
Abstract
Dementia is a severe neurodegenerative disorder and it can be categorized into several subtypes by different pathogenic causes. We sought to comprehensively analyzed the prevalence of dementia from perspectives of geographic region (Asia, Africa, South America, and Europe/North America), age, and gender. We searched PubMed and EMBASE for relevant articles on dementia published from January 1985 to August 2019. In these studies, analyses were stratified by geographic region, age, and gender. Meta-regression was conducted to identify if there were significant differences between groups. We included forty-seven studies. Among the individuals aged 50 and over in the community, the pooled prevalence for all-cause dementia, Alzheimer’s disease, and vascular dementia were 697 (CI95%: 546–864) per 10,000 persons, 324 (CI95%: 228–460) per 10,000 persons, and 116 (CI95%: 86–157) per 10,000 persons, respectively. In our study, the prevalence of all-type dementia in individuals aged 100 years and older (6,592 per 10,000 cases) is 244 times higher than in those aged 50–59 (27 per 10,000 cases). The number of people living with dementia approximately doubles every five years. The prevalence was greater in women than in men (788 cases versus 561 cases per 10,000 persons) in overall analysis. In individuals aged 60 to 69 years, AD prevalence in females was 1.9 times greater than that in males (108 cases versus 56 cases per 10,000 persons), while the prevalence of VaD was 1.8 times greater in males than in females (56 cases versus 32 cases per 10,000 persons). Prevalence rate was higher in Europe and North America than in Asia, Africa, and South America.
INTRODUCTION
Dementia is one of the most common neurodegenerative diseases. It induces memory loss, thinking impairments, and declining ability to perform everyday activities. Alzheimer’s disease (AD), vascular dementia (VaD), dementia with Lewy bodies, and frontotemporal dementia are the most common underlying pathologies. The available data showed that AD made up about 60% of cases of dementia and VaD accounted for 20% [1, 2]. It is difficult to make a distinction between AD and VaD due to their overlaps in symptomatology, pathophysiology, and risk factors [3–5]. Each pathology contributes at different levels, resulting in a range of patients with pure cerebrovascular disease and pure AD representing the extremes of the spectrum [3, 5].
Until 2018, the global number of people living with dementia has been estimated at 50 million [6], and the number will triple by 2050. This population aging has significant effects on the emergence of dementia, following the growth in disability and dependence [7, 8]. The numbers and proportion of older people are rapidly increasing in developing countries (India, Latin America, and China) [9] and dementia made the largest contribution to disability in these regions [7]. It has been a huge burden for families, health-care systems, and even the whole society to care and support patients with dementia [10]. Globally, the cost of the disease is about a trillion US dollars a year, and the expenditure is forecast to double by 2030.
In theory, door-to-door or population-based random sampling in these studies offers a more reliable way since the method include potential patients who do not seek health care [11]. However, the diversification of screening tools has to be recognized as a major problem in the estimation of the true prevalence [12] and the variation in language and culture, as well as levels of literacy, make it a huge barrier to overcome.
Our study is to examine the prevalence of dementia and its major causes worldwide through a meta-analysis of published, population-based epidemiological studies (see Supplementary Material 1). This analysis is an update and extension of previous reports on the epidemiology of this disease [13].
MATERIALS AND METHODS
Selection of studies
We searched both PubMed and EMBASE databases with search strategy of using terms “dementia”, or “Alzheimer’s Disease”, and terms “prevalence”, or and “epidemiology” (see Supplementary Material 2). The bibliographies of prior systematic reviews were also checked manually. We included studies published in English or Chinese. Articles had to simultaneously meet the following inclusion criteria: 1) population-based random samples or door-to-door surveys; 2) original data; 3) prevalence and/or epidemiology estimate of dementia; 4) age and sex explicitly grouped. As people in institutions showed higher prevalence, we included studies only in communities. Two reviewers independently read titles and abstracts of publications imported into the electronic databases and excluded duplicate data and those that did not meet the inclusion standards. If the two reviewers had disagreement, a third reviewer would join in and discuss until reaching consensus.
Data extraction
A standard data collection form was created to extract basic demographic information, including geographic location, study types, methods used to identify population, data sources (i.e., communities or communities and institutions), screening tests, diagnostic criteria, and recruitment period, etc. For consistency, the numbers of dementia cases and screening population were used to calculate the prevalence (see Supplementary Material 3). Age and sex data were recorded for subgroup analyses. The pooled prevalence rate reported in each study was 1 in 10,000.
Quality assessment
An assessment tool (see Supplementary Material 4 for quality criteria) was employed to estimate the representativeness of each prevalence study included [14]. The tool assessed three aspects, including sample representativeness, methods used to determine the presence of dementia, and statistical methods. Studies were scored on a scale from 0 to 8 based on the extent to which they fulfill 8 assessments. Articles with 8 points showed best performance on statistical analysis, criteria assessment, and population representativeness (see Supplementary Material 5 for quality criteria assessment score).
