
Abstract
Background:
Major surgery has been associated with perioperative neurocognitive disorders (PND), but the contributing factors and long-term prognosis are uncertain. We hypothesize that preclinical Alzheimer’s disease (AD) might predispose to cognitive deterioration after surgery.
Objective:
To analyze the effect of amyloid-β on the cognitive trajectory after orthopedic surgery in a sample of non-demented subjects.
Methods:
Non-demented individuals older than 65 years that were on the waiting list for orthopedic surgery with spinal anesthesia underwent a neuropsychological assessment before and after surgery. During surgery, cerebrospinal fluid samples were obtained to determine AD biomarkers.
Results:
Cumulative incidence of PND was 55.2%during a mean follow-up of nine months. The most affected cognitive domains were executive function and constructional praxis. The presence of abnormal levels of amyloid-β was associated to a postoperative impairment in verbal and visual memory tests. According to their AD biomarker profile, participants were categorized as either Amyloid Positive (A+) or Amyloid Negative (A-). The incidence of PND did not differ between both groups. The A- group showed a tendency similar to the global sample, worsening in executive function tests and improving on memory scales due to practice effects. In contrast, the A + group showed a notable worsening on memory performance.
Conclusion:
Our findings support the hypothesis that surgery may promote or accelerate memory decline in cognitively asymptomatic subjects with brain amyloid-β deposits.
INTRODUCTION
The prevalence of cerebral amyloid pathology in cognitively asymptomatic individuals increases with age. It has been estimated that 21.1%of the population at the age of 65 will have a positive amyloid scan or a pathological cerebrospinal fluid (CSF) amyloid-β determination, and which will double by the age of 90 [1]. According to the new NIA-AA Research Framework for Alzheimer’s disease (AD), these individuals are considered to be within the spectrum of AD [2]. However, their prognosis is currently uncertain, and to a large extent we do not know which factors are associated with their progression to dem-entia of the AD type.
Due to the aging of our societies and advances made in medical care, an increasing number of elderly and more fragile people are considered candidates for major surgery. In preoperative screenings, respiratory and cardiovascular functions are routinely checked; however, it is not commonly assessed how the brain is going to cope with the intervention.
Perioperative neurocognitive disorders (PND) designate a cognitive decline occurring in the context or after a surgical procedure. The rate of PND has been estimated to be approximately 15%at 3 months. A recent systematic review reported a pooled incidence of PND after non-cardiac surgery at 3 months of 11.7%but ranging between 5.2%and 46.3%[3]. Indeed, in orthopedic patients, there have been re-ported incidences as high as 72%[4]. This variability is partially explained by the great heterogeneity among studies regarding the neuropsychological criteria defining PND, the timing of evaluation and the tests administered, which are sometimes limited to brief bedside tests such as the Mini-Mental State Examination (MMSE). This also has precluded outlining a specific neuropsychological profile of PND. One additional methodological difficulty is the fact that PND is a dynamic entity as, by definition, it con-stitutes a decline from a previous cognitive situation and in many cases, it can remediate entirely within 3 to 12 months [5, 6]. This means that the incidences will vary depending on the time point of assessment and that for its estimation it is necessary to have a baseline evaluation. Great efforts have been made to establish more precise definitions of PND, which resulted in a consensus article published in 2018 [7]. The developed framework recommends specific terms depending on the time point of assessment and the degree of cognitive impairment. The term Postoperative Major Neurocognitive Disorder is proposed for those cases with an objective decline in the neuropsychological performance greater than 2 standard deviations (SD) in the period comprised between 30 days and 12 months after surgery. However, this body of recommendations does not specify individual neuropsychological tests or the number of tests required in the diagnostic work-up.
Even though PND has been recognized for more than one century, many questions about its pathogenesis remain unsolved. The risk factors most fre-quently described for PND include advanced age, low level of education, postoperative delirium, and use of sedatives [3, 6]. Multiple reports have linked it to a greater morbimortality [8] and an increased risk of dementia [9, 10]. This raises the question of whether PND can be promoted or even constitutes an early manifestation of AD in an undiagnosed individual. Unfortunately, not many studies addressing PND include an evaluation of AD biomarkers, but an association between low levels of amyloid-β in CSF and a higher incidence of PND has been reported [11] as well as gradual cognitive impairment [12] and lower CSF amyloid-β/total tau ratio in PND patients [13].
