NN = 2.78-fold (F test p value <0.0001). The 2-hydroxybutyrate (alpha-hydroxybutyrate) and 3-hydroxybutyrate (beta-hydroxybutirate) suggested as prognostic biomarkers to predict the onset of diabetic complications in women with gestational diabetes after delivery [215]. Alpha-hydroxybutyrate is an early plasma biomarker of insulin resistance and glucose intolerance in a nondiabetic population [216]. The four highest fecal AHB values of C&A belongs to individuals with obesity/T2DM. AHB is produced by the intestinal bacterium Escherichia coli K12 strain [217].
3-hydroxybutyrate (BHB) shows 100% prevalence in NNI and C&A, while the level ratio C&A/NNI = 1.51-fold (F test p value <0.0001). This ketone body is produced in alcoholic ketoacidosis and fasting [218].
Prevalence of N-methylhydantoin is higher in C&A (54.28%) versus NNI (26%) and in CRC (77%) versus controls (73%). The mean level of detectable N-methylhydantoin is lower in C&A versus NNI (2.52-fold, F test p value 0.0028**). 1-Methylhydantoin is produced by bacterial creatinine deaminase in the intestinal tract of uremic patients and retaken up into the body. The 1-methylhydantoin (N-methylhydantoin) induced apoptosis as well as cell changes consistent with necrosis [219].
Prevalence of sarcosine (N-Methylglycine) is higher in both C&A and CRC versus controls. The sarcosine level is higher in C&A versus NNI (1.43-fold, Welch’s t test p value 0.0434*, F test 0.0030**, the four definitive outliners removed). Sarcosine, an N-methyl derivative of the amino acid glycine and a metabolic product of choline, plays an important role for prostate cancer aggressiveness and progression [220].
The amino sugar glucosamine is 2.18-fold higher in C&A versus NNI (p values t test 0.0004***, F test 0.0047**). The anti-inflammatory actions of glucosamine on arthritic disorders are suggested. Glucosamine infusion in rats mimics the beta-cells dysfunction of T2DM [221]. Cholesterol level is 1.22-fold higher in C&A versus NNI (F test p value 0.0298*).
In exhaled breath condensate samples of human patients, the two metabolic discriminant features, 4-hydroxycyclohexylcarboxylic acid (higher prevalence in C&A than NNI) and pyroglutamic acid, differentiated the acute pulmonary exacerbations from the stable cystic fibrosis with 84.6% accuracy [222]. 4-hydroxycyclohexanecarboxylic acid is derived from Spanish-style green table olives [223].
Inositol pathway: Inositol/inositol phosphates
Prevalence of inositol-1,4,5-triphosphate (IP3), which is implicated in Ca2+ signaling, is higher 2-fold in C&A than in NNI (Supplementary Table 1). The difference in the level of IP3 between C&A and NNI is statistically significant (C&A/NNI = 5.48-fold; p value 0.0037). A variety of alterations in [Ca2+]-regulation may contribute to the neuronal damage in stroke and AD [224]. In AD, Ca(2+) dyshomeostasis represents a global phenomenon affecting virtually all cells in the brain [225]. The nanomolar concentrations of amyloid β-peptide (component of AD plaques) increase the IP3 receptor and mitochondrial calcium concentrations [226]. Prevalence of inositol 1-phosphate (IP1) is higher in C&A and CRC than in controls. Heatmap depicting metabolites of statistically significant differences between C&A and NNI populations [14] includes IP1 with a higher C&A level. Here, in the Welch’s test, the difference in the IP1 levels between C&A and NNI is statistically significant (C&A/NNI = 2,218-fold; p value <0.0001). Figure 2 illustrates the inositol phosphate interactions in the general scheme linking ADAS to AD, T2DM, and CRC. The IP3 produces by hydrolysis of phosphatidylinositol 4,5-bisphosphate (PIP2), a phospholipid (phosphoinositide) that is located in the plasma membrane, by phospholipase C (PLC). Oligomeric amyloid-β decreases the level of PIP2 that regulates key aspects of neuronal function [227]. PIP2 was selectively enriched in granulovacuolar degeneration bodies and NFTs [228]. It is widely accepted that IP1 is a major product of