Data synthesis
The prevalence and 95% confidence intervals (CI95%) were calculated based on the number of dementia cases and participants collected. Data were stratified into several subgroups by age, gender, and geographic region. Geographic regions included South America, Asia, Africa, Europe, and North America. Data from Europe and North America were merged together, not only because both regions have a small number of published articles, but also because the predominant population in both regions is whites. Subtypes of dementia, whose prevalence studies were reported in two or more studies, such as AD and VaD, were analyzed in the same way. We calculated Cochrane Q statistic and used I2 to quantify the magnitude of heterogeneity between studies. A random effects model was used to calculate merged prevalence rates and 95% confidence intervals. Since prevalence rate is a ratio, estimates were pooled using a double arcsine transformation to standardize the data [15]. Meta-regression was employed to discover significant differences between groups. A sensitivity analysis was performed (see Supplementary Material 6 for sensitivity analysis). The source of statistical heterogeneity would be reviewed and reviewers would discuss whether the source was excluded.
R version 3.3.2 was used for all statistical analyses. The R package for meta-analysis was employed to generate the merged estimates and forest plots. The metaphor package was used to conduct the meta-regression by restricted maximum likelihood estimation [16]. A p value < 0.05 was considered statistically significant.
RESULTS
The search yielded a total of 25,455 citations from PubMed and EMBASE. After reading the abstracts, 25,088 publications were excluded as clearly ineligible, leaving 367 for further review. A total of 202 articles were excluded with various reasons: 95 did not report an epidemiology or prevalence of dementia, 55 provided no original data, 29 were not population-based, 13 were not in English or Chinese, and 10 were published before 1985. Finally, 47 door-to-door or population-based prevalence studies were identified (Fig. 1).
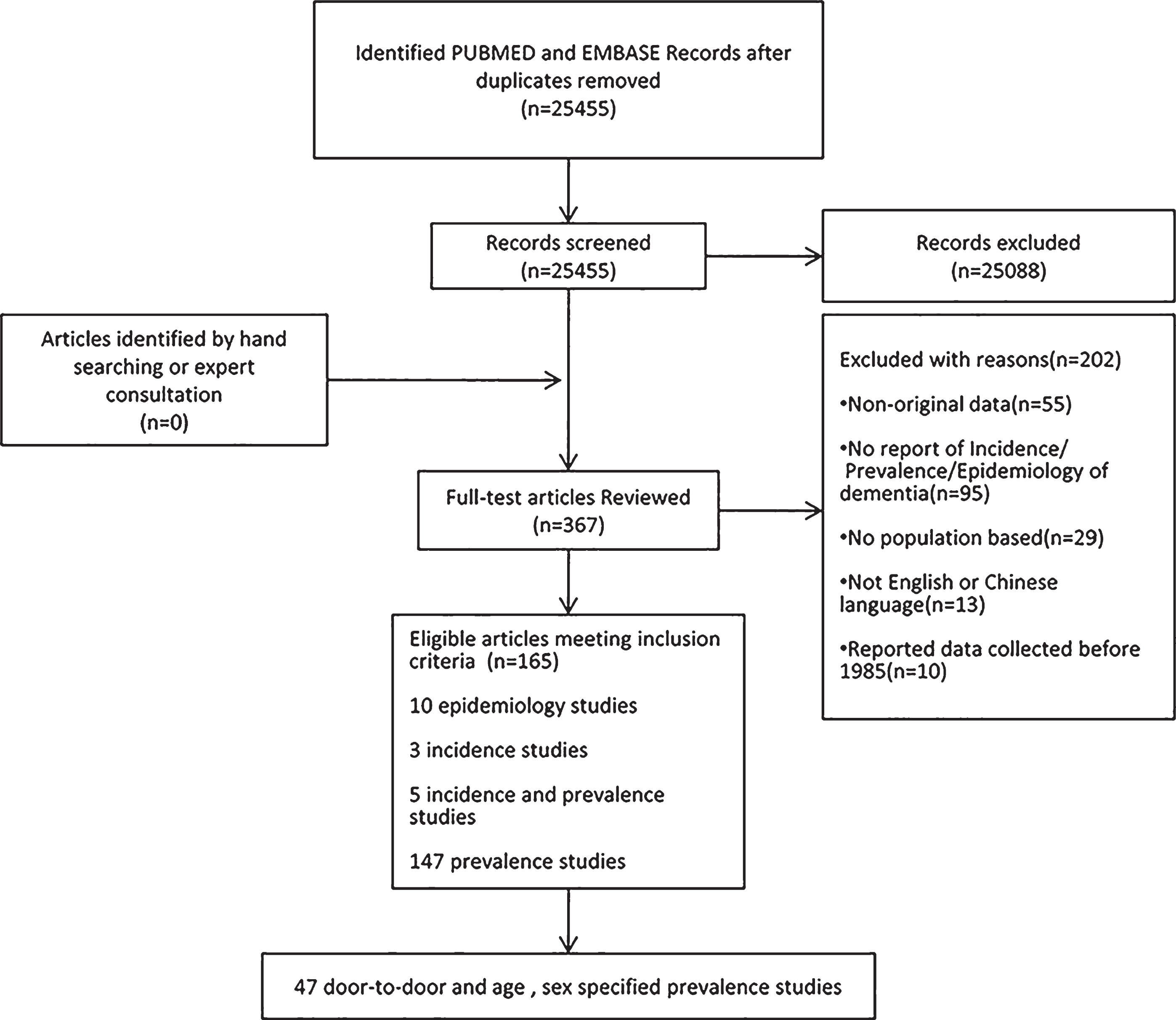
Study flow diagram.
