
Abstract
Background:
The lack of effective pharmacological or behavioral interventions for memory impairments associated with Alzheimer’s disease (AD) emphasizes the need for the investigation of approaches based on neuromodulation.
Objective:
This study examined the effects of inhibitory repetitive transcranial magnetic stimulation (rTMS) of prefrontal cortex on recognition memory in AD patients.
Methods:
In a first experiment, 24 mild AD patients received sham and real 1Hz rTMS over the left and right dorsolateral prefrontal cortex (DLPFC), in different sessions, between encoding and retrieval phases of a non-verbal recognition memory task. In a second experiment, another group of 14 AD patients underwent sham controlled repeated sessions of 1Hz rTMS of the right DLPFC across a two week treatment. Non-verbal recognition memory task was performed at baseline, at the end of the two weeks period and at a follow up of 1 month.
Results:
Right real rTMS significantly improved memory performance compared to right sham rTMS (p = 0.001). Left real rTMS left the memory performance unchanged as compared with left sham rTMS (p = 0.46). The two sham conditions did not differ between each other (p = 0.24). In the second experiment, AD patients treated with real rTMS showed an improvement of memory performance at the end of the two weeks treatment (p = 0.0009), that persisted at 1-month follow-up (p = 0.002).
Conclusion:
These findings provide evidence that inhibitory rTMS over the right DLPFC can improve recognition memory function in AD patients. They also suggest the importance of a new approach of non-invasive brain stimulation as a promising treatment in AD.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the most common type of dementia, characterized by a progressive impairment of episodic memory function, progressively leading to global cognitive decline [1]. Neurodegenerative processes associated with AD induce hippocampal atrophy and a gradual disruption in functional connectivity between brain systems, particularly those dedicated to memory [2]. No currently existent treatments can prevent or efficiently cure the memory and/or the other cognitive deficits associated with AD. Pharmacological interventions remain purely symptomatic and, so far, are unable to stop the disease-related neuropathological changes [3]. This stresses an imperative need for the further investigation of alternative or adjunctive therapeutic interventions for AD.
Non-invasive brain stimulation methods, such as repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS), may represent alternative tools targeting the improvement of cognitive function in AD [4–6]. Brain stimulation induces modulation of neural excitability in the targeted brain regions as well as in the adjacent functionally connected areas [7, 8]. Importantly, these neuromodulatory changes and the resulting behavioral effects are known to outlast the stimulation duration [9] enabling to modulate neural activity underlying cognitive processes [10, 11].
Although a number of studies have suggested that brain stimulation may represent a promising tool targeting cognitive impairments in AD and other dementing illnesses [4], there is still seldom and contrasting information on the therapeutic potential and the mechanism of action of these techniques. A handful of studies reported that increasing excitation over temporal/parietal and prefrontal areas using excitatory brain stimulation methods, such as anodal tDCS or high-frequency rTMS enhances cognitive functions in patients with mild cognitive impairment (MCI) and AD, as well as in elderly with subjective memory complaints [12–21]
Looking specifically at the effects of anodal tDCS on episodic memory in AD, Ferrucci et al. [22] reported an improvement in a word recognition memory test in ten mild AD patients following bilateral anodal tDCS delivered over the temporo-parietal areas. Boggio et al. [23] reported enhanced visual recognition memory performance in ten mild-to-severe AD patients after anodal tDCS applied over the temporal and the prefrontal cortices. In a subsequent study of 15 AD patients, the same researchers demonstrated lasting visual recognition memory improvement following anodal tDCS applied bilaterally over the temporal areas [24].
In another single case study [25], an improvement of several cognitive measures, including immediate visual memory, was observed following two cycles of anodal tDCS of the left dorsolateral prefrontal cortex (DLPFC) in a patient with posterior cortical atrophy.
On the other hand, Cotelli et al. [26] reported a significant improvement in face-name associations learning following memory training irrespective of whether placebo or anodal tDCS was applied over the left DLPFC of mild-to-moderate AD patients.