In this work, we describe the trajectory of the cognitive performance in a sample of non-demented elders undergoing elective orthopedic surgery and the influence of preclinical AD pathology. For that purpose, a comprehensive neuropsychological examination was performed before and after surgery and CSF samples were collected during spinal anesthesia to determine AD core biomarkers. We hypothesize that preclinical AD might predispose to cognitive deterioration after surgery, and in those individuals with amyloid-β pathology in their brains we might expect a worsening in neuropsychological performance.
MATERIALS AND METHODS
Study design and inclusion criteria
Our population sample was composed of indivi-duals older than 65 years and free of dementia who were included in the waiting list for orthopedic surgery with spinal anesthesia for a hip or knee rep-lacement. The baseline visit took place 1–2 months prior to surgery and participants were clinically and cognitively assessed by a neurologist and a neuropsychologist. Also, a functional evaluation was carried out through the Clinical Dementia Rating Sum of Boxes (CDR sob) [14] by a certified rater (APC). Individuals with dementia (CDR ≥1 and/or MMSE ≤24) were excluded, as well as those with substantial comorbidities and those conditions that could significantly interfere with the neuropsychological assessment, as severe hypoacusia or reduced visual acuity.
After surgery, participants were followed up during their hospitalization to detect the occurrence of delirium using the CAM test (Confusion Assessment Method), which was administered once a day by a neurologist (AGS) [15].
A second clinical and cognitive evaluation was repeated in the following 6 to 8 months and it included the same neuropsychological battery from the baseline visit and CDR sob to detect a possible functional deterioration. Incident cases of dementia were established based on the information extracted from the clinical interview and/or a CDR result ≥1, according to current diagnostic criteria [16].
This study was approved by the Local Ethics Committee and written informed consent was obtained in all cases.
Neuropsychological evaluation and definition of PND
Our goal was to test whether the cognitive pattern associated to PND resemble those changes typical of early AD. According to this, a comprehensive neuropsychological protocol was designed in order to evaluate which cognitive domains were more affected in PND, with a special emphasis in those which could be more vulnerable to AD pathology. Thus, the neuropsychological examination comprised the main cognitive areas, including verbal memory (Free and Cued Selective Reminding Test (FCSRT) [17], Memory and Weschler Memory Scale-III Logical Memory subtest (WMS-III LM) [18]); visual memory (Rey-Osterrieth Complex Figure Test (RCFT) Free Delayed Recall [19–21], CERAD Constructional Praxis Recall [22]); attention and executive function (Forward, Backward and Total Digit Span [23], Trail Making Test parts A and B [23], Phonemic Fluency [24]); language (Boston Naming Test [25], Semantic Fluency [24]); constructional praxis (RCFT Copy [19–21], CERAD Constructional Praxis [22]); and visuospatial function (the Number Location subtest from the Visual Object and Space Perception Battery (VOSP) [26]).
Baseline cognitive functioning was evaluated based on reference values established by NEURO-NORMA, a multicentric study which evaluated the performance of the Spanish population in the most frequently used neuropsychological tests and thus offers normative values for each age and educational range [27]. There exist available NEURONORMA normative values for the following tests that were part of our battery: FCSRT, RCFT, Digit Span, TMTA and TMTB, Letter Fluency, Semantic Fluency, Boston Naming Test, and VOSP. To estimate the incidence of PND, One-year Reference Norms of Cog-nitive Change in Spanish old adults from the NEURONORMA sample were used to calculate the Sta-ndardized Regression-Based scores (SRB) for each participant and test [28]. This is a methodology that allows the comparison of the expected cognitive change over time in the general population to a specific subject and offers an estimation that takes into account practice effects, age, and educational level. For its calculation, firstly the latter test score is predicted based on the baseline score and the soci-odemographic variables which resulted significant in the regression analysis for that particular test. After that, the predicted score is subtracted from the actual second score and divided by the standard error of the estimate (SEE). The result is expressed in standard deviations (SD). This same method has been previously used to compare the evolution in neuropsycho-logical performance between postoperative patients and control groups [11, 29]. According to the current framework recommendations, PND was defined at the individual level when SRB was equal to -2 SD or more in at least one of the neuropsychological tests included in NEURONORMA.
