
Abstract
Dementia is an age-related clinical condition, with higher incidence rates in older ages. However, there is some evidence that a reverse epidemiology is also observed. Namely, the cohort analysis of dementia incidence rates by birth in selected populations demonstrated a decreased incidence of dementia in late life across the last twenty years, possibly due to decreased incidence of cardiovascular disorders and increased education and cognitive reserve. In line with that, age is probably a proxy for other pathophysiological processes rather than a strictly causative factor for the onset of dementia, especially in oldest old persons. The present narrative review provides an update on the clinical interplay between the spectrum of brain aging, cardiovascular morbidity, dementia pathologies, and their clinical expression in the oldest old patients. Available evidence suggests that vascular prevention in the perspective of dementia largely involve middle ages, with an apparent reverse epidemiology in oldest old. Similarly, the present findings underline how cognitive resilience and frailty may be key relevant mediators in the modulation of the clinical expression of brain mixed neuropathologies in persons over 85 years old, providing a new integrated conceptual framework.
Keywords
INTRODUCTION
As life expectancy is steadily increasing, old age subjects aged 85 years and more (oldest old), are estimated to be the fastest growing segment of the population in the next decades worldwide. The prevalence of dementia doubles every 4–5 years after the age of 60 years [1], and the estimates of dementia prevalence steeply increase to over 60% in the oldest old [2], foreseeing that the incidence rate of dementia doubles from ages 65 to 90 years [3, 4]. However, the cohort analysis of dementia incidence rates by birth recently demonstrated a decreased incidence of dementia for those American subjects born after versus before July 1929. The decreased trend was associated with a decreased incidence for myocardial infarction and stroke and a notable increase of diabetes. Similarly, Skoog et al. [5] observed a decline in dementia prevalence of 85-year-old subjects that was mainly explained by higher education and lower odds for dementia with stroke in later born birth cohorts. The findings may be also related to an increased cognitive reserve and better treatment of stroke in later-born cohorts.
While the risk of dementia increases with age, dementia is not an inevitable clinical condition associated with chronological aging. Age is probably a proxy for other pathophysiological processes rather than a strictly causative factor for the onset of dementia: this is particularly true after the age of 90 years where a broader variability in prevalence rates for dementia, including a decreased trend, was observed [6].
Alzheimer’s disease (AD) is considered to be the most common cause of dementia in older adults [7, 8]. However, growing evidence indicates that with aging, mixed dementia (MixD) turns out to be the most prevalent subtype, especially in older adults aged 80 years and more, ranging from 20–25% to 35% of all cases of dementia [8]. In line with that and based on the neuropathological standpoint, Corrada et al. reported that autopsies on oldest old patients confirmed the high prevalence of mixed brain neurodegenerative conditions, including MixD, synucleinopathy, TAR DNA-binding protein 43 kDa (TDP-43) accumulation, and astrogliopathy [9].
Moreover, the autopsy experience in the Alzheimer’s Disease Neuroimaging Initiative (ADNI) population confirmed [9] that, whereas the in vivo diagnostic accuracy of AD was very high (97%), mixed pathology in patients converted to dementia and come to death was found in majority of cases. The importance of midlife cardiovascular diseases (CVD) as a preventative way to reduce the incident risk for dementia in later life is well ascertained [10, 11]. Namely, hypertension, diabetes mellitus, angina, myocardial infarct, atrial fibrillation, and cerebrovascular accident confer a substantial increased risk for dementia in later life [12]. In addition, CVD has been reported to play a causative role in the onset of dementia, including AD [13]. Indeed, cardiovascular comorbidity is a frequent clinical condition in the oldest old population and, although the close linkage between dementia and CVD has been extensively investigated [13 –15], there is still a gap of knowledge about how CVD might mediate the risk of dementia across the aging process and how these risk factors relate to each other to build the risk for brain neurodegeneration in the more advanced ages.
Few studies, such as the 90+ Study [3, 9] and the LBC1921 study [16] as well as limited narrative reviews [2 , 17–19] addressed the pathophysiological link between cardiovascular comorbidity and dementia in cohorts of nonagenarians and centenarians. However, this segment of old age population still remains underrepresented in clinical trials, contributing to the poor understanding in this field [20].
Additionally, the rate of progression of frailty, characterized by low physiological reserve to environmental stressors in older adults was significantly associated with the accumulation of brain insults, such as macro-infarcts, and cerebrovascular disease [21, 22], including AD dementia. In line with that, frailty could be potentially considered the real harbinger of dementia, especially in the more advanced ages [23, 24].
Taking this as the current scientific background, the present narrative review provides an update on the clinical interplay between the spectrum of brain aging, cardiovascular morbidity, dementia pathologies, and their clinical expression in the oldest old patients.
A literature search in PubMed, Medline, and the Cochrane databases of all articles published with the medical subject heading keywords “dementia”, “mixed dementia”, “mixed brain pathologies”, “Alzheimer’s disease”, “oldest old”, “cerebrovascular disease”, “cardiovascular factors”, “cardiovascular comorbidity”, “brain aging”, “hippocampal sclerosis”, “cognitive resilience”, and “frailty”. The indicated keywords were matched in all of the potential combinations and all types of clinical studies were included if they enrolled also oldest old patients.
THE SPECTRUM OF BRAIN AGING AND THE THRESHOLD OF THE CLINICAL EXPRESSION OF DEMENTIA IN THE OLDEST OLD: A PATHOPHYSIOLOGICAL INSIGHT
Brain aging and AD neuropathology
Age-related changes in the human brain are characterized by region-specific patterns, such as an age-related linear grey matter volume decrease until the age of 70, with an annual atrophy rate of approximately 2.0%. After the age of 70, longitudinal data indicate an accelerated neurodegeneration, specifically in the hippocampus [25]. Noteworthy, increased volumetric reduction according to aging in prefrontal cortex were also observed, suggesting a highly region dependent atrophy pattern in older adults.
Indeed, there is evidence for a specific brain vulnerability of fronto-striatal regions as the individual ages. It is generally accepted that white matter volume follows an inverted ‘U-shape’ curve peaking in midlife [25]. Namely, a specific vulnerability of prefrontal connections with advancing age and according to an anterior-posterior gradient was reported, pointing to a frontal fiber disconnection [26]. The putative molecular mechanisms underlying brain aging include altered calcium signaling, genomic alterations, reductions of synaptogenesis and neurite outgrowth, demyelination, microglial activation with neuroinflammation, changes to cellular metabolism, mitochondrial dysfunction, and astrocytic hypertrophy with reduced neuronal activity [25].