As to TMS interventions in AD, while most studies targeted the left DLPFC, there are some studies exploring TMS effects on episodic memory targeting other brain regions. Koch and colleagues [27] chose as a target of neuromodulation the default mode-network, whose intrinsic connectivity is abnormal in AD, and it is suggested to be one of the earliest hubs of disease degeneration [28]. The authors found an improvement of long-term memory in AD after 2 weeks of high-frequency excitatory rTMS of the precuneus.
As it can be seen from this literature review, few studies have explored the effects of inhibitory neurostimulation on episodic memory in neurodegenerative disorders. A deficit of inhibition is encountered since the early stages of neurodegenerative disorders, and it is putatively linked to the amyloid cascade hypothesis and to network dysfunction [2]. Furthermore, neuroimaging studies reported increased activation in the right DLPFC combined with memory deficits in MCI and AD [29, 30], and some studies [31] showed an inverse relationship between right DLPFC activation and episodic memory performance. Therefore, targeting inhibitory neurotransmission through brain stimulation could represent a reasonable option for treatment of memory deficits in neurodegenerative disorders.
Turriziani and colleagues [32] explored the effects of 1Hz rTMS applied over the right and the left DLPFC during a non-verbal recognition memory task to MCI patients. A significant improvement in recognition memory performance was documented following application of these inhibitory rTMS trains to the right, but not to the left DLPFC. A similar pattern of results in MCI patients was recently reported by Cui et al. [33].
Since MCI and AD are considered to lie on a continuum of the same neurodegenerative processes, one could hypothesize that low-frequency inhibitory rTMS of the right DLPFC might improve memory performance also in patients with AD.
The aim of the present study was to investigate whether inhibition of the right DLPFC can enhance memory performance in AD. Over two different experiments, we tested the effects of 1Hz rTMS delivered in a single or in repeated sessions to the right and left DLPFC on non-verbal recognition memory tasks in mild AD patients.
MATERIALS AND METHODS
Subjects
Experiment 1
Twenty-four native Italian-speaking patients (15 females and 9 males) in the dementia phase of AD [34] were recruited from a neurologically-led cognitive disorders clinic. Patients underwent, for diagnostic purposes, a complete clinical investigation, including medical history and neurological examination, a complete blood screening, a neuropsychiatric evaluation, a brain MRI scanning, and an extensive neuropsychological assessment exploring all cognitive domains. They were rated on some standardized clinical scales that included MMSE, Activity Daily Living (ADL), and Instrumental Activities of Daily Living scale (IADL). Complete laboratory analyses and neuroimaging diagnostic procedures (MRI) were carried out to exclude other causes of progressive or reversible dementias, to have a clinically homogenous mild AD patient group. In all patients, signs of concomitant cerebrovascular disease on MRI scans were carefully investigated and excluded in all patients. Informed consent was obtained from all patients in accordance with the independent local Ethics Committee.
All patients were on cholinesterase inhibitor (donepezil or rivastigmine) therapy.
Table 1 shows demographic and clinical data of AD patients.
Experiment 1. AD patients’ demographic, clinical data and cognitive scores
Experiment 2
Fourteen patients in the dementia phase of AD (5 males), different from those recruited in experiment 1, participated in this experiment. Demographic and clinical characteristics of the cohort are summarized in Table 2. They all completed the protocol successfully, attending all experimental sessions.
Experiment 2. Demographic data and neuropsychological assessment at baseline of the two groups of AD patients (real rTMS and sham rTMS group)
Experimental procedure
The same experimental task and procedure (Fig. 1A) previously used by Turriziani et al. [32] with MCI patients were adopted. Two versions (A and B) of a three-alternative, forced choice, pencil and paper non-verbal recognition memory task were administered (Fig. 1B). Both versions employed black and white photographs of unknown Caucasian women, approximately 25 years old, with Italian physiognomic characteristics, neutral expression, and no obvious distinguishing features.
