
Abstract
This study surveys the development of Alzheimer’s disease (AD) in the research literature, the scientific community, and the journals containing AD papers over a 35-year period. Research papers on AD published from 1983 to 2017 in journals indexed in the Web of Science were analyzed in seven five-year periods. The number of AD papers increased from 1,095 in 1983–1987 to 50,532 by 2013–2017 and in the same time period, the number of participating countries went from 27 to 152. The US was the most prolific country throughout, followed by several European countries, Canada, Australia, and Japan. Asian countries have emerged and by 2013–2017, China surpassed all but the US in productivity. Countries in Latin America and Africa have also contributed to AD research. Additionally, several new non-governmental institutions (e.g., ADNI, ADI) have emerged and now play a key role in the fight against AD. Likewise the AD scientific publishing universe evolved in various aspects: an increase in number of journals containing AD papers (227 journals in 1983–1987 to 3,257 in 2013–2017); appearance of several AD-focused journals, e.g., Alzheimer’s & Dementia, Journal of Alzheimer’s Disease; and the development of special issues dedicated to AD. Our paper complements the numerous extant papers on theoretical and clinical aspects of AD and provides a description of the research landscape of the countries and journals contributing papers related to AD.
Keywords
INTRODUCTION
Whatever source of information is used by researchers, clinicians, politicians, the government, or the general public; whatever media is employed to broadcast this information; wherever it originates in the world; and whatever population size is involved, the findings and future prospects are the same: Alzheimer’s disease (AD) is a major scientific challenge and an expanding public health crisis that will continue to increase with the growing and aging population [1, 2].
While scientific activity and public awareness of AD was limited during the first half of the 20th century, a surge of interest among scientists and the public at large began in earnest in the 1970s. The combination of scientific research, technological advancements, and political will has led to the progressive understanding of the mechanisms of AD followed by improvements in diagnosis and treatment. Scientific and clinical knowledge about AD is regularly explicated, condensed, and sometimes simplified in books [3] and review papers [2 , 5].
Recently, bibliometric and scientometric studies have quantified and analyzed the AD research literature: Ansari and others [6] described various parameters of the AD literature for two years from Index Medicus; Sorensen [7] provided an interesting analysis of the top-100 investigators in AD research from 1985–2008 using productivity, h-index, and citation index; Sorensen and his colleagues [8] used co-authorship and co-MESH term analyses to bridge “bench” (scientific discoveries) and “bedside” (clinical investigations) components to benefit patients through clinical trials; cholinesterase inhibitors in research publications were used to find overall trends in the AD scientific literature published between 1993 and 2012 [9]; using a concept graph-based network analysis, Song and others [10] applied three analytical techniques to the AD research literature—productivity, network, and content; Lee and others [11] mapped the AD research literature using “entitymetrics” to provide perspectives of indexers, authors, and citers; Serrano-Pozo and others [12] provided a detailed examination of trends in the AD research literature including publication and patent output, funding, impact, and topics; and more recently, Chinese medical researchers [13] reviewed 30 years of the AD literature with special attention to China’s contribution to basic AD research.
The objective of this paper is to survey the last 35 years (1983–2017) of AD research using the Science Citation Index Expanded (SCI-E) so as to extend the landscape of the AD research literature. The following approaches were undertaken: a geographic overview of the development of AD research based on scientific papers; a brief description of several international non-governmental institutions dedicated to the research investigation and management of AD; and a bibliometric description of the scientific journals publishing research on AD. We hope that it will provide an informative view of the evolution and structure of research on AD, useful to scientific and medical researchers, clinicians, decision makers and funding organizations.
METHODS
Publications on AD for 35 years were collected in November 2018 from the SCI-E of the Web of Science (WoS). All publications designated as “articles” with “Alzheimer*” in their titles, abstracts, or keywords (where the asterisk retrieves “Alzheimer” and all extended variants) and published from 1983 to 2017 were considered for analysis.
Articles retrieved were then analyzed in seven five-year periods from 1983–1987 to 2013–2017. The following aspects were considered: the number of articles authored by researchers in each country—articles issued from more than one country were assigned equally to each contributing country; the top-10 most prolific journals for which Impact Factors (IFs) for 2017 were collected through the Thomson Scientific Journal Citation Reports. Articles originating from England, Scotland, Wales, and Northern Ireland were assigned to the United Kingdom (UK), and the European Union (EU) were the official member States (Countries) registered during each of the seven five-year periods. “Articles” and “papers” are used interchangeably throughout.
Limitations
In all bibliometric studies of medicine and biology based on the scientific literature, the results depend on the choice of database(s) and the search parameters used. We chose the SCI-E of the WoS for several reasons: it is an historical database and includes papers from 1900 to the present; it contains the major scientific and medical publications (primarily in journals) used by researchers for informing themselves and disseminating their research results; it is the database generally chosen by information scientists for bibliometric analysis of studies spanning many decades; and we are well-versed in the use of the database. We decided to consider papers earmarked as “articles” with the keyword “Alzheimer*” in their titles, abstracts, and (generally) author-provided keywords so that mainly original research papers on AD will be retrieved. Such limitations undoubtedly underestimate the number of publications on AD; however, we are confident that we have retrieved the bulk of the most relevant research and clinical literature on AD from 1983 to 2017. Despite the increasing use of bibliometric indicators other than productivity (e.g., citation analysis) in research evaluation at the level of researchers, research groups, departments, or institutions [14], we decided to focus primarily on AD research productivity of countries (incorporating all levels) and journals publishing AD-related research papers. Furthermore, citation analysis would require the relationship of each paper’s citations vis-à-vis citations from all other AD papers, with the added complexity of papers with multiple authors (with multiple motivation for citing) from various countries [15]; such bibliometric analysis is beyond the scope of this study.
Though AD is the most common cause of dementia in older adults, there are many other causes of dementia. Including the term “dementia” retrieved nearly 20% more publications (not already within our AD literature); however, of these additional “dementia” publications, many may not be relevant to AD. We therefore elected to confine our search to only dementia related to AD and AD in broader context. Additionally, although the revival of interest in AD research dates to the early 1960s with: the first meeting on AD organized by Sir Martin Roth in the UK in 1961; the first NIH grant on AD awarded to Robert Terry in 1961; and the first seminal papers on the electron microscopy of Alzheimer cytopathology by Robert Terry [16] and Michael Kidd [17], a search from 1961+ yielded very few papers early on, single digits in the 1960s and double digits in the 1970s. Not until 1983 did we get into triple digits (100+), hence the decision to look at the literature of AD from 1983–2017 (c. 35 years).
RESULTS AND DISCUSSION
As the bibliometric results below will show, the landscape of the scientific publishing community working on AD has developed and expanded greatly over the last 35 years (1983–2017) in several directions: output of articles in (mostly) journal publications; growth of journals in which the articles are distributed; increasing number of countries contributing and collaborating in AD research; and development of supranational organization dedicated to the management of AD. The discussion following the results is divided into: major contributing countries or geographical areas; international and national institutions supporting AD; specialized, generalized, multidisciplinary, and “predatory” journals containing AD papers; and broad subject categories or classifications in which AD research papers appear in the WoS database. Figures show comparative growth of papers (Fig. 1) and journals (Fig. 3) for Alzheimer, Parkinson, Cancer, HIV, and the total WoS database; Figure 2 compares growth in Alzheimer and Parkinson papers broadly classified (categorized) in Clinical Neurology, Neurosciences, or both. Figure 4 provides a ‘qualitative’ view of the ‘journal-universe’ of AD research papers in the WoS database in 1983–1987 and 2013–2017. Tables present publication outputs by countries for seven five-year periods from 1983–2017 (Table 1), and for the top-20 countries for papers in 2017, viz. life expectancy, population, and GDP per capita (Table 2). The top-10 most productive journals on AD are listed along with their assigned WoS categories, and for 2017, the journal IFs and rankings in the WoS categories (Table 3). Table 4 lists journals focusing on AD.