Similarly, advancing age is associated with functional activation changes within the prefrontal and posterior network. In fact, neurophysiological methods such as electroencephalography or magnetoencephalography, as well as functional imaging techniques as functional magnetic resonance imaging, providing the opportunity to examine neural activation, have indicated a specific age-associated functional vulnerability of prefrontal areas [26].
However, there is high heterogeneity in functional difference with aging, due to multifactorial changes of functional connectivity and to individualized biologically age-related modifications in the brain. This means that the threshold clinical transition from normal to pathological brain aging is far to be understood, especially in the very old ages, remaining unclear to what degree older adults may compensate with brain resilience for such deficits over time.
Brain aging is also associated with brain accumulation of argyrophilic grains, neuromelanin, corpora amylacea, neurofibrillary tangles, extracellular amyloid-β (Aβ), and lipofuscin that promote detrimental effects at multicellular levels, including increased apoptosis, death, and altered functioning of astrocytes, microglia, neurons, and oligodendrocytes.
It is noteworthy that, in oldest old subjects, a consistent amount of the neuropathological hallmarks of AD (Aβ and tau protein deposits) has been observed, although this brain intracellular and extracellular accumulation was unrelated to the clinical manifestation of dementia [27 –29].
It could be hypothesized that AD neuropathology can simply reflect the acceleration of the molecular scaffold of brain aging. So far, different gradients of structural decline have been observed, with substantial qualitative and quantitative differences that may count for substantial neurocognitive dissociations between brain physiological aging and brain neuropathology [28]. Indeed, quantitative differences seem to relate to the extent and progression of changes while qualitative changes (e.g., brain volume, white matter integrity, cerebral activation, functional connectivity, and neurotransmission) and may reflect the true distinguishing line for brain neurodegeneration [28].
In line with that, the Consortium to Establish a Registry for Alzheimer’s Disease [CERAD] system showed that the prevalence of neurodegenerative diseases increases with age [3], although a decreased incident rate for dementia in subjects older than 90 years was also observed. Notably, 25% –50% of oldest old’s brain autopsies displayed a lower rate of AD hallmarks, with a substantial reduction of brain neuritic amyloid plaque density [27].
Similarly, recent neuropathological findings from the Georgia centenarian study pointed out that AD-type pathology was associated with poor cognition, although it was not the only variable counting for dementia in the very old ages [29]. In particular, the pathophysiology on centenarians’ brains included hippocampal sclerosis, TDP-43 accumulation, and cerebral atrophy [29], indicating the wide range of AD-type neuropathological heterogeneity observed in non-demented very old subjects [30, 31]. Sharing this neuropathological background in the oldest old, further investigation is warranted to better understand the strength of association between AD-type pathology and cognition in older ages and their different clinical trajectories compared to younger old adults [29 , 33].
From a neuropsychological standpoint, attentional and executive dysfunctions, including cognitive flexibility, reasoning, focused and divided attention, processing speed [34], short-term/episodic memory and working memory dysfunction are reported in very old subjects (Table 1). Although there is a linear decrease of age-related cognitive alterations, very old individuals display a higher heterogeneity in cognitive dysfunctions, with even a sharper decline, suggesting that the interplay among neural activation, functional connectivity, and structural brain changes could draw highly individualized clinical trajectories [35, 36].
The spectrum of brain aging, its clinical entities with related neuroanatomic and neurophysiological main findings
So far, the dissociation between normal brain aging and dementia need further investigation to be based upon the identification of a specific clinical profile.
Hippocampal sclerosis of aging
Hippocampal sclerosis-aging (HS) has been identified as the major substrate of the amnestic syndrome in a significant proportion of cognitively impaired oldest-old patients [37, 38]. Recent autopsy neuropathology insights have contributed to build a new integrated conceptual framework for HS, on the basis of the aging process. HS is a common neuropathological finding, characterized by cell loss, gliosis, and atrophy in the bilateral hippocampal formation [39]. It is noteworthy that this common clinical condition in the oldest old subjects is out of proportion to AD neuropathological features in the same structures. HS pathology is a true disease of older age and may occur independently of AD pathology, although it is generally misdiagnosed as AD with a linear age-related increase. This means that each added life is associated with an increased risk for HS neuropathology at autopsy [40]. Further, surviving each additional year above 90 is more associated with the risk of HS disease than with the risk for developing AD pathology. Indeed, HS is observed in over 20% of individual autopsies over age 85 and, from a clinical standpoint, HS is known to cause a significant cognitive impairment that may rival AD cognitive deficits [41].
So far, there is a limited understanding of HS and the lack of animal models for clinical biomarkers contribute to this poor knowledge. Some prior findings suggest that arteriosclerosis of multiple brain regions is associated with HS [42] and a series of neurodegenerative molecular features were also observed, including abnormal proteostasis with protein misfolding, supporting the hypothesis of a synergistic mixed model for HS of aging [39].
Recently, a unique brain neuropathological profile has been identified, including a series of genetic risk factors, extrahippocampal TAR DNA-binding protein 43 kDa (TDP-43) pathology, and brain arteriolosclerosis. These neuropathological findings and, in particular, the frequently associated ABCC genetic variant and the vascular insults mediated induction of TDP-43 phosphorylation and misfolding, prompted the clinical reconsideration of HS, with its updated nosology to cerebral age-related TDP-43 with sclerosis (CARTS) [37]. It could be hypothesized that age-related chronic vascular dysfunction might lead to different TDP phenotypes, such as HS, that may represent the high magnitude of neglected causes of dementia in the oldest old.
From a neuropsychological standpoint, HS is characterized by less pronounced cognitive impairment with disproportionate episodic impairment, with relatively high verbal fluency but low wordlist recall, that seems to be the distinguished features of HS [44]. In turn, HS seems to display mild clinical decline over time, making difficult the diagnostic understanding of border zones between the aging brain, the wide spectrum of HS-associated cognitive deficit and non-AD pathology. It could be hypothesized that HS might co-occur with minimal AD pathology, counting for the perceived disassociation between cognitive status and AD in the oldest old (Table 1).