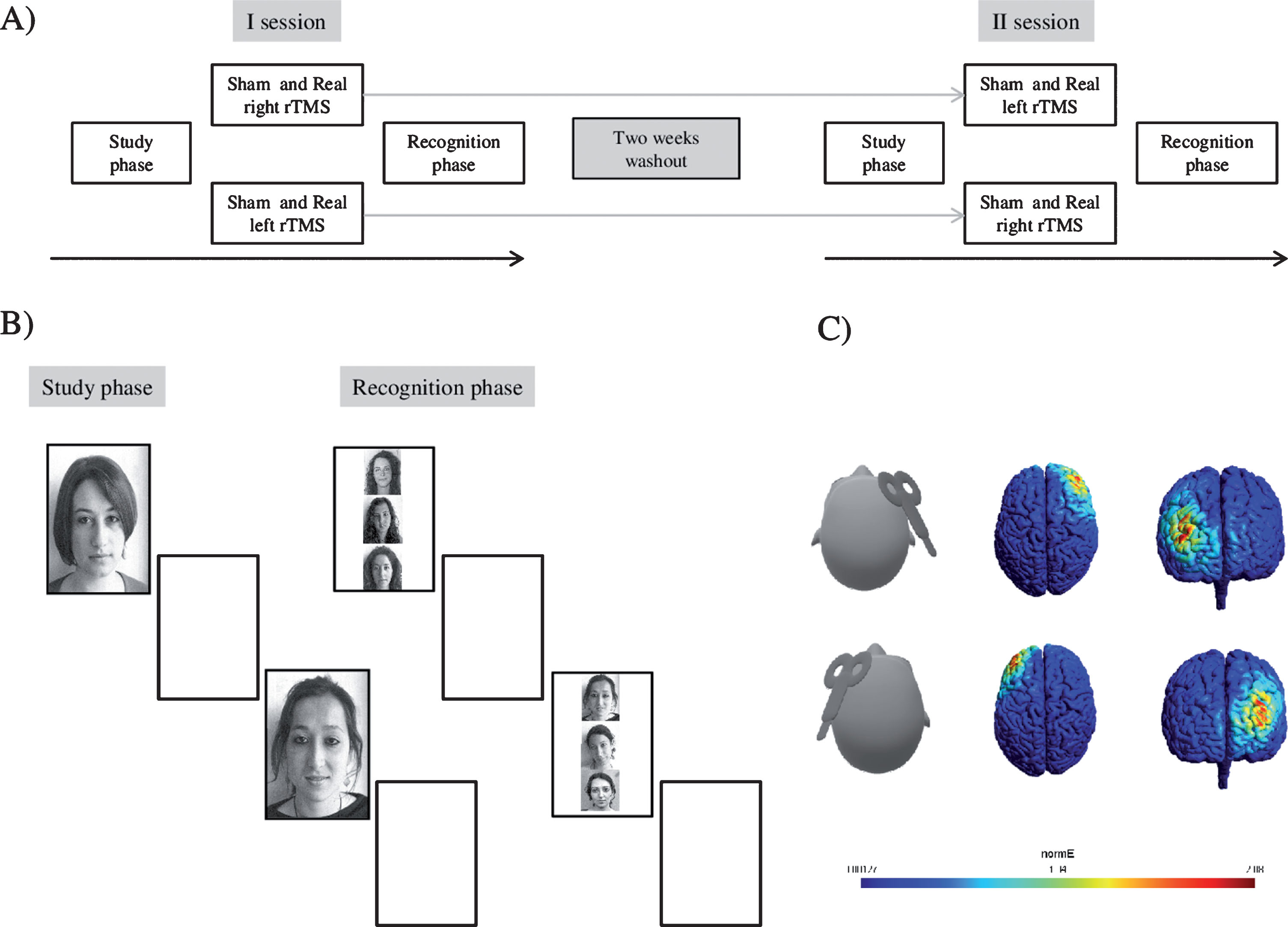
A) AD patients participated in two TMS sessions different as to the coil position. During the first session patients underwent to both a sham and a real TMS of the dorsolateral prefrontal cortex (DLPFC) in the left or in the right hemisphere. After a two weeks washout interval, patients were crossed over to a stimulation of the contralateral hemisphere. Patients performed the study phase of the recognition memory test (RMT), followed by 10 min of real or sham TMS. After TMS end, the recognition phase was performed. B) The “paper and pencil” task consisted of a study phase and a recognition phase. During the study phase, 30 study faces were presented for 3 s each. Encoding phase was followed by 10 min of real or sham TMS. After stimulation’s end, the recognition phase started and patients were presented with 30 triplets of stimuli comprising the target stimulus and two distracters vertically arranged. In this phase patients were asked to point to the stimuli they had seen before. C) Simulated electric field strength generated by the TMS figure-8 coil over the left and right DLPFC, respectively. The maximum strength of the electric field is color-coded from 0.00127 to 2.08 mV/mm.
