
Abstract
Background:
Recent work has supported use of blood-based biomarkers in detection of amnestic mild cognitive impairment (MCI). Inclusion of neuropsychological measures has shown promise in enhancing utility of biomarkers to detect disease.
Objective:
The present study sought to develop cognitive-biomarker profiles for detection of MCI.
Methods:
Data were analyzed on 463 participants (normal control n = 378; MCI n = 85) from HABLE. Random forest analyses determined proteomic profile of MCI. Separate linear regression analyses determined variance accounted for by select biomarkers per neuropsychological measure. When neuropsychological measure with the least shared variance was identified, it was then combined with select biomarkers to create a biomarker-cognitive profile.
Results:
The biomarker-cognitive profile was 90% accurate in detecting MCI. Among amnestic MCI cases, the detection accuracy of the biomarker-cognitive profile was 92% and increased to 94% with demographic variables.
Conclusion:
The biomarker-cognitive profile for MCI was highly accurate in its detection with use of only five biomarkers.
INTRODUCTION
In the Alzheimer’s disease (AD) field, blood-based biomarkers have been proposed as a cost- and time-effective mechanism for screening, diagnosis, and assessment of risk for disease progression [1, 2]. A number of studies have focused on the identification of biomarkers of mild cognitive impairment (MCI). Although it is unclear whether neurodegenerative processes trigger or are the subsequent result of activation of the immune system [3], inflammatory markers are among the most explored group of biomarkers for the detection of MCI. TNFα, a pro-inflammatory cytokine that exhibits both neuroprotective [4] as well as neurodegenerative properties [5], has been extensively studied. Several studies have linked increases in TNFα to the presence of both AD and MCI [6–8].
Other inflammatory biomarkers that have been related to MCI include IL-10, an anti-inflammatory cytokine that in animal models has resulted in increased amyloid-β accumulation [9]. I-309, a glycoprotein that belongs to a family of inflammatory cytokines, has been identified as one of the top six biomarkers correlated with severity of cognitive impairment (MCI/AD) [10]. In blood-based models, I-309 was found in both the proteomic profile for AD among Non-Hispanic Whites [7] as well as in the profile for amnestic MCI (aMCI) among Mexican Americans [11]. CRP levels have also been linked to MCI [12] although the direction and nature of the relationship is unclear [13, 14].
Additionally, a number of other blood-based biomarkers have shown promise in detecting MCI. Beta 2 Microglobulin (B2M), an immune protein that plays a role in distinguishing one’s own cells from that of invading pathogens [15], has been identified as being increased across several proteomic profiles for AD [6, 7] as well as aMCI in a sample of Mexican Americans [11]. Recent research has found that thrombopoietin (THPO), a glycoprotein that regulates platelet production, is the strongest predictor of clinical AD when compared to other blood-based biomarkers; however, this was ethnic specific and only found for Non-Hispanic Whites [16].
As shown above, the relationship between MCI and various biomarkers can be impacted by ethnicity. O’Bryant and colleagues have been successful in generating a serum-biomarker profile of AD among Mexican Americans [17]. The top markers within the serum-biomarker AD profile of Mexican Americans were found to be predominately metabolic in nature [17]. A proteomic profile for aMCI among Mexican Americans has also been identified [17]. The proteomic profile for aMCI was found to be more like the inflammatory-based profile identified among AD for Non-Hispanic Whites than that for Mexican Americans [6]. The overall biomarker profile was found to be 96% accurate in determining aMCI status among Mexican Americans with a sensitivity of 82% and specificity of 97% [11]. When demographic variables were included into the model, the level of accuracy remained at 96%; however, there was a noted increase in specificity to 99% [11].
Early work on the biomarkers of AD and MCI focused predominantly on biomarkers that demonstrated a significant overlap with the disease state. As neuropsychological assessments are commonly utilized as a means of identifying disease presence as well as severity, it was hypothesized that biomarkers related to AD/MCI would account for a significant amount of variance in neuropsychological measures commonly utilized to diagnose such disorders. This approach referred to as molecular neuropsychology sought to identify biomarker profiles of neurocognitive functioning [18]. Random forest analyses were utilized to create neuropsychological test-specific biomarker risk scores that were entered into linear regression models predicting the respective neuropsychological test scores. The biomarker risk scores alone were shown to account for a minimum of 12.9% to upwards of 47% of the variance in neuropsychological scores [18].