However, the physician perception is far from being accurate in the identification of HS in more advanced ages, even far behind that of pathologists [45]. Thus, new investigations are warranted to better sharpen our ability to discriminate between HS and AD, especially in the diagnosis of dementia subtypes in the very old ages [44].
Cognitive resilience
Growing evidence indicates that the individual cognitive resilience may represent the mediator of brain neuropathological burden, modulating the progression rate to late life dementia. Based on dementia research, cognitive resilience has been described also as “cognitive reserve” and “aging well” [46]. However, these terms represent overarching concepts that explain why some older adults maintain intact cognitive abilities despite brain aging or AD-like brain neuropathologies [47] and in a narrow sense, cognitive resilience refers to overcoming substantial development of brain hallmarks for AD that would normally result in dementia [47].
So far, there is a little understanding about how some older adults may build cognitive resilience throughout their life span. The definition of cognitive resilience relies on the presence of educational/occupational attainment, premorbid intelligence quotient, leisure, cognitive and mental stimulating activities [48].
Recently, Bowles et al. [49] compared mid-life characteristics from autopsies cases with intermediate and high levels of AD pathology. Notably, the odds of being resilient were associated with higher college education, less than two brain microinfarcts, lack of hippocampal sclerosis, and an average higher brain weight at death. Interestingly, no differences in atherosclerosis or arteriolosclerosis burden were reported between the groups. It could be conceiving that a component of continuous learning could mitigate the impact of brain neuropathology on cognitive performance over time, with a potential increased threshold for the development of late life dementia (Table 1).
In contrast, the LIBRA index for brain health was recently developed to assess the individual’s prevention potential for dementia. The LIBRA index is based on modifiable risk factors such as diabetes, depression, physical activity, hypertension, hypercholesterolemia, coronary heart disease and mild to moderate alcohol use that may be considered a proxy of cognitive resilience.
Interestingly, the risk for dementia increased with higher LIBRA scores in mid-life whereas this same index was unable to prognosticate the development of dementia in the oldest old [50].
However, the current operational definition of resilience showed its limitations, since it does not accurately reflect the multiple levels of cognitive resilience throughout aging. In addition, the lack of any systematic definition of cognitive resilience, its measurement and its longitudinal assessment may affect the study results comparability. Moreover, other data suggest that the socioeconomic status may explain the association between lifestyle conditions, as measured with LIBRA index, and dementia risk, representing a novel proxy of functional reserve [51].
In addition, comorbidity and vascular burden, especially in later life, could have an additional impact on resilience and, similarly, the inclusion of neuritic plaques (CERAD consortium) and BRAAK staging, as reference hallmarks for AD pathology, may have underscored the huge spectrum of mixed dementia pathology in the oldest old [52]. In line with these assumptions, cognitive resilience may have similarities with the geriatric concept of “intrinsic capacity” that refers to the preservation of individual physical and mental capacities throughout the aging process [53]. In line with that, two main mechanisms could be taken into account for the understanding of brain resilience/intrinsic capacity in the very old ages. The first putative mechanism relies on the number of synapses and brain volume that should build brain resilience to AD pathology with neuronal plasticity over time. An alternative hypothesis includes the ability to recruit alternative brain networks with brain compensation that could allow the maintenance of appropriate cognitive performance despite repeated vascular and neurodegenerative insults [54]. The brain network of compensation, mainly focused on the right dorsolateral prefrontal cortex (DLFC) showed wide metabolic correlations with specific cortical areas in both hemispheres (e.g., frontotemporal cortex, parahippocampal gyrus, and precuneus) in highly educated prodromal AD patients, as compared with poorly educated prodromal AD ones. The metabolic connectivity analysis of the DLFC showed an increased neural reserve in higher educated prodromal AD patients with the recruitment of compensatory neural networks that may count for this buffering effect, providing new evidence in the field of neural reserve and physiologic networks of subjects with higher education [54].
According to this assumption, the EMIF-AD 90+ Study [55] is currently aimed at better discriminating the boundaries between brain resilience and cognitive impairment in the oldest-old, with the measurement of a wide range of potential protective vascular factors, including hallmarks of aging, markers of neurodegeneration, social networks, and psychical activity that ultimately could contribute to brain resilience on a multifactorial basis.
Table 1 illustrated the over mentioned clinical entities on the basis of the main neuroanatomic and neuropsychological findings.
FROM THE BRAIN-HEART AXIS TO DEMENTIA IN THE OLDEST OLD
The Danish Centenarian Study reported that almost 50% of cases of dementia in centenarians were associated with cerebrovascular causes [55] with a broad spectrum of clinical entities, ranging from large cerebral infarcts due to large vessel disease (e.g., multi-infarct encephalopathy) to cortical microinfarcts, subcortical lacunas, microhemorrhages, and white matter lesions with cerebral small vessel disease. However, the authors concluded that cerebrovascular diseases are equally common in centenarians with and without dementia.
Similarly, the 90+ Study demonstrated that, in very old ages, vascular brain pathology was characterized by predominant small vessels disease with smaller lacunar and micro infarcts, that seem to be the key relevant mediators of both cognitive deficits and dementia [8]. While mixed pathology seems typical of very old ages [56], the relative weight of cerebrovascular lesions on cognitive impairment seem lower in the oldest old in comparison with earlier ages [57].
Namely, cerebral amyloid angiopathy has been shown to contribute to dementia in late life, being independently associated with an increase in the odds of AD clinical diagnosis [58]. The clinical expression of moderate-to severe cerebral amyloid angiopathy is characterized by lower cognitive performance processing and perceptual speed ability disproportionate to AD neuropsychological findings. However, the underlying potential mechanisms, including brain microbleeds, microinfarcts, white matter hypoxia, and neurobiological correlates, such as neuroinflammation and oxidative stress, are still partially understood, so far [59].
Giannakopoulos and colleagues found that neuritic plaques, neurofibrillary tangles, cortical microinfarcts, and subcortical lacunas are prevalent neuropathologic features of the aging brain that could also drive the neurodegenerative trajectories in the more advanced ages, with a synergistic effect [60].