There was a study phase and a recognition phase. In the study phase, 30 study stimuli were presented. Each stimulus was presented individually by the examiner on a white A4 sheet for 3 s. The recognition phase was administered after a 10-min interval. In the recognition phase, the examiner presented 30 triplets of stimuli comprising the target stimulus and two distracters on individual white A4 sheets. In each triplet, the target was presented with two other similar distracters, vertically arranged. The patients were asked to point to the stimulus they thought they had seen before.
During the 10-min interval preceding the recognition phase, real or sham rTMS were delivered. Sham rTMS was the control condition. Real rTMS and sham rTMS were delivered to the left and right DLPFC over four separate experimental sessions. There were two experimental sessions on one day (real rTMS and sham rTMS of one hemisphere) and two experimental sessions two weeks later (real rTMS and sham rTMS of the other hemisphere; see Turriziani et al. [32] for further details). The order of administration of real rTMS, sham rTMS and of the two memory tasks was counterbalanced across subjects and across the four experimental sessions.
rTMS was delivered by means of a MagStim Super-Rapid magnetic stimulator (Magstim Company, Whiteland, Wales, UK), using a figure-of-eight coil (70 mm in diameter). In all patients, rTMS was applied over the left and right DLPFC. For localization of the left and right DLPFC, the tip of the intersection of the two coil loops was lined up with the F3/F4 sites of the 10–20 EEG system. The Tailarach coordinates of the stimulated cortical site were automatically estimated in a representative subject from an MRI constructed stereotaxic template using Softaxic software. The coil was positioned over the DLPFC and constantly monitored using the Softaxic neuronavigation system (EMS, Bologna, Italy) coupled with a Polaris Vicra infrared camera (NDI, Waterloo, Canada). They corresponded approximately at±41, 44, and 29. The electric field induced by this coil position was simulated using SimNIBS 2.0 [35] and a finite element head model template (Fig. 1C). The simulation revealed the target regions as the left or the right DLPFC. Inhibitory rTMS was applied using trains of 600 stimuli at a frequency of 1Hz and at an intensity of 90% of the motor threshold (MT). MT was defined as the lowest TMS intensity (as assessed by single-pulse TMS) able to induce a visible muscle twitch of the contralateral hand in at least 50% of a sequence of 10 consecutive trials. MT was determined on the same hemisphere of the stimulated DLPFC. There were no interhemispheric differences in MT values (left hemisphere: 56.6±5.6%; right hemisphere: 56.2±6.5%). Sham rTMS blocks were conducted with the coil positioned perpendicular to the scalp ensuring that no magnetic stimulation reached the brain.
In experiment 2, patients were randomly assigned to two groups: a sham rTMS group, undergoing to sham 1Hz rTMS of the right DLPFC, and a real rTMS group, undergoing real 1Hz rTMS of the right DLPFC. In both groups, 1Hz rTMS trains of 600 stimuli were delivered over the right DLPFC for five consecutive days per week across a two-weeks treatment (i.e., 10 sessions).
rTMS intensity was set at 90% of individual motor threshold, as in experiment 1. Localization of the target right scalp site was made as described for experiment 1.
