
Abstract
Background:
Although the effects of various types of cognitive interventions have been evaluated, effectiveness and cost-saving effect of the combination of the different cognitive interventions is unknown.
Objective:
This study aimed to evaluate the feasibility of conducting a definitive trial to assess the effectiveness of combined cognitive intervention.
Methods:
A matched controlled trial of learning therapy (LT), a combination of cognitive training and stimulation, was conducted. The samples were recruited from the nursing homes. Inclusion criteria were as follows: age 65 years or older, clinical diagnosis of dementia, level of activities of daily living at II or above, Mini-Mental State Examination score between 10 and 26, receiving long-term-care services without history of LT, and provision of written consent. The primary outcomes were safety, validity of eligibility, retention rate, and effect on the functions of daily living represented by Criterion Time for Certification of Needed Long-Term-Care (CT for CNLTC) at 12 months. Cost-benefit analysis was also conducted to assess the cost saving effect of LT.
Results:
No serious adverse events were detected. The exclusion rate at the screening phase was 5% and the retention rate was 77% at 12 months. LT demonstrated statistically significant improvement in CT for CNLTC at 12 months (Δ=18.8, almost equivalent to “one” degree of the care needed level) and saved the long-term-care cost by JPY 200,000 (USD 1,618).
Conclusions:
LT is effective for improving care recipients’ level of care needed and has a cost saving effect. A randomized controlled trial is required to verify these findings.
Clinical Trial Registration:
This study was approved by the ethics committee at Keio University School of Medicine (ID: 20150061). This trial was registered at University hospital Medical Information Network Clinical Trial Registry (UMIN-CTR ID: UMIN000018223).
INTRODUCTION
Because dementia is now a global issue, many countries recognize it as a societal challenge, and policies for treatment of dementia at the national and regional level have been developed [1-3]. In 2015, 46.8 million people across the world developed dementia, and by 2050, the number will rise to 131.5 million [4]. Such a rapid rise in its prevalence will lead to considerable burden on the society. In 2015, the global cost of dementia was estimated to be 818 billion USD and is expected to reach 2 trillion USD in 2030 [4]. From the estimates in specific countries, the societal cost of dementia in the US was 157–215 billion US dollars [5], 26 billion pounds in UK [6], and 1.45 trillion yen in Japan [7]. Additionally, 80%–90% of the total cost consists of the cost for care [5–7], and the cost for care increases as the level of care needed increases [8].
Because the pharmacotherapy lacks evidence for improving behavior problems, quality of life, time of entry into an institution, mortality, progression of disease, and burden of illness on caregivers [9–12], non-pharmacological therapies such as cognitive interventions have received considerable attention [13–15]. Cognitive interventions are divided into three sub-categories: cognitive stimulation, cognitive training, and cognitive rehabilitation [16]. Cognitive stimulation focuses on the enhancement of cognitive and social functioning through group interactions and activities [17]. Cognitive training involves a theory-based standardized curriculum, which involves individual or group-based learning in order to improve the cognitive function [18], and it sometimes involves learning through a computerized program [19–22]. Cognitive rehabilitation aims to mitigate the effect of cognitive impairment on the functions of daily living through individualized programs to learn how to cope with difficulties of the specific activities of daily life [20, 23].
Although the outcomes of cognitive interventions have been meta-analyzed in several studies [24–29], the results have been inconsistent. One study [27] revealed that cognitive training improves both cognitive function and the functions of daily living in people with dementia. However, Olazaran et al. [26] and Bahar-Fuchs et al. [28] failed to show any significant effect on the cognitive function and the functions of daily living with cognitive training and rehabilitation. Oltra-Cucarella et al. [30] conducted a meta-analysis controlling effects of the control group, and showed that while the cognitive training improved the cognitive function considerably, no improvement was detected for the functional outcomes. On the contrary, cognitive rehabilitation improved function in targeted domains, but no notable improvement was observed for the cognitive function.