Similarly, the MRC CFAS study contributed to substantiate the notion that a higher brain vascular burden could be a correlate of late-onset dementia, since multiple vascular lesions were more frequently found in older subjects with dementia than in those without dementia. However, concurrent cerebrovascular disease is a common finding in old age subjects with dementia, that was suggested to lower the threshold for mixed dementias such as AD and alpha synucleopathies, addressing the need for appropriate targeted treatments for cerebrovascular diseases [61, 62]. In line with these notions, cardiovascular comorbidity could represent a key relevant mediator for the development of dementia in the oldest old. Indeed, with aging, coronary and systemic vascular flow reserve declines, in parallel with increased brain atrophy and neuronal loss. These anatomo-functional underpinnings may ultimately induce cerebral hypoperfusion with the energy crisis of the neurovascular unit, accelerating neurodegenerative pathways [63] due to chronic cerebral hypoperfusion and increased risk of embolic stroke.
In addition, de la Torre et al. observed that the maintenance of adequate brain perfusion was of key relevance for the prevention of dementia in very old ages [64]. On the basis of this theoretical model, seven cardiovascular hemodynamics factors were suggested to play a role in the connection between the aging brain and cardiovascular comorbidity, supporting the heart-brain hypothesis [65] and/or heart brain axis [66]. Namely, lungs, heart, the large elastic vessels (aorta), baroreflex, cerebrovascular arteries (carotid, middle cerebral, and vertebral arteries), the small cerebral vessels (contributing to 50% of the overall cerebral resistance of the healthy brain) and the cerebrospinal venous system were suggested to contribute to late life cognitive disorders, including dementia, by virtue of epigenetic damage of DNA, systemic inflammation with reduced nitric oxide production, altered endothelial function and overall reduced brain blood flow [67].
CLUSTERS OF CARDIOVASCULAR COMORBIDITY AND DEMENTIA IN THE OLDEST OLD
Cardiovascular comorbidity in older adults includes hypertension, atrial fibrillation (AF), heart failure (HF), that are known to induce alterations of cardiac output, blood pressure, pulse wave velocity, aortic and carotid stiffness, causing a reduced cerebral blood flow (CBF). In very old age patients, these chronic hemodynamic alterations could critically attain the threshold of cerebral hypoperfusion, potentially accelerating the cognitive trajectories [67]. However, the specific contribution of each cardiovascular comorbidity in the development of dementia in the oldest old is still largely unexplored.
Blood pressure
Hypertension represents a common clinical condition in older adults, with a linear age-related steep increase in the oldest old; three main biological mechanisms such as neuroinflammation, oxidative stress, and vascular dysfunction (Vascular Health Triad), have been, so far, implicated in the aging process and the development of both hypertension [68] and dementia [69].
It is noteworthy that mid-life hypertension is an independent predictor of late life dementia. In line with that, the 20-year observational period of cumulative cardiovascular risk in midlife was significantly associated with lower CBF in later life, outlining that midlife vascular risk profiles rather than later-life vascular risk profiles showed the strongest association with cerebral blood flow in older age [70 –72].
In contrast, receiving a diagnosis of hypertension after the age of 80 years was observed to be a protective factor for the development of dementia in very advanced ages [73].
Similarly, the Rotterdam study, Gothenburg H-70 study [74], and Adult Changes in Thought study [75], respectively, supported the inverse correlation between increased systolic blood pressure and dementia in old age subjects over 80 years [76]. Moreover, the Kungsholmen Project demonstrated that a lower diastolic blood pressure was significantly associated with the risk of dementia in the very old patients [77]. Similarly, Qiu et al. showed that lower diastolic pressure was associated with the development of dementia, due to the presence of severe atherosclerosis and arteriosclerosis, especially in the oldest old subjects [78]. In line with these notions, it could be hypothesized that lower systolic blood pressure values may further impair CBF autoregulation, resulting in brain diffuse ischemia, that ultimately accelerate the clinical expression of dementia.
Although several large clinical trials suggested that the use of anti-hypertensive medications in mid-life may reduce the risk of cardiovascular events, mortality and late-onset dementia, antihypertensive medications in the oldest old have not yet been consistently associated with reduced incident dementia (SCOPE) [79]. Similarly, the Hypertension in the Very Elderly Trial cognitive function assessment (HYVET-COG) study showed that antihypertensive treatments in individuals >80 years old did not reduce the development of dementia, although a further metanalysis demonstrated a possible protective effect with ambiguous evidence [80].
Given the uncertainty regarding the optimal blood pressure levels in the oldest old to preserve cognitive function, it is also important to clarify the role of blood pressure variability on cognitive outcomes. It has been suggested that wide fluctuations in the individual blood pressure hold a worse prognostic value on dementia outcomes, although the magnitude of this association and pathogenetic mechanism are largely unknown in the very old patients [81, 82].
Notwithstanding that, it is generally accepted that in older and frailer subjects, increased blood pressure seems to play a physiological compensatory mechanism for the maintenance of both adequate cerebral perfusion and cognitive performance. So far, this is an important and still debated issue [83, 84]. In contrast, in the SPRINT MIND study [85], that included subjects with high vascular risk and excluded frailest subjects, treating blood pressure intensively reduced the risk of cognitive impairment and the combined rate of conversion from mild cognitive impairment to dementia, while it did not result in a significant reduction in the overall risk of developing late life dementia.
In line with these notions, the ADNI study observed that CBF impairment was the earliest and strongest predictor of AD progression when considering a wide range of AD markers, including brain atrophy, functional connectivity, Aβ deposition, plasma and cerebrospinal fluid markers [86]. In particular, the cerebrovascular dysregulation triggered by systemic hypotension may even precede and accelerate neurodegeneration, indicating CBF as a promising imaging biomarker for preventative interventions, especially in old age subjects [87].
Table 2 illustrated the most relevant associations between blood pressure levels the risk of dementia in older age subjects.
Association between blood pressure levels and risk of dementia in the oldest old
SPB, systolic blood pressure; BP, blood pressure; CBF, cerebral blood flow; MRI, magnetic resonance imaging; DPB, diastolic blood pressure; MAP, mean arterial pressure; PP, pulse pressure; MMSE, Mini-Mental State Examination; ADL, Activities of Daily Living; IADL, Instrumental Activities of Daily Living; AD, Alzheimer’s disease.
Atrial fibrillation
AF is an emerging epidemic in the older population and it has been growingly associated with the development of clinical or silent cardioembolic stroke and with increased risk of vascular dementia [88]. Based on a pathophysiological standpoint, both dementia and AF share many common risk factors and preventative lifestyles habits. It could be hypothesized that dementia association with AF is a large spectrum of repetitive cerebral injuries that might result in both macroembolia and microbleeds. Notably, as the brain ages, microbleeds have been also correlated with hippocampal atrophy that, in presence of silent brain infarcts, micro-thromboembolism, bleeding, brain hypoperfusion, and increased systemic inflammatory state may also account for the development of AD dementia, although with limited evidence, so far [89].
