
Abstract
Background:
Both sleep quality and depression could affect cognitive performance in older adults. Previous studies have suggested that there are bi-directional relationships between sleep quality and depression. Possibly, the influence of sleep quality on cognition is partly mediated by depression, and vice versa.
Objective:
We aimed to assess the mediation effects of sleep quality and depression on each other’s relationship with various cognitive functions in non-demented older adults.
Methods:
Correlations were examined among sleep quality indices, depressive severity score, and five cognitive functions in 206 cognitively normal (CN) older adults and all participants that included these CN and 40 mild cognitive impairment (MCI) individuals. We then analyzed the mediation effects for the significant cognitive correlations of sleep disturbance and depression using the bias-corrected Bootstrap method in the two populations.
Results:
Both sleep disturbance and depression were significantly correlated with memory recall and processing speed. In CN, depression could mediate the relationships of sleep disturbance with both cognitive functions, while sleep disturbance could only mediate the relationship of depression with processing speed, but not memory recall. However, in all participants, sleep disturbance could mediate the relationships of depression with both cognitive functions.
Conclusion:
Different mediation effects in the two models in CN older adults might suggest differential mechanisms underlying the pathways from sleep disturbance and depression to various cognitive functions. The mediation results in all participants might indicate that the mechanisms underlying the pathways from sleep disturbance and depression to memory recall were different between MCI and CN older adults.
INTRODUCTION
The relationship between sleep quality and cognitive function has long been of interest to researchers. Studies have shown that sleep quality problems are associated with poor performance in different cognitive functions, including processing speed, episodic memory recall, and executive function in older adults [1–4]. Studies have shown that sleep deprivation could reduce the clearance rate of amyloid-β in the brain, which leads to a higher risk of cognitive impairment [5–8]. Evidence has also indicated a specific relationship between sleep and memory, showing that memory is consolidated in the hippocampus during slow-wave sleep [9].
Depression also affects cognitive performance in older adults [10–12]. Depression has been related to lower performance on memory, executive function, language, and visuospatial function in 2,036 non-demented older adults aged over 65 years [13]. A longitudinal study demonstrated that depressive symptoms at baseline could predict cognitive decline in 1,586 non-demented individuals aged over 50 years [14]. Low levels of motivation and interest, the core symptoms of depression, have been related to slower processing speed [13, 15]. Individuals with depressive disorder have shown the hippocampal atrophy and memory decline [16, 17].
A relationship also exists between sleep quality and depression, and the connection between them might be bi-directional [18–20]. Evidence shows that individuals with chronic insomnia are at a higher risk of developing depression, as chronic insomnia could disrupt the balance of the hypothalamic-pituitary-adrenal axis, leading to depression [21–25]. Alternatively, depressive individuals are prone to having sleep disturbances [26]. A longitudinal study demonstrated that depressive symptoms at baseline would lead to more sleep complaints at a 4-year interval in 4,848 adults aged 50 years or older [27]. The suggested mechanism is that depression could suppress the secretion of melatonin, interfering with the circadian rhythm, and disrupting sleep [28]. It is noteworthy that the occurrences of sleep quality problems and depression did not solely depend on each other, but also many other factors (e.g., symptoms, severity level, personality, and time) [26]. Moreover, their occurrences were not simultaneous, as longitudinal studies have shown that the time lag that the individuals with sleep disturbance developed depression could be over months [24, 25].
Based on these lines of evidence, it was possible that older adults who recently had either sleep quality problems or depressive symptoms developed to have the other condition in a single direction, and their influences on cognitive function might be partly mediated by each other. The mediation analysis is a useful tool to identify the mechanisms underlying the pathway from sleep disturbance and depression to cognitive decline [29]. However, to our knowledge, only a few studies have tapped on the mediation effect that involves sleep, depression, and cognitive function in older adults; and the results were inconsistent. Biddle and colleagues performed step-wise regression analyses, and showed that the inclusion of depression did not change the significant correlations of objective sleep efficiency with reaction time and executive function in 74 older men [30]. A recent study used sleep and depression to predict the occurrence of cognitive impairment (defined by the cut-offs of the Mini-Mental State Examination, MMSE) in community-dwelling older adults aged ≥65 years. The results showed that the difficulty in initiating sleep had a significant mediation effect on the relationship between depression and cognitive impairment in older men [31]. Meanwhile, most studies only controlled for depression and sleep problems as the confounding factors in the analyses of cognitive function in older adults [32–35].