Although the previous studies provided relevant information about cognitive interventions, some limitations still exist. First, long-term outcomes when two cognitive interventions (e.g., cognitive training and cognitive stimulation) are used in conjunction have not been evaluated. Second, it is not clear whether cognitive interventions contribute to cost saving of the public the long-term-care expenditure.
“Learning therapy” (LT) is a combined form of cognitive training and cognitive stimulation developed by Kawashima and Yamasaki and KUMON Institute [31]. In this program, instructors encourage people with dementia to practice simple calculation, reading dialogue, and open dialogue between the instructors and participants. The instructors are encouraged to praise and acknowledge when participants have accomplished an exercise. The safety, feasibility, and efficacy of LT on cognitive function have been investigated in previous study [32]. It reported no serious side effects, acceptable discontinuous rate, and statistically significant improvement in cognitive function, measured by the Mini-Mental State Examination (MMSE) [33] at 6 months [32]. However, the effect of long-term LT, especially on the function of daily living, is still unknown. Furthermore, the cost-saving effects of LT on long-term-care insurance has not been quantified.
Therefore, we conducted a pilot study to assess the feasibility of conducting a randomized trial and provide data estimating the parameters required to design such a trial. There were two main objectives of this preliminary trial. The first objective was to investigate the feasibility of the definitive trial by assessing the safety of the intervention, the validity of the eligibility criteria for the trial, and the retention rate at 5 and 12 months. The second objective was to evaluate the clinical outcomes by estimating a mean difference between groups in the function of daily living and the reduced monetary load on the national long-term-care insurance.
METHODS
Design
This was a prospective matched controlled trial of two parallel groups over one year. The protocol of the trial can be referred from the trial’s registration [34]. This study was conducted in 23 residential nursing homes across Japan.
Recruitment procedure
Prospective participants for both groups (i.e., the intervention and the controlled group) were recruited from each nursing home in July 2015. We first recruited the participants for the intervention group before recruiting volunteer participants at each facility that met the same inclusion criteria to serve as the control group. Face-to-face interviews were held with their proxies in order to provide sufficient information regarding the risk and benefit from participation in the trial. Eligibility was also confirmed from the interviews as well as on the basis of the inclusion and exclusion criteria mentioned below. Those who agreed to participate in the trial and their proxies were requested to provide written informed consent.
Ethics approval
This study was approved by the ethics committee at Keio University School of Medicine (ID: 20150061). This trial was registered at University hospital Medical Information Network Clinical Trial Registry (UMIN-CTR ID: UMIN000018223) [34].
Inclusion criteria
Participants were eligible for inclusion if they met the following criteria: age 65 years or older; clinical diagnosis of dementia by a physician; the long-term-care insurance; and the level of activities of daily living II or above, as assessed of late by the long-term-care insurance service scheme; provision of written informed consent; baseline score between 10 and 26 on MMSE; living in nursing homes; and no previous experience of the intervention.
Exclusion criteria
Those who had difficulty in undergoing follow-up for longer than six months after the baseline assessment (e.g., people expected to be discharged from the nursing homes shortly) and any other severe medical condition that made participation in the study difficult were excluded.
Allocation
Because this was not a randomized controlled trial (RCT), we recruited the participants who wished to undergo interventions and the control group simultaneously in each nursing home.
Procedures
Participants allocated to the LT arm were provided 30 min of intervention daily, 5 days a week, for a pair of participants (an instructor and two participants). The instructors, who were caregivers at each nursing home and had approximately a 10-h official training before starting LT under supervision, including learning how to properly use the materials and how to relate and provide feedback to the participants, offered LT following the manuals. The study period was between July 2015 and July 2016.