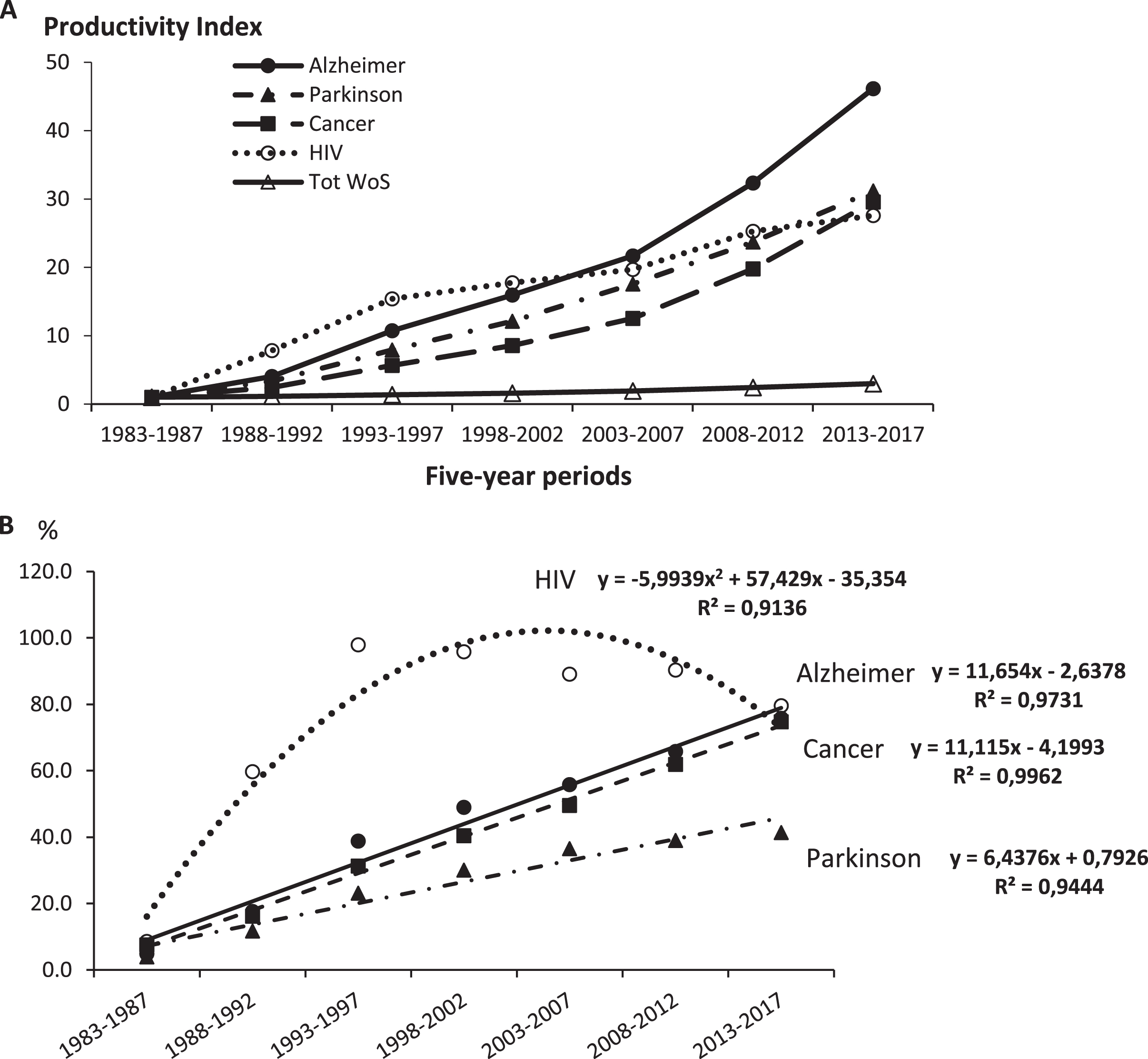
Growth of papers on Alzheimer, Parkinson, Cancer, and HIV in the WoS database from 1983–2017. A) Time course of papers on Alzheimer, Parkinson, Cancer, and HIV during 1983–2017 in the WoS database. Productivity index = number of papers on Alzheimer, Parkinson, Cancer, and HIV during each 5-year period/number of papers during the first five-year period. The number of papers on AD (Parkinson; Cancer; HIV) = 1,095 (885; 16,834; 1,924) for 1983–1987; 17,449 (10,711; 144,045; 34,155) for 1998–2002 and 50,532 (27,594; 498,058; 53,059) for 2013–2017. B) Spreading of publications on Alzheimer, Parkinson, Cancer, and HIV within the WoS database expressed as the ratio of the # of papers/the total WoS papers (*10000, except for Cancer,*1000).
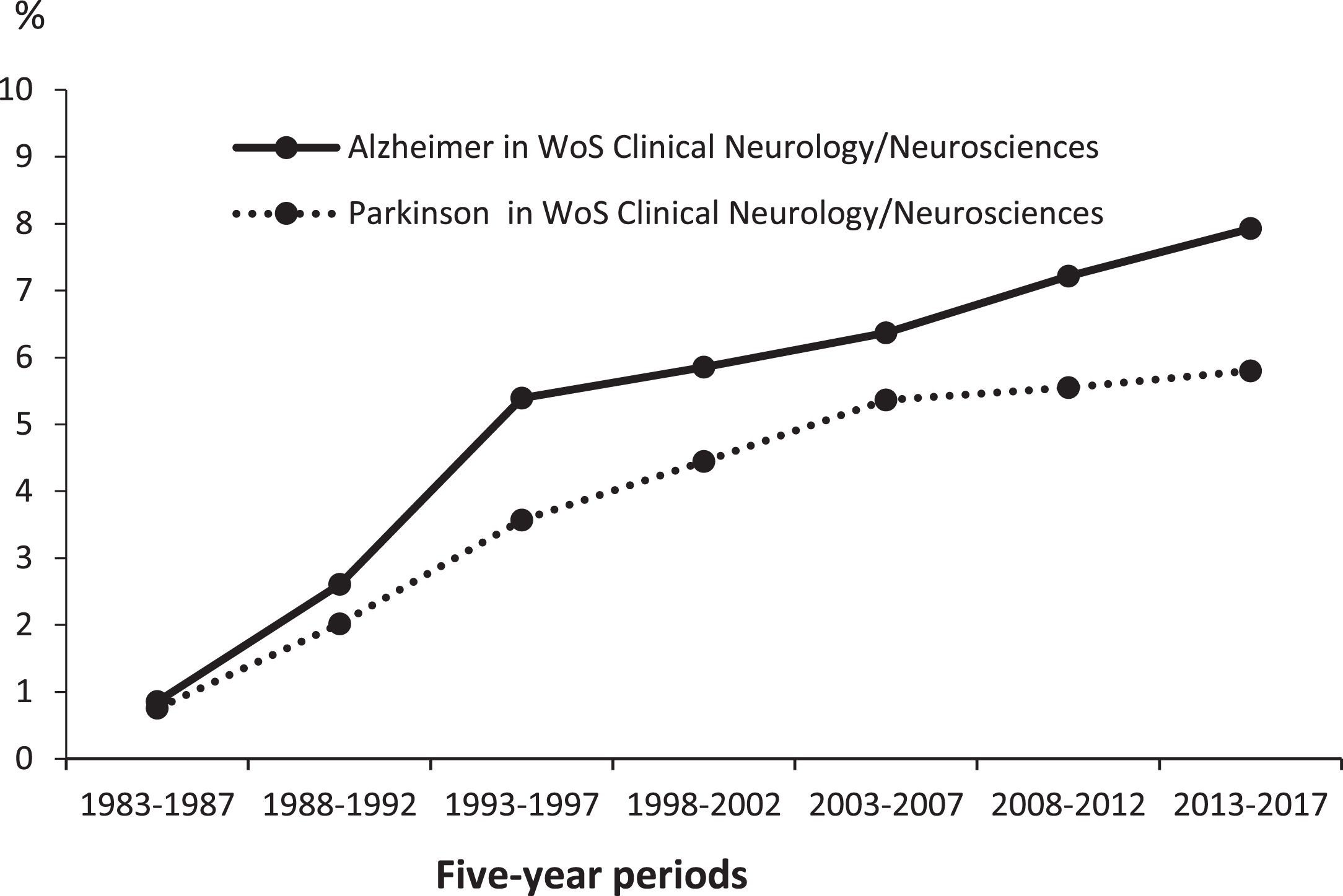
Percentage growth of papers in Alzheimer and Parkinson in the WoS database for Clinical Neurology/Neurosciences categories from 1983–2017. The number of papers on AD and Parkinson in the WoS database on Clinical Neurology/Neurosciences Categories = 620 and 548 for 1983–1987; 9,774 and 7,418 for 1998–2002; and 19,887 and 14,556 for 2013–2017.
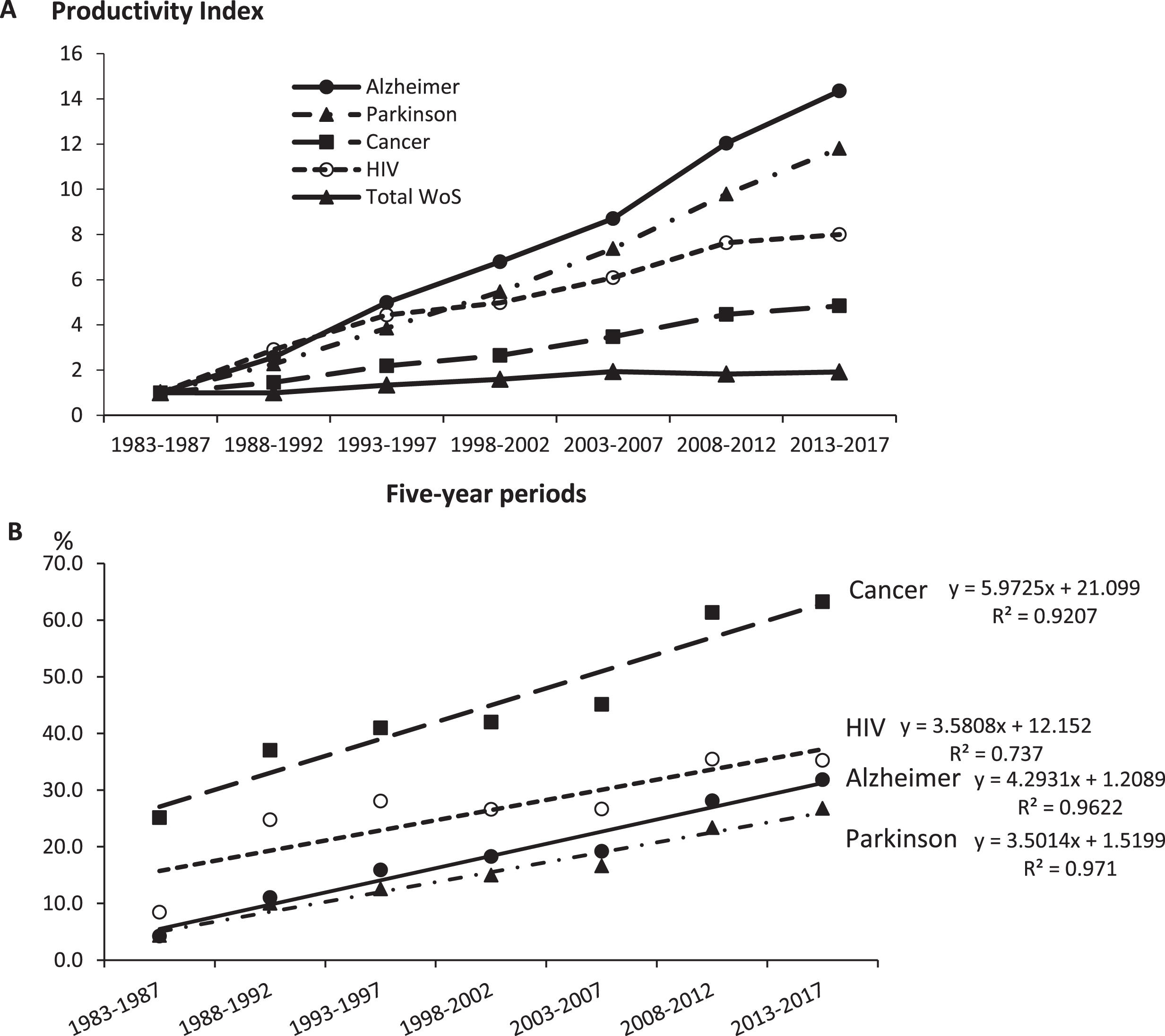
Growth of journals publishing papers on Alzheimer, Parkinson, Cancer and HIV in the WoS database from 1983–2017. A) Time course of journals publishing papers on Alzheimer, Parkinson, Cancer, and HIV during 1983–2017 in the WoS database. Productivity index = number of journals publishing papers on Alzheimer, Parkinson, Cancer and HIV during each five-year period / number of journals publishing papers during the first five-year period. The number of journals publishing papers on AD (Parkinson; Cancer; HIV) = 227 (232; 1,337; 451) for 1983–1987; 1,544 (1,267; 3,550; 2,247) for 1998–2002 and 3,257 (2,739; 6,470; 3,607) for 2013–2017. B) Spreading of journals on Alzheimer, Parkinson, Cancer and HIV within the WoS database expressed as the ratio of the # of journals/the total WoS journals (*100).