Previous studies have used the approach of two single-directional mediation models to deal with a similar situation, in which there were two risk factors in bi-directional relationships with a sequential order for the same outcome [36, 37]. In the present study, we estimated the relationship coefficients for two possible mediation models, using a Bootstrap procedure. The prevalence of mild cognitive impairment (MCI) in non-demented older adults has been reported around 16.8% [38], and marked sleep quality decline and depressive symptoms have been shown in MCI patients [39, 40]. We performed the mediation analysis in 206 cognitively normal (CN) older adults, and 246 non-demented older adults that included 206 CN and 40 MCI individuals. We had three primary hypotheses: 1) sleep quality and depression both had mediation effects on each other’s relationships with cognitive functions; 2) their mediation effects might vary across different cognitive functions; and 3) possibly, the two mediation models in non-demented older adults were different from those in CN older adults. Furthermore, we investigated whether the combined changes in sleep quality and depression could have a synergistic predictive effect on cognitive performance. Additionally, we explored the influence of MCI on sleep quality indices, and the moderation effects of MCI and gender in the mediation models.
METHODS
Participants
The participants were drawn from an ongoing epidemiological study on the community-dwelling non-demented older adults living in the city of Shenzhen, Guangdong province, starting from November 2015. The exclusion criteria for the epidemiological study were diagnosed dementia based on DSM-IV criteria [41], developmental disability, psychotic symptoms, schizophrenia, bipolar disorder, multiple sclerosis, motor neuron disease, progressive malignancy, or MMSE≤24. From the initially recruited individuals (n = 262), we excluded those who had the following conditions: missing data on neuropsychological data (n = 7), missing data on Pittsburgh Sleep Quality Index (PSQI, n = 4), or education < 5 years (n = 5). Eventually, 246 participants aged 60–83 years (67.05±4.48) were included in the present study.
The present study was approved by the ethics committee of Shenzhen University, and written informed consent was obtained from each participant.
Pittsburgh sleep quality index and geriatric depression scale
The quality of sleep in the last month was evaluated by the 18 self-rated questions of the PSQI (Item 1–9) [42]. The time or duration of sleep was reported in Items 1–4. Items 5–9 that consist of 14 questions were scored from 1 to 4, with a higher score indicating a worse condition. Seven sleep quality indices and a global score can be derived from this questionnaire. The seven indices included sleep duration (hours of sleep at night, Item 4), sleep disturbance (the sum of scores of Item 5b–5j), sleep latency (the time spent in bed before falling into sleep; Item 2 was scored with 1–4 and then added with the score of Item 5a), subjective sleep quality (Item 6), use of sleeping medication (Item 7), daytime dysfunction (sleepiness at daytime and lack of energy at work, the sum of scores of Item 8–9), and habitual sleep efficiency that was calculated as Item 4/(Item 3–Item 1). Each index score was then weighted on a 0–3 scale, and then added together to obtain the global PSQI score. Among these sleep quality indices, sleep disturbance encompasses the problems in sleep architecture (different sleep stages), sleep continuity (initiating and maintaining sleep), and sleep-wake schedule [43]. The severity level of depressive symptoms of all participants was assessed with a 15-item version Geriatric Depression Scale (GDS) [44].
Neuropsychological tests
The performance of all participants on five cognitive domains, namely memory recall, processing speed, executive function, language, and visuospatial function, were evaluated with standardized neuropsychological tests, administered by trained psychology graduates. Memory recall was assessed by the Rey Auditory Verbal Learning Test trial 5 and 6 (AVLT-5, AVLT-6) [45] and Rey-Osterrieth Complex Figure Test recall trial (Rey-O recall) [46]. Processing speed was evaluated by Trail Making Test A (TMTA) [47], the Stroop test - trials A and B (Stroop-A and -B) [48], and Symbol Digit Modalities Test (SDMT) [49]. Executive function was assessed by the Stroop test -Trial C (Stroop-C) and Trail Making Test B (TMTB). Language function was measured by the Category Verbal Fluency Test-Animals (CVFT) and the 30-item version of Boston Naming Test (BNT) [50, 51]. The visuospatial function was measured by Rey-Osterrieth Complex Figure Test copy trial (Rey-O copy) and Clock Drawing Test (CDT) [52].
Diagnostic criteria of MCI
Forty participants were classified as MCI patients, and the remaining were CN individuals (n = 206), based on the international MCI consensus criteria [53]: 1) preservation of independence in functional abilities, which was defined with a cut-off score of 0 on the Chinese version of the Activities of Daily Living Scale (ADL) - 20 items [54] that was developed from the scale by Lawton [55]; 2) report of a decline in cognitive function, either from the participant or their informant; and 3) having cognitive impairment, which was defined by the scores of at least two neuropsychological tests within one cognitive domain were lower than –1.5 standard deviation (SD) of the normative data [56]. This definition of cognitive impairment was also applied to more than one cognitive domain.
Statistical analysis
All statistical analyses were performed using SPSS 21 (IBM Corp., Armonk, USA). Domain scores were calculated by first transforming each component neuropsychological test into a z-score, then forming the average of these z-scores, and finally transforming this average score into a z-score. The raw scores of TMTA, TMTB, Stroop-A, -B, and -C (time to completion) were multiplied by minus one so that higher scores indicated better performance across all measures.