Analytical procedures
The lumbar puncture performed for the anesthe-tic procedure was used to obtain a sample of CSF for the assessment of amyloid-β (Aβ42), total tau (t-tau), and phosphorylated tau (p-tau181). The lev-els of biomarkers were quantified by ELISA INNOTEST (Innogenetics, Fujirebio Europe, Belgium) and interpreted according to cut-off points previously established in our center based on two independent samples of subjects with AD and healthy volunteers. Individuals were categorized according to an Aβ42 cut-off point of 663.5 pg/mL in A + and A-. Those participants A- but with t-tau above the cut-off point of 455.8 pg/mL were considered as SNAP (Suspected Non-Alzheimer Pathology). Our cut-off point value for p-tau181 levels was 68 pg/mL.
Statistical analysis
Incident PND cases were defined based on current recommendations [7]. Differences in baseline characteristics according to the development of PND were tested by independent samples t-test and χ2. Changes in postoperative cognitive performance compared to baseline were investigated by linear mixed models. In order to test specifically the effect of amyloid-β status (A + versus A-) on each neuropsychological result over time, we included the interaction between amyloid-β and time, in addition to age, sex, amyloid-β, and time as covariates. We were also interested in comparing the cognitive performance between groups depending on their AD CSF biomarker status at each time point, which was analyzed by independent samples t-test and sex and age-adjusted by general linear models. Correction for multiple comparisons was made with False Discovery Rate (FDR). All data analyses were performed in SPSS (Statistical Package for Social Sciences, 10.0.1).
RESULTS
Demographics and basal assessment
We recruited 44 participants, predominantly fe-males (65.9%), with a mean age of 73.4 (range 65–94 years). They all underwent at least an initial neuropsychological evaluation and CSF analysis. The mean MMSE score was 28.4 (range 25–30). The CSF analysis revealed at least one abnormal AD biomarker in 13 subjects (29.54%). An abnormal level of Aβ42 was found in 10 of them (22.7%), who were considered the A + group. Only one of the A + had, in addition, an abnormal level of p-tau181 and borderline t-tau. The other three subjects showed abnormal levels of t-tau and p-tau181 with unaltered Aβ42 and so were categorized as SNAP (Table 1). The A- group combined SNAP and subjects with normal CSF biomarkers.
Sample Characteristics
SD, standard deviation; MMSE, Mini-Mental State Examination. CSF Neurodegeneration Biomarkers N (%) expresses the percentage of subjects with abnormal neurodegeneration biomarkers for each subgroup.
According to the CDR evaluation, 19 participants obtained a score of 0.5 in the baseline evaluation and therefore were categorized as mild cognitive impairment (MCI). None of these participants have previously sought for clinical advice because of cognitive complaints. There were no significant differ-ences in their mean age in comparison with the cognitively unimpaired group (74.9±5.6 versus 72.2±6.9 years, p = 0.18) and they displayed a borderline normal score on the MMSE, with a mean value of 27.3±1.3, but still significantly lower that the cognitively unimpaired group, who obtained a score of 29.2±1.1 (p < 0.001). It is noteworthy that only five subjects of the MCI group showed abnormal levels of amyloid-β, a similar percentage that in the cognitively unimpaired group (26.3%versus 20%, p = 0.72).
Incidence of PND and neuropsychological pattern
Participants were clinically followed up during the hospital stay after surgery to monitor the occurrence of delirium, which occurred in four cases (9%). The postoperative evaluation was only possible for two of these patients and, of these, one developed PND.
A postoperative neuropsychological assessment could be completed in 29 participants (65.9%). Although in the baseline visit all participants consented in taking a postoperative evaluation, 15 subjects did not agree to come back. Fourteen of them argued lack of interest and a fifteenth participant continued with important mobility problems in spite of his knee replacement. It was possible to contact all of them by a phone call and their medical histories were reviewed to confirm that there had not been major complications associated to their surgical interventions. The group of participants without an available postoperative evaluation did not show significant differences in their baseline characteristics from the group who underwent it, including age (74.1±7.6 years, p = 0.62), MMSE scores (28.4±1.2, p = 0.91). and percentage of participants with a CDR sob = 0.5 (46.7%, p = 0.76). Additionally, the group without a postoperative evaluation included 20%of subjects with abnormal levels of amyloid-β (3/15), which represents a non-significant lower percentage than the group of participants who agreed to come back, which was 24.1%(7/29, p = 1.00).