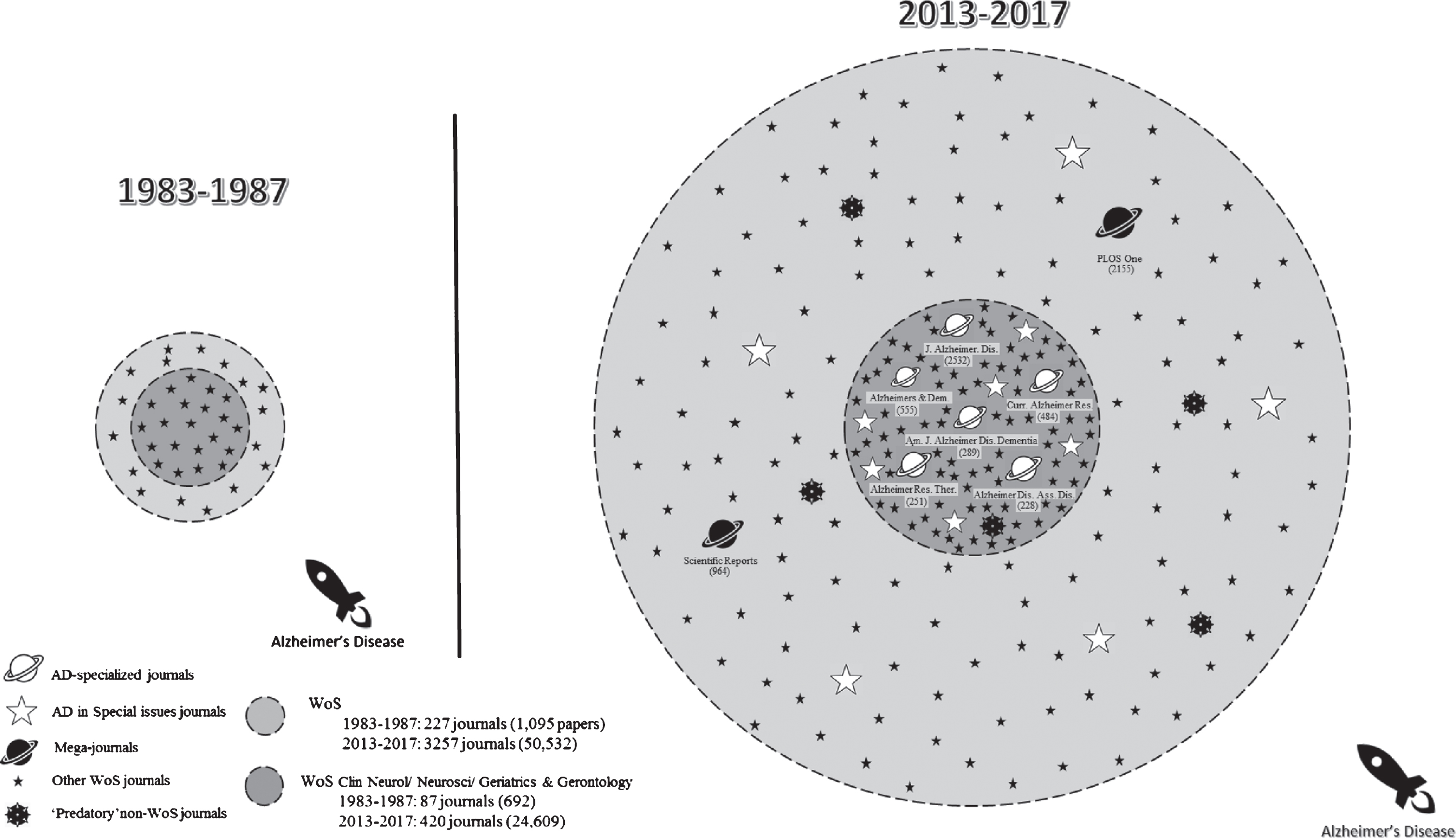
“Journal- universe” publishing AD research papers. Circles are proportional (in terms of the number of journals) to the change between extreme five-year intervals. Symbols are not proportional to the “magnitude of change”; they provide the reader a qualitative but not a quantitative view of the changes between 1983–1987 and 2013–2017.
Number of Countries with ≥ 10 AD research papers in seven five-year periods (1983–2017). The total numbers of Countries for each period are at the top and the numbers of Countries with <10 papers for each period are at the bottom
Socio-economic data (2017) for the top-20 most productive countries in AD research—ranked in decreasing order of # papers in 2017. (Highest values (rank 1) in columns 2, 4, 6, 8, and 10 are bolded.)
Top-10 most productive journals in AD research in seven five-year periods (1983–2017); numbers and percentages of journal publications in each period and WoS categories; Journal Impact Factors (IF) and journal rankings in WoS categories for 2017
List of scientific journals focusing on Alzheimer’s or Neurodegenerative Diseases (1986–2017)
Growth of AD publication
During the period 1983–2017, the number of research papers on AD increased 46-fold: 1,095 papers in 1983–1987 to 50,532 in 2013–2017. Figure 1 provides comparative growth rates for the number of papers on Alzheimer, Parkinson, Cancer, HIV, and the total WoS database. AD showed the greatest productivity rate over the other diseases from 2008–2017. The fact that AD publications increased more rapidly than for Cancer or HIV illustrates the heightened awareness of governments and institutions as well as the mobilization of the scientific and medical communities to further basic and clinical research in AD. Figure 2 provides comparative growth rates as percentages of papers on Alzheimer and Parkinson published during 1983–2017 in journals indexed in the WoS database under the subject categories of Clinical Neurology or Neurosciences: initially less than one percent for either Alzheimer (0.85%) or Parkinson (0.75%) during 1983–1987, and increasing to 7.92% (Alzheimer) and 5.80% (Parkinson) during 2013–2017.
Countries
Table 1 shows the countries in decreasing order of the number of papers on AD: 27 countries in 1983–1987, 73 in 1993–1997, 94 in 2003–2007, and 152 in 2013–2017. Results are discussed below for six major countries (according to productivity of AD papers in 2013–2017); for other noteworthy countries; and for other countries by broad geographical areas.
USA
Since the creation of the National Institute of Aging (NIA) in 1974, the US has occupied a major place in the development of fundamental and clinical research on AD. In a 1976 editorial published in the Archives of Neurology, the neurologist and “Alzheimer’s Activist” Dr. Robert Katzman identified AD as “a major killer” [18]. During the 35-year period surveyed, the publishing productivity of the US increased more than 25-fold (from 645 articles published during 1983–1987 to 16,901 in 2013–2017), despite a decrease in the share of global AD papers (58.9% in 1983–1987 to 33.4% in 2013–2017) (Table 1).
Development of AD research structures in the US
In the early 1980s, the US developed an important infrastructure focusing on AD: the creation by the NIA of five AD Research Centers (ADRC/ADC) in 1984. Currently, there are 32 ADRCs (some having satellite centers and/or branches) throughout 21 States. The National Alzheimer Coordinating Center (NACC) was established in 1999 to facilitate collaborative research and data-sharing among the ADCs, which subsequently expanded their outreach and led to the development of further programs including:
Alzheimer’s Disease Cooperative Study in 1991 to develop AD clinical trial evaluation methods and conduct clinical studies for new treatment;
Alzheimer’s Disease Neuroimaging Initiative in 2004 to identify the earliest changes in brain structure and function that signal AD onset and progression;
Alzheimer’s Disease Genetics Consortium in 2009 to conduct genome-wide association studies for identification of genes associated with an increased risk of developing late-onset AD;
Alzheimer’s Clinical Trials Consortium in 2017 to accelerate and expand studies for therapies in Alzheimer’s disease and related dementias.
An analysis of the growth and impact of ADCs from 1985–2012 showed publications increasing from about 100 in 1985 to over 600 in 2010, totaling 12,170 publications in the 28-year span, and conducting “high-impact, multi-university collaboration” [19]. Finally, Khachaturian and Khachaturian [20] have provided a 30-year chronology (1980-2010) of key federal strategic plans, task force reports, directives, and editorials placing AD research as a national priority and stating that “there is global unanimity of opinions among policy makers, scientists, caregivers and advocacy groups about the urgency of seeking a solution to the pending public health crisis.”