We used the Shapiro-Wilk test to examine the normality of variables and used the Mann-Whitney test for the variables that were not normally distributed to compare the differences in demographics, neuropsychological tests, and GDS between CN and MCI individuals. The difference in gender was compared using the Chi-square test. We used linear regression analysis to examine the predictive effects of MCI status (coded as 0/1, 1 = MCI, 0 = CN) and the interaction term between MCI status and gender (coded as 0/1, 1 = female, 0 = male) on seven sleep indices and the global PSQI score, with MCI, gender, MCI*gender, age, years of education, and body mass index (BMI) category included as the predictors. BMI was calculated as the weight (kg) divided by the square of height (m) and then categorized into underweight (BMI < 18.5), normal (18.5≤BMI < 25), overweight (25≤BMI < 30), and obese (BMI≥30).
To provide a summary of the relationships among sleep indices, depression, and cognitive functions and establish the basis for the following mediation analyses, we then performed partial correlation with five cognitive performance, seven sleep indices, the global PSQI score, and GDS in all participants, CN, and MCI groups. The controlled covariates included age, gender, years of education, BMI category, and MCI status (only for all participants). The significance threshold for the partial correlation of sleep quality index and GDS with each cognitive performance was set at p < 0.01 to correct for the multiple comparisons of five cognitive domains. For other statistical analyses, the significance threshold was set at p < 0.05.
Based on the results of partial correlation analyses (p < 0.01), we specifically examined the mediation effects of sleep disturbance and GDS on each other’s relationships with memory recall and processing speed in CN and all participants. We used the bias-corrected Bootstrap method in the PROCESS Procedure for SPSS, written by Andrew F. Hayes (http://www.afhayes.com) [57, 58]. The Bootstrap samples were set to be 5000, and the 95% confidence intervals (CI) were reported. If zero was not included in the 95% CI, the effect was considered statistically significant [59]. The covariates included age, gender, years of education, BMI category, and MCI status (only for all participants).
We also examined the predictive effects of five interaction terms on cognitive performance in CN and all participants using three linear regression models. Model 1 included the interaction terms of MCI with sleep disturbance and GDS; Model 2 included the interaction terms of gender with sleep disturbance and GDS; Model 3 included the interaction term between sleep disturbance and GDS to examine if their combined changes could be more than their additive effects. The independent and dependent variables for each Model were detailed in the caption of the relevant table. MCI and gender were both coded as 0 (CN and male) and 1 (MCI and female).
RESULTS
Descriptive statistics
The descriptive statistics on the demographics, neuropsychological tests, and GDS for all participants (n = 246), CN older adults (n = 206), and MCI patients (n = 40) were shown in Table 1. Compared with CN, MCI individuals were older (p = 0.03) and had significantly lower performance on the neuropsychological tests in memory, processing speed, executive function, language, and visuospatial function (p < 0.05), but no significant difference in gender ratio, years of education, BMI, and GDS.
Descriptive statistics of demographics, neuropsychological tests and GDS in all participants, CN and MCI groups
GDS, Geriatric Depression Scale; MMSE, Mini-Mental State Examination; Stroop-A/B/C, Stroop test trail A/B/C; AVLT, Auditory Verbal Learning Test; SDMT, Symbol Digit Modalities Test; CVFT, Category Verbal Fluency Test; BNT, Boston Naming Test; BMI, body mass index. *p < 0.05, **p < 0.01, ***p < 0.001. The normality of each variable was examined by the Shapiro-Wilk method. The differences between CN and MCI groups in demographics, cognitive performance and GDS were examined with the Mann-Whitney test. For the comparison of gender, the Chi-square test in Crosstabs was used.
The descriptive statistics of seven sleep indices and the global PSQI score in all participants were shown in Table 2. The interaction item between MCI status and gender had a significant prediction effect on daytime dysfunction (Beta = 0.26, p = 0.02), as this score was lower in female than male in CN group (3.49±1.85 versus 3.68±1.73), while higher in female than male in MCI group (4.04±2.37 versus 2.67±1.40).
Descriptive statistics of sleep quality indices in all participants (N = 246) and the predictive effects of MCI status and its interaction with gender on sleep quality indices
PSQI, Pittsburgh Sleep Quality Index; BMI, body mass index; *p < 0.05, **p < 0.01, ***p < 0.001. ahabitual sleep efficiency and the global PSQI score were calculated in 218 participants (179 in CN and 39 in MCI groups). The descriptive statistics of seven sleep indices and the global PSQI score in all participants were shown. The predictive effects of gender, age, years of education, BMI category, MCI status (MCI/CN = 1/0), and an interaction item between gender (female/male = 1/0) and MCI status on each sleep quality index in all participants were examined in a linear regression model. Also noted, the effect of MCI status shown here was for males only (i.e., when gender was coded zero) and the effect of gender was for CN only (i.e., when MCI status was coded zero), as the interaction term of MCI status and gender was in the model.