The postoperative assessment allowed to identify PND in 16 subjects (Cumulative Incidence = 55.2%) during a mean follow-up period of 264±28 days. There were no cases of incident dementia in this period. The most commonly affected domains in these individuals were constructional praxis (62.5%) and executive function (56.3%) (Fig. 1). The development of PND was not significantly associated with any of the baseline characteristics, although differences in basal MMSE were borderline significant (Table 2).
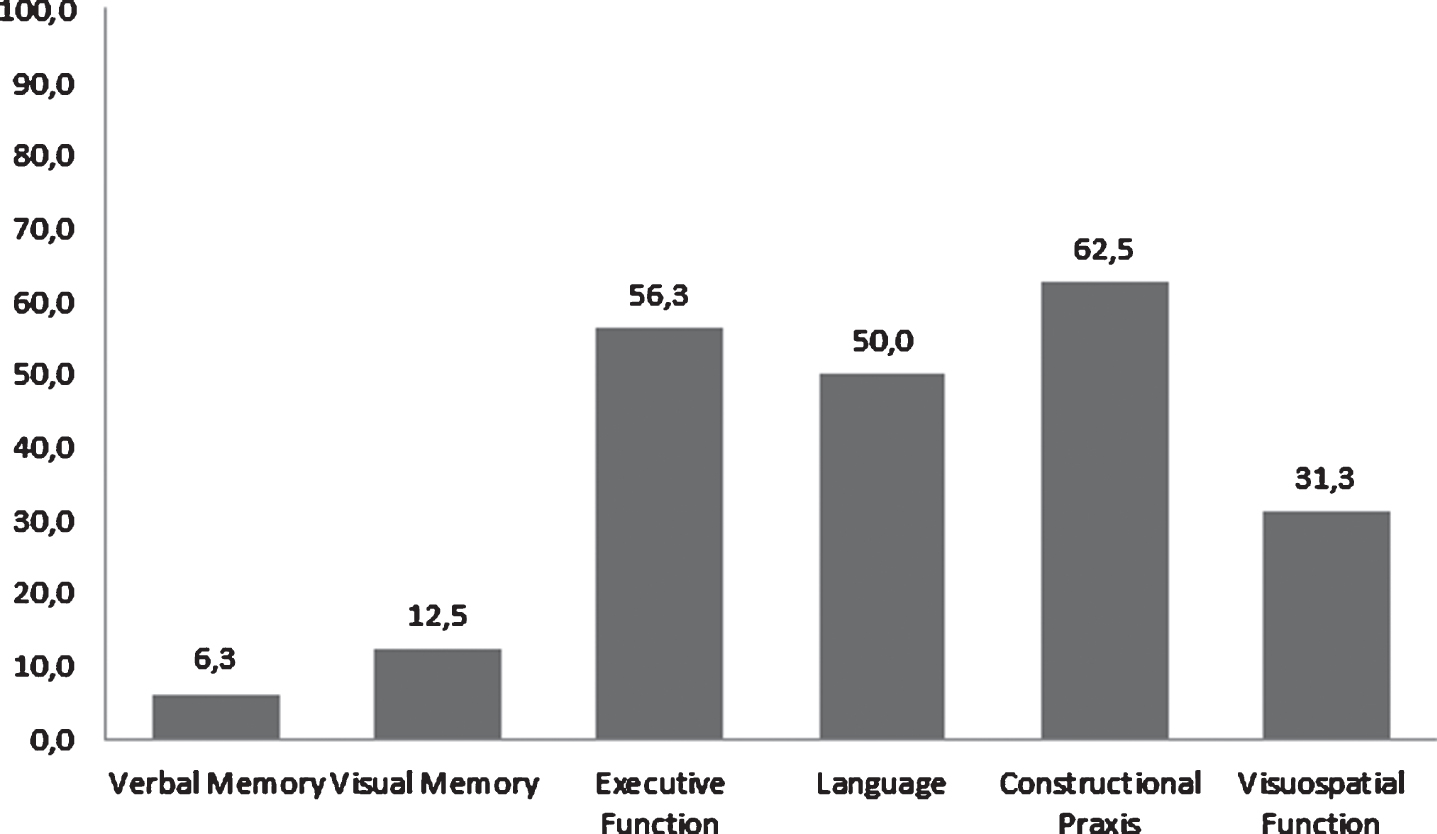
Percentage of PND subjects with significant impairment in each cognitive domain (SRB worsening≥2SD after surgery), including Verbal Memory (FCSRT), Visual Memory (RCFT Free Delayed Recall), Attention and Executive Function (Digit Span, TMTA and TMTB and Letter Fluency), Language (Semantic Fluency and Boston Naming Test), and Visuospatial Function (VOSP).