In both rTMS groups, non-verbal recognition memory task was administered at baseline (T0), at the end of the two-weeks treatment (T1), and at 1 month follow up (T2; see Fig. 2 for details).

Schematic representation of the experimental protocol in experiment 2.
RESULTS
Experiment 1
Accuracy (i.e., percentage of correctly recognized items) was analyzed using ANOVA for repeated measures, with Side (left versus right) as a between-subject effect, and Condition (sham versus real rTMS) as a within-subject factor. Planned comparisons were applied where appropriate.
Condition (F1,23 = 5.94, partial eta squared = 0.20, p = 0.02) effect was significant whereas Site effect was not (F1,23 = 2.06, partial eta squared = 0.20, p = 0.16). There was a significant Condition x Site interaction (F1,23 = 15.69, partial eta squared = 0.40, p = 0.0006). Right real rTMS significantly improved memory performance compared to right sham rTMS (F1,23 = 12.64, p = 0.001) (Fig. 3). In contrast, no significant difference was found between left real rTMS and left sham rTMS (F1,23 = 0.55, p = 0.46). The two sham conditions did not differ between each other (F1,23 = 1.40, p = 0.24).
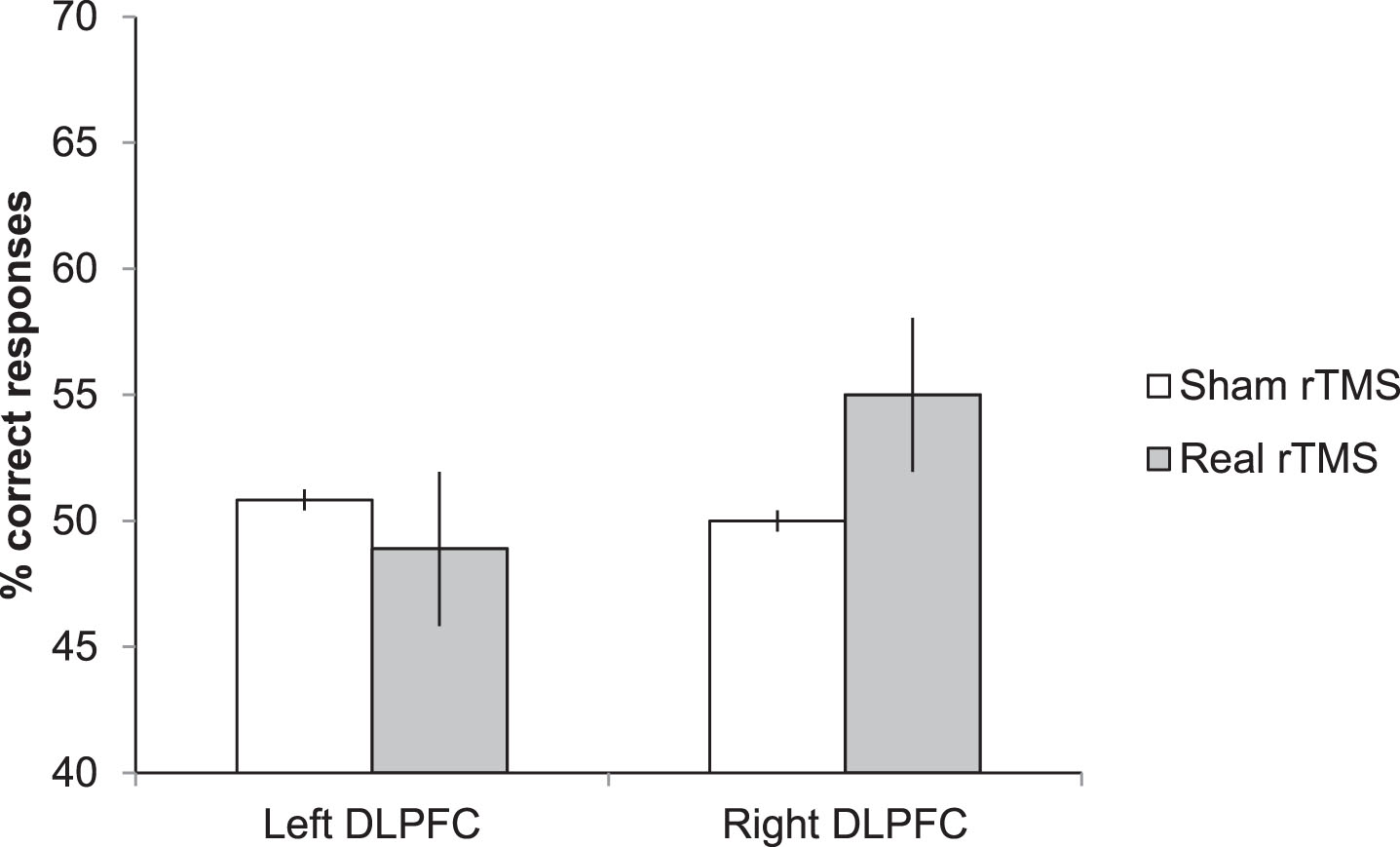
Experiment 1. Memory performance of AD patients following real rTMS and sham rTMS over the left and right DLPFC. Right rTMS significantly improves the performance on recognition memory test.
In addition, we explored whether the recognition memory improvement after low frequency rTMS over the right DLPFC is related to patients’ demographic, clinical, and cognitive characteristics. The rate of non-verbal recognition memory improvement for each AD patient was obtained by subtracting the recognition memory score (mean % correct) following right sham stimulation condition from the score following the right DLPFC rTMS condition (rate of