Of the 47 included studies, 25 were from Asia [17–41], 17 from Europe and North America [42–58], 3 from Africa [59–61], and 2 from South America [62, 63]. In addition to the prevalence of all types of dementia, 22 articles reported the prevalence of AD, among which 17 also covered that of VaD (see Supplementary Material 7). Most studies conducted a two-stage survey to identify patients with dementia. In phase 1, participants were screened by questionnaires. The Mini-Mental State Examination (MMSE) and its other versions were widely used. In phase 2, all cases that showed questionable or definite cognitive impairment in phase 1 were examined by a health care professional (usually a neurologist). A diagnosis was confirmed by consensus of several professionals. The Diagnostic and Statistical Manual of Mental Disorders (DSM; DSM-III, DSM-IV, or DSM-V) were adopted in most studies to identify patients with dementia; the 10th edition of the International Classification of Disease (ICD-10) was applied to only one study; and the diagnostic criteria in three studies were unclear. AD was diagnosed using the National Institute of Neurological and Communication Disorders and Stroke-Alzheimer’s disease and Related Disorders Association (NINCDS-ADRDA). VaD was confirmed by the National Institute of Neurological Disorders and Stroke-Association Inter-nationale pour la Recherche et l’EnseignementenNeuroscience (NINDS-AIREN).
The effect of age on the prevalence