In addition, in older age subjects with AD at autopsy, a high prevalence of cerebral microvascular injuries is observed, that may be associated with microembolism and/or hypoperfusion associated with AF [90]. The Rotterdam Study addressed, cross-sectionally, the association between AF and dementia, with a > 2-fold increased risk both in presence and absence of stroke [91]. Since then, a series of prospective studies supported this causal association [92], although a paucity of studies investigated the relation between AF and dementia in ≥80 years old subjects.
Bunch and colleagues supported the notion that AF was independently associated with all forms of dementia, although the highest risk of AD was in patients younger than 70 years [89].
In contrast, the Atherosclerosis Risk in Communities Neurocognitive (ARIC-NCS) study [3] which followed a large cohort of patients for over 20 years, showed that incident AF was associated with a 23% higher risk of dementia, even after adjustments for cardio- and cerebrovascular risk factors or incident ischemic stroke, both in those under and over the age of 57 years. So, there might be a time dependent association between these two clinical entities, as AF needs to develop at a younger age to contribute to the onset of dementia at a later stage, emphasizing the importance of diagnosing and treating AF to prevent dementia in older age.
In fact, subjects with AF are likely to reach the thresholds of dementia at earlier ages than individuals with no history of AF and interestingly, even the age of onset of incident AF may play a key role in modifying the individual cognitive trajectories, leading to a more rapid decline progressively at ages 70, 75, 80, and 85 years, respectively [94].
Recently, Saglietto and co-workers demonstrated that AF confers a nearly 30% increased risk for dementia, independently of cerebrovascular accidents [95].
Yet, in the Kungsholmen Project (1987–2000), Marengoni et al. explored the association of chronic AF with stroke, dementia, and AD in a longitudinal (6-year follow-up) assessment in very old patients and, notably, a significant association between AF and stroke, as first ever event, was observed. However, neither dementia nor AD were associated with AF either in the whole cohort or any stratified subgroup identified by sociodemographic, use of antithrombotic treatments and APOE genotype [96]. Similarly, the Vantaa 85+ study, a longitudinal population-based study of subjects aged 85 and older, observed that AF was associated with increased incidence of stroke in very old individuals but not with dementia in a similar fashion to all other traditional cardiovascular risk factors [97]. Moreover, in the HYVET-COG, AF did not demonstrate a significant relationship with the development of dementia in hypertensive adults, aged 80 and over [88]. Conversely, in the Helsinki Aging Study, the presence of AF significantly preceded a worsening in Mini-Mental State Examination (MMSE) scores at 5 years follow up, but after 10-year follow-up changes in MMSE score were no longer associated to history of vascular conditions such as hypertension, myocardial infarction, AF, and stroke [98].
So far, an association between AF and dementia has been mainly observed in observational studies, although the magnitude of this association weakens in the oldest old as a result of the aging process, the coexistence of cardiovascular risk factors, multimorbidity, and metabolic alterations that could predispose to AF, adding clinical complexity to the understanding of late life dementia [99 –102]. Namely, the metanalysis of Santangeli et al. concluded that AF independently increases the risk of incident dementia in elders without acute stroke and normal baseline cognitive function [103].
Table 3 illustrated the key relevant associations between AF and dementia in the oldest old.
Association between atrial fibrillation and dementia in the oldest old
AF, atrial fibrillation; AD, Alzheimer’s disease; MMSE, Mini-Mental State Examination.
HF heart failure
Chronic HF is a major public health problem, affecting especially older adults as a consequence of aging. In addition, about 60% of patients with HF have at least three comorbidities, including cognitive dysfunction and/or dementia. Some evidence sought to characterize the pathophysiological HF related processes that are predominantly associated with dementia, indicating that inadequate cerebral perfusion, chronic hypoxia damage, altered cerebrovascular reactivity, arterial hypotension, and production of pro-inflammatory cytokines are of key relevance for the neurodegenerative changes [104 –107].
Qiu et al. demonstrated an association between HF and AD dementia in old age subjects and it was observed that low diastolic pressure additively contributed to the increased risk for AD [108].
The Framingham Offspring Study demonstrated that, in a cohort of participant free of clinical stroke, dementia and transient ischemic attacks (with a mean age 69 years), a decreased myocardial function (reduced cardiac index) was an independent predictor of the development of dementia, including AD, over a mean observation of 7 years [109]. The lower cardiac index was associated with smaller brain volume and increased white matter hyperintensities.
Additionally, HF increases the risk of emboli and microvascular pathology, such as white matter lesions and lacunae, which are, in turn, related to an increased risk of overall dementia [110 –112]. Moreover, it was also observed that in patients with NYHA class III/IV HF, CBF was substantially, but reversibly, reduced, suggesting that the impaired redistribution of cardiac output inadequately maintained CBF in patients with severe chronic HF. Heart transplanting was observed to improve CBF and cognitive performance although only in very young patients [112, 113]. In line with these findings, patients with advanced HF run a greater risk of developing dementia and cardiac structural changes, such as higher levels of left ventricular hypertrophy which were observed to be associated with increased cognitive decline in older subjects (mean age 75 years old) independent of cardiovascular risk factors, comorbidities, and medications [114].
Based on a pathophysiological standpoint, little is known on the molecular mechanisms underpinning dementia and HF in older adults. Advancing age, neuroinflammation, oxidative stress, mitochondrial dysfunction, and brain hypoperfusion are, so far, the main molecular scaffolds that participate in neurocognitive disorders associated with HF, including the expression of AD related markers (BACE1 and Aβ deposition) in the hippocampus [115, 116].
However, the great majority of studies has been performed in young old age subjects (mean age 70 years), predominantly in male subjects with systolic dysfunction [117]. Few studies included both diastolic and systolic dysfunctions [118], and it is plausible to hypothesize that different structural cardiac dysfunctions may count for different types of neurocognitive disorders. This is especially true for the oldest old subjects, who have a high prevalence of diastolic dysfunction, further limiting the generalizability of the observed associations. Considerable evidence confirmed the multifactorial origin of dementia in HF but, so far, the identification of a risk profile for the development of dementia in the oldest old is still missing. In line with these assumptions, it could be speculated that interventions targeting cardiovascular risk factors and pertaining to blood pressure, HF, and AF might be more important for the younger-old in decreasing the risk of late life dementia. Conversely, vascular dysfunction including blood-brain barrier integrity, brain microbleeds, and CBF seems to be the major risk factor for late onset dementia, lowering the threshold for dementia for a given AD or mixed brain pathology [119 –121].