Partial correlation
The partial correlation analyses (Table 3) showed that memory recall and processing speed were both significantly negatively correlated with sleep disturbance and GDS in CN and all participants (p < 0.01). GDS was significantly correlated with most sleep quality indices in CN and all participants, except for the use of sleeping medication and habitual sleep efficiency.
Partial correlation of sleep quality, GDS and cognitive domains in all participants, CN and MCI groups
CN, cognitively normal older adults; MCI, mild cognitive impairment; GDS, Geriatric Depression Scale. The partial correlations with sleep quality indices, GDS, and five cognitive domains were examined in all participants, CN, and MCI groups, adjusted for age, gender, years of education, body mass index category, and MCI status (only for all participants). *p < 0.01, **p < 0.001.
Mediation analyses
No multicollinearity problem was found for all predictors in the mediation effect analyses [60]. In CN older adults (Fig. 1), the total effects of both sleep disturbance and GDS on memory recall were significant (sleep disturbance: B = –0.179, p = 0.008, 95% CI [–0.312, –0.047]; GDS: B = –0.208, p = 0.002, 95% CI [–0.340, –0.076]). The mediation effect of GDS on the sleep-memory relationship was significant (B = –0.072, 95% CI [–0.144, –0.008]), while the mediation effect of sleep disturbance on the GDS-memory relationship was not significant (B = –0.048, 95% CI [–0.116, 0.011]). The direct effects of sleep disturbance on memory decreased to non-significant (B = –0.107, p = 0.154, 95% CI [–0.254, 0.040]), while the direct effect of GDS remained significant (B = –0.160, p = 0.034, 95% CI [–0.307, –0.013]).
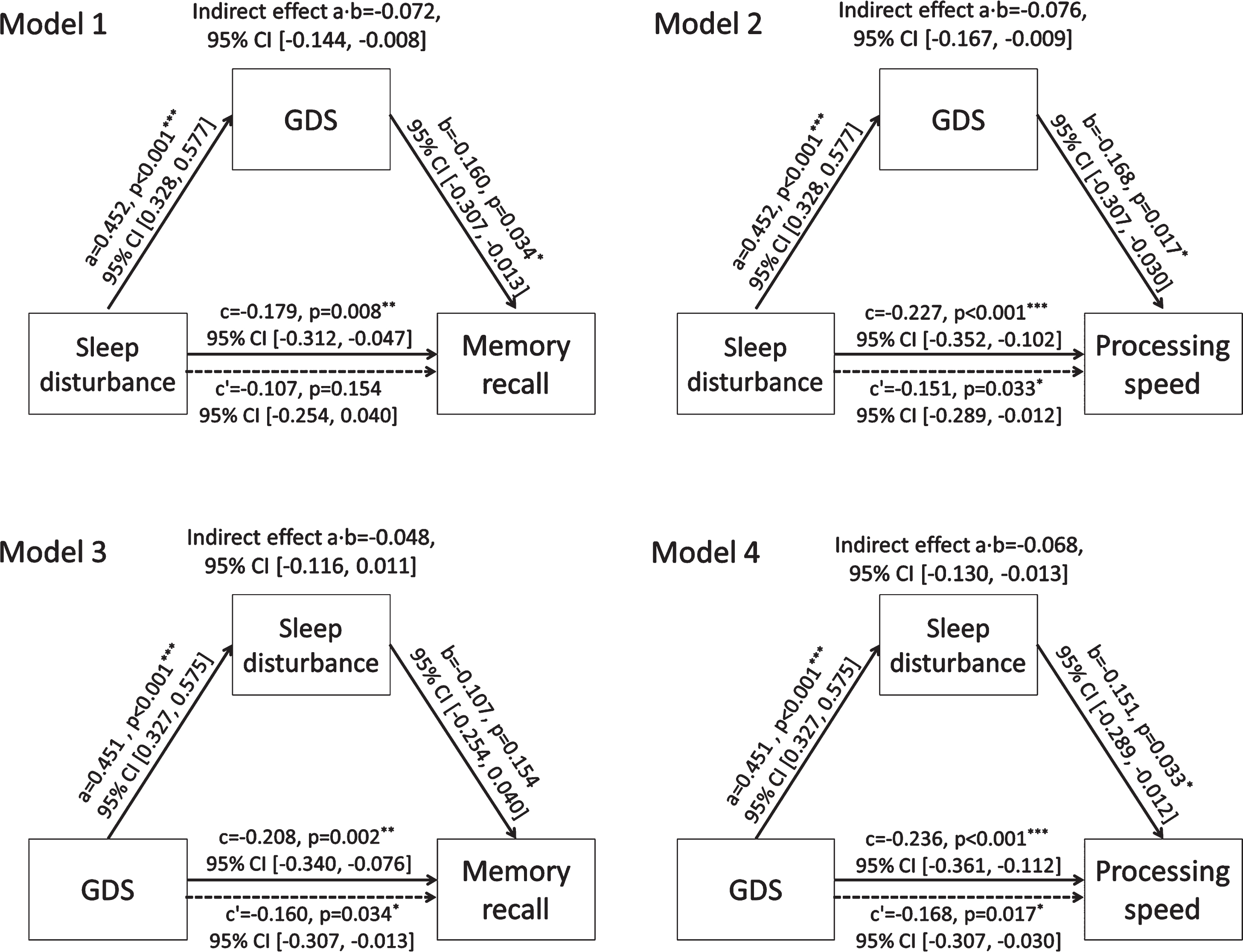
Mediation effects of sleep disturbance and depression on each other’s relationships with memory recall and processing speed in cognitively normal older adults. Four mediation models were used to examine the effects of sleep disturbance and Geriatric Depression Scale (GDS) on memory recall and processing speed in cognitively normal older adults. Path a indicates the relationship from the independent variable to mediator, Path b indicates the relationship from the mediator to outcome with the presence of independent variable, Path c indicates the total relationship from the independent variable to outcome, and Path c’ indicates the direct relationship from the independent variable to outcome. Age, gender, years of education, and BMI category were controlled as the covariates. The presented effect size of each relationship was unstandardized coefficient. The mediation effect was considered to be significant if the 95% confidence interval (CI) did not include zero. Model 1–2): independent variable = sleep disturbance, mediator = GDS, outcome = memory recall or processing speed; Model 3–4): independent variable = GDS, mediator = sleep disturbance, outcome = memory recall or processing speed.