Research funding for AD in the US
By 2010, the US government acknowledged the importance of AD and in 2011, President Obama signed the National Alzheimer’s Project Act (NAPA) making research into the prevention and treatment of AD a national priority [21]. Following NAPA, the National Plan to Address Alzheimer’s Disease in 2012 aimed at “assisting individuals and families affected by Alzheimer’s and other dementias by advancing research, enhancing care and support, and increasing collaboration across federal, state, and tribal governments” [22]. At the same time the Chief Medical and Scientific Officer of the Alzheimer’s Association urged the federal government to increase research funding of AD [23]. Consequently, NIH funding for AD research increased from $562 million for 2014 to $1,789 million for 2018, far ahead of funding for other neurological diseases such as Parkinson’s disease ($193 million), epilepsy ($184 million), multiple sclerosis ($112 million), and just behind Dementia in general at $1,881 million [2, 24]. In addition, the NIA, the leading institute at NIH for AD and related dementias (ADRD), appropriated $400 million in 2017 for AD/ADRD research in collaboration with multiple institutes across NIH [25]. More recently, President Trump signed a bill allocating $2,340 million to fund AD research in 2019 [26]. The importance of US funding of AD-related research is also evidenced in nine out of 20 grants within the tau funding database from 2006–2016 from US institutions contributing over $1,720 million, mostly from NIH. Tau protein aggregation “has emerged as a potential unifying factor across several neurodegenerative diseases” including AD [27]. Although AD research funding through NIH has increased in recent years, it remains far behind estimated funds to other major diseases for FY2019: $2,305 million for AD, $3,045 million for HIV/AIDS, and $6,610 million for cancer. Considering that limited cures exist for cancer and therapies exist to arrest or slow the progression of HIV, none are currently available for AD. Moreover, AD is “the most expensive disease in America”—$2,770 million in 2018 excluding the staggering financial and emotional cost of unpaid caregivers [28]. The fairly recent development of AD biomarkers means early diagnosis of AD “before the dementia stage”; this has the potential of considerably reducing medical and care costs [1]. In addition to federal funding of AD, other non-profit organizations in the US (as well as in other countries) are forming “public-private partnerships” to support AD research [29, 30].
Research publications of AD in the US
The leading position of the US in AD research publications corroborate bibliometric studies of literature on AD [31]; on topics directly related to AD, namely cholinesterase inhibitor research [9]; and on other neurodegenerative disease such as Parkinson’s disease [32]. Some major scientific contributions in AD research pioneered in the US during our 35-year study period include: the identification of a novel cerebrovascular amyloid protein, known as amyloid-beta, the chief component of AD brain plaques [33]; the “simultaneous” discovery of protein tau as a major component of AD paired helical filaments by Dr. Grundke-Iqbal and colleagues [34] and by a Belgian-French team [35, 36]; the first demonstration of tau immunotherapy in mice [37]; and the introduction of an influential model of biomarker changes during AD progression [38].
The importance of the US is also illustrated by the fact that: it is the principal collaborative country of the ten most productive countries on AD (data not shown); it is a major actor in the revision/updating of the definition, criteria, guidelines, and recommendations of/for AD [39 –41]; from 1984 to 2008 more than one-half of the top-100 most productive investigators in AD research were affiliated to institutions in the US [7]; it was involved in the organization of early AD Congresses and International Conferences; and AD research has progressed with the BRAIN Initiative® (Brain Research through Advancing Innovative Neurotechnologies) launched in 2013 which aims “to deepen understanding of the inner workings of the human mind and to improve how we treat, prevent, and cure disorders of the brain” [42 –44].
China
In ancient China, the earliest description of dementia was found in the Yellow’s Emperor Internal Classic written some 2000 years ago [45]. Paralleling a 2017 figure of some 9.5 million AD sufferers in China [46] is the rapid increase of AD publications by Chinese researchers from 1998 to 2017 in our study, with China second to the US in the number of papers published in the latest period, 2013–2017 (Table 1). This increase in publications corroborates those shown by Dong et al. [13], and in a recent study of cholinesterase inhibitors for AD treatment [9]; it also accords with China’s increase of research publications in Parkinson’s disease, another neurodegenerative disease [32].
A milestone study published in 2000 compiled 16 previous epidemiological studies on dementia performed on the Chinese population [47]. The authors attributed the heterogeneous results observed to various parameters: “differences in sampling procedures, the age structure of the population surveyed, data collection methods and diagnostic criteria used”. They also highlighted the decades of using traditional Chinese medicine in the treatment of dementia and the abundance of basic and clinical research; but stated that “there is little information on dementia research in China in the international literature”. Since 2000, China has increased its participation in AD research with some major contributions: a 2014 study describing the atomic structure of γ-secretase, a protease complex responsible for cutting the transmembrane domain of the amyloid-β protein precursor (AβPP) to form the amyloid-β protein, an aggregation-prone product that accumulates in the brain in AD [48]; collaboration with the Alzheimer’s Disease Neuroimaging Initiative (ADNI) “to develop biomarkers for Alzheimer’s disease, to evaluate the effects of lifestyle risk factors on Alzheimer’s disease progression, and to establish and validate MRI and PET images, cerebral spinal fluid measures and blood biomarkers as possible predictive measures of the disease” [49]; and the identification of two AD susceptibility loci represented by common disease-associated variants in the Chinese population that could also provide information about functional effects of these genetic variants in the pathogenesis of the disease [50].
The recent increase of Chinese AD publications in the WoS can be explained by: the worldwide increase of clinical and scientific interest in AD; the pressure and incentive of the Chinese government to publish in journals indexed in the WoS databases [51 –53]; the increase funding allocation for dementia research by the National Natural Science Foundation of China [54]; and the recent development of the Chinese Brain Science and Brain-Inspired Intelligence project, a 15-year plan (2016–2030) with multiple theoretical and practical aims [55]. Additionally, there is an abundance of scientific literature published in Chinese that are not indexed in the WoS; for example, a 2008 study showed that less than 6% of the 2,500 journals belonging to one of five large biomedical databases from China (CBM, CMCC, CNKI, VIP, and Wanfang) were indexed in Medline [56], and therefore a large number of publications may be missed when not searching Chinese databases; this was confirmed recently by Cohen and co-authors [57].
When compared to the US, China’s AD publishing profile differs in several aspects. Firstly, from 1998 to 2017, the share of Chinese AD papers doubled from one period to the next (1.8% for 1998–2002; 4.0% for 2003–2007, 8.8% for 2007–2012, and 16.1% for 2013–2017) while that of the US declined from 45.3% to 33.4% during the first and last five-year periods (Table 1), and the rise in its rankings from 20th in 1988–1992, to 8th in 2003–2007, 3rd in 2008–2012, and finally 2nd in 2013–2017 is particularly striking; furthermore, it is estimated that China’s scientific output will shortly overcome that of the US [58]. Secondly, when the ratio (2.07) of AD papers (US/China) was analyzed, those published in AD-focused journals, prestigious multidisciplinary journals, or Neurological/Neuroscience key journals were mainly skewed towards the US, for example: J Alzheimers Dis, 3.09; Alzheimers Dement, 17.85; Curr Alzheimer Res, 1.46; Nat Commun, 5.05; Proc Natl Acad Sci U S A, 6.24; Lancet Neurol, 15.50; and Nat Neurosci, 7.80. Thirdly, in using a specific AD h-index, Sorensen [7] showed that more than one-half of the top-100 most prolific AD investigators were affiliated with US institutions, while none was affiliated to any Chinese institution. These differences invite further studies to fully explicate the recent appearance of China in the landscape of AD research. No doubt China’s estimated 9.5 million people with dementia [59] and projected to exceed 20 million in 2050 [60] will see a continuing rise in Chinese AD research.
UK
Since the 1960s, the UK has played a major role in the development of modern neuroscience and the founding of the first British neuroscience society in 1968, the Brain Research Association later renamed in 1996, the British Neuroscience Association [61]. From the late 1970s, the British Medical Research Council (MRC) made funding research on AD a priority [62]. Therefore, not surprisingly, our study showed that from 1983 to 2017, the UK increased its scientific literature on AD 28-fold: from 164 papers (1983–1987) to 4,647 (2013–2017) positioning it among the top-three most productive countries (Table 1).
The first National Dementia Strategy for England was implemented in 2009; for Scotland in 2010; and for Northern Ireland and Wales in 2011 [63]. Several major contributions of the UK in AD research include: the Alzheimer’s Research UK (ARUK) trust founded in 1992 with the mission “to defeat dementia”. Since 1992 ARUK’s total funding commitment is over £101 million; it has awarded 786 for “pioneering research” and is currently funding 143 research projects in the UK and abroad [64]; the launching in 2017 of the UK Dementia Research Institute (UK DRI) with six centers in leading universities devoted to AD research and funded by the MRC, the Alzheimer’s Society, and ARUK; the Brains for Dementia Research project set up in 2007 and jointly funded by ARUK and the Alzheimer’s Society to address the shortage of brain tissue from individuals and to support a “network of brain bank facilities across England and Wales” which monitors “the memory, thinking and behaviour of each prospective donor” and “provides researchers with a complete medical history to accompany the donated brain tissue, allowing them to see how brain changes correlate with symptoms” (http://brainsfordementiaresearch.co.uk/brain-donation/). A recent publication shows the “evolution in a longitudinal brain donation cohort” to comply with the changing needs of the research community [65]; and the organization in 2013 of the G8 Dementia Summit to “set out an international response to dementia with the aim of identifying a cure or a disease modifying therapy by 2025” [66]; and the results of a recent study performed at King’s College of London revealing a feedback loop underlying brain degeneration in AD which may explain the failure of numerous drug trials [67].