The early work using the molecular neuropsychology approach, focused exclusively on Non-Hispanic Whites. The first study examined IL7 and TNFα in combination with one measure of executive functioning (Clock-4 point), along with demographics obtained an overall detection accuracy for AD at 90% within the total sample [19]. When broken down by Clinical Dementia Rating (CDR) scale scores, those with a CDR = 0.5–1, were detected with an overall accuracy of 91% while those with a CDR = 0.5 were detected with a comparable accuracy rate (AUC = 0.91) [19]. This work was able to create a biomarker-cognitive profile of early and very early AD cases, which yielded a high accuracy.
Subsequent research using the molecular neuropsychology approach refined the methodology and included the top five molecular markers (IL5, IL6, IL7, TNFα, and CRP) from a previously developed algorithm for AD [6] along with one neuropsychological measure, identified as having the least amount of variance overlap with the select biomarkers. This study found that the highest variance accounted for was related to measures of immediate and delayed memory [11], whereas measures of attention, language, and executive function demonstrated substantially lower shared variance with the selected biomarkers. The Controlled Oral Word Association (COWAT) displayed the lowest amount of variance overlap (5%) and was selected for inclusion in the model [19]. When combined with the five selected biomarkers and demographic variables, the COWAT added to the diagnostic accuracy and correctly classified 91% with a sensitivity and specificity of 90% and 92%, respectively [19].
Prior work has been successful in demonstrating that blood-based biomarkers can be combined with select neuropsychological tests to accurately detect early and even very early forms of AD using the molecular neuropsychology approach [19, 20]. The current study extends this line of work towards the detection of MCI, specifically among Mexican Americans. This study seeks to 1) generate an overall proteomic profile for MCI, 2) evaluate overlap between select proteins and neuropsychological measures, and 3) generate cognitive-biomarker profiles for the detection of MCI.
METHODS
Participants
Data were analyzed on 463 participants age 50 and above with and without cognitive impairment (normal control n = 378; MCI n = 85). The current project leverages a community-based protocol the Health and Aging Brain among Latino Elders (HABLE), an ongoing epidemiological study of cognitive aging among Mexican Americans. Recruitment for HABLE is based on a community-based participatory research (CBPR) approach. The CBPR approach has been shown to hold comparable recruitment samples to that of the community at large [21]. CBPR involves both traditional means of recruitment (i.e., distribution of flyers, mail-outs) as well as partnering with local communities through community presentations, engagement with community recruiters (promotoras), and contact with social groups in the community. HABLE has an IRB approved protocol with each eligible participant (and/or informants for cognitively impaired individuals) providing written informed consent.
Participant screening
As part of the HABLE protocol, all participants undergo a comprehensive medical examination as part of an annual primary care visit. The annual exam includes a medical exam (including a neurological examination), clinical labs, review of current medications, and medical diagnoses. Each participant also undergoes a clinical interview (consent, inclusion/exclusion, and informant report), neuropsychological testing, and a venipuncture for biobanking purposes. Research diagnoses are determined through a consensus panel, which is made up of two licensed clinical neuropsychologists, a nurse practitioner, and community health workers. Consensus diagnosis is based on the NINCDS-ADRDA criteria [22] for AD and Mayo criteria for MCI [23]. Cognitively normal individuals are those determined to have performed within normal limits on neuropsychological assessments.
The neuropsychological assessment includes measures of global cognitive functioning/status (Clinical Dementia Rating Scale [24]), attention (Digit Span [25] and Trail Making Test Part A [TMTA] [26]), executive function (Trail Making Test Part B [TMTB] [26] and Clock Drawing [27]), memory (Wechsler Memory Scale Logical Memory I [LMI], Logical Memory II [LMII], Visual Reproduction I [VRI], Visual Reproduction II [VRII] [25]), language (Boston Naming Test [BNT] [28], animal naming and FAS Verbal Fluency [COWAT] [29]), premorbid IQ (American National Adult Reading Test [AMNART] [30]), depression (Geriatric Depression Scale [31], Neuropsychiatric Inventory-Questionnaire [32]), and daily function (Independent Activities of Daily Living scale [33]). Our research team has generated norms for English- and Spanish-speaking Mexican Americans on these tests [2].