improvement = right DLPFC rTMS – right DLPFC sham). We used Pearson’s correlation coefficient to explore the potential relationships between the rate of memory improvement in mild AD patients and their: 1) demographic and clinical characteristics; and 2) neuropsychological performance. The rate of memory improvement in mild AD did not correlate with patients’ age (r = 0.452, p > 0.47) or years of education (r = –0.298, p > 0.40). There was also no significant correlation between the rate of improvement and patients’ MMSE (r = 0.259, p > 0.47), ADL (r = 0.04, p > 0.66), and IADL scores (r = –0.264, p > 0.78). No significant correlations were found between the rate of memory improvement and the performance on neuropsychological tests (TIB: r = 0.11, p > 0.78; Rey’s 15 words immediate: r = 0.16, p > 0.66 and delayed recall: r = 0.31, p > 0.41; Rey’s Figure copy: r = 0.29, p > 0.43; Incomplete letters r = 0.44, p > 0.23; Stroop test completion time: r = –0.47, p > 0.23; number of Stroop errors: r = 0.08, p > 0.83; and the Naming test: r = 0.42, p > 0.25).
Experiment 2
No differences in age (F1,12 = 0.04, p = 0.82) and education (F1,12 = .72, p = 0.41) were observed in the two groups of AD patients. Moreover, there were no differences in MMSE (F1,12 = 1.59, p = 0.23), ADL (F1,12 = 1.00, p = 0.33), and IADL (F1,12 = 1.35, p = 0.26) scores. The groups of AD patients did not show any differences in all cognitive domain evaluated: Raven’s Progressive Matrices (F1,12 = 0.22, p = 0.64), Rey’s 15 words immediate recall (F1,12 = 0.79, p = 0.38), Rey’s 15 words 15-min delayed recall (F1,12 = 3.32, p = 0.10), VOSP (Incomplete Letters) (F1,12 = 0.01, p = 0.91), Attentional Matrices (F1,12 = 0.10, p = 0.74), Copying of drawings (F1,12 = 0.07, p = 0.79), Phonological verbal fluency (F1,12 = 0.21, p = 0.65), Naming Test (F1,12 = 2.16, p = 0.16).