Characteristics of subgroups according to the development of PND
PND, postoperative neurocognitive disorder; SD, standard deviation; MMSE, Mini-Mental State Examination. Alzheimer’s Biomarkers status expresses the number and percentage of subjects who did or did not developed PND in each amyloid subgroup.
The postoperative assessment was compared with the preoperative results (Table 3). As expected, we observed an improvement in FCSRT scores due to a practice effect. Globally, the most impaired cognitive domain was executive function, since the performa-nce on the Digit Span was significantly worse than in the first examination, both in the Forward (p = 0.002) and in the Total subtests (p = 0.003), in that an average of one digit less could be repeated than in the pre-surgical assessment. Other non-amnestic domains were also significantly impaired, as CERAD Constructional Praxis, which decreased on average 0.89 points out of 11 (CI 0.21–1.57, p = 0.04).
Pre and postoperative neuropsychological performance in the global sample and in Amyloid-β - and Amyloid-β+ Groups
FCSRT, Free and Cued Selective Reminding Test; WMS-III LM, Weschler Memory Scale-III Logical Memory subtest; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; RCFT, Rey-Osterrieth Complex Figure Test; VOSP, Visual Object and Space Perception Battery; SE, standard Error. In bold, p < 0.05. *p-values adjusted by age and sex by Linear Mixed Models including the interaction between amyloid-β and time for the global sample; and, for amyloid-β + and –groups, including only age and sex as covariates.
AD biomarkers and PND
AD biomarker status was not significantly associated with PND. A + individuals tended to develop PND more frequently than A-, but this trend did not reach statistical significance (Table 2). Anecdotally, all individuals with SNAP developed a non-amnestic PND.
We tested the effect of amyloid-β status over time in the global sample (Table 3). A significant interaction was demonstrated for all the subitems of the WMS-III LM (p = 0.0086 for Total Delayed Recall), and also for the CERAD figure recall (p = 0.046). The interaction with amyloid-β was not significant in any of the other neuropsychological tests.
The comparison between pre- and postoperative evaluations in each group remarks these findings. The A- group presented a similar tendency as repor-ted for the global sample, with an improvement in most FCSRT subtests and the WMS-III LM, which in this subgroup reached statistical significance. Add-itionally, like in the global sample, A- subjects significantly worsened on the Digit Span test (Forward and Total subtests (p = 0.005 and p = 0.02 respectively), with Semantic Fluency (p = 0.04) also being impaired in this subsample. In contrast, the A + group showed a marked worsening after surgery on most memory results, mainly on the WMS-III LM, in several subtests like WMS-III LM Immediate Recall (p = 0.029), and therefore evolving in the opposite direction than A- (Table 3).
Cognitive performance was compared between the A- and A + groups at each time point of evaluation. At the preoperative assessment, A- subjects tended to show slightly higher scores in all memory tests than A+, but this did not reach statistical significance in any case. Similarly, in the rest of the neuropsychological testing no significant differences were found between groups. Nevertheless, at the postoperative evaluation, A + individuals performed significantly worse on most subitems of the WMS-III LM than A- participants, both for total immediate (Story B, p = 0.043) and delayed recall (Story B, p = 0.021) (Table 4).
Comparison of neuropsychological performance between Amyloid-β –and Amyloid-β+Groups
FCSRT, Free and Cued Selective Reminding Test; WMS-III LM, Weschler Memory Scale-III Logical Memory subtest; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; RCFT, Rey-Osterrieth Complex Figure Test; VOSP, Visual Object and Space Perception Battery; SE, standard error. In bold, p < 0.05. *p-values adjusted by age and sex by General Linear Models.
Results were tested for multiple comparisons, but no one of them survived to the corrected FDR-threshold.