Serum collection procedures
Serum samples are collected according to the recently established guidelines by the international working group [34] as follows: 1) fasting blood collected using 21 g needle, 2) sample tubes collected in the following order: blood culture tube, coagulation tube, serum, heparin, plasma EDTA tube, 3a) serum tube will be allowed clot for 30 min at room temperature in a vertical position, 3b) plasma tubes gently inverted 5–10 times, 4) the tube will be centrifuged with horizontal rotor for 10 min at 2000×g within 1 h of collection, 5) 1.0 mL aliquots of serum will be transferred into polypropylene (cryovial) tubes, 6) sample ID (Freezerworks™ barcode labels) will be firmly affixed to each aliquot, and 7) samples will be placed into –80°C freezer within 2 h of collection for storage until assay completion.
Assays
Serum samples were assayed in duplicate via a multi-plex biomarker assay platform using electrochemiluminescence (ECL) through a SECTOR Imager 2400A from Meso Scale Discovery (MSD; http://www.mesoscale.com). The MSD platform has been utilized extensively to assay biomarkers associated with a range of human diseases including AD [35–38]. ECL technology uses labels that emit light when electrochemically stimulated, which improves the sensitivity of detection of many analytes even at very low concentrations. ECL measures have well-established properties of being more sensitive and requiring less volume than conventional ELISAs [37]. Twelve MSD plates were run with the following proteins: Fatty acid binding protein (FABP), B2M, pancreatic polypeptide (PPY), CRP, sICAM1, sVCAM1, thrombopoeitin, α2 macroglobulin (A2M), exotaxin 3, TNFα, tenascin C (TNC), interleukin (IL)-5, IL6, IL7, IL10, IL18, TARC, SAA, IL1β, I309, and Factor VII. The biomarkers were selected due to previous work linking them with AD among Mexican Americans [11, 17]. Of note, the select blood-based biomarkers did not require age-adjustment given the analytic approach through machine learning techniques. Internal QC protocols are implemented in addition to manufacturing protocols including assaying consistent controls across batches, analysis of impact of protocol variability (e.g., freeze thaw cycles), and assay of pooled standards across lots.
Data analysis
Analyses were performed using R statistical software. Analyses took place in a series of steps. First to determine the difference in demographic characteristics between MCI and cognitively normal participants, one-way ANOVAs were conducted to examine group differences for categorical (gender) and continuous variables (age, education, and biomarkers). Next, the sample was randomly assigned into a training and test set, with 50% of the total 85 MCI cases (n = 48) placed into the training set along with 194 (50%) of the cognitively normal control cases. The remaining 50% of the sample were placed into the test set for purposes of providing validation for the model.
A random forest analysis was conducted to examine the proteomic profile of MCI. The top five biomarkers determined by this analysis were then utilized within future random forest models. Next, the amount of explained variance between the individual neuropsychological measures and the top five biomarkers identified within the proteomic profile for MCI was evaluated through separate linear regression models. Specifically, the separate linear regression models were conducted within the training set utilizing the top five markers as the dependent variables with each individual neuropsychological measure (memory [WMS-III Logical Memory I and II; WMS-III Visual Reproduction I and II], language [COWAT, BNT], and executive functioning [TMTB]) as the independent variable. These analyses determined the amount of explained variance by the top biomarkers for each of the individual neuropsychological measures. The purpose was to identify the neuropsychological measure with the least amount of variance overlap with the biomarkers and to then utilize that specific measure in combination with the select biomarkers to establish a cognitive-biomarker profile for predicting MCI.
Once the neuropsychological measure was identified, additional random forest analyses were conducted within the training set to examine the predictive ability of the top five biomarkers and the one identified neuropsychological measure in the detection of MCI. The same combined biomarker-cognitive algorithm was then applied to the test set for purposes of validating the model. Supplementary random forest analyses were conducted with the training set wherein demographic variables (age, gender, and education) were also included to create a biomarker-cognitive-demographic model to examine if this further enhanced the detection accuracy of the model. As with the initial biomarker-cognitive model, the combined algorithm for the biomarker-cognitive-demographic model was then applied to the test set for validation. Variable importance was determined based on mean decrease in accuracy, which is defined as the decline in model accuracy due to randomization of that variable. A higher mean decrease in accuracy therefore reflects the higher the importance of that variable within the model.