LT is a combined form of cognitive training and cognitive stimulation aiming to improve the function of daily living by increasing motivation and self-esteem through simple tasks: arithmetic calculation and reading aloud a paragraph of sentences [31]. Typically, each participant, on average, completed 6 worksheets of each task specifically prepared for each participant, followed by assessment by the instructors. Throughout the sessions, instructors were urged to praise and encourage the participants in a kind manner. When participants had difficulty, the instructors gave them appropriate guidance to help them complete the tasks. The participants spent the first 20 min reading/writing and solving arithmetic problems (i.e., cognitive training) and the last ten minutes for group conversation facilitated by an instructor (i.e., cognitive stimulation). Through this process, the participants’ sense of self-efficacy and connection with others was enhanced. The level of tasks offered to each participant was determined from 18 levels based on the results of a brief pre-test using materials from the LT to assess individual cognitive ability.
Feasibility outcomes
Feasibility outcomes were assessed by safety (assessed by the occurrence of any serious adverse events), validity of eligibility criteria (assessed by the exclusion rate at the screening stage), and retention rate at 5 and 12 months.
Clinical outcomes
Primary clinical outcome
The primary clinical outcome was the mean difference in the level of care needed, measured by the change in Criterion Time for Certification of Needed Long-Term Care (CT for CNLTC) between the two groups. We compared the change in CT for CNLTC in both groups, adjusting covariance of the samples, i.e., age, sex, the care needed level, level of activity of daily living, MMSE [33], Frontal Assessment Battery (FAB) [35], Physical Self-Maintenance Scale/Instrumental Activity of Daily Living (PSMS/IADL) [36], and EuroQuality of Life 5-dimension-5 L (EQ5D) [37] by the propensity score. We measured CT for CNLTC at baseline and at 5 and 12 months. We selected CT for CNLTC as the primary outcome for two reasons. First, CT for CNLTC is the structured and standardized framework used to assess the level of care needed nationwide in Japan. Second, the score of CT for CNLTC determines the expenses covered by long-term-care insurance; hence, it helps determine monetary benefits and is useful for cost-benefit analysis (CBA). If an elderly person wishes to receive the long-term-care services, she/he needs to receive assessment for the CT for CNLTC. The care manager assesses the elderly individual’s physical and mental functions in five areas (i.e., activities of daily living, instrumental activities of daily living, behavioral and psychological symptoms of dementia, functioning training related activity, and medical related activity), with 80 questions in total. The assessment questions and the methods for evaluating each question are completely standardized and manualized [38] in order to minimize variability. The CT for CNLTC is automatically generated by the computer program, which predicts CT for CNLTC on the basis of the assessment results. The level of care needed is determined by the score of CT for CNLTC. Higher scores indicate that more advanced care is needed. A score of > 32 is recognized as the “care needed” state, as shown in Supplementary Table 1. In this trial, the primary outcome was assessed by independent assessors at baseline and at 5 and 12 months. Independent assessors were masked as much as possible. Participants and their caregivers were instructed not to disclose their allocated treatment during the assessment interviews.
Cost-benefit analysis
With respect to economic evaluation, we conducted CBA using the scores of CT for CNLTC as clinical outcomes rather than cost-effectiveness analysis (CEA) with EQ5D because CBA would have a bigger impact than CEA since the results of CBA are easier to understand and apply. CBA results are represented by “net monetary benefit,” while CEA results are represented by “incremental cost effectiveness ratio.”
Cost-benefit analysis was conducted by calculating the average net monetary benefit. In order to estimate the net monetary benefit, first, the effectiveness measured by CT for CNLTC was converted into monetary benefit. As previously mentioned, the upper limit of the expenses covered by the public the long-term-care insurance is determined by the level of care needed, which is categorized depending on the CT for CNLTC (i.e., CT for CNLTC, 32–49, 50–69, 70–89, 90–109, and 110-, corresponding to the care needed level from 1 to 5, respectively). Based on the “tariff” established by the government (Supplementary Table 1) [39] and the distribution of the participants’ care needed level (56 of 57 participants’ care needed level were between levels 1 and 4), we determined that one unit of CT for CNLTC is equivalent to JPY 2,590 (USD 21.0) per month. This figure was calculated by dividing JPY 202,000 (JPY 306,000 [upper limit at care needed level 4] – JPY 104,000 [upper limit at support needed level 2] by 78 units (i.e., total units of CT for CNLTC between care needed levels 1 and 4). With respect to cost, the wages of the instructors and the cost for LT materials were included in the assessment. Hourly wage of the instructors was JPY 1,702 (USD 13.8), derived from the national survey in 2013 [40], and the monthly material costs were set as JPY 2,000 (USD 16.2) (i.e., the price regulated by the KUMON Institute). Cost-benefit analysis was conducted by the bootstrap method. The bootstrap method is based on generating multiple replications of the statistic of interest by sampling with replacement from the original data [41]. By repeating and re-sampling for 500 times, mean net monetary benefit and the probability of cost saving were calculated. The costs were presented both in JPY and USD (JPY 129.24 was assumed equivalent to USD 1 based on the purchasing power parity in July 2015) [42]. Analyses were conducted from the national long-term-care insurance perspective.