DISCUSSION
There is compelling evidence that systemic inflammation plays a role in neurodegeneration. Amyloid plaques build up in the brain decades before cognitive symptoms appear, and several authors posit that these deposits might increase susceptibility to inflammatory-mediated neurodegeneration [30, 31]. Therefore, intense systemic inflammatory responses might have a larger impact on A + individuals. We aimed to investigate this hypothesis by testing the effect of amyloid-β on cognitive performance over time in a sample of subjects who underwent a major surgery. Significant interactions emerged for tests which assess verbal (WMS-III LM) and visual memory (CERAD figure recall), but not other cognitive functions, which supports our hypothesis that, in individuals with amyloid–β brain pathology, major surgery may trigger an amnestic cognitive decline, a clinical picture consistent with the earliest manifestations of AD.
More specifically, we observed that, according to the presence or absence of brain amyloid-β, surgery triggered different cognitive patterns. A + individuals developed a significant worsening in verbal memory tests and showed no significant practice effect, which was very prominent in the A- group, meaning that meanwhile the A- tended to improve in the second assessment, the A + individuals did not imp-rove significantly or even worsened after surgery. These changes in opposite directions led to the fact that, despite the neuropsychological performance of the A + group at baseline was indistinguishable from that of the A- group, after surgery we found statistically significant differences in several memory tests between both groups. On the other hand, in the A- group we can test the amyloid-β-independent effect of surgery, which may constitute a distinctive phenomenon. We found that these A- individuals followed a different cognitive trajectory, with a predominance of non-amnestic cognitive impairment after surgery. In this group, such decline cannot be attributed to Alzheimer's pathology and therefore points to an effect of surgery by itself, which might be related to neuroinflammatory or other unidentified factors. We can hypothesize that, in subjects with amyloid-β brain pathology, this phenomenon is probably combined and enhanced by the amyloid-β pathology-related neuroinflammation, resulting in a different clinical presentation than in A- subjects. This also could constitute a potential explanation of why some individuals—those without amyloid-β brain pathology—develop a PND that may remediate in the following months after surgery; whereas others, in preclinical AD stages, show a progressive course that eventually leads to dementia.
Studies addressing PND and including AD bio-markers are scarce, but most of them have observed a relationship between AD biomarkers and a worse cognitive trajectory. Evered et al. [11] evaluated 57 subjects who underwent an elective total hip replacement and found a higher incidence of PND at 3 months in the group of subjects with amyloid-β below the cut-off point (27.3%versus 4.3%, p = 0.01). Similar to our study, the greatest effects of low amyloid-β were demonstrated for the CERAD Auditory Verbal Learning Test, in addition to Semantic Fluency and Grooved Pegboard Test at 3 months postoperatively, and for TMTB and Controlled Oral Word Associated Test at 12 months postoperatively. Also, Wu et al. [13] described a significantly lower ratio of amyloid-β versus total tau in the group of subjects who developed PND at 3 months. Two additional studies of orthopedic surgery patients found a correlation between lower CSF amyloid-β/total-tau ratio and poorer results on verbal memory and visuospatial tests [32] and an association between low amyloid-β and high t-tau and lower cognitive performance [33], but both lacked control groups or normative values, so PND could not be evaluated. The only study to date using amyloid PET instead of CSF biomarkers to identify preclinical AD tracked the cognitive trajectory of cardiac surgical patients [34]. Even though they could not find an association between global cortical amyloid burden and PND, subjects with an abnormal amyloid deposition in the hippocampus showed a significantly greater decline in verbal memory tests, in a similar fashion as in our study. Interestingly, these subjects also showed a rate of amyloid deposition from 6 weeks to one year after surgery significantly greater than in other non-surgical published cohorts, as high as ten-fold that reported in scan-negative subjects, which raises the question of whether surgery may accelerate amyloid deposition in A + individuals.