RESULTS
The demographic characteristics and neuropsychological test performance for the MCI and the cognitively normal control group of the HABLE sample can be found in Table 1. Descriptive data of the twenty-one biomarkers across the two diagnostic groups can be found in Table 2. MCI cases were identified as being significantly older (p < 0.001), having fewer years of education (p < 0.001), and as predominantly female (p = 0.001). Significant differences were found between the MCI group and the normal controls for six of the biomarkers. The MCI group had higher levels of A2M (p = 0.03), B2M (p < 0.001), FABP (p < 0.001), IL10 (p = 0.001), IL6 (p = 0.002), and TNFα (p < 0.001) as compared to normal cognitive control cases.
Demographic Characteristics and Neuropsychological Test Performance of Mild Cognitive Impairment and Cognitively Normal Control Groups
CDR, Clinical Dementia Rating Scale; COWAT, Controlled Oral Word Association Task.
Descriptive Data for Twenty-one Proteins Examined across MCI and Cognitively Normal Control Cases
Platform: ELISA, Enzyme-linked immunosorbent assay. Assay: A2M, Alpha 2-macroglobulin; B2M, Beta 2-macroglobulin; CRP, C-reactive protein; FABP, Fatty Acid Binding Protein; FVII, Factor VII; IL10, Interleukin 10; IL18, Interleukin 18; IL1 β, Interleukin 1beta; IL5, Interluekin 5; IL6, Interleukin 6; IL7, Interleukin 7; PPY, Pancreatic Polypeptide; SAA, Serum amyloid A; sICAM1, soluble intercellular adhesion molecule-1; sVCAM1, soluble vascular cell adhesion molecule-1; TNC, Tenascin c; TNFα, Tumor necrosis factor alpha.
The proteomic profile of MCI was determined through random forest analyses within the training set. Across the total twenty-one biomarkers examined, the top five biomarkers identified within the Gini Plot among Mexican Americans with MCI were TNFα, IL10, I309, Thrombopoietin, and B2M (Fig. 1). As shown in Fig. 2, the overall accuracy (area under the curve [AUC]) of the biomarkers in the detection of MCI compared to cognitively normal control cases was 82% (SN = 0.98 [95% CI: 0.95–0.99]; SP = 0.46 [95% CI: 0.32–0.61]).
Results from the separate linear regression models evaluating explained variance of the top five biomarkers for each of the neuropsychological measures examined found variability across cognitive domains. Specifically, explained variance was greatest for a measure of language (i.e., naming) accounting for upwards of five percent. Across memory-based measures, explained variance ranged from two to four percent. Within the domain of executive functioning, the set shifting measure selected (TMT B) accounted for only one percent, which was the lowest explained variance across cognitive measures evaluated. TMT B requires participants to engage in a complex attention task wherein they shift between sets of information [39]. Because TMT B was found to have the least amount of variance overlap with the top five biomarkers, it was selected for further analysis. This was done to maximize the strengths of the approach by minimizing overlap.