The meta-analysis showed an increasing prevalence of all-type dementia with age: 27 per 10,000 in persons 50 to 59 years; 80 per 10,000 in persons 55 to 64 years; 183 per 10,000 in persons 60 to 69 years; 267 per 10,000 in persons 65 to 74 years; 514 per 10,000 in persons 70 to 79 years; 1,510 per 10,000 in persons 80 to 89 years; and 3,572 per 10,000 in persons 90 to 99 years; 6,592 per 10,000 in persons over age 100 (Fig. 2). The prevalence of all types of dementia in individuals aged 100 years and older was 244 times higher than that in individuals aged 50–59 years. The number of people with dementia approximately doubles every five years of age globally. For AD and VaD, 86 and 40 per 10,000 in the 60 to 69 age group; 307 and 105 per 10,000 in the 70 to 79 age group; 1,088 and 235 per 10,000 in the 80 to 89 age group; 2,615 and 548 per 10,000 in persons over age 90, respectively (Figs. 3 and 4). Although prevalence rates grew dramatically with age, the difference in prevalence rate between age groups was not statistically significant.
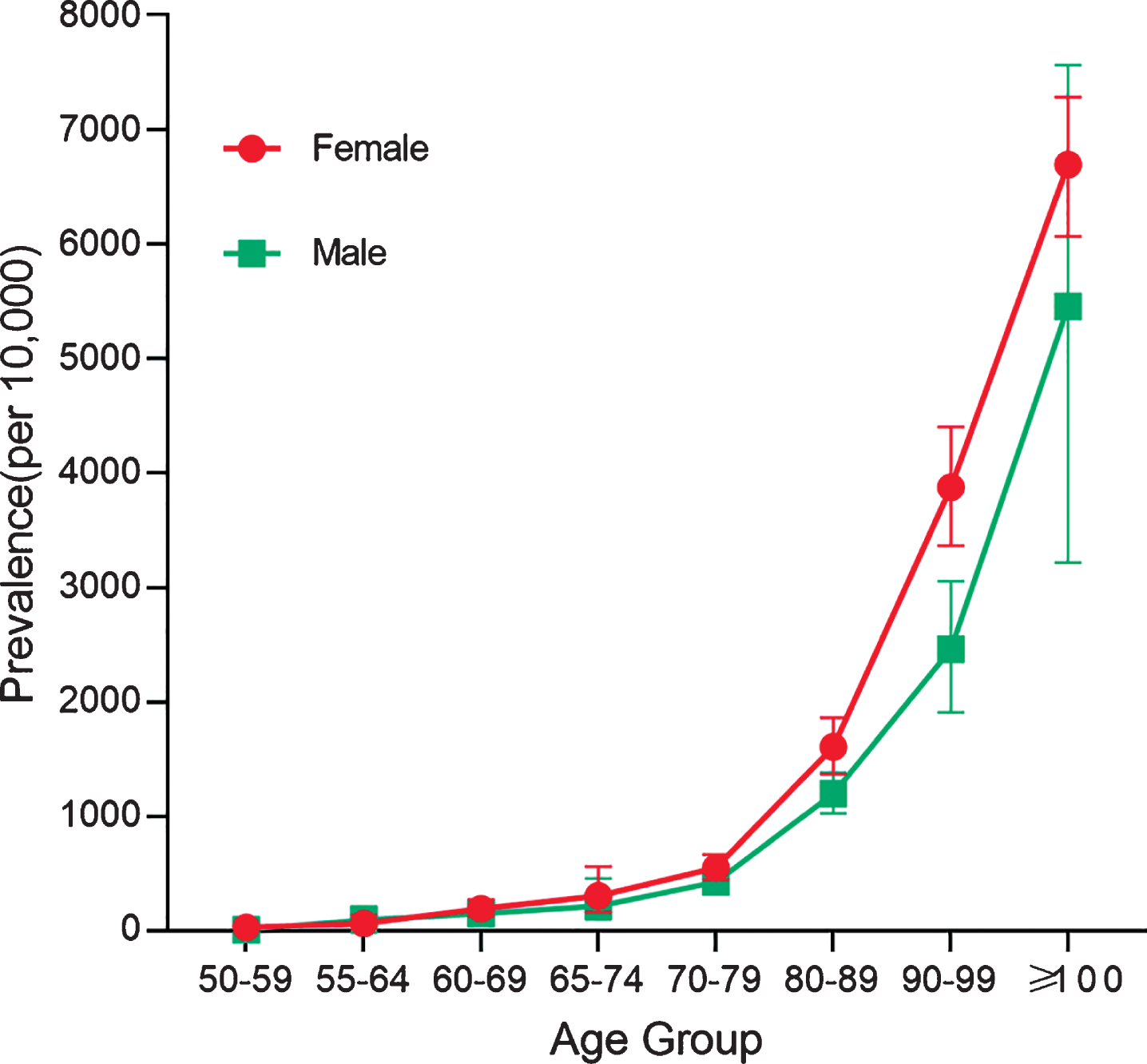
Prevalence of all-type dementia in groups stratified by gender (men = green, women = red) and age. Except for people aged 55 to 64 years, the prevalence of all-type dementia was higher in females compared to males. The pooled prevalences for the groups aged 50 to 59 years, 55 to 64 years, 60 to 69 years, 65 to 74 years, 70 to 79 years, 80 to 89 years, 90 to 99 years as well as 100 years and older were 12, 99, 153, 220, 431, 1,202, 2,464, and 5,455 per 10,000 persons in males, respectively. In females, the pooled prevalences were 33, 67, 195, 308, 554, 1,611, 3,879, and 6,694 per 10,000 persons.
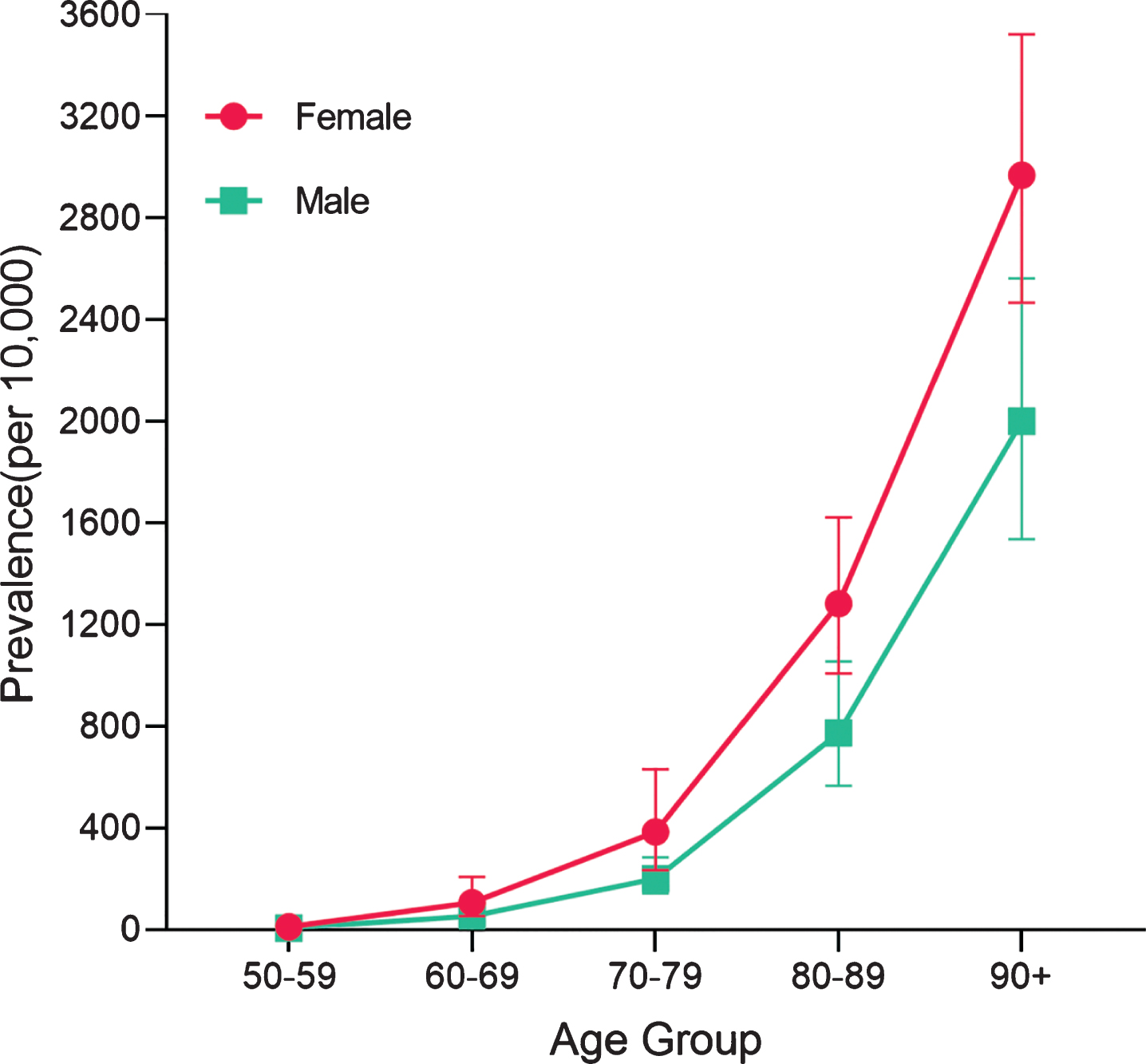