Germany
In 1906 Alois Alzheimer (1864–1915) a German clinical psychiatrist and neuropathologist described the first case of “presenile dementia” which later was called AD [68]. Henceforth, Germany has been at the forefront of research in AD—always ranked among the top-five most productive countries since 1988; its productivity increased 15-fold from 242 papers in 1988–1992 to 3,654 in 2013–2017 (Table 1).
Several milestones illustrate the scientific contribution of Germany in AD research: in 1991, two German researchers of the Zentrum der Morphologie of Frankfurt proposed a six-stage neuropathological progression of AD-related changes [69]; in 2007, a German group at Saarland University provided evidence of the role of the key innate immune receptor (TLR4) in neuroinflammation in AD [70]; in 2013, a group from the University of Bonn suggested a role for the inflammasome in AD [71]; and in 2017, a German/Dutch group used a cryo-electron microscopy to 4.0Å resolution to provide detailed insight into the architecture of Aβ 1–42 fibrils to understand differences in pathogenic familial mutations and the molecular mechanism underlying fibril growth [72].
At the national level, the German Center for Neurodegenerative Disease (DZNE) was founded in 2009. Its aim is to investigate the similarities and differences of various neurodegenerative diseases and to develop new preventive and therapeutic approaches. Spread over ten sites with 80 working groups, its important research activities can be illustrated by almost 200 scientific publications during the 2013–2017 period, and by the development of a longitudinal multicenter observational study focusing on subjective cognitive decline in the context of AD [73].
At the European Union level, Germany has continuously participated in European projects: for example, in the 7th FP (2007–2013), Germany coordinated various projects such as Memory Loss in Alzheimer’s Disease: Underlaying Mechanisms and Therapeutic Targets and Quantum Dot-Based Highly Sensitive Immunoassays for Multiplexed Diagnostics of Alzheimer’s Disease. More recently Germany collaborated in the Aetionomy project to develop a “mechanism-based taxonomy”, that is, identifying biological pathways involved and the etiology of Alzheimer’s and Parkinson’s diseases. Germany also participates in the European Prevention of Alzheimer’s Disease consortium (http://ep-ad.org/), and in the Synaptic Dysfunction in Alzheimer’s Disease (SYDAD), a European training network which involves collaborative research programs to reveal the mechanisms behind synaptic dysfunction in AD.
Italy
For three earlier five-year periods, Italy ranked 7th among the top countries in AD research publications: 202 papers in 1988–1992, 546 in 1993–1997, and 971 in 1998–2002; however, for the last three five-year periods, it ranked 5th overall: 1,623 papers in 2003–2007; 2,368 in 2008–2012, and 3,202 papers in 2013–2017 (Table 1). Italy has a long and active tradition in neurological research [74, 75]. Some of Italy’s many contributions to knowledge on AD, such as: numerous publications of debate or review papers which question and drive the validity of the underlying hypothesis on AD origins and mechanisms [76
–78]; funding by the Italian Ministry of Health of a Strategic Programme involving ADNI-based imaging markers to develop and validate a protocol for the diagnosis and tracking of AD in the prodromal phase [79]; and participation in different 7th FP EU projects including: the coordination of the project, European Consortium for Stem Cell Therapy for Neurodegenerative Diseases, which received more than € 15 million in funding; the coordination of the project Nanoparticles for Therapy and Diagnosis of Alzheimer’s Disease (NAD) (http://www.nadproject.eu/) which aims to develop nanoparticles for Alzheimer’s diagnosis and therapy, involving 19 European research centers in 13 European countries; and the development of the Italian Project on the Epidemiology of Alzheimer’s disease (I.PR.E.A.), an EU Joint Programme - Neurodegenerative Disease Research [80].
Japan
From 1983 to 2017, Japan ranked among the top-six most productive countries in publication of AD research: its productivity increased from 35 publications in 1983–1987 to 2,840 in 2013–2017 (Table 1).
Since the early 1970s, Japan has been actively involved in research on aging and AD [81, 82] and in the last decade, it launched three dementia research programs: 1) In 2007, the Japanese Alzheimer’s Disease Neuroimaging Initiative (J-ADNI) project received funding from the Ministry of Health, Labor and Welfare (MHLW), the New Energy and Industrial Technology Development Organization (NEDO), seven domestic and four international pharmas to set up 38 clinical sites [83]; over 500 participants who had either mild AD, late amnestic mild cognitive impairment (MCI) or were cognitively normal from these sites were studied over 2–3 years to provide “more plausible sample size estimation for a clinical trial of AD-modifying treatments“ [84]. The overall results “support the feasibility of bridging clinical trials in the prodromal stage of AD between Asia and Western countries” [85]. 2) In 2015, the Organized Registration for the Assessment of Dementia on Nation-wide General Consortium toward Effective Treatment in Japan (ORANGE Registry) was established with the aim “to establish an appropriate care method for dementia by collecting information on people in various stages of health”. 3) In 2016, the Integrated Registry of Orange Plan (IROOP) was implemented “to clarify symptoms that appear before the onset of dementia ... ” and “to promote clinical research and clinical trials for the development of drugs expected to improve cognitive function” [86, 87].
A major contribution of Japan to AD research was the discovery of human inducible pluripotent stem cells (iPSCs) by the 2012 Nobel Prize in Physiology and Medicine, Dr. Yamanaka and his colleagues at Kyoto University [88] and the utilization of iPSC-derived neurons as investigating tool for AD research [89, 90]. Japan also contributes to the fundamental debate on AD origins and mechanisms as illustrated by a recent reconsideration of amyloid hypothesis and tau hypothesis and concluded that “suppression of tau production currently seems to be the most promising target for development of AD therapeutic drugs” [91].
With its average age of 46.1 years, Japan is among the top-three most elderly country [92]; its annual growth rate of total prevalent cases of AD (4%) is well above those of the US and European countries such as Germany, France, Italy, or Spain [93]; and its exploding cost of dementia, estimated to be $18.8 billion in 2060 [94] are further reasons for developing and increasing AD-research in Japan.
Lastly, Japan started its Brain Mapping by Integrated Neurotechnologies for Disease Studies (Brain/MINDS) project in 2014 [95] using a small primate animal model, the common marmoset. The project presents numerous advantages for AD researchers, one of which is an appropriate transgenic model of neurodegenerative disease [96, 97].
Other countries
It would be simplistic to focus attention on AD research contribution just on the six most productive countries. In Europe for example, Belgium scientists went beyond the assumption that “point mutations in the presenilin-1 gene (PS1) are a major cause of familial Alzheimer’s disease”; they showed that “inhibition of PS1 activity is a potential target for antiamyloidogenic therapy” in AD [98]. France developed and funded three National Alzheimer plans: (1st) 2001–2005, € 105 million; (2nd) 2004–2007, € 200 million; and (3rd) 2008–2012, € 1,058 million [99, 100]. These three plans were extended by a Neurodegenerative Disease Plan [101]. A recent bibliometric study showed that between the second and third plan “French scientific output in AD increased 3.9-fold more than the overall level of French scientific output ... ” and that “ ... French scientific output in AD increased more in quantity and quality by comparison to several major countries ... ” [102]. In the Nordic countries, seven scientists were ranked in the top-100 most prolific researchers on AD [7].
Other important contributions to AD research are from two English-speaking countries: Australia and Canada. In the early 1980s, a Western Australian research group collaborated with West German researchers to “purify and characterize the cerebral amyloid protein that forms the plaque core in Alzheimer disease ... ” [103]. In 2006, the Australian Imaging, Biomarkers & Lifestyle (AIBL) study was developed in Perth and Melbourne to improve diagnosis of AD and to discover treatments and lifestyle factors for preventing or delaying the onset of AD. The AIBL study published more than 300 articles from 2010–2019 (https://aibl.csiro.au/). Early in the 2000s, the Australian Ministers of the Department of Health developed the Dementia Initiative, making Dementia a National Health Priority (2005–2010 and ongoing), and the National Framework for Action on Dementia for 2006–2010, later extended by the National Framework for Action on Dementia from 2015–2019. In 2016, Henry Brodaty (Australian Professor) was awarded the international Ryman Prize for dementia research over 30 years. Australia has also organized domestic conferences (e.g., Australian Dementia Forum in 2019) as well as international conferences such as the ADI 1988 conference in Brisbane and more recently the ADI 2015 in Perth. Canada’s contribution to AD include inter alia: demonstrating that the amyloid precursor protein gene and the Alzheimer’s locus were one and the same [104, 105]; contributing to the concept of cognitive impairment not dementia [106], a precursor of the concept of MCI; developing the Canadian Brain Imaging Research Platform (CBRAIN), a web-based collaborative research platform providing transparent access to the heterogeneous computing and data resources available across Canada and around the world [107]; developing a national dementia strategy in 2017; and becoming an integral part of the North America ADNI project [108].
In Asia, South Korea is an active participant in the field of AD as illustrated by: the development in 2000s of a longitudinal hospital-based registry of dementia patients by the Clinician Research for Dementia of South Korea (CREDOS) funded by the Ministry of Health, Welfare, and Family Affairs [109]; the Dementia Comprehensive Management Measure in 2008, followed in 2012 by the publication of the Second National Dementia Management Master Plan 2013–2015 [110]; and the Korean Brain Aging Study for the Early Diagnosis and Prediction of Alzheimer’s Disease (KBASE) cohort started in 2014 to develop new biomarkers involving two university hospitals and two public centers around Seoul [111].
It should be noted that the progressive globalization of medicine and research has favored the development of international network/institution/private-public partnership/programs either specifically dedicated to AD or neurodegenerative diseases (e.g., ADNI, GAAIN, Pharmacog, EU-JPND), or to more general areas such as the Innovative Medicine Initiative (IMI) and BrainNet Europe (BNE). Such structures need to be developed and nurtured as they have synergistic effects on leading countries in AD research and provide efficient tools to reinforce collaboration between developed and developing countries.