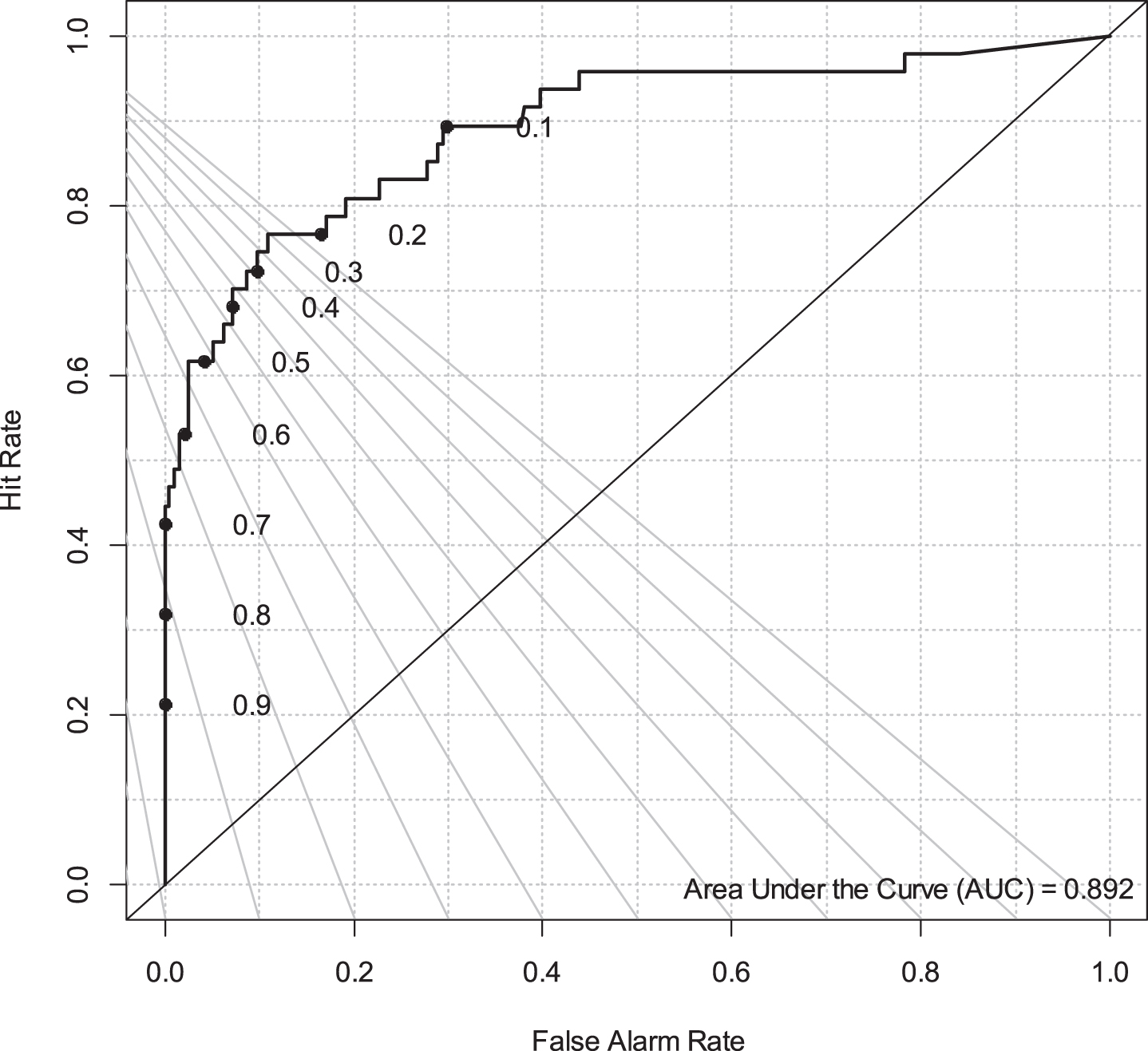
When the top five biomarkers were combined with one neuropsychological measure, TMT B, to create a biomarker-cognitive profile, the overall accuracy level (AUC) of the training set in determining MCI from cognitively normal control cases was 90% (SN = 0.95 [95% CI: 0.91–0.97]; SP = 0.617 [95% CI: 0.46–0.75]) (Fig. 3). When applied to the test set, the area under the curve increased to 94% (Fig. 4). When demographic variables (age, gender, education) were included within the initial training set along with the top five biomarkers and TMT B, the overall detection accuracy remained at 90% (SN = 0.96 [95% CI: 0.92–0.98]; SP = 0.59 [95% CI:0.44–0.73]) (Fig. 5). When the same biomarker-cognitive profile that included demographics was applied to the test set, the area under the curve increased to 96% (Fig. 6). The model consisting of the top five biomarkers, demographics, and TMT B showed that TNFα contributed the most importance to the classification, closely followed by age and IL10 with education shown to contribute the least (Fig. 7).

Gini plot for top twenty-one biomarkers for the detection of MCI.

The overall accuracy (area under the curve) of the twenty-one biomarkers in determining MCI.
The overall accuracy (area under the curve) of the top five biomarkers and TMT B in determining MCI in the training set.

The overall accuracy (area under the curve) of the top five biomarkers and TMT B in determining MCI in the test set.

The overall accuracy (area under the curve) of the top five biomarkers, demographics, and TMT B in determining MCI in the training set.

The overall accuracy (area under the curve) of the top five biomarkers, demographics, and TMT B in determining MCI in the test set.

Mean decrease accuracy of the top five biomarkers, demographics, and TMT B in the training set.
In order to place the current findings into the context of clinical diagnostic predictions, positive (PPP) and negative (NPP) predictive power were calculated. PPP and NPP were calculated based on Baye’s theorem as previously described [40] utilizing an estimated base rate for MCI of 20% within a community-based population. This reflects the likelihood that a clinician would be correct (PPP) or incorrect (NPP) in classifying a Mexican American as having MCI based on the current findings. Assuming a 20% base rate, PPP = 0.387 and NPP = 0.98 based on the sensitivity and specificity estimates outlined above.