the dephosphorylation of inositol polyphosphates. Inositol polyphosphate 5-phosphatase subfamilies include SHIP2, OCRL, and INPP5B involved in insulin regulation and Lowes syndrome [229]. SHIP2 expression is increased in CRC tissue in comparison to adjacent normal tissue, and this is correlated with decreased patient survival. Moreover, SHIP2 is more active in CRC tissue, suggesting that SHIP2 can induce oncogenesis in colonic epithelial cells [230]. SHIP2 inhibition decreases tau protein (component of AD NFT) hyperphosphorylation (P-tau) induced by amyloid-β thus supporting usage of SHIP2 inhibitors for AD treatment [231]. Tryptamine stimulates inositol phosphate accumulation in a dose-dependent way in rat cortical slices with dominated form inositol monophosphate [232]. Tryptamine functions as a full agonist at the PLC signaling pathway [69, 233]. The results suggest that the PLC isozymes are differentially involved in AD [234]. Tryptamine binds to phospholipid liposome [235] and to lipid fraction containing phosphatidylserine and phosphatidylinositol [236]. [3H]tryptamine binds also to whole rat brain synaptic plasma membranes. These binding was decreased by treatment with Azure A (Giemsa solution) and phospholipase A2, while phospholipase D had no effect [236]. Moreover tryptamine upregulates (4.1-fold) the gene encoding amyloid-β precursor-like protein 2 [237]. In urinary metabolomics of newborns infected by human cytomegalovirus, the most important metabolites characterizing the clustering of the samples were: myo-inositol, glycine, 3-hydroxybutyrate, 3-aminoisobutyrate (BAIBA), creatine, taurine and betaine [238]. A stereoisomer of inositol, myo-inositol, presents in a variety of cell types and is obtained from the following three major sources: de novo synthesis from glucose-6-phosphate (G-6-P), sequential dephosphorylation of phosphoinositides, and membrane transport from extracellular fluid. The biosynthesis of inositol follows a common pathway involving first the conversion of G-6-P to myo-inositol-1-phosphate (MIP) catalyzed by MIP synthase, followed by dephosphorylation catalyzed by MIP phosphatase (MIPP). In AD brains, the MIPP activity and its protein level were significantly higher than in control brains [239]. Disruption of inositol homeostasis has been associated with a number of illnesses, including bipolar disorder, AD, bulimia, metabolic syndrome, T2DM, and epilepsy [240]. Fecal chiro-inositol is lower in C&A than in NNI: prevalence (1.76-fold) and level (5.1-fold, F test p value <0.0001****). The urinary excretion of chiro-inositol was much lower in T2DM patients than in control subjects [241]. The enhanced inositol phosphate accumulation was demonstrated in platelets from the diabetic patients [242]. In plant foodstuffs, inositol is preferentially present as phytic acid (IP6). The main sources of phytate are cereals and legumes, including oil, seeds and nuts [243]. Phytases are phosphohydrolytic enzymes that initiate stepwise removal of phosphate from phytate [244]. Phytase, a phosphatase that catalyzes the hydrolysis of indigestible phytic acid (myo-inositol hexakisphosphate), present in Lactobacillus strains isolated from farmhouse goat’s milk cheeses—in the 10 strains of L. plantarum and in 2 strains of L. paracasei of 80 strains [245] (15% of isolated strains). Lactobacillus can be found in plants or material of plant origin, silage, fermented food (yogurt, cheese, olives, pickles, salami, etc.), as well as in the oral cavities, gastrointestinal tracts, and vaginas of humans and animals [246]. Prevalence of inositol phosphates (IP) IP3, IP4, IP5, and IP6 is higher in C&A than in NNI and unidentified in CRC and the controls while the tryptamine-inducible IP1 is higher in both C&A and CRC compared to controls. The difference in the level of IP6 (myo-inositol hexakisphosphate) between C&A and NNI is statistically significant (C&A/NNI = 7.69-fold; F test p value <0.0001). Myo-inositol pentakisphosphate (IP5) level is 