Accuracy of verbal recognition memory tasks was analyzed using ANOVA for repeated measures, with Treatment (sham versus real rTMS), as a between-subject effect and Time (T0, T1, T2) as a within-subject factor. Planned comparisons were applied where appropriate. Treatment effect was not significant (F1,12 = 1.63, partial eta squared = 0.12, p = 0.22), whereas Time effect was significant (F2,24 = 6.21, partial eta squared = 0.34, p = 0.0067). There was a significant Treatment x Time interaction (F2,24 = 7.44, partial eta squared = 0.38, p = 0.0031). Planned comparisons revealed that real rTMS protocol significantly improved memory performance in T1 compared to T0 (F1,12 = 19.08, p = 0.0009). Moreover, this enhancement of memory performance remains even at follow up assessment (T2). Specifically, there was an improved accuracy at T2 when compared to T0 (F1,12 = 26.56, p = 0.002) whereas there was not significant difference in recognition memory performance between the T1 and T2 time points (F2112 = 0.15, p = 0.70).
No significant difference was found in sham rTMS protocol when comparing T0 to T1 (F1,12 = 0.08, p = 0.77), T0 to T2 (F1,12 = 0.02, p = 0.87), and T1 to T2 (F1,12 = 0.01, p = 0.89).
There was no significant difference between the two groups of AD patients at T0 (F1,12 = 0.33, p = 0.57) whereas the memory performance of the two groups differs following the real rTMS protocol (F1,12 = 4.89, p = 0.04) and after 1 month of treatment cessation (F1,12 = 4.57, p = 0.05) (Fig. 4).

Experiment 2. Memory performance of AD patients at baseline (T0), at the end of two-weeks treatment with right DLPFC rTMS (T1) and at 1 month follow up (T2).
These findings indicate that real rTMS protocol improves the recognition memory in AD patients and this improvement is still significant 4 weeks after the end of stimulation.
DISCUSSION
This study shows that 1Hz rTMS over the right DLPFC may enhance episodic memory performance relative to sham and left DLPFC rTMS in AD patients. Improvement of recognition memory is persistent for at least one month if the rTMS trains are delivered on a daily basis for two consecutive weeks. These findings, together with previous results documenting memory improvements in MCI patients following 1Hz rTMS over the right DLPFC [32, 33], suggest that temporary inhibition of the right DLPFC results in a beneficial effect for episodic memory function in MCI and AD patients.
As to the proposed mechanism of action of TMS underlying these results, the most conservative explanation links the present findings with previous reports of recognition memory improvement following excitatory brain stimulation of the left DLPFC. In fact, considering the transcallosal modulation of brain excitability associated with 1Hz rTMS trains, it is reasonable to make a parallel between findings of memory improvement following either left DLPC excitation or right DLPFC inhibition using brain stimulation.
In addition to this simple explanation, we could provide some additional suggestions about the possible neurophysiological mechanisms at the basis of the positive effect of this procedure.
First, neuroimaging findings reporting that during episodic memory tasks MCI and AD patients show hyperactivations in the DLPFC [36]. These activations have been frequently interpreted as reflecting compensatory mechanisms [37]. Accordingly, additional neural resources located in the DLPFC areas are thought to be recruited to compensate for the hippocampal atrophy typically associated with AD. However, some studies showed that prefrontal hyperactivations are correlated with memory deficits in MCI and AD, suggesting that hyperactivations in the PFC may represent a dysfunctional use of brain resources in AD, rather than reflect compensatory mechanisms. Additionally, Meinzer et al. [38] have suggested that the beneficial effects of brain stimulation among MCI patients in a verbal generation task may be more associated with reductions of aberrant hyperactivity of prefrontal regions.