Prevalence of AD in groups stratified by gender and age. Females showed higher prevalence of AD than males. The pooled prevalences for the groups aged 50 to 59 years, 60 to 69 years, 70 to 79 years, 80 to 89 years, as well as 90 years and older were 8, 56, 203, 776, and 1,999 per 10,000 persons in males, respectively. In females, the pooled prevalences were 14, 108, 387, 1,284, and 2,966 per 10,000 persons.
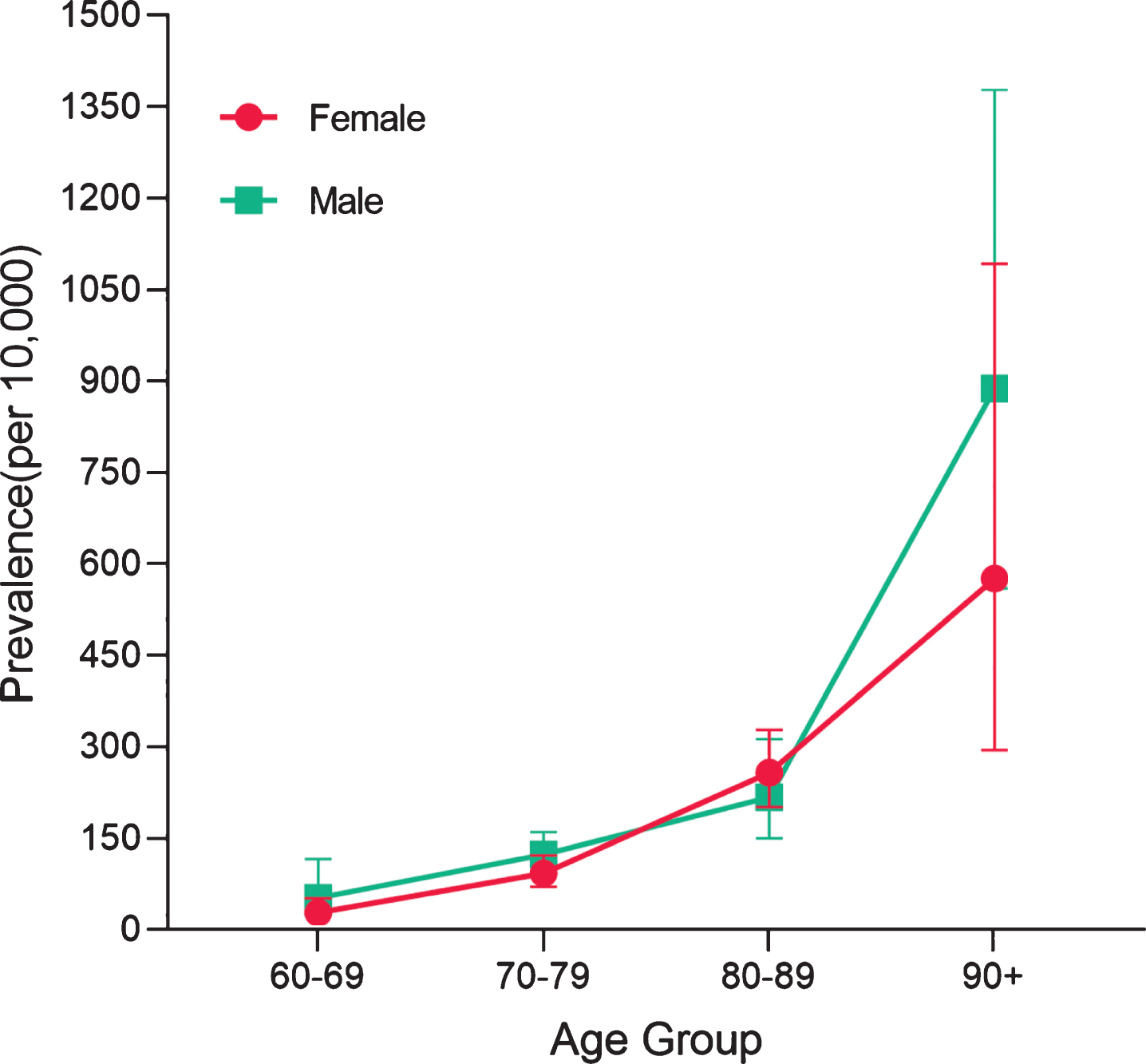
Prevalence of VaD in groups stratified by gender and age. The gender preponderance was not showed in cases with VaD. The pooled prevalences for the groups aged 60 to 69 years, 70 to 79 years, 80 to 89 years, as well as 90 years and older were 56, 127, 220, and 887 per 10,000 persons in males, respectively. In females, the pooled prevalences were 32, 96, 260, and 577 per 10,000 persons.
The sustained growth momentum of prevalence with age was reflected in geographic distribution as well (Fig. 5). No significant difference was found between Asian and European individuals of the same age. Studies conducted in Africa and South America were insufficient to be analyzed by age and geographic location.
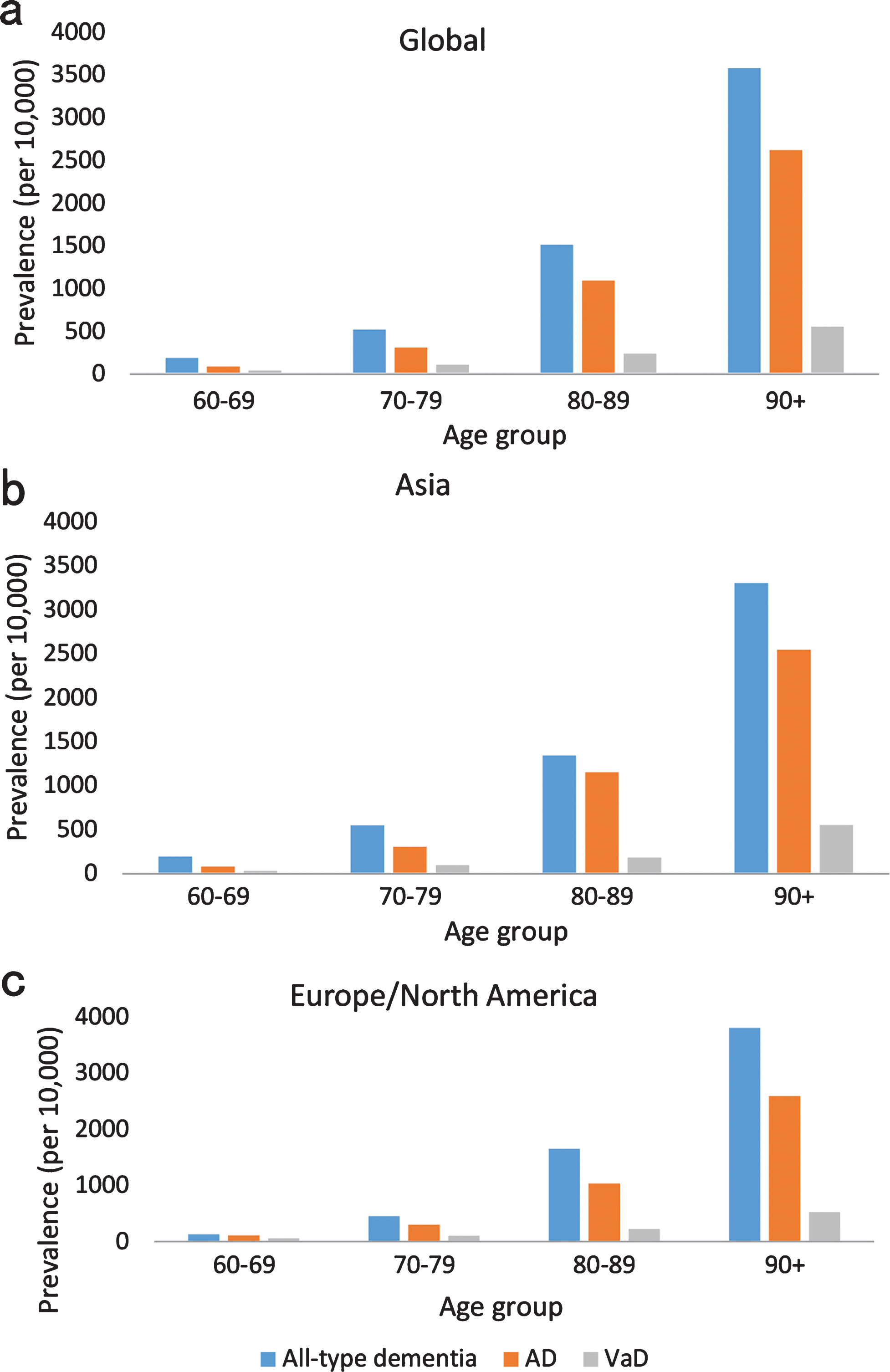
Prevalence of all-type dementia, AD, and VaD in groups stratified by age and geographic location. The sustained growth momentum of prevalence with age reflected in geographic distribution. Panel a shows the global prevalences of all-type dementia for the groups aged 60 to 69 years, 70 to 79 years, 80 to 89 years, as well as 90 years and older were 183, 514, 1,510, and 3,572 per 10,000 persons; the pooled prevalences of AD were 86, 307, 1,088, and 2,515 per 10,000 persons; the pooled prevalences of VaD were 40, 