For processing speed, the total effects of sleep disturbance and GDS were both significant (sleep disturbance: B = –0.227, p < 0.001, 95% CI [–0.352, –0.102]; GDS: B = –0.236, p < 0.001, 95% CI [–0.361, –0.112]). Their mediation effects on each other’s cognitive relationship were both significant (GDS: B = –0.076, 95% CI [–0.167, –0.009]; sleep disturbance: B = –0.068, 95% CI [–0.130, –0.013]). Their direct effects remained significant (sleep disturbance: B = –0.151, p = 0.033, 95% CI [–0.289, –0.012]; GDS: B = –0.168, p = 0.017, 95% CI [–0.307, –0.030]).
In all participants (Fig. 2), the total effects of sleep disturbance and GDS on memory were both significant (sleep disturbance: B = –0.190, p = 0.001, 95% CI [–0.306, –0.075]; GDS: B = –0.181, p = 0.002, 95% CI [–0.296, –0.065]). Their mediation effects on each other’s relationship with memory recall were both significant (GDS: B = –0.052, 95% CI [–0.108, –0.002]; sleep disturbance: B = –0.059, 95% CI [–0.115, –0.009]). The direct effects of sleep disturbance on memory remain significant (B = –0.139, p = 0.032, 95% CI [–0.266, –0.012]), while the direct effect of GDS decreased to non-significant (B = –0.122, p = 0.060, 95% CI [–0.249, 0.005]).
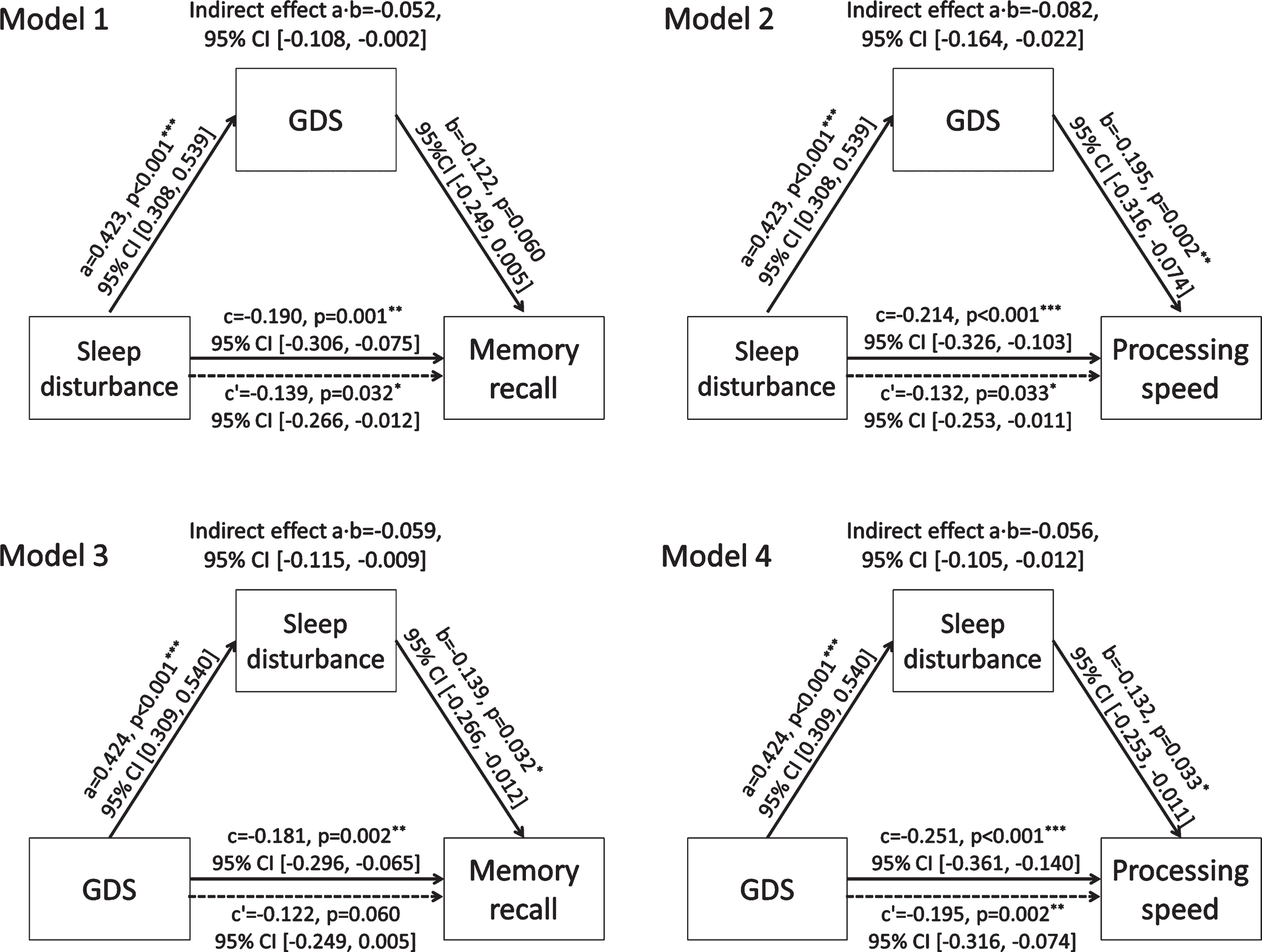
Mediation effects of sleep disturbance and depression on each other’s relationship with memory recall and processing speed in all participants. Four mediation models were used to examine the effects of sleep disturbance and Geriatric Depression Scale (GDS) on memory recall and processing speed in all participants. Path a indicates the relationship from the independent variable to mediator, Path b indicates the relationship from the mediator to outcome with the presence of independent variable, Path c indicates the total relationship from the independent variable to outcome, and Path c’ indicates the direct relationship from the independent variable to outcome. Age, gender, years of education, BMI category, and mild cognitive impairment status were controlled as the covariates. The presented effect size of each relationship was unstandardized coefficient. The mediation effect was considered to be significant if the 95% confidence interval (CI) did not include zero. Model 1–2): independent variable = sleep disturbance, mediator = GDS, outcome = memory recall or processing speed; Model 3–4): independent variable = GDS, mediator = sleep disturbance, outcome = memory recall or processing speed.