Geographical areas
EU
From 1983 to 2017, the share of EU publications on AD research was moderate (24.5% of all AD publication for 1983–1987) and then increased from between 36.8% –40.7% during 1993–2017 (Table 1). This relatively high sustained share can be attributed to the following: continuing and increasing scientific interest of EU members in AD research; growing number of member states in each five-year period, from 12 members in 1983–1987 to 28 in 2013–2017; continuing investment of the EU in AD research as shown by the increasing number of AD-projects in each successive Framework Programmes (FP) for Research and Technology Development—fewer than five for each of the first three FPs from 1984 to 1994 and increasing to 37 for FP4 (1994–1998), 267 for FP7 (2007–2013), and 211 for the current period (2014–2020). Two AD-research projects illustrate the recent (Horizon 2020 FP) EU investment: 1) Amyloid imaging to Prevent Alzheimer’s Disease (AMYPAD) aimed at “(a) improving the diagnostic workup of patients suspected of AD and their management; (b) stratifying risk for AD and selecting homogenous groups for intervention; and (c) quantifying treatment effects more accurately”, funded for € 27.3 Million (including € 11.9 Million for the EU) for five years (2016–2021) involving 7-EU members: France, Germany, Luxembourg, Netherland, Spain, Sweden, UK; 3 industrial partners, 2 SMEs and 1 patient organization; and 2) Promoting Active Ageing: Functional Nanostructures for Alzheimer’s Disease at Ultra-Early Stages (PANA) which focuses on “developing theranostic nanostructures that specifically recognize very-early molecular markers of AD, which can be detected by means of non-invasive imaging methodologies (MRI and/or PET –common techniques accessible in most hospitals) and eventually can provide a therapeutic action if needed”. This project was launched in 2016 and EU-funded for € 7.7 Million involving seven EU-members: Belgium, Finland, Lithuania, Luxembourg, Netherland, Portugal, and Spain.
Recently, a comprehensive review paper written by a panel of experts gave an overview of the present situation in Europe regarding AD and outlined a number of challenges (prevention, diagnosis, treatment, biology, health economics, etc.) that need to be addressed to reduce the burden of dementia. The authors highlighted several points constituting “bottlenecks to progress in basic, translational, and clinical AD research”: primarily inadequate investment, funding and human resources and fragmentation and poor coordination of research efforts. It is hope that this review will reach policymakers in all sectors of AD, especially as the EU is well-positioned for global leadership with “its excellent health-care delivery system, basic single payer model, outstanding research infrastructure, and strong pharmaceutical industry base” [112].
The commitment of Europe in AD research can also be measured by the development of various structures (organizations, associations, consortia, non-governmental associations, etc.) for funding students and young researchers, and/or participating in research or clinical projects. One such structure is the IMI (http://www.imi.europa.eu), a public-private partnership between the European Union and the pharmaceutical industry association, European Federation of Pharmaceutical Industries and Associations (EFPIA) to fund health research and innovation. Two IMI funded structures to facilitate access to human health data are “cohort-derived” data sources within AD and include: the European Medical Information Framework (EMIF) (http://www.emif.eu/) and the Aetionomy which developed a “mechanism-based taxonomy” of Alzheimer’s disease and Parkinson’s disease (mentioned above) and have just successfully completed their five-year funded period. The European Prevention of Alzheimer’s Dementia (EPAD) Consortium is an interdisciplinary research program composed of public and private sector organizations working towards understanding the early stages of AD in order to deliver new preventive treatments; thus fulfilling the IMI Alzheimer’s Disease Research Platform. In 2014 IMI launched IMI2, the second phase “proof of concept study for the secondary prevention of Alzheimer’s dementia” [113]. Currently, 18 projects (programmes) are registered in the IMI ambit.
European research on AD will surely benefit from the Human Brain Project launched in 2013 by the European Commission’s Future and Emerging Technologies, and for which one main objective is to “create and operate a European scientific research infrastructure for brain research, cognitive neuroscience, and other brain-inspired sciences” [114]. Over 1,000 publications on AD have either been issued or are in the pipeline from the various projects.
Latin America
Recent publications highlighted the importance of AD in Latin America [115 –117]; some qualifying dementia as an “emergent silent tsunami” [118]. Latin America has a long tradition in clinical neurology [119], and its recent investment in AD research is illustrated by the explosion of its scientific output during the last 35 years surveyed: three papers for all Latin American countries in 1983–1987, 320 in 1998–2002, and 2,057 in 2013–2017 (Table 1). During this period, the progression in the number of AD papers showed that countries in Latin America fall into three groups: 1) five countries in order of productivity (Brazil, Mexico Chile, Argentina, and Colombia) ranging from 1,157 to 165 papers in 2013–2017; 2) another five countries in order of productivity (Cuba, Uruguay, Peru, Panama, and Ecuador) with from 25 to 11 papers; and 3) the remaining Latin American countries with fewer than 10 papers.
Brazil is the most productive Latin American country with more than one-half (56.2%) of the 2,057 papers by Latin American researchers in 2013–2017. A recent study of Brazilian research publications on cognitive impairment and dementia from 1999–2013 showed a rising trend in both quantity and quality [120]. Publications from the 10/66 Dementia Research Group showed that 10% of 217 papers published between 2000–2019 focused on Brazil. Van Noorden [121] highlights the “impact gap” among the South American countries: while “Brazil dominates the publication record” research quality (impact or influence) lags behind the rising output. South American papers are still struggling “to attract citations from the rest of the world”. Engedal and Laks [122] encouraged Brazil to set up a nationwide dementia plan (along the lines of the European plans) to “increase the number of people being diagnosed ... and to improve the quality of care and quality of life for people with dementia and their families”.
Mexico is the second most productive Latin American country with 307 AD-papers published during 2013–2017. A recent publication projected that some 3.5 million elderly Mexicans will be affected by AD in 2050 and an Alzheimer’s Plan of Action has been proposed to promote prevention and early diagnosis and to support patients and their caregivers [123].
Although the population of Mexico is over 7.3 times that of Chile (132 million versus 18 million), they have similar percentages (0.5–0.6%) of AD in their populations [124] and similar numbers of papers (≈300) in 2013–2017. The landscape of aging and dementia in Chile was recently updated [125] and although the average annual cost of dementia in Chile is lower in comparison to high-income countries, the proportion of total cost related to informal cost (daycare) is higher; socioeconomic status is the major determinant of cost and leads to income (and gender) inequality [126]. Consequently, the government of Chile adopted a national plan on dementia in 2017.
Argentina (with 222 AD papers) was the first Latin American country to join the ADNI structure in 2011 [127, 128]. Colombia (with 165 AD papers) is involved in an important collaboration with Germany to provide novel insights into the pathophysiology of familial AD [129], and participates in a collaborative project COLBOS (COLombia-BOSton) between the Fundación Universidad de Antioquia, Colombia, and Massachusetts General Hospital in Boston to study a large kindred group with the PSEN1 E280A mutation [130].
The remaining Latin American countries with small or negligible publications do not reflect a lack of interest in AD research; rather it may be more likely a lack of government involvement. According to the World Population Ageing report [131], from 2015–2030, “the number of older people is expected to grow fastest in Latin America and the Caribbean with a projected 71% in the population aged 60 years or over.” Hence, AD research in this region needs to be encouraged.
Africa
Sharing only 1.2% of the 50,532 AD-papers published during 2013–2017 and having only five countries with more than one AD-paper/year during this period, Africa is the struggling relation in the AD research community. Such observation was noted earlier [33, 132], and is in accordance with the lagging situation of Africa’s research in various fields of neurology such as headache research [133], multiple sclerosis [134], and Parkinson’s disease [32]. This strongly contrasts with the urgent need for African countries to increase its worldwide battle against AD.
Various studies show that the current and projected demographics of Africa (including its AD population) in future decades will be a major concern for the political, social, scientific, and medical communities: the population of Africa (currently 1.32 billion) is predicted to nearly double in 2050 [135] and those 60 years or older will increase over threefold—from 68.7 million to 225.8 million in 2050 [136]. With an aging population one can predict an equally dramatic increase in the number of people with AD. In Sub-Saharan Africa (population currently 1.08 billion), a recent report estimated that people with dementia will increase more than 250% from 2.13 million in 2015 to 7.62 million in 2050 [137]. Africa has ongoing social crisis, civil war, and delays in delivery of medical and therapeutic equipment for neurodegenerative disease when compared to other countries [138]; Africa also bears the burden of the HIV epidemic where Sub-Saharan Africa is home to 53% of the world’s population living with HIV [139].
Despite all these difficulties, research on AD in Africa is progressing. Firstly, although few African countries contributed more than 10 papers on AD in each five-year period from 1983 to 2007, the last two five-year periods saw increases: 219 papers from 21 countries in 2008–2012 and 609 papers from 39 countries in 2013–2017 (Table 1). Secondly, three countries (Kenya, Nigeria, and South Africa) are developing national dementia plans. Thirdly, 30% of the African countries (16 of 54) are among the 94-member associations of the Alzheimer’s Disease International; the mission of the association is “to strengthen and support Alzheimer associations, to raise awareness about dementia worldwide, to make dementia a global health priority, to empower people with dementia and their care partners, and to increase investment in dementia research”. It is hoped that with the help and support of the international scientific communities, Africa will bridge the gap separating it from developed countries in order to partake in the latest AD research and therapeutic standards.