105, 235, and 548 per 10,000 persons. Panel b shows that in Asia, the pooled prevalences of all-type dementia for the groups aged 60 to 69 years, 70 to 79 years, 80 to 89 years, as well as 90 years and older were 195, 550, 1,343, and 3,299 per 10,000 persons; the pooled prevalences of AD were 83, 307, 1,152, and 2,541 per 10,000 persons; the pooled prevalences of VaD were 31, 99, 184, and 553 per 10,000 persons. Panel c shows that in Europe and North America, the pooled prevalences of all-type dementia for the groups aged 60 to 69 years, 70 to 79 years, 80 to 89 years, as well as 90 years and older were 134, 463, 1,660, and 3,800 per 10,000 persons; the pooled prevalences of AD were 115, 310, 1,040, and 2,595 per 10,000 persons; the pooled prevalences of VaD were 64, 112, 234, and 531 per 10,000 persons.
Gender influence on the prevalence
The impact of gender on the prevalence rate of dementia was stratified and estimated by age group and by geographic position as well. Females in the 80 to 89 (1,611 per 10,000) and 90 to 99 (3,879 per 10,000) age groups showed a significantly higher prevalence rate of all types of dementia compared with males of the same age (1,202 per 10,000 versus 2,464 per 10,000; p < 0.05). A slight, nonsignificant female superiority of all types of dementia and AD was present in most other age groups. The sexual preponderance was not shown in cases with VaD. In individuals aged 60 to 69 years, the prevalence of AD in females was 1.9 times higher than that in males (108 cases versus 56 cases per 10,000 persons), while the prevalence rate of VaD was 1.8 times higher in males than females (56 cases versus 32 cases per 10,000 persons). Nevertheless, the differences did not reach statistical significance.
In the analysis stratified by geographic region, females in Europe and North America showed a significantly increased prevalence rate of all types of dementia (1,238 per 10,000) compared to males in the same region (878 per 10,000; p < 0.05), while gender difference in the prevalence rate was not statistically significant in Asia. Data were insufficient to analyze the difference between males and females in other age and region groups.
The impact of geography on the prevalence
Prevalence rate was higher in Europe and North America (1,123 cases per 10,000 persons) than in South America (648 cases per 10,000 persons), Asia (523 cases per 10,000 persons), and Africa (275 cases per 10,000 persons). The preponderance did not reach statistical significance (Table 1). However, our study identified in the 60- to 69-year-old population a lower prevalence of dementia in Europe and North America (not reaching statistical significance) compared with other regions.
Prevalence of dementia by sex and geographic location (per 10,000)
DISCUSSION
General comments on methodology
Our study has ascertained that some differences in prevalence rates of all types of dementia, AD, and VaD were associated with age, gender, and geographic region. Many factors, such as education levels, genes, and obesity [64], have been reported to be responsible for the prevalence rates. Confounders arising from populations or methodological differences within the included studies were inevitable in our findings, as in all other meta-analyses.