For processing speed, the total effects of sleep disturbance and GDS were both significant (sleep disturbance: B = –0.214, p < 0.001, 95% CI [–0.326, –0.103]; GDS: B = –0.251, p < 0.001, 95% CI [–0.361, –0.140]). Their mediation effects on each other’s cognitive relationship were both significant (GDS: B = –0.082, 95% CI [–0.164, –0.022]; sleep disturbance: B = –0.056, 95% CI [–0.105, –0.012]). Their direct effects remained significant (sleep disturbance: B = –0.132, p = 0.033, 95% CI [–0.253, –0.011]; GDS: B = –0.195, p = 0.002, 95% CI [–0.316, –0.074]).
We did not perform the mediation analyses on the language, executive function, and visuospatial function in CN group and all participants, as their relationships with sleep disturbance and GDS did not reach the significance level (p > 0.01).
Interaction terms of MCI status and gender with sleep disturbance and GDS
The predictive effects of five interaction terms of MCI* sleep disturbance, MCI*GDS, gender*sleep disturbance, gender*GDS, and sleep disturbance*GDS on memory recall and processing speed in CN group and all participants were all non-significant (Table 4).
Linear regression to examine the interaction terms in all participants and CN group
*p < 0.05, **p < 0.01, ***p < 0.001. GDS, Geriatric Depression Scale; CN, cognitively normal older adults; BMI, body mass index; B, unstandardized coefficient; Beta = standardized coefficient. The predictive effects of five interaction terms on memory recall and processing speed were examined using three linear regression models in all participants and CN older adults. For each model, MCI and gender were coded as 0 (CN and male) and 1 (MCI and female), and z-standardized sleep disturbance and GDS were used as the predictors and to calculate the interaction terms. In Mode 1, the predictors consisted of MCI, sleep disturbance, GDS, MCI*sleep disturbance, MCI*GDS, age, gender, years of education, and BMI category. In Model 2, the predictors consisted of gender, sleep disturbance, GDS, gender*sleep disturbance, gender*GDS, age, years of education, BMI category, and MCI (only for all participants). In Model 3, the predictors consisted of sleep disturbance, GDS, sleep disturbance *GDS, age, gender, years of education, BMI category, and MCI (only for all participants).