In our analysis, we could not demonstrate a higher incidence of PND in A + subjects, as was expected initially. Current diagnostic recommendations state that score decrements after surgery should be considered in terms of z-scores, calculated preferably by means of normative data or control groups, and that a change larger than 2 SD at any test should be sufficient for PND diagnosis, but it is not specified which particular neuropsychological tests should be ordinarily applied. Our neuropsychological asse-ssment was very extensive, as one of our goals was to understand the cognitive pattern of this syndrome, which has not been clearly defined up until now. In our work, the diagnosis of PND was based on SRB, a standardized score which compares the change over time in a test performance in a specific subject to the expected change for general population. Therefore, the calculation of SRB is only possible for those tests normalized for the Spanish population. Even though several memory tests were part of our assessment (FCSRT and WMS-III LM), to calculate the SRB for the verbal memory domain we used only the FCSRT, the only one standardized for Spanish population [15]. FCSRT is a test based on a list of words and therefore it is susceptible to practice effect. Despite the fact that that we used SRB to account for it, we think that it likely explains an underestimation of PND cases due to memory. As Fig. 1 shows, only a minority of individuals were categorized as PND due to a memory worsening (≥2 SD SRB). Conversely, the WMS-III LM, which showed a significant association with the effect of amyloid-β over time and demonstrated the differentiation between A + and A- groups postoperatively, is not standardized for Spanish population and therefore could not be used for the calculation of PND incidence.
In the overall sample, the cognitive domains most commonly affected after surgery were executive fun-ction and constructional praxis. In the A- group, we found a similar non-amnestic-pattern, mainly with a significant impairment in Digit Span and Verbal Flue-ncy along with the previously mentioned improvem-ent in memory tests. Interestingly, a reverse pattern was observed in A + individuals. In this group, Digit Span and other tests tended to show a slight impairment that was not statistically significant, but a rema-rkable worsening was observed in the WMS-III LM and CERAD memory tests. According to our results, screening for PND should include a battery of tests assessing the main cognitive domains, especially exe-cutive functions and constructional praxis, and ideal-ly memory tests with low susceptibility to practice effects.
Our results must be interpreted with caution due to the small sample size and the limited statistical significance of some of the observed effects, which did not survive a correction for multiple comparisons. Therefore, our study must be considered predominantly as hypothesis-generating for future studies. A potential limitation is that the NEURONORMA reference norms of cognitive change used for the estimation of PND incidences are designed for one year of time interval between neuropsychological assessments, but in our work the mean interval was 264 days. However, in our case, this fact would bias towards the null, as we would be overestimating the rate of change of reference controls and consequently diminishing our power to detect changes in our study population, so we think that this point does not invalidate the observed differences. Furthermore, it could be considered that the observed memory impairment in A + subjects can be justified just by the presence of amyloid-β brain pathology alone. Regarding this, it should be noted that the great majority of A + subjects (9 out of 10) had normal values of total and p-tau, which is consistent to Alzheimer’s pathologic change (A + /T-/N-) according to the current diagnostic res-earch framework, and thus can be considered at the first stages of preclinical AD. Currently it is known that amyloid-β CSF levels are abnormal up to 20 years before the onset of symptoms, and even up to 10 years before p-tau levels are abnormal. The rate of memory decline in A + /T-/N- subjects has not been clearly defined in the literature, but it is generally regarded as a rather stationary condition until the mo-ment in which other less known mechanisms trigger neurodegenerative changes, including tau pathology, neuroinflammation, and ultimately neuronal damage. According to this, our sample of A + subjects are community-dwelling individuals who did not ref-erred cognitive complaints and showed a mean MMSE of 28.4. In this scenario, it is hard to expect the observed memory worsening in a timeframe of 6.5 months (the mean interval between neuropsychological assessments in A + subjects was 195 days), and the influence of a superimposed factor, in our case a major surgery, seems a more plausible explanation that the progression of pathology by itself. In this way, our findings would support the hypothesis that factors related to major surgical procedures might affect those individuals with brain amyloid-β pathology by promoting or accelerating neurodegenerative changes. However, larger samples with a longer period of follow-up to assess dementia conversion risk, as well as multimodal evaluations taking into account inflammatory and neurodegenerative components, are needed to disentangle the diverse and complex phenomena implicated in PND.
Footnotes
ACKNOWLEDGMENTS
We thank all volunteers for their generous contribution to this research. We thank Biobanco Valdecilla for their support.
Pascual Sánchez-Juan was supported by grants from IDIVAL, Instituto de Salud Carlos III (Fondo de Investigación Sanitario, PI08/0139, PI12/02288, PI16/01652), JPND (DEMTEST PI11/03028) and the CIBERNED program Acción Estratégica en Salud integrated in the Spanish National I + D+i Plan and financed by Instituto de Salud Carlos III (ISCIII) –Subdirección General de Evaluación and the Fondo Europeo de Desarrollo Regional (FEDER –Una Manera de Hacer Europa).