Besides, differences in inclusion and diagnostic criteria of the studies included in an analysis can influence the prevalence rates. The frequency of dementia varied dramatically when different systems of diagnostic classification were used [65]. A few studies have reported lower prevalence rates by applying ICD-10 criteria compared with DSM-III [56] or DSM-III-R [65] for the reason that ICD-10 includes more detailed requirements. Disagreement also existed in different versions of DSM [65]. The criteria commonly used to diagnose dementia can differ by up to 10 times in the number of diagnosed patients. When it comes to VaD, the major difficulty is the absence of a strict and reliable definition [66]. The concept of VaD refers only to the latest stage of the cognitive decline occurring in patients with cerebrovascular disease and it may encompass other types of dementia, leading to overlaps of the prevalence estimates. Variation in methods of identification may have showed a significant influence on the reported rates of dementia across studies as well. Traditionally, two or more phases of ascertainment were conducted in most of the population detection included. Multiphase studies are complicated by high loss to follow-up occurring between the screening and diagnostic assessments [67], leading to under- or overestimation of the genuine prevalence [68]. The poor coverage of population estimates in many world regions may have profound effects on reported prevalence rates [69]. Coverage was good in high-income countries, but estimates were lacking in many developing countries. However, 60% people with dementia live in low or middle income countries. Studies included in our study showed geographic maldistribution as well.
Geographic variability
Analyses of geographic variation of prevalence are easily confounded by demographic variations between populations. We attempted to control for the effects of demographic differences by comparing within age groups across regions. The differ of region in the prevalence could be attributed to diversities of environments and genes.
Gender division
Our analysis displayed gender differences in the prevalence, with a higher prevalence rate of all-type dementia and AD in females than in males, particularly those at older ages (80 to 89- and 90 to 99-year age groups; p < 0.05). The gender difference had less impact on the prevalence of VaD. The higher prevalence of dementia among women than men has been reported in most of epidemiology studies. A meta-analysis of dementia prevalence in Europe identified 85-year-old as an age-shed: under 85 years old, the prevalence rate of VaD was higher in men compared to women; thereafter, the prevalence in women was higher [70]. However, our study failed to verify this.
A prospective cohort conducted by Helmer et al. [71] showed that women with dementia had longer survival than men with dementia, particularly for AD, although some evidence showed that women with dementia seemed to lose slightly more years of their remaining lifespan than men [72]. A higher incidence among older women may contribute to gender effect on prevalence [73]. The absence of gender preponderance in VaD may be explained partly by diagnostic uncertainties [4], and partly by complicated underlying mechanisms [66].
Age factor
Our study identified that dementia prevalence sharply increased with age across all regions of the world, which is in agreement with some previous studies [75]. The prevalence rates may continue growing with extended lifespan. Until 2016, dementia had been the fifth-largest cause of death after ischemic heart disease, chronic obstructive pulmonary disease, intracerebral hemorrhage, and ischemic stroke [74]. For persons aged over 70 years, dementia was only second to ischemic heart disease as causes of death [75]. The rising tendency with age probably contributed to an underestimate of the true prevalence, especially for the oldest old.
A few studies have reported that in surveys conducted among Chinese individuals, usually one year was added to participants’ actual age [76], which may influence the results. When it comes to the oldest old, patients are probably detected through their families, caregivers, or medical records rather than themselves [51], which also affects the results because the number of elderly patients in any given study is mostly small. Thus, a few reported cases can have significant impact. Nevertheless, the increase in prevalence with age is not suitable for all age groups. Previous studies showed that people aged at least 110 years can maintain normal cognitive function at 100 years of age probably due to extremely low frequencies of the dementia-related gene in supercentenarians [77].
The prevalences of dementia were easily affected by the lifespan of individuals and changes over time in the incidence of dementia. Although we did not perform a time trend analysis of dementia prevalence, we might expect that the prevalence of dementia continues growing over time in the aging population and increases in incidence, as well as no effective disease-modifying cure or treatment for the disease [74].
Our study has displayed slight differences in the prevalence of dementia and its major types between subgroups stratified by age, geographic region, and gender; nevertheless, it has also indicated the problems immanent in conducting epidemiologic studies across broadly diverse cultures, populations, and regions. Methodological defects and variability exist in studies included in our analysis more or less. Consensus statements on minimum scientific standards for epidemiological research are expected to improve the quality and consistency of follow-up studies.
Our systematic review suggests the possibility of geographic variation in the prevalence rate of dementia despite the maldistribution of studies included. Further epidemiologic evaluations with standardized diagnostic criteria and screening instruments are warranted to ensure greater comparability.
As aging is expected to continue, the key to reducing burden and related costs is to identify effective preventive or treatment measures. We expect to encourage policymakers, civil organizations, and multidisciplinary researchers to recognize dementia as a rising threat to global health, especially in developing countries. We hope that our study will contribute to the priority of dementia in social care and public health priority worldwide.
Footnotes
ACKNOWLEDGMENTS
This study was supported by grants from the National Natural Science Foundation of China (91849126, 81571245, and 81771148), the National Key R&D Program of China (2018YFC1314700), Shanghai Municipal Science and Technology Major Project (No.2018SHZDZX01) and ZHANGJIANG LAB, Tianqiao and Chrissy Chen Institute, and the State Key Laboratory of Neurobiology and Frontiers Center for Brain Science of Ministry of Education, Fudan University.