DISCUSSION
Sleep disturbance and depression with memory recall in CN older adults
Our study showed a significant relationship (also referred to as total predictive effect in the Bootstrap method) between sleep disturbance and memory recall in CN older adults. Sleep is generally characterized by sleep architecture and continuity, consisting of different sleep stages, duration, and sequences [61, 62]. Intact sleep architecture benefits memory. In particular, the stage of slow-wave sleep is beneficial for declarative memory, as the synaptic plasticity in the hippocampus is enhanced at this stage [9, 63]. During rapid eye movement sleep, procedural and emotional memory has been consolidated [63, 64]. Our finding was in line with the previous result that poor memory recall was correlated with chronic insomnia in community-dwelling older adults aged over 60 years [65].
Our study also showed a significant total predictive effect of GDS on memory recall in CN older adults, consistent with previous studies [10, 66]. Depression, an affective disorder, manifested with low motivation and disturbed cognitive function, which can disrupt the balance of endocrine function, and influence brain structure and connectivity. The effects of depression on memory appear at several aspects: 1) the influence of low motivation on memory recall by reducing the ability of thinking and concentration; 2) depression as a source of stressor to induce the dendritic atrophy in the hippocampus [67, 68]; 3) the disruption of functional connectivity in default mode network [69], which all contribute to the memory recall decline.
Our study demonstrated a significant mediation effect of depression on the sleep-memory relationship and non-significant mediation effect of sleep on the depression-memory relationship in CN older adults. Evidence showed that sleep loss could disturb emotional regulation by inhibiting top-down control from the prefrontal cortex to the amygdala [70], which then led to memory decline. The remaining non-significant direct effect of sleep disturbance on memory suggested that a large extent of the total sleep-memory relationship might be via the influence of depression. Although depression could disrupt sleep architecture to affect memory recall [71], this mediation effect might account for a relatively small extent of the total depression-memory relationship. The significant influences of depression in memory recall remained at the aspects of motivation, hormonal, and brain structural integrity.
Sleep disturbance and depression with processing speed in CN older adults
Our results on the significant total predictive effect of sleep disturbance on processing speed in CN older adults were consistent with previous studies [2]. Sleep architecture disruption on slow-wave sleep and rapid eye movement sleep has been associated with decreased processing speed [72, 73]. Sleep continuity (consisting of total sleep time, sleep latency, wake after sleep onset, and sleep efficiency) was also correlated with processing speed in older adults aged over 65 years [74]. Sleep deprivation could increase reaction errors and slow reaction times [75, 76]. Moreover, daytime sleepiness has been associated with sustained processing speed decline in non-demented older adults [77].
We also found a significant total predictive effect of depression on processing speed in CN older adults. The severity level of depression was negatively correlated with processing speed in 944 non-demented older adults aged over 60 years [10]. Major depressive disorder patients have exhibited decreased neural activity in the dorsal medial prefrontal cortex and worse performance on processing speed-demanding tasks [78, 79]. Major depressive patients also showed significant gray matter volume decrease in the superior frontal gyrus and lingual gyrus, which contributed to sustained processing speed decline [80].
Both sleep disturbance and depression had significant mediation effects on each other’s relationships with processing speed in CN older adults. As described above, sleep disturbance could impact emotional regulation by disrupting the top-down prefrontal control, slowing down processing speed [70]. However, sleep continuity might not be subject to the mediation of depression, which possibly explained the remaining significant direct effect of sleep on processing speed. Similarly, depression could disrupt sleep architecture, which then affected the performance of processing speed [71]. As depression had a diffuse influence on the brain network of processing speed [78–80], some brain areas might not be affected by the mediation of sleep disturbance. That might be the reason for the remaining significant direct effect of depression on processing speed in CN older adults.
Sleep disturbance and depression with memory recall and processing speed in all participants
The results of mediation analyses on processing speed in all participants were similar to those in CN older adults. However, contrary to the results on memory recall in CN older adults, in all participants, the direct effect of GDS on memory was non-significant, and the direct and mediation effects of sleep disturbance on memory were significant. As the mediation analyses in all participants (n = 246) differed from those in CN (n = 206) in the included 40 MCI patients, the difference in participants might be the reason for the discrepant results. By checking the partial correlation results in CN older adults and MCI patients, we found that the effect size (represented by the correlation coefficient r) of GDS-memory relationship was weaker in MCI than in CN, while the effect size of sleep-memory relationship was stronger in MCI than in CN. The non-significant depression-memory relationship in MCI has been reported previously [40]. One study had even shown a reverse relationship in MCI, with poorer memory correlated with less depressive symptoms. The explanation was that poor memory recall might affect the self-report of depressive symptoms in MCI patients [81]. Meanwhile, the significant relationship between sleep quality and memory in CN older adults was still evident in MCI, as reported in previous studies [39, 82]. These discrepant mediation results in all participants and in CN older adults might suggest a distinct mechanism underlying the relationships of memory with sleep quality and depression between MCI and CN older adults.