Arterial stiffness
Arterial stiffness (AS), measured as pulse wave velocity, has been associated with evidence of cerebral small vessel disease and fibrillar Aβ deposition in the brain. Greater AS is also associated with the extent of white matter disease and Aβ accumulation over time in older adults without dementia, irrespective of blood pressure. AS may be the underlying mechanism linking both hypertension and dementia and, notably, AS of the central and carotid segments correlated with the burden of multiple types of dementia pathologies. Higher AS corresponds to increased pulse wave velocity from the heart to the brain and it is directly associated with increased Aβ burden. In addition, AS seems to be associated with the overlap of dementia pathologies, that includes white matter disease, cerebral microbleeds, Aβ deposition, and lower brain volume [122].
It is noteworthy that pulse wave velocity is associated with Aβ deposition in the brains of very elderly adults and the associations among central AS and mixed brain pathologies have been documented in individuals aged more than 80 years compared to the younger cohort of 70 older adults [123].
So far, it is known that hypertension contribute to the progression of AS, accelerating its progression as the patient ages [124]. The current body of evidence seems to relate AS to multiple aspects of dementia pathologies in later late and may serve as a key relevant mediator linking aging, cardiovascular risk factors and dementia [125].
It is noteworthy that the ARIC-NCS study found a cross-sectional association of central AS and pressure pulsatility with mild cognitive impairment and dementia [126]. Longitudinal studies have observed an association between vascular stiffness and cognitive decline, both in population-based samples [127] and in the oldest old [128].
In line with that, future longitudinal studies in very old subjects are needed to unravel the pathogenetic changes in arterial stiffness, brain structural abnormalities, brain aging, and conversion to dementia [129].
Hypercholesterolemia
Longitudinal studies have shown a strong association between mid-life high total cholesterol and AD [129, 130] and, furthermore, AD patients were observed to have lower HDL levels and higher LDL levels than matched controls [131 –133]. Moreover, previous observations reported that the intake of lipid lowering medications was associated with reduced brain neurodegenerative pathology, resulting in decreased amyloid deposition [134]. The link between AD and cholesterol has also been supported by the identification of clusters of genes (e.g., apolipoprotein E4, ABCA 7, and single- nucleotide polymorphisms for clusterin) that affect lipid brain metabolism [135]. However, the relationship between cholesterol and dementia at the population level is unclear since it may vary over the lifespan. In particular, in late life, no association was found between hypercholesterolemia and dementia and, in contrast, low cholesterol levels have been observed to be predictive of dementia [136, 137].
In addition, changes in cholesterol levels between visits were predictive of dementia, being the quartile of greatest decrease in cholesterol related to increased risk of overall dementia, with a similar trend for AD. Indeed, in an elderly cohort followed for 32 years, a decreased level of cholesterol was modestly associated with the risk of dementia in later life [137]. In line with this notion, the cholesterol-dementia relationship needs to be observed continuously over the middle to late lifespans as well as not only among those who survived to old age, representing a survival bias/competing mortality.
Notably, the unintended decrease of cholesterol (e.g., not via medications or cholesterol-lowering diet) as the individual ages, may be more indicative of dementia risk, suggesting that, the observed decline may be associated with regions affected by amyloid deposition, such as hypothalamus, responsible for homeostatic regulation.
A recent metanalysis [138] consolidate this evidence and showed that in late life, total cholesterol was not associated with dementia, although some isolated studies found a biological plausibility between late life lipids and brain health. Notwithstanding that, it is noteworthy that all the late life studies were commenced when many patients accumulated significant AD pathology. It could then be hypothesized that without understanding the true cholesterol trajectory over time, it is unfeasible to draw solid and scientific sound conclusions. Moreover, patients with high LDL/non-HDL cholesterol profile were significantly lost at follow-up due to other comorbidities, entangling the whole issue.
In line with these results, participants with studies that modelled trajectories in older age subgroups are warranted to interpret the whole life course perspective on the current findings in this field. The decline in metabolic parameters such as blood cholesterol levels, body mass index, blood pressure seems to be a significant mediator of higher risk for dementia according to aging.
Diabetes mellitus
Type 2 diabetes (T2D), its longer duration and poor glycemic control have been growingly associated with worsening cognitive performance, including the development of dementia, vascular dementia, and AD. In the ARIC study (Atherosclerosis Risk in Communities) by Rawlingl and colleagues, higher HbA1c values were associated with incident dementia but, similarly, lower levels (HbA1c 5.8%, 40 mmol/mol) were also associated with an higher risk of incident dementia [139]. Moreover, in older patients with T2D, a clinical history of sever hypoglycemic episodes was associated with a greater risk for dementia. Overall, 10% of older diabetic patients develop AD in later life, supporting the metabolic interplay between glucose dysfunction and AD brains (“type-3 diabetes”) [140].
Epidemiological studies indicate a strong connection between AD and T2D, since they both share a series of vascular risk factors such as vascular lesions, hyperglycemia, hyperinsulinemia, atherosclerosis, and hypertension. Similarly, two main molecular mechanisms are considered the main molecular scaffold for this association, and namely, the insulin resistance and leptin resistance [140]. Insulin resistance may mediate lower glucose cerebral uptake and insulin receptor and insulin like growth factor 1–2 receptors in brain might form heterodimers, modulating intracellular insulin pathways. In addition, recent insights have shed new light on the association between IGF-1 receptor stimulating activity and increased dementia incidence in hetero- and homozygotes of the ApoE ɛ4 allele [141].
Similarly, leptin resistance is associated to impaired blood barrier transport with defective brain molecular pathways (AMPK increase activity). Although the role of leptin in the development of T2D-related dementia is speculative, it is noteworthy that in a 9-years follow-up of older adults, the higher the leptin levels were, the lower the risk of developing dementia, including AD [142].