2.37-fold and myo-inositol tetrakisphosphate (IP4) is 3.3-fold higher in C&A than NNI. When applied extracellularly, myo-inositol hexakisphosphate (IP6) and myo-inositol pentakisphosphate (IP5) can inhibit the growth and proliferation of tumor cells [247–249]. C&A participants originate from five different towns in western Oklahoma: Clinton, Concho, Geary, Hammon, and Kingfisher, and NNI from Norman, Oklahoma. Subsistence strategy for both populations C&A and NNI is Industrial Agriculture. Phytate-degrading recombinant Lactobacillus cultures expressing Bacillus subtilis phytase used as probiotics in broiler chickens [250]. I hypothesize that a part of Western Oklahoma participants may possess enzyme phytase in gut microbiota with a higher proportion of microbial phytase carriers in C&A than in NNI population or/and C&A consume more processed food containing IP. Increase in specific kinase activity can also cause increase in IP, particularly, inositol trisphosphate 3-kinase B (ITPKB) phosphorylates inositol 1,4,5-trisphosphate into inositol 1,3,4,5-tetrakisphosphate. The ITPKB protein level was increased 3-fold in the cerebral cortex of most patients with AD compared with control subjects, and accumulated in dystrophic neurites associated to amyloid plaques [251].
The environmental bacterium Legionella pneumophila, a natural parasite of environmental amoebae and the causative agent of a severe pneumonia termed Legionnaires’ disease, metabolizes myo-inositol through the iol gene products, thus promoting the growth and virulence of the pathogen [252]. Myo-inositol detected in all the samples of both NNI and C&A is 1.75-fold higher in C&A than in NNI (statistically significant difference: t test p value 0.03*, F test p value 0.0006***). Increased cerebral myo-inositol revealed with proton MR spectroscopy was demonstrated in AD [253], in the dementia of Down syndrome [254,] and in patients with glioblastoma multiforme [255]. Myo-inositol is clustered in human cytomegalovirus infection with 3-aminoisobutyrate, which prevalence is higher in CRC while 3-aminoisobutyric acid (or β-aminoisobutyric acid, BAIBA) prevalence is lower in C&A compared to controls. The 3-aminoisobutyrate is a conjugate base formed by deprotonation of BAIBA carboxylic acid group. BAIBA level is 1.9-fold higher (p value <0.0001 in F test) in C&A compared to NNI. The 3-aminoisobutyrate was good discriminator for CRC patients [256]. In humans, plasma BAIBA concentrations increase with exercise [257]. Prevalence of chiro-inositol and three other serum metabolites theobromine, 7-methylurate and 3-methylxanthine of the 10 most influential metabolites for discriminating between the Dietary Approaches to Stop Hypertension (DASH) and control dietary patterns altered in C&A and CRC compared to controls [258]. The DASH dietary pattern is recommended for cardiovascular disease risk reduction.
Nucleic acids DNA and RNA components
The fecal deoxyribose level was 1.6-fold lower in C&A than in NNI (t test p value 0.0074, F test p value 0.0009). This can be due to the presence of gut bacteria that utilize deoxyribose. The bacterium that can grow with deoxyribose as its sole source of carbon was characterized [259]. Deoxyribose is one of the building blocks of DNA and is released when cells die and their DNA degrades. Another DNA component thymine is 1.46-fold lower (t test p value 0.0046) in C&A compared to NNI. Lethality under thymine starvation or thymineless death in bacteria is known for decades. Given that thymineless death is similar in mammalian cells [260], this phenomenon can be related to the C&A health status. The plasma metabolite thymine was altered in AD (2.05-fold higher level) compared to normal controls [261]. Prevalence of both fecal metabolites deoxyribose and thymine is lower in CRC than in control. Guanine, one of the four main nucleobases found in the nucleic acids DNA and RNA, is 1.62-fold higher in C&A compared to NNI (t test p value 0.0005***), increased in AD [176].