Secondary clinical outcomes
To evaluate the broad range of the participants’ functions, the secondary clinical outcomes involved MMSE [33], FAB [35], PSMS/IADL [36], and EQ5D [37]. These scales were assessed at the baseline, 3 month, 5 months, 9 month, and 12 months. In this study, we targeted people with dementia, including those with severe cognitive impairment. We were concerned that results from self-reported rating scales would lack validity. Therefore, we decided that caregivers at the institutions, who were involved in the daily care of the recipient, should rate the scales based on their observations of the participants. A brief description of each scale is given below.
MMSE: MMSE is a simplified scored form of the cognitive mental status examination. This form includes 11 questions and requires only 5–10 min to administer; therefore, it is practical to use serially and routinely. The score ranges from zero to 30. Lower scores indicates lower cognitive function [33].
FAB: FAB consists of six subtests exploring the following: conceptualization, mental flexibility, motor programming, sensitivity to interference, inhibitory control, and environmental autonomy. The FAB is easily administered at bedside and takes approximately 10 min. A higher score (the highest is 18) indicates better function [35].
PSMS/IADL: PSMS/IADL is a device developed by Lawton et al., which assesses “Physical Self-Maintenance” and “Instrumental Activity of Daily Living.” PSMS evaluates six types of behavior, such as using the toilet, feeding, dressing, grooming, physical ambulation, and bathing. IADL assesses the functions such as the ability to use the telephone, shopping, food preparation, housekeeping, laundry, using a mode of transportation, managing medications, and handling finances. Each behavior in PSMS and function in IADL is scored zero or one. Then, the scores of PSMS and IADL range between zero to six and zero to eight, respectively. A higher score represents better function [36].
EQ-5D: EQ-5D comprises a short, descriptive, system questionnaire and a visual analogue scale (EQ VAS) that are cognitively undemanding, taking only a few minutes to complete. The questionnaire provides a simple descriptive profile of a respondent’s health state. The EQ5D VAS provides an alternative way to elicit an individual’s rating of their own overall current health. When the descriptive system profile is linked to a “value set,” a single summary index value for health status is derived. This index value, ranging between zero (or death) and one (or perfect health) can be used in economic evaluations of healthcare interventions [37].
Sociodemographic data obtained at baseline included age, sex, level of care needed, and the level of activities of daily living. Information of the number of the LT sessions during the intervention period was also collected to assess the engagement of the participants.
Statistical analysis
Because there are no previous studies that have evaluated the effect of LT for the level of care needed under the long-term-care insurance scheme, we did not perform a formal sample size calculation. Considering the feasibility of the study, we decided to recruit 30 participants for each group, with 60 samples in total.
Analysis was conducted on an intention-to-treat basis for all samples. With respect to the primary and secondary outcomes, the least-squares means (LS means) and their 95% confidence intervals (CIs) were estimated using a mixed-effects model for repeated measures (MMRM) that includes treatment group, week, and group-by-week interaction as fixed effects with a compound symmetry covariance matrix among time-points; Kenward–Roger degrees of freedom adjustment was used. Mean for each group at each time-point and between-group mean differences were estimated using appropriate contrasts in the MMRM. Missing values were not imputed.