Another explanation points to deficits in inhibitory neurotransmission in AD, which are associated with neurotoxic effects [39], as well as with disruption of inter-network connectivity [40]. The DLPFC is a critical hub for network integration in memory due to its connections with hippocampus and parahippocampal structures [41]. These connections are pathologically disrupted in AD and in MCI, where an increased parahippocampal-prefrontal FC is predictive of impaired episodic memory [42]. Therefore, inhibitory rTMS targeting the DLPFC may modulate a dysfunctional interaction between DPLFC and the hippocampus, thereby improving the functioning of episodic memory systems, especially during memory retrieval [43, 44]. On the other hand, it cannot be excluded that right rTMS applied before the memory recognition phase could also have modulated cognitive operations occurring in post-encoding phases [45].
The unbalance between excitation and inhibition in the AD brain is also associated with disruption of functional connectivity between DMN and hippocampal structures [40]. Although in the present study we did not directly target DMN structures, it could be possible that inhibiting right DLPFC resulted in down regulation of a fronto-parietal network, with concomitant changes in functional connectivity of anti-correlated networks, such as the DMN [33]. Previous studies have shown these opposite effects on fronto-parietal and DMN networks using tDCS [46, 47]. Indeed, it has been demonstrated that DMN activity, particularly in its posterior components, is necessary for recognition memory retrieval [48], is impaired in AD [49], can be restored in AD patients by excitatory rTMS of the precuneus [27], and is modified in MCI patients by 1Hz rTMS of the right DLPFC [33].
The selective effects on memory encountered following right DLPFC rTMS would argue for a right hemispheric lateralization of DLPFC for memory retrieval [32]. Another point that could explain the selectivity of right DLPFC effects of rTMS is the supposed dominant role of the right DLPFC for inhibitory interactions with subcortical and posterior cortical regions supporting executive control [50].
A recent study [51] reported that 1Hz rTMS trains alleviate neuropathological changes, restore the impairment of hippocampal long-term potentiation and reduce memory deficits in an amyloid-β-induced toxicity rat model. Although our findings and experimental design are profoundly different, these results concur in stressing the importance of deficits of inhibitory neurotransmission in AD and the power of 1Hz rTMS to modulate cognitive functions in this disease.
The results of the second experiment, although on a limited number of patients, suggest that repeated trains of 1Hz rTMS of the right DLPFC can be proficient at improving recognition memory even after 4 weeks follow up and could thus potentially indicate new directions for symptomatic restoring memory in AD.
Future research using larger samples of patients and further focusing on the investigation of the duration of rTMS effects is needed. This would allow deeper evaluation of the extent to which rTMS may represent a promising therapeutic intervention for memory impairments in pathological aging. Related to this issue, since enhanced ability to recall information would have greater impact on daily living than improved recognition memory, future studies using different memory tests with the same 1Hz rTMS paradigm repeated across multiple interventions would also contribute to assess the true clinical significance of these procedures.
Another interesting point deserving further investigation is the link between brain hyperexcitability and neuropsychological deficits across AD clinical stages. Since neuronal hyperexcitability is mainly characterizing preclinical and early stages of AD [52], it is possible that TMS strategies targeting inhibitory mechanisms would be most effective in the early stages of the disease, such as those examined in the present study. On the other hand, the absence of correlations between the rate of memory improvement following TMS and the performance on neuropsychological tests in AD patients does not argue toward a strict dependence of neuromodulation effects on the prodromal AD status.
In conclusion, our findings show that inhibitory rTMS may be a potential effective strategy for treating patients with early AD for whom, currently, there is no available therapy. This evidence agrees with an emerging framework considering circuit-based dysfunctions as a model for cognitive impairment [2] and indicates the DLPFC as a potentially useful target region of intervention to successfully improve memory in AD.
Footnotes
ACKNOWLEDGMENTS
This work received a proportion of funding from the department of Health’s National Institute for Health Biomedical Research Centre funding scheme and from AIRAlzh Onlus-COOP Italia. All financial and material support for this research has no any potential conflicts.