Short peptides in human fecal samples/gut microbiota
The prevalence and levels of short peptides are demonstrated in Supplementary Table 1 and Fig. 1. The level of histidylvaline is 1.92-fold higher in NNI versus C&A (F test p value <0.0001****). The level of aspartylphenylalanine is 1.18-fold higher in NNI than in C&A (F test p value 0.0382*); serylleucine - C&A/NNI = 1.4-fold (t test p value 0.042*, F test p value 0.0001****); glycylalanine – NNI/C&A = 1.18-fold (F test p value 0.0351*); phenylalanylvaline - NNI/C&A = 1.22-fold (F test p value 0.0084**); arginylleucine C&A/NNI 1.35-fold (F test p value <0.0001****); tyrosylvaline level NNI/C&A = 1.29-fold (F test p value 0.0146*); lysylproline NNI/C&A = 1.23-fold (t test p value 0.2, F test, p value 0.0631); pyroglutamylvaline NNI/C&A 1.27-fold (F test p value 0.0019**); histidylisoleucine NNI/C&A = 1.357 (t test p value 0.2, F test p value 0.0004***); gamma-glutamyltyrosine level NNI/C&A = 1.3 (t Test p value 0.0233*, 3 outliners removed by GraphPad Prism), the prevalence ratio NNI/C&A = 1.52. The level of asparagylleucine is higher (1.55-fold) in C&A versus NNI (p values t test 0.0256*, F test 0.0002***). N-acetyl-aspartyl-glutamate (NAAG), a peptide neurotransmitter, is lower in both C&A and CRC versus controls. The NAAG level is lower in C&A versus NNI (1.28-fold, t test p value <0.0001****). The Welch’s t test indicates that along with an increase in some short peptides in C&A that can reflect higher proteolysis, the decrease is also revealed in C&A. The decrease in short peptides detected in C&A group can be caused by deficiency in tRNA aminoacylation/protein biosynthesis in microbes found predominantly in human stool. The resulting average values for some peptides are with no significant differences between NNI and C&A because the data reflect both decrease and increase. Based on the peptide prevalence (Supplementary Table 1), the peptide decrease is expected to be more profound than could be estimated by Welch’s t test in the C&A gut microbiota. Because at least two processes are coincided, the increased proteolysis and tRNA aminoacylation/protein biosynthesis impairment, the data show the combined processes. In such a situation, the analysis of prevalence is informative. Both the deficiency in amino acids and abundance of biogenic amines (Table 3, Fig. 1) lead to the protein biosynthesis decline. The decline in NAAG exemplifies the reduction in bioactive peptides. The levels of the total 81 peptides is compared with the tryptamine levels in NNI and C&A (Fig. 1H). The one of the three highest tryptamine samples correspond to the lowest total peptide’s level (sample NO13). Figure 1H shows the tryptamine (T)-high samples (NO1 and NO13) versus T-low (NO2) and non-detectable (ND) tryptamine (NO7 and NO15) samples of NNI group. The distribution of individual values demonstrates both high and low peptide levels in the samples with detectable tryptamine. In the microbial cheese ripening, the greatest range of proteolysis correlates with the BA content [262, 263]. Amino acid starvation-induced macroautophagy leads to selective degradation of proteins important for protein translation [264]. In C&A, the amino acid decrease (starvation) correlates with BA abundance and rise of some peptides that characterize the protein degradation. It was shown that the tryptamine effects are dose-, time-, and diet-dependent and include tryptamine-induced seizures and death in animals [2]. It is noteworthy that the traditional diet of American Indian including C&A people contains maize, or corn, an important crop to tribes, and beans. In rumen fluid of the ruminant animal goat, metabolomics revealed that a high grain feeding (50% maize) increased tryptamine levels (284.08μM) compared to control with no maize feeding (145μM) [265]. Tryptamine was the main BA detected in beans, and its concentration considerably increased during the germination [266]. In