With respect to cost-benefit analysis, missing data were imputed by Last Observation Carry Forward. The significance level was set at 0.05 (two-tailed) for all analyses.
In order to ascertain the robustness of the results of the primary clinical outcome with ITT analysis, two sensitivity analyses with the completers samples and the samples alive at the end of the study period were conducted. Statistical analyses were performed with SPSS version 9.3 (IBM, Armonk, NY, USA), EXCEL ver. 16 (Microsoft, Redmond, WA, USA), and STATA ver. 13 (StataCorp, College Station, TX, USA).
Role of the funding source
The Ministry of Economy and Trade and Industry had no role in the following processes: the study design, collecting data, analysis, interpretation, and in the writing of the paper. KUMON Institute, the other funding source, had a role in collecting data from each facility and no role in the study design, analysis, interpretation, and in the writing of the paper. The corresponding author and two coauthors (KF and AN) have had full access to all the data used in this study. Final responsibility for the decision to submit the paper for publication lies with the corresponding author.
RESULTS
Participant characteristics
Table 1 shows the basic characteristics of the included participants. There were no significant differences in age, sex, care needed level, ability to perform ADLs, CT for CNLTC, MMSE, FAB, IADL, PSMS, and EQ5D among the groups.
Baseline sociodemographic and clinical characteristics
CT for CNLTC, Criterion Time for Certification of Needed Long-Term Care; MMSE, Mini-Mental State Examination; FAB, Frontal Assessment Battery; PSMS, Physical Self-Maintenance Scale; IADL, Instrumental Activities of Daily Living; EQ5D, Euro-QoL 5 dimension.
Feasibility outcomes