Top-20 countries in 2017
When the top-20 most productive countries in 2017 are viewed through socio-economic lenses (Table 2), three groups may be perceived: 1) countries with closely similar rankings in both the number of AD papers and their GDP per capita: USA, Germany, France, South Korea, and Turkey; 2) in contrast, countries at the top one-half ranked by GDP per capita but at the bottom one-half ranked by their output of AD papers: Australia, Sweden, Netherland, Switzerland, Taiwan, and Belgium; and 3) contrasting further, countries that are productive but ranked at the bottom one-half of their GDP per capita: China, UK, Italy, Japan, Spain, and India. To make further comments on the three groupings or on the 16 (80%) developed countries as among the main contributors of research publications in AD is not possible without additional information; though we note that 12 (60%) developed countries had > $40 K GDP per capita and that three are perhaps “punching below their weights”. Contrariwise, of the four (20%) emerging markets or developing countries, China and India, both with low GDP per capita and are the most populous countries on Earth, are making sizable AD research contributions and, with the other two countries (Brazil and Turkey), are contributing to AD research well above their “expected possibilities”. The live expectancy for 70% of the countries is >80.0 years with Japan leading. The 20 countries represent more than one-half of the world population. Finally, of the remaining 132 countries (Table 1), there are 80 (53%) countries with fewer than 20 papers published during 2013–2017; a large number are developing countries partly or entirely in the southern hemisphere.
Institutions
With AD correlated to an increase of our aging population, the clinical, societal, and scientific communities have developed non-governmental and/or supranational institutions to organize the fight against AD. These organization now play a key role in AD research and clinical management and, without neglecting the numerous other existing association/institution, three of the main organizations are discussed briefly.
Alzheimer’s Disease Neuroimaging Initiative
In 2004, the US NIA launched a large private-public partnership to set up the ADNI; its goals were to use neuroimaging, biochemical, and genetic biological markers to track the progression of AD in human brains and to improve clinical trials for the prevention and treatment of AD. The initial study for five years (ADNI-1) involved 800 cohorts (200 elderly controls, 400 mild cognitive impairment or MCI, and 200 AD) from 57 sites in the US and Canada; it was extended in 2009 for two years by a Grand Opportunities grant (ADNI-GO) with an addition of 200 early MCI. The study was further extended for five years in 2011 (ADNI-2) with the addition of from 100–150 participants in each group (expanding the MCI to include early, late and late-mild participants). By ADNI-3 (from 2016 for five more years), the project added another 133 elderly controls for a final cohort of over 1,000 participants to go beyond developing biomarkers, to study the “use of tau PET and functional imaging techniques” for AD clinical trials.
An important characteristic of ADNI project is that it has made all its data available worldwide without embargo to scientists, pharmaceutical companies, and government-funded investigators. Open data access is through the data archive hosted at the Laboratory of Neuroimaging (LONI) at the University of Southern California (http://adni.loni.usc.edu/).
Since its creation in the US, the ADNI project has gradually spread worldwide: 1) The European ADNI project was founded in 2005 and collaborated with Pharmacog, a pan-European partnership mainly funded by the EU, the IMI, and the EFPIA [79, 140]. 2) In Australia, the AIBL, an ADNI project, was launched in 2006; one of the AIBL study found that there was no suggestion of an association between post-traumatic stress disorder and the brain deposition of amyloid or tau in Australian Vietnam veterans with post-traumatic stress disorder [141]. 3) The J-ADNI was launched in 2007 in collaboration with 11 pharmaceutical and seven imaging companies [83], and a second phase (J-ADNI2) was launched in 2015. 4) The Chinese ADNI (C-ADNI) project was launched in 2012 and one of its aims is to explore the relationship among multiple-modality MRI/PET, clinical cognitive and biofluid data for validation of biomarkers in the abnormalities and cognitive decline of patients. 5) In Latin America, the Argentina ADNI (Arg-ADNI) project was launched in 2013 with the intention of using the same methodological approach to study the adult offspring of AD patients with autonomic and circadian abnormalities [128]. 6) Also in 2013, the Korean ADNI (K-ADNI) project was funded by the Korean Ministry of Health and Welfare along with private industry; it included individuals with either vascular MCI or subcortical vascular dementia. 7) In 2012, the Taiwan ADNI initiated a three-year longitudinal study. 8) Plans to develop ADNI studies in Brazil and India are currently underway.
During the last 15 years, ADNI has been very active and has progressed in the understanding of AD mechanisms; it has also implemented an efficient publishing strategy whereby papers presenting results of their studies are regularly published in a variety of journals. A quick search showed that some 900 ‘article-type’ papers have been published in the WoS from 2013–2017, providing ADNI to weigh in just as prominently as countries ranking between 15th and 20th in publication productivity; additionally, substantial review papers are periodically published by members of ADNI [108 , 142–145]. Several years ago, two issues of the journal Alzheimer & Dementia were dedicated to the progresses in AD research resulting from ADNI projects [146, 147].
ADNI is an exemplar of a consortium of non-profit/charity organizations collaborating with governmental, industrial and private organizations worldwide. Such structures have sizable funds, personnel competencies and compatibilities to engage in major AD projects involving research, clinical trials, and support for patients and caregivers. A search on Consortia-pedia (https://consortiapedia.fastercures.org/) identified 21 active consortia involved in AD, and in 2017 there were 25 non-profit organizations involved in advancing the challenges of AD [29]. These structures are now part of the landscape of AD research in the medical community and the public at large.
Alzheimer Disease International (ADI)
In 1984, the ADI was created “to strengthen and support Alzheimer associations, to raise awareness about dementia worldwide, to make dementia a global health priority, to empower people with dementia and their care partners, and to increase investment in dementia research”. ADI has become the global umbrella for numerous (94) non-profit associations worldwide mainly to support people with dementia and their families.
In 1998, the 10/66 Dementia Research Group (DRG) affiliated with ADI was created “to quantify the prevalence and incidence of dementia in less-studied countries, learn about the causes of dementia, describe care arrangements for people with dementia, quantify the impact of providing care on caregivers and encourage the development of appropriate support services and evaluate their effectiveness”. The 10/66 DRG programs focuses on “66% of people with dementia living in low and middle income countries and 10% or less of population-based research ... carried out in those regions”. A large epidemiological study performed on 16 countries in the 10/66 regions (Latin America and the Caribbean, Africa, India, Russia, China and South East Asia) found that: 1) the incidence of dementia in low-or-middle-income-countries is similar to those in high Income countries; 2) DMS-IV dementia [148] incidence is two times lower than that of the 10/66 DRG criteria [149]; and 3) cognitive reserve might counter the effect of neurodegeneration in late life [150]. Additionally, the 10/66 DRG research protocols and dementia diagnostic criteria were recently used in other countries such as Central African Republic, Congo, Iran, Lebanon, Portugal, and Singapore [151]. The studies of dementia epidemiology performed by the 10/66 DRG since 1998 resulted in more than 200 publications, most of them (>150) being published in the last 10-year period, 2008–2017 [151].
Additionally, ADI is represented in the international scientific and medical community through the following: 1) Alzheimer’s Research & Therapy: journal publishing articles suggesting breakthroughs in the field of AD and other neurodegenerative conditions; 2) World Alzheimer Reports: an annual publication providing general information on Alzheimer and dementia from various perspectives: economic, societal, clinical, scientific, epidemiologic, etc.; 3) World Alzheimer’s Day (September 21st) to raise awareness about AD and dementia; 4) International Conference of Alzheimer’s Disease International since 1984 as well as the organization and participation in regional conferences mostly held in low-or-middle-income-countries; and 5) close collaboration with the World Health Organization to promote AD and other neurodegenerative diseases.
Alzheimer Association (AA)
Among the numerous AD-focused institutions that have emerged in the US is the Alzheimer’s Association (AA), the largest non-profit voluntary organization founded in 1980 by J.H. Stone; it claims to be “the leading voluntary health organization in Alzheimer’s care, support and research” (https://www.alz.org/). Since 1982, AA has become an integral part of the scientific community through: 1) investing over $455 million in nearly 3,000 scientific investigations worldwide; 2) creating three journals: Alzheimer’s & Dementia (in 2005), and more recently in 2015, two open access journals, Alzheimer’s & Dementia: Diagnosis, Assessment & Disease Monitoring and Alzheimer’s & Dementia: Translational Research & Clinical Interventions; 3) organizing the annual Alzheimer’s Association International Conference since 1988 which claims to be the “largest and most influential international meeting dedicated to advancing dementia science”; 4) creating the Alzheimer’s Association International Society to Advance Alzheimer’s Research and Treatment in 2008 for individuals interested in Alzheimer’s and dementia science.
During the last decade AA, together with the NIA, contributed to AD research by sponsoring: the last set of neuropathological diagnostic criteria for AD [152, 153], the last set of clinical diagnostic criteria for dementia due to AD [39], MCI due to AD [154], pre-clinical AD [155], and the Research Framework that defines AD based on the A/T/N biomarker classification [41]. Additionally, the AA website offers a wide range of information and services for various individuals and groups interested in aspects of AD: patients, caregivers, physicians, scientists, clinicians, the media, institutions, and so on. Finally, AA also publishes annual reports (latest, 2020) entitled Alzheimer’s Disease Fact and Figures on the global situation regarding AD and regularly participates in the establishment of guidelines, criteria, definition and recommendations that are used to adjust/update current practice in the treatment of AD (https://www.alz.org/alzheimers-dementia/facts-figures).
As is the case for other diseases such as Cancer and HIV, the previous description of the strength and efficiency of non-governmental organization shows the importance and necessity of such (national or supranational) organization in the battle against AD. Additionally, collaboration between these structures and governmental structures are encouraged to build a synergetic framework and to optimize research and medical progress in AD.
Journals
Over the 35-year study period the huge development of research on AD led to an explosion and diversification of journals publishing AD papers. This evolution concerns both the number and the specificity of the journals targeted by AD research.
From 1983 to 2017, the number of journals publishing AD papers increased 14-fold: 227 journals in 1983–1987 versus 3,257 in 2013–2917 (Fig. 3). Figure 4 illustrates the evolution of the AD “journal universe” from 1983 to 2017: the “publishing space” of the AD scientific literature expanded considerably, including the number of journals specific to AD research and the number (and diversity) of journals publishing AD papers.