DISCUSSION
This study was the first to examine the molecular neuropsychology approach among Mexican Americans. An executive functioning measure, TMT B, was identified among this sample as having the lowest amount of explained variance by the identified biomarkers (TNFα, IL10, B2M, Thrombopoietin, and I309). This finding differed from that of our prior work that identified the COWAT as having the lowest variance explained among a sample of Non-Hispanic Whites with AD [19]. This discrepancy in findings reflects the presence of both diagnostic and sample differences that lend further support for the need to examine ethnic differences. This study also was able to refine the number of biomarkers necessary for distinguishing diagnostic categories from twenty-one down to five biomarkers. The results showed that for distinguishing MCI cases from cognitively normal controls, the addition of demographics did not significantly change the detection accuracy of the biomarker-cognitive profile.
The highly accurate biomarker profile was composed of biomarkers (TNFα, IL10, I309, and B2M) related primarily to inflammatory processes. The biomarkers were varied in their inflammatory role as both pro- and anti-inflammatory proteins were identified. Additionally, several glycoproteins related to inflammatory cytokines were found among the top biomarkers for MCI suggesting the impact of extensive and interrelated inflammatory processes. These findings are consistent with our recent work that identified the biomarker profile of aMCI among Mexican Americans and found similar elevations in biomarkers of TNFα and IL10 [11]. Additionally, our prior work has linked many of the same proteins identified in the overall proteomic profile for MCI to specific cognitive domains. For example, TNFα and Thrombopoietin have previously been linked to the domains of memory and executive functioning [18] and IL10, Thrombopoietin, and TNFα linked to the domain of attention [18]. As impairment across the areas of memory, executive functioning, and attention are frequently observed among MCI cases, it very likely represents a specific biological profile for this particular diagnostic category.
Within the final model consisting of the top five biomarkers, demographics, and TMT B, the top three contributing variables to the diagnostic classification were TNFα, followed by age and IL10. The relative importance of these variables is consistent with prior literature linking increased TNFα with AD and MCI [6–8]. As expected, age was also a highly important variable to the model. It is well-known that advancing age is the greatest risk factor for AD. However, our results indicate that certain biomarkers, such as TNFα may also reflect underlying mechanisms of neurodegeneration. TNFα tends to increase with age [41], and therefore the interaction between these two factors may represent an important focus for future studies. Of note, the results further showed that although education level was different between diagnostic groups, education itself, when included into the classification model, was only minimally significant in predicting diagnostic state when compared to all other variables included within the model.
Our work has supported the use of profiles, either biomarker or cognitive-biomarker profiles in the detection of AD and MCI [6, 42]. Others have also sought to identify single biomarkers of disease state; however, the results have been inconsistent particularly among MCI. A recent analysis revealed that both fraction (serum versus plasma) as well as platform can significantly impact how a biomarker presents within a disorder [43]. The use of a compilation of biomarkers allows for biological variability within a disorder to be accounted for. This can be particularly important for heterogeneous diagnostic categories such as MCI, which does not always reflect a linear disease progression such that it does not always serve as a prodromal stage for AD. Therefore, allowing for multiple biomarkers within a diagnostic model may better reflect biological changes at different disease stages particularly early on in the disease. In support of this, differences between previously derived proteomic models for Hispanic, Mexican Americans with AD versus aMCI reflect different combinations of biomarkers [11, 17]. Within the current study, a mixture of biomarkers of inflammation and metabolic processes were identified within the final MCI cognitive-biomarker model. Future work should continue to evaluate and refine proteomics selected specifically for the detection of MCI.