With respect to the safety of the interventions, no severe adverse events were documented in either arms during the study period. Figure 1 indicated the flow of the study participants. Among 30 eligible participants in each arm, three in the control arm were excluded. Thus, 30 and 27 participants in the LT and control arms, respectively, were included. Six and 13 of 57 participants lacked assessment at 5 and 12 months, respectively. The reasons were discharge from the institution (2 in LT and 4 in control), death (2 in LT and 2 in control), and withdrawal from the study (2 in LT and 1 in control). The average number of LT sessions was 175.3 (SD: 70.2).
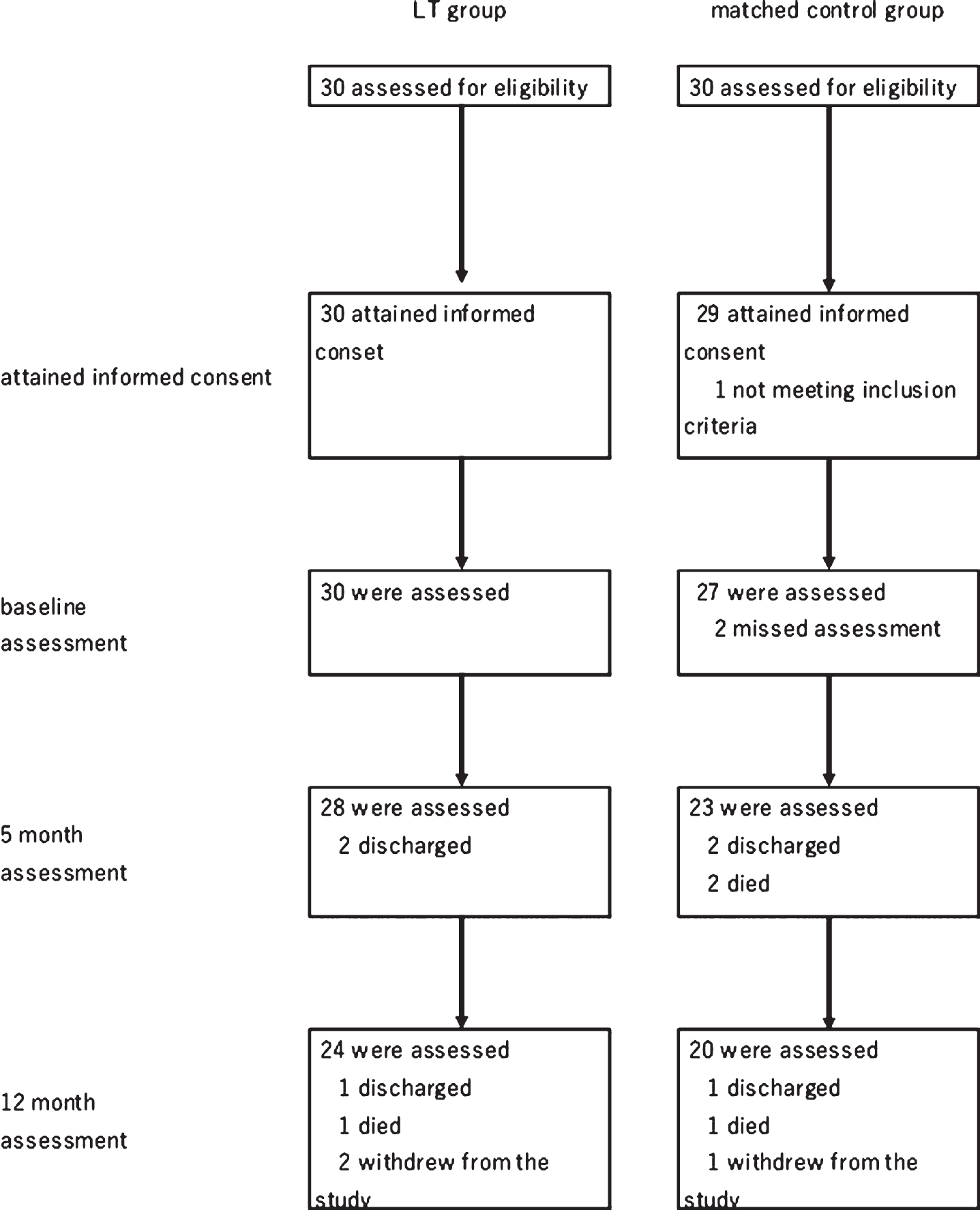
Flow chart of the participants in the study.
Primary clinical outcome
The mean changes in CT for CNLTC at 12 months were greater for the control than the LT arm (17.5 versus 0.8) and the mean difference in CT for CNLTC among the groups at 12 months were significant (Δ=18.8 [p = 0.01]), while that at 5 months did not reach significance (Δ=9.0 [p = 0.23]) (Table 2).
Transition of the primary and secondary outcomes
CT for CNLTC, Criterion Time for Care needed of Long-Term Care; MMSE, Mini-Mental State Examination; FAB, Frontal Assessment Battery; IADL, Instrumental Activities of Daily Living; PSMS, Physical Self-Maintenance Scale; EQ5D, Euro-QoL 5 dimension.
Cost-benefit analysis
The results of 500 times bootstrap simulation revealed that the incremental benefit and cost of LT at 12 months was JPY 296,732 (USD 2,400) and JPY 98,326 (USD 795), respectively. Thus, the net monetary benefit was JPY 198,406 (USD 1,605) (Table 3). Figure 2 shows the scatter plots of 500 times bootstrap simulations. The results revealed that the probability of the net monetary benefit being beyond zero (i.e., the probability of cost saving) was 90.8%.
Results of 500 times probabilistic sensitivity analysis
LT, learning therapy; NMB, net monetary benefit. one JPY was equal to 123.62 USD.