Saskatchewan, Canada between 2005 and 2010, the overall age-standardized incidence of epilepsy was 62 per 100,000 person-years, while for self-declared registered Indian aboriginal population of the same province, the overall age-standardized incidence of epilepsy was 122 per 100,000 person-years [267]. Epilepsy was a well-recognized disease in pre-Columbian cultures of Native American tribes [268]. The disproportionately high rates of T2DM-related mortality and complications among Indigenous populations of Australia, Canada, New Zealand, and the United States were reported [269, 270]. The causal link between seizure and constipation is a common belief among patients and physicians while constipated mice are more prone to seizure [271]. This correlation supports a role of gastrointestinal conditions in the pathogenesis of epilepsy affecting about 60 million people worldwide. Constipation is also associated with cardiovascular events [272].
Public health
The control of tryptamine content is utmost important for human life because tryptamine readily crosses the blood-brain barrier [53] and induces seizures [8, 273] at concentrations than can be detected in food. In the US, seizure-related deaths take more than 5,000 lives each year [274]. High seizure frequency is strongly associated with increased mortality. Seizures and epileptic activity is frequently associated with AD [275], particularly in the early stages of AD [276]. Epilepsy is associated with a high rate of premature mortality from direct and indirect effects of seizures. Sudden unexpected death in epilepsy (SUDEP) is the second leading neurologic cause of total lost potential life-years after stroke. The present and earlier reported [2] analysis of tryptamine produced by human gut microbiome is a response to a call for action against seizure-related deaths [274]. Controlling seizures will save lives. Death records show that American Indian and Alaska Native death rates for both men and women combined were nearly 50% greater than rates among non-Hispanic whites during 1999–2009 (https://www.cdc.gov/media/releases/2014/p0422-natamerican-deathrate.html).
Conclusions
The present study reveals: 1) the common signaling pathways in AD and other diseases marked by ADAS; 2) the alterations in metabolic pathways uncovered in this study correlate with dysbiosis in C&A [14]; 3) the ADAS-linked prevalence of fecal metabolites in C&A and CRC shed light on interfacing mechanism of tryptamine-induced inositol phosphate signaling; 4) L-amino acids decarboxylase activity (AAD) of human gut is critical for production of cytotoxic BA in ADAS-linked pathology. The AAD modifying factors discussed here are vitamin B6, salt stress, and low pH; 5) impairment of protein biosynthesis machinery in human gut microbiome and human cells can play a causative role in ADAS linked pathologies. The amino acids-to-biogenic amines conversion regulates the protein biosynthesis at the levels of: 1) aminoacyl-tRNA synthetase (ARS) enzymatic activities, and 2) transcription of genes encoding ARS in the decarboxylase gene clusters. Altogether the data support conclusion that neurodegeneration is a part of the generalized protein biosynthesis machinery dysfunction. The targeted metagenomics revealed the gut microbial metabolites that expand the knowledge of human pathophysiology. The data on AD related comorbidity and concomitant diseases along with our data on targeted gut metagenomics sequence analysis support that AD is a systemic widespread disease that start from the human gut dysbiosis. The BA produced from amino acids by gut microbiome spread to the system through the damaged vascular and intestinal cells. This damage results from the BA non-specific cytotoxicity that can target and kill any cells in any organs of the human body including brain, vascular, and intestinal cells while the BA affinity to its degrading MAO enzymes is lower than BA affinity to ARS.