Although it is widely known that insulin resistance (IR) is a precursor of T2D and two longitudinal studies found that midlife IR was associated with a slightly increased risk of AD, Lee et al. recently observed an inverse correlation between IR and AD incidence in late life [143 –145]. According to this hypothesis, late life IR may be considered as a short-term state of hyperinsulinemia that could provide a short-term positive effect on memory and brain function, especially in very old age subjects. This notion is in line with the findings that late life higher levels of blood pressure, cholesterol, and body mass index, respectively, seems to be protective factors on the risk of developing dementia. Thus, hyperinsulinemia and short-term IR seem to be indicators of better health status and brain cognitive performance.
Conversely, late life diabetes status and hyperglycemia were observed to be associated with incident dementia in a cohort of older adults (mean age 76 years), after a longitudinal follow up of 5 years. Namely, a J-shaped association curve between HbA1c and incident dementia was found and both glycated albumin and fructosamine were associated with the risk of dementia [145]. Recently, Hanyu contributed to the identification of a specific subgroup of very old age patients with T2D that developed a different type of dementia, referred as diabetes related dementia (DrD), irrespective of AD pathology or cerebrovascular disease. Namely, the DrD-clinical phenotype of patients was characterized by very old ages, higher hemoglobin A1c, lower frequency of apolipoprotein E4 carrier, less severe temporal atrophy, higher frequency of insulin therapy, and slower progression of cognitive impairment, with prominent executive dysfunction. It is noteworthy that frequencies of frailty and sarcopenia/dynapenia were highly associated with this subtype of dementia, supporting the notion that DrD could be a modifiable cause of dementia in the conceptual framework of frailty [146].
FRAILTY AND DEMENTIA IN THE OLDEST OLD
Frailty is a complex and multidimensional geriatric syndrome, characterized by reduced homeostatic response to environmental stressors. Recent advances showed that dementia may be understood in the light of the accumulation of clinical deficits that increased the vulnerability to stressors [147].
The understanding of the relationship between frailty and dementia implies that the cumulative incidence of death differs between individuals which may display different degree of frailty.
Notably, frailty is growingly considered a harbinger of dementia; a series of neuropathological studies indicate that the rate of frailty progression is consistently associated with the accumulation of brain AD hallmarks (Aβ and hyperphosphorylated tau protein) and vascular brain insults, such as macro-infarcts and cerebrovascular disease [148, 149]. However, the link between frailty and dementia is poorly understood and, it is still unclear whether the clinical trajectories may run along the same pathogenetic pathways. Although higher levels of frailty have been independently associated with an increased risk of dementia, it is noteworthy that frailty should be considered alongside the longitudinal assessment of repeated cognitive performance [23]. Frailty was observed to predict the development of dementia with a modulating effect on the cognitive trajectories. In line with these notions, Wallace et al. [22] found that the huge spectrum of frailty in age-matched older adults was able to shape the clinical expression of dementia in relation to AD brain pathology. On the basis of these findings, it could be hypothesized that frailty might lower the threshold for the clinical expression of AD pathology as the individual ages, and a series of shared pathophysiological mechanisms such as immunoendocrinosenescence, insulin resistance, and inflammation could also count for this tight association [150].
So far, limited evidence pointed out that the presence of white matter vascular hyperintensities in T2-weighted MRI images was associated with an increased risk for dementia and frailty, especially with advancing age. Furthermore, the burden of white matter hyperintensities was observed to correlate with several markers of frailty, such as grip strength and walking speed. In line with this notion, Buchman et al. demonstrated that brain macroinfarcts and nigral neuronal loss may represent a common pathophysiological ground for the development of both dementia and frailty [149], boosting the pathophysiological interplay between frailty and dementia mixed pathology.
So far, the frailty construct has been linked to dementia in both cross-sectionally and longitudinal studied, and the inclusion of both conceptual frameworks for frailty, such as the cumulative model of clinical deficit accumulation and the physical frailty construct were equally investigated [22 , 152].
The operationalization of these clinical constructs in the framework of dementia may have important clinical implications for preventative approaches and multimodal interventions to delay both cognitive and clinical frailty [152] and warrant systematic observation in the next future.
The multidimensional assessment of frailty that includes the late life contribution of specific cardiovascular risk factors may substantially refine our understanding of the late life development of mixed dementia [152].