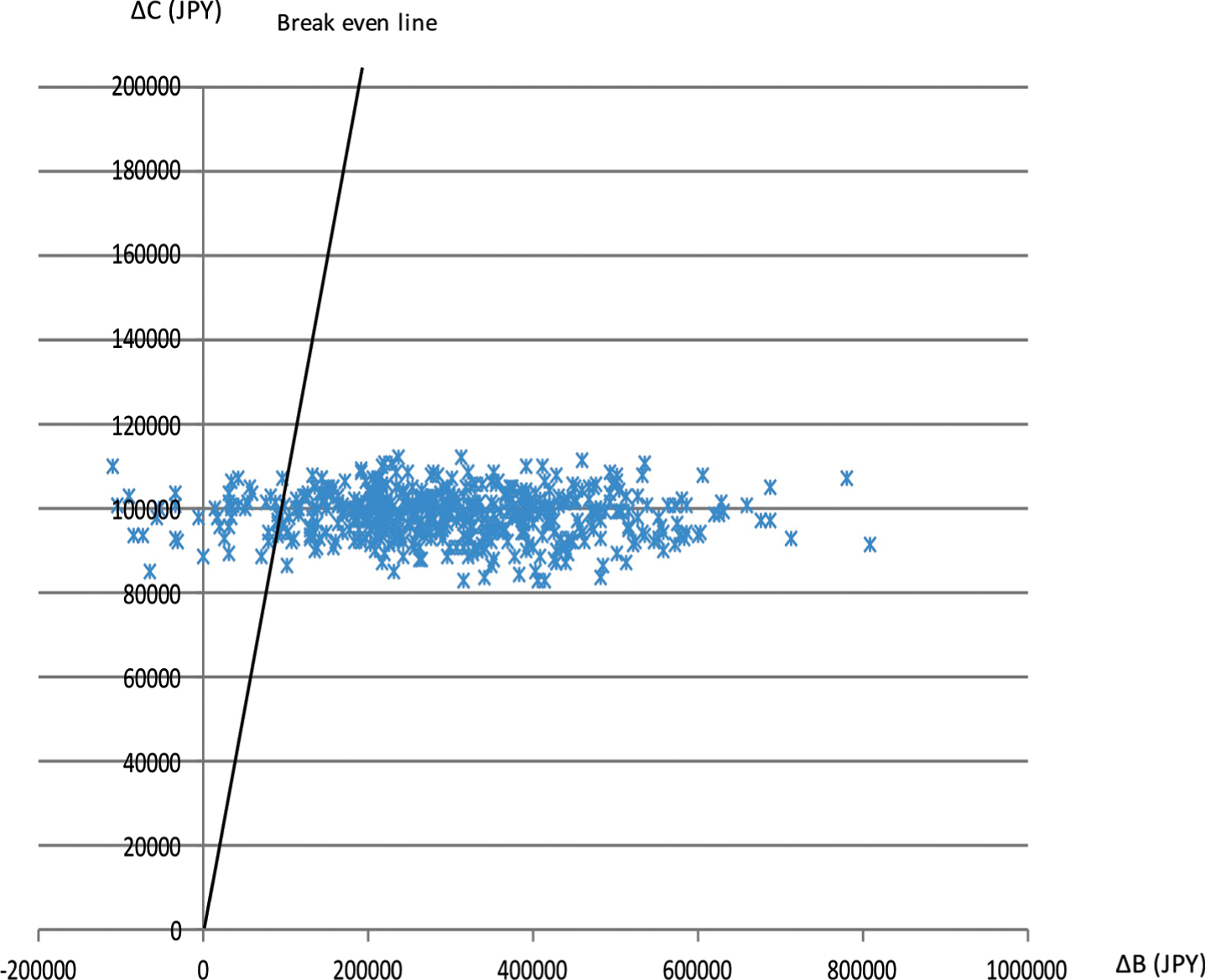
Scatter plots of the results of bootstrap re-sampling.
Secondary clinical outcomes
As shown in Table 2, although the between-group difference in EQ5D (0.10, p = 0.01) and IADL (0.6, p = 0.05) at 5 months was significant, no other scale showed any significance.
Sensitivity analysis
The results of the two sensitivity analysis with completers sample and the alive samples at 12 months indicated that the results of the primary clinical outcome and cost saving analysis were unchangeable from ITT analysis (completers samples: Δ=17.6 (p = 0.02), expected CBA = JPY 192,523 (USD1,557), probability of LT being cost benefit 88.8%; alive samples: Δ=20.0 (p = 0.01), expected CBA = JPY 244,581 (USD 1,978), probability of LT being cost benefit 93.2%). Therefore, we judged the results of ITT analysis were robust.