Interactions of sleep disturbance and depression with MCI and gender on memory recall and processing speed
None of the five interaction terms showed significant predictive effects on memory recall and processing speed in CN older adults and all participants. The non-significant result for the interaction between sleep disturbance and GDS indicated that their combination might not have a synergistic effect on the two cognitive functions in non-demented older adults. For the two interaction terms of gender, the results suggested that there was no significant gender difference in the cognitive relationships of sleep disturbance and depression. For the interaction terms of MCI, the results indicated that the differences between MCI and CN on the cognitive relationships of sleep disturbance and depression did not reach the statistical significance. However, it might be due to a small sample size of MCI patients.
Daytime dysfunction in female MCI individuals
Our results showed that the interaction between MCI diagnosis and gender had a significant prediction effect on daytime dysfunction. Several epidemiological studies showed that the prevalence of MCI was higher in females (11.6%) than in males (8.0%) in older adults [83–85]. This gender difference has been linked to the protective effect of estrogen. Animal experiments showed that estrogen could assist synapse formation in the hippocampal dendritic spines, improving cerebral blood flow and glucose metabolism, as well as reducing the aggregation of amyloid-β protein [86]. In late life, the estrogen level reduces and fluctuates more in women, while the estrogen level is relatively stable via the metabolism of testosterone in men [87].
Daytime dysfunction is a risk factor of MCI in older adults. Excessive daytime sleepiness has been associated with cognitive decline [88, 89], and MCI patients reported a higher level of daytime dysfunction than healthy controls [90]. Based on the two lines of evidence, we might infer that the combination of female and daytime dysfunction possibly indicated an even higher risk for MCI. That was consistent with our observation, in which the female MCI individuals had a higher daytime sleepiness score than the male MCI (4.04±2.37 versus 2.67±1.40). In contrast, the female healthy older adults were not higher than their male counterparts (3.49±1.85 versus 3.68±1.73).
Limitations
The current findings did not reveal any significant correlation between cognitive performances and sleep quality indices/GDS in MCI patients; hence the analyses on the mediation effects of sleep and depression were not performed in MCI. The null results might be due to a small sample size of the MCI group (n = 40). Although the overall sample size in our study (n = 246) was sufficient, the prevalence of MCI in our study was 16%, consistent with previous epidemiological studies in community-dwelling non-demented older adults [38]. A further investigation with larger sample of MCI individuals would be necessary. Another limitation of this study was due to the cross-sectional design, which restricted our understanding of the causal relationship and temporal sequence between sleep, depression, and cognition. For the older adults who had sleep quality problems or depressive symptoms for a long time, there was a possibility which was a loop or more loops formed between the two conditions. However, the loop models cannot be solved in the present study, as cross-sectional data could not differentiate the bi-directional relationship coefficients between sleep quality and depression [91].
Conclusion
Our results showed significant relationships between sleep disturbance and GDS, and both were significantly correlated with memory recall and processing speed in CN and all participants. In CN older adults, under the model with sleep disturbance as the independent variable and depression as the mediator, we found that sleep disturbance had a direct predictive effect only on processing speed, and depression had significant mediation effects on both cognitive relationships of sleep disturbance; under the model with depression as the independent variable and sleep disturbance as the mediator, we found that depression had direct predictive effects on both cognitive functions, while sleep only had a significant mediation effect on the depression- processing speed relationship. In all participants, the mediation effects of both factors on processing speed were similar to those in CN older adults, while their mediation effects on memory recall were different from those in CN older adults. These findings might suggest differential mechanisms underlying the two possible pathways from sleep disturbance and depression to cognitive functions, and the relationships in the two pathways might also vary between MCI patients and CN older adults.
Footnotes
ACKNOWLEDGMENTS
This study was supported by the National Natural Science Foundation of China (No. 31700960), the Shenzhen-Hong Kong Institute of Brain Science-Shenzhen Fundamental Research Institutions grant (2019SHIBS0003), the Natural Science Foundation of Guangdong Province of China (No. 2017A030310336), the National Key Research and Development Program of China (2018YFC1315201, 2018YFC1315202), and the Shenzhen Science and Technology Research Funding Program (KQTD2015033016104926). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. We would like to thank all elderly people who participated to this study, and we are thankful for our research team for their efforts in this study.