Development of journals specialized in AD research
The appearance of journals dedicated to neurodegenerative disorders has contributed to the further growth of publications on AD: there were none among the top-10 journals in 1983–1987, but three in 2013–2017: Journal of Alzheimer’s Disease (launched in 1998), Alzheimer’s and Dementia (in 2005), and Current Alzheimer Research (in 2004). With a further three specialist AD journals—American Journal of Alzheimer Disease and Other Dementias, Alzheimer’s Research and Therapy, and Alzheimer Disease and Associated Disorders—these six journals concentrated close to one-tenth (8.8%) of the 50,532 papers published during 2013–2017 (Table 3). Information provided by Pubmed shows 24 ‘active’ neurodegenerative disease journals launched from 1986–2017 (Table 4), considerably more than the six AD-specific journals indexed in the SCI-E database. Additionally, as AD mainly relies on neurological dysfunctions and affects mostly the elderly, journals classified in one or more of the three WoS categories (Neurosciences, Clinical Neurology, and Geriatrics & Gerontology) are natural outlets for publishing AD research. This can be seen in 25 of the top-100 most productive journals on AD in 2013–2017 that have one of the following keywords in their titles: Alzheimer, aging, geriatric, gerontology, or neurodegenerative (data not shown); further evidence is illustrated by the close relationship between AD and two journals, namely Neurology, a reputed journal in the field of neurology, and Neurobiology of Aging, an emblematic journal in geriatrics and gerontology. Over the 35-year span of the study, these two journals were always in the top-10 most productive journals on AD. Furthermore, the percentages of AD papers in the two journals have generally increased in the earlier years before the appearance of AD specific journals in the later years: for Neurology it went from 4.2% in 1983–1987 to 19.1% in 2008–2012 and then 17.0% in 2013–2017; for Neurobiology of Aging, it went from 25.1% (1983–1987) to 70.2% (1998–2002) and then 62.0% in 2013–2017. Lastly, Cappai [156] described the significant contributions of papers in the Journal of Neurochemistry on the molecular basis of AD from 1980–2016; Journal of Neurochemistry appears in the top-10 journals in four of the five-year periods from 1993–2012 (Table 3).
Special issues dedicated to AD
Another major source of AD information is the regular publication by journals of “Special Issues” consisting of papers on recent advances of topics on (or related to) AD. A brief search revealed dozens of Special Issues on AD in journals during 1997–2017 with most from 2008–2017. One example can be seen in the journal Neurobiology of Aging which is in the top-10 from 1983–2017:19 of its 24 Special Issues from 1995 to 2017 were on specific aspects of AD (e.g., therapies, bio- or molecular-markers) or conferences, symposia, and congresses (or their abstracts) on AD. Special Issues on AD have also appeared in non-neurodegenerative disease journals such as The Open Nuclear Medicine Journal [157], Biochemical Pharmacology [158], and Molecules [159]; and in general medical journals such as PLOS Medicine [160], and the Journal of Internal Medicine [161].
Multidisciplinary journals publishing AD papers
Interestingly, since 1998 Multidisciplinary Sciences journals were always present in the top-10 most productive journals on AD: Annals of the New York Academy of Sciences and Proceedings of the National Academies of Science from 1998 to 2007 plus two newcomers, PLOS One and Scientific Reports, from 2008 to 2017. The latter two are ‘mega-journals’ that are inter alia peer reviewed, fully open access, and delivered electronically [162]. The presence of the two mega-journals among the top-10 most productive journals was shown in a recent study performed on another neurodegenerative disease [32] and was explained by a ‘size-effect’ induced by the high volume of papers published by these two journals, generally several thousand papers annually [162] as compared to others in the top-10 publishing a few hundred papers annually.
Prestigious journals publishing AD papers
Another channel that is used to alert and inform the scientific and lay community is the publication of AD research in prestigious scientific journals. For example, in 2013–2017 four multidisciplinary journals (Nature, Nature Communications, The Lancet, and Science, all with IFs > 12) published more than 200 papers on AD. Not surprisingly, AD research during 2013–2017 also featured in prestigious neurological/neuroscience journals such as Neurology (425 articles), Brain (270), JAMA Neurology (188), Neuron (67), Nature Neuroscience (49), and in more general biomedical journals such as Nature Medicine (26), Cell (25), PLOS Biology (18), and Nature Genetics (8). Exposure of AD research in prestigious high impact journals contributes not only to the diffusion of information within the professional community, but also to the society at large through the distillation of (often) complicated scientific/medical articles by specialist journalists for dissemination in the popular press such as, newspapers and magazines—for example, The New York Times or The Economist. Alternatively, as the number of social media users worldwide is over two billion and growing, the lay community users of social media are sharing AD information within their support groups while the professional social media users are educating the public in AD research and recruiting volunteers for clinical studies (see for example, [163]). We also note that three of the top-10 AD publishing journals (PLOS One, Neurology, and Scientific Reports) belong to the top-30 of a set including the most influential medical journals according to Wikipedia [164].
Predatory journals
The professional community should be aware of recent so-called “predatory” journals (journals that publish for a fee without providing adequate reviewing or editing services) and publishers with “questionable marketing and peer review practices” which are negatively impacting the explosive growth of “scholarly open access publishing funded by article processing charges” [165]. Beall’s “List of Predatory Journals and Publishers” (https://beallslist.weebly.com/) provides over a thousand publishers who publish from a few to over 100 journals. Beall’s List also includes, inter alia, links to “Non-recommended medical periodicals” and “News”, including a 2018 item from Nature on “The undercover academic keeping tabs on ‘predatory’ publishing” [166]. Readers and researchers will be interested in a list of 101 ‘suspected’ predatory open access journals in neurology and 87 in neurosciences; a small percentage of articles from these journals were found in two large databases, Scopus and PubMed [167]. More general cautionary steps and recommendations for choosing ‘reputable’ journals for publishing research are provided by Masten and Ashcraft [168] and Shamseer et al. [169].
Evolution of the top-10 most productive journals
While almost all of the top-10 most productive journals on AD in 1983–1987 (ranked by number and percentage of publications on AD) were “generalist” journals in the fields of Neurosciences and Neurology (Annals of Neurology, Neuroscience Letters, Archives of Neurology, Neurology, Canadian Journal of Neurological Sciences, etc.), journals specifically dedicated to AD started appearing in 1998 (Journal of Alzheimer’s Disease) and in the most current period (2013–2017), it was joined by two others (Alzheimer’s & Dementia and Current Alzheimer Research) accounting for 7.1% of the AD papers (Table 3). During the same period two “generalist” journals (PloS One and Scientific Reports) published 6.2% of the AD papers. Along with five other neurosciences/neurology journals, the top-10 most productive journals concentrated nearly one-fifth (18.9%) of all the 50,532 AD papers published during 2013–2017; at the opposite end of the journal/productivity spectrum, nearly two-thirds (65.6%) of the 3,257 journals with AD papers published five or fewer papers. With the exception of the two “generalist” journals, the other eight are classified (wholly or partially) within the WoS categories of Neurosciences or Clinical Neurology and sometimes in both. Not surprising the two ‘aging’ journals (Neurobiology of Aging and Frontiers in Aging Neuroscience) are also in the category Geriatrics & Gerontology.
Journal distribution among WoS categories
This increase was matched by the growth of journals dedicated to neurodegenerative disease research; hence, catering for the needs of scientists and clinicians in the field (Fig. 4). In 1983–1987 there were 227 journals with papers on AD research and 87 (38.3%) were indexed in one to three of the WoS categories Clinical Neurology, Neurosciences, and Geriatrics & Gerontology for 63.2% of AD papers (n = 1,095). However, by 2013–2017 only 420 (12.9%) of 3,257 journals in one to three of the same WoS categories, concentrating 48.7% of AD papers (n = 50,532) (Fig. 4). By examining AD papers only in journals indexed in these three highly relevant WoS categories, the percentages of journals increased from 49.1% in 1983–1987 to 84.8% in 2013–2017.
During the last decades, AD research has been integrated into the scientific publishing establishment as illustrated by the dozens of journals (or special issues) focusing on AD research and the numerous publications of AD papers in prestigious/leading multidisciplinary journals. Additionally, AD papers have spread into almost all medical and biological fields, though concentrated mostly in Clinical Neurology and Neurosciences areas. Readers and researchers interested in AD can now find or publish AD papers in journals belonging to a vast spectrum of scientific fields.
Conclusion
During the past 35 years, the landscape of AD research has been expanding. Research on AD had dramatically increased as illustrated by the explosion in the number of publications on AD: the average number of AD papers/year was 220 during 1983–1987, and has continuously grown to exceed 10,000 AD papers/year during the last five-year period (2013–2017). This evolution was accompanied by a 14-fold increase in the number of journals publishing AD research having several characteristics: specialist journals on AD; generalist scientific and medical journals; Special Issues on AD in both specialist and generalist journals; mega-Omic journals; and specialist or generalist “predatory” journals.
In the same period the AD research community has expanded to include 27 countries in 1983–1987 and 152 countries in 2013–2017, with the rapid emergence of China in the last ten years of our study and the negligible research visibility of the African countries. Initiated in the US, this rapid evolution was accompanied by the development of a variety of national and international Institution/Association/Organization programs and initiatives (e.g., AA, ADI, ADC network, 10/66 DRG, ADNI, EPAD consortium, EU-JPND, etc.) that contribute in shaping the societal, medical, scientific, and political AD communities. Gradually built over several decades, the dual framework of medical research consisting of governmental/national structures (national research structures dedicated and/or supporting AD research) and international association/organization has evolved into an efficient structure in the treatment and management of AD.
The challenges of finding suitable treatments for the rapidly growing number of AD patients in an aging population, and the steady progress in AD research in the last decades in various fields (Genetics, General Medicine, Neuroimaging, Drug Delivery, Nanomedicine, Biomarkers, Animal Models, etc.) are major arguments for the continuation of scientific, medical, financial, and political investments in AD research.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/19-1281r3).