DISCUSSION
Although numerous studies to date have evaluated the effectiveness of each specific cognitive interventions, no study has assessed the effects of combinational interventions or their effect on saving the long-term-care insurance expenditure. This study was unique in that context.
The present findings indicated that LT improved the care-needed level but did not improve the cognitive function. These results seem to contradict Kawashima’s results indicating the LT improved MMSE significantly. However, the significance in the previous study was at six months. Although the mean difference in MMSE in the study did not reach significance, it showed significant tendency at five months (p = 0.07). Therefore, we judged the difference between two studies was acceptable. The result in the study was similar to the results related to cognitive rehabilitation, rather than cognitive training, which improved the function of daily living, despite no improvement in cognitive function. While the study was still being designed, we hypothesized that LT would improve cognitive function more than the function of daily living because LT is majorly cognitive training despite being a combination program. However, the results revealed a contrast. We thought the discrepancy occurred because positive feedback, given during cognitive stimulation, like appraisal and acknowledgment played a significant role despite having a shorter role in LT. Moreover, the cognitive training may have served as a medium to provide such positive feedbacks. By completing LT practice daily, the participants showed improvement in self-efficacy and motivation. Subsequently, the careers can more easily transform such positive psychological changes to improving the function of daily living by targeting the next challenging behavior, such as eating or cleaning with less support. Once they succeeded in improving the function of daily living, they were more motivated and engaged more in the LT, leading to a virtuous cycle. In this context, LT worked not only as cognitive training, but also as in assisting the careers to support the care recipients in improving their function of daily living. Thus, LT seemed to affect the function of daily living more rather than the cognitive function.
With respect to the magnitude of LT’s effect on the function of daily living, the results showed that LT improved 18.8 unit of CT for CNLTC, which is almost equivalent to “one” care-needed level. The difference is substantial from the clinical perspective because the difference between the care-needed levels 2 and 3 is described as follows. Level 2: People who need partial daily assistance for either activity of daily living or instrumental activity of daily living. Level 3: People who need full daily assistance for either activity of daily living or instrumental activity of daily living [43]. However, this impact became more prominent when we observed the effect of LT on cost saving, because it saved JPY 200,000 annually. This results in a win-win relationship between the individuals with dementia and the society.
Although this study provides insightful results, it has some limitations. First, this was not an RCT. Therefore, we could not exclude all biases that we can in an RCT. Second, although the care recipients and caregivers were asked to not reveal their group to the assessors of CT for CNLTC, we did not determine whether the assessors were blinded. Subsequently, the possibility of an assessment bias was not excluded. Future research must address these limitations.
Conclusions
The effect of LT on the function of daily living and cost saving for the long-term-care insurance were evaluated in the matched controlled study. The results indicated that LT improves the function of daily living and saves the long-term-care insurance expenditure. An RCT must be conducted in future to ascertain these results.
List of the residential nursing homes participated in the study
Fureai-no-sato Dokai, Eijuen, Koyoju, Hidamari-no-ki, Sakuranbo, Felio Momochi, Felio Tenjin, Care house Donguri, Group home Donguri, Rikigo-Tsukushi-an, Seifuen, Grand home Furugo, Care manshion Hidaka, Izumi-no-sono, Wakoen, Nikkai care center Rokucho, Silver support Hoshi-ni-negai-wo, Sowaen, Accommoder, Tateyama care center Yume club, Country harvest Kitamoto, Ikoi-no-ie, and Ikoi-no-ie Kanegae.
Footnotes
ACKNOWLEDGMENTS
We would like to thank all residential nursing homes for their contribution to this study implementation. The nursing homes that cooperated for this study are listed below. We also would like to express our gratitude to KUMON Institute for their contributions in collecting data from these nursing homes.