This new conceptualization supports the notion than dementia, especially in the very advanced ages, is a complex disease and it may serve as an interesting platform for the future understanding of the complex relationship between the highly heterogeneous phenotypic disease clinical expression of dementia and its brain mixed neuropathology (Fig. 1).
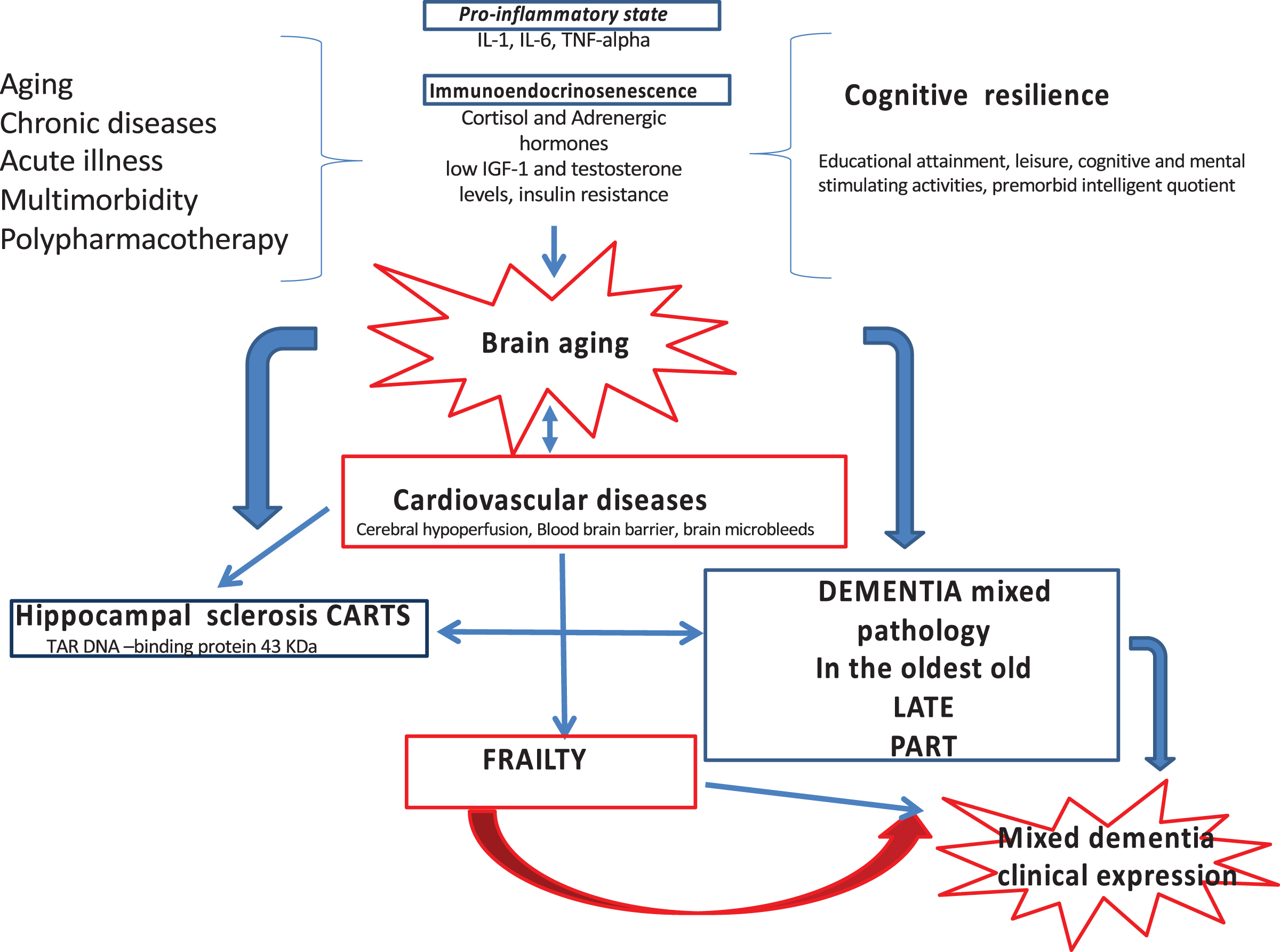
Newly developed conceptual framework on brain aging, cardiovascular comorbidity, dementia phenotypes, and clinical expressions in the older ages. MixD, mixed dementia; HS, hippocampal sclerosis, CARTS: cerebral age-related TDP-43 with sclerosis; CVD, cardiovascular disease; LATE, limbic-predominant age-related TDP-43 encephalopathy; PART, primary age-related tauopathy.
BRAIN MIXED DEMENTIA IN THE OLDEST OLD
In line with these above-mentioned assumptions, the recent formalization of limbic-predominant age-related TDP-43 encephalopathy (LATE diagnostic criteria) increased awareness of the mixed dementia forms of the oldest old. LATE-neuropathological changes included TDR 43 proteinopathy with a staging system according to autopsy findings, with or without coexisting hippocampal sclerosis pathology (LATE-neuropathological changes-NC). LATE is an amnestic dementia syndrome that mimic AD, sharing some genetic risk variants and pathogenetic mechanisms with both frontotemporal degeneration and AD. Many subjects with LATE have comorbid brain pathologies such as Aβ plaques and tauopathies. Due to the rapid expanding demography of oldest old subjects, the working group aimed at developing standardized diagnostic criteria, promoting awareness and research of this distinguished pathway of dementia in the very advanced age [153].
Similarly, the consortium term of primary age-related tauopathy (PART) was proposed by pathologists that observed localized neurofibrillary degeneration in brains from aged people with mild cognitive dysfunction. The diagnosis of PART is histological in nature, exhibiting mild to moderate tau deposits as neurofibrillary tangles (NFT), without or with few Aβ plaques [154].
In particular, biochemical and immunohistochemical studies indicated that the NFTs in PART contain mixed three-repeat (3R) and four-repeat (4R) isoforms of tau proteins, as seen in AD [155]. However, considering PART as being on the AD continuum is an area of active research, although it has been increasingly discouraged [17 , 157].
Indeed, PART is estimated to affect roughly 20% of aged people in their 80s or older, and is associated with a less severe cognitive impairment with lower Braak NFT stages than AD, with fewer, or absence of, Aβ plaques. In addition, the frequency of APOE ɛ4 is much lower compared with AD [158].
Notably, PART has been demonstrated to co-exist with other brain neurodegeneration such as TDP-43 proteinopathy, including cerebral age-related TDP-43 and hippocampal sclerosis, which has been identified in approximately 30% of PART cases as well [159].
Determining a common pathology in very old aged brains, with recognition of PART, will provide a further foundation for a better understanding of mixed age-related neurodegenerative changes and their mixed accumulated neuropathology.
CONCLUSIONS
Eventually, a better understanding of the brain “mixed” pathologies of the very old age is warranted, due to the growing biological complexity that serve for the identification of appropriate patient groups for targeted clinical trials.
In the very advanced age, TDP-43 pathologies seem to be a crossroad for brain mixed neurodegeneration with multiple overlapping pathological phenotypes that include CARTS and HS (Fig. 1). On one hand it could be hypothesized that new and unraveled neurobiological substrates, otherwise overshadowed by NFT and amyloid plaque neuropathological features in younger persons, could play a pathogenetic role in the onset of dementia in late life. On the other hand, a better understanding of the definition and measurement of the construct of cognitive resilience with the identification of reserve, maintenance, and compensation may help explaining the paradox of resilience according to aging, boosting validity in very old ages as well. Moreover, the longitudinal assessment of its neural and behavioral correlates according to aging may unveil the plausible mechanisms of individual cognitive resilience also in late life in the face of typical age-related neural decline [160].
Notably, the present findings contribute to shape a new conceptual framework due to the heterogeneous and complex underpinnings of dementia in the oldest old. Namely, the intersections of the aging brain with common age-related chronic conditions such as cardiovascular diseases will need a radical change in the paradigm of dementia causation in late life. In line with that, a sharp reverse epidemiology for cardiovascular diseases is observed in the very advanced ages, with opposite prognostic associations compared to middle life and young old. This new epidemiology of the oldest old addresses the need of a brand-new thinking regarding disease etiopathogenesis, the temporal and causative origin, its development and clinical expression of brain mixed dementia in older ages. Similarly, the relationship of dementia with frailty in very old ages may reveal several nested high hurdles on how cognitive resilience and frailty may be key relevant mediators in the modulation of the clinical expression of brain mixed neuropathologies in persons over 85 years old. The identification of this clinical interplay may inspire new and continuous efforts in preventing or delaying cognitive decline in late life.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/19-1075r2).