Initial work utilizing the molecular neuropsychology approach to predict AD was conducted among a sample of Non-Hispanic Whites utilizing a different analytic platform (Rules Based Medicine) [20]. Research efforts have shown that differences in analytic platform can impact protein expression [43], which has a downstream impact on proteomic selection for disease modeling. It is therefore difficult to compare prior efforts utilizing the molecular neuropsychology approach with current results as differences in sample demographics and analytic platform inhibit a direct comparison. Differences in both sample and platform likely contributed to differences in results found across studies. Despite limitations in allowing for direct comparisons, similar methodological approaches showed improvement upon inclusion of demographic and neuropsychological measures, thus providing increased support for implementation of the molecular neuropsychology approach. Research efforts are currently underway to analyze the same proteomic biomarkers as well as neuropsychology tests utilized within the current study on n = 1000 Hispanic, Mexican Americans and n = 1000 Non-Hispanic Whites for purposes of cross-validation. As Mexican Americans are among the fastest growing segment of the aging population, their base rate estimates of disorders such as MCI are expected to steadily increase. The development of a screening test that can be readily implemented within a community primary care setting holds substantial impact particularly among this population as they have been previously shown to present more frequently to primary care settings and less frequently to specialty care clinics [44]. Additionally, prior work has shown that Mexican Americans present with MCI at younger ages, therefore a brief screening test such as the one utilized in this study requiring less than 5 min to conduct within a primary care setting would enable for continued follow-up for purposes of identifying early cognitive changes thus allowing for targeted treatment to be implemented in a timely and proactive manner.
Although this study examined only one time point, future work should examine longitudinal data to see if the derived biomarker-cognitive profiles change over time as individuals convert from MCI to AD. Additionally, follow-up studies should explore what impact (if any) common medical conditions have on the derived biomarker-cognitive profiles as this has considerable treatment implications for practitioners. It will be particularly important that future work focus on medical conditions such as cardiovascular disease, which is among the top leading causes of mortality among Hispanics in the United States [45]. Ongoing efforts are being undertaken to collect brain neuroimaging in order to start evaluating the direct and indirect effect that vascular factors have on cognition among Hispanic, Mexican Americans. Age is an addition risk factor for both cardiovascular as well as neurodegenerative diseases and was utilized as a covariate in the derived biomarker-cognitive profiles as has been done in our prior work [6, 20]. Future work should further explore the relationship between age and inflammation and how those risk factors individually and in combination may contribute to disease processes.
A limitation to this study is the use of TMT B in both the initial diagnostic criteria for MCI and then later within the biomarker-cognitive profiles. Although TMT B was utilized as part of a larger consensus review process for diagnosis in combination with all other neuropsychological measures, its use in the combined profile did result in overlap of the diagnostic criteria, despite its limited variance shared with the biomarkers. Future work should consider addressing this overlap in neuropsychological measures through the use of separate neuropsychological measures for the initial diagnosis and for the derived profile models. Another limitation is the refined number of biomarkers utilized within the diagnostic models as this might limit the obtained sensitivity and specificity. The five biomarkers included in this study for further analyses were selected based on their high variable importance (Mean Decrease in Gini >2) for the diagnostic model of MCI. Of note, the remaining 16 biomarkers, although important to the overall diagnostic model, produced comparable and notably lower variable importance (Mean Decrease in Gini <2) and were excluded from further analyses (Fig. 1). Other biomarkers identified among MCI cases should be further considered along with common markers related to neurodegeneration including tau, neurofilament light, and amyloid-β.
The molecular neuropsychology approach utilized in this study has shown utility in both aMCI and AD, which lends support for its application among cases of prodromal AD (i.e., MCI cases who are also amyloid positive). An ongoing study focused on the detection of AD within primary care (Alzheimer’s Disease in Primary Care study) is currently collecting data, which will allow for application of this approach to be evaluated among this diagnostic group who are more likely to convert to dementia due to AD. The 2015 Gerontological Society of America workgroup reported that “older adults are inadequately assessed for cognitive impairment during routine visits with their primary care providers” [46] despite recommendations set by the Centers for Medicare and Medicaid Services, which requires that primary care providers conduct a cognitive exam as a part of their annual visit. Due to a number of reasons including the volume of patients seen and time constraints, there is an urgent need for cost effective and rapidly scalable screening tools for AD particularly in primary care settings. Having a screening tool such as the one proposed in this study (biomarker-cognitive profile) would allow diagnostics to be streamlined where those who screen positive could be referred to a specialty clinic. This same model has been successfully implemented in other areas such as cancer and cardiovascular disease where primary care physicians are able to pre-screen for follow-up treatment.
Footnotes
ACKNOWLEDGMENTS
Research reported here was supported by the National Institute on Aging of the National Institutes of Health under award number R01AG054073. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The research team also thanks the local Fort Worth community and participants of the Health & Aging Brain Study.