
Abstract
Background:
Treatment decisions based on guidelines rather than patients’ preferences determine adherence to and compliance with treatment, which, in turn, could improve health-related outcomes.
Objectives:
To summarize the stated treatment and care preferences of people with dementia (PwD).
Methods:
A systematic review was conducted to assess the stated preferences of PwD. The inclusion criterion was the use of quantitative methods to elicit stated preferences, enabling a ranking of preferences.
Results:
Eleven studies revealed preferences for diagnostics, treatment decisions, patient-related outcomes, care services, end-of-life care, leisure activities, and digital life story work. PwDs prefer accurate, pain-free, and comfortable diagnostic procedures without radioactive markers as well as being accompanied by a caregiver. PwD’s quality of life (QoL), self-efficacy, and depression were equally most important for PwD and caregivers. However, PwD memory was only important for caregivers but not for PwD, and caregiver QoL was moderately important for PwD but least important for caregivers. Additionally, comfort and family involvement were most important for patients’ end-of-life care, whereas caregivers most preferred good communication and pain management. Also, preferences depend on the living situation: Patients living not alone prefer a regular care provider most, whereas those living alone only want to live nearby the caregiver. Preferences for leisure activities did not differ between past and present ratings, indicating that PwD prefer activities that have always been carried out.
Conclusion:
Only a few studies have applied quantitative methods to elicit the preferences of PwD. More research is needed to capture the stated preferences for the treatment, care, and support of PwD to improve health-related outcomes and the allocation of healthcare resources.
INTRODUCTION
All over the world, life expectancy is increasing, leading to an aging society and an increase in age-associated illnesses, such as dementia [1]. Currently, there are approximately 46.8 million people with dementia (PwD) worldwide, and most of them suffer from Alzheimer’s disease [2]. Half of the affected people are older than 80 years old, and two-thirds are women [2]. Without a cure, it is estimated that there will be 131.5 million PwD in 2050 worldwide [3].
PwD requires a timely diagnosis and evidence-based patient-centered treatment to delay the progression of the disease. Attenuating functional and cognitive decline could improve or at least maintain patients’ health-related quality of life (HRQoL) [4–6]. However, treatment guidelines are based on clinical evidence from different studies that aimed to improve, in most cases, clinical outcomes. Such outcomes are often not strictly associated with an improvement in health-related quality of life that could be noticed subjectively by the patients. In addition, other patient-related treatment characteristics, such as the mode of administration of drugs, are rarely considered in clinical studies. Therefore, the perspective of the affected patients and the patient preferences are rarely taken into account in both evidence-based guidelines and treatment and care decisions.
During the progression of dementia, PwD become increasingly cognitively and functionally impaired, resulting in an increasing need for care and further support. In the beginning stages of the diseases, approximately 75% of PwD are living at home, and the majority are supported by their close relatives [7]. Living next to their relatives at their own home is one major preference of many PwD [8]. In these times, PwD’s relatives provide informal care [9]. In most cases, the disease progresses to such a point that the informal caregivers cannot manage the intensity or the community-dwelling living situation, so institutionalization becomes inevitable [10]. Thus, it can be assumed that the priorities and preferences of PwD and their informal caregivers change over the course of the dementia [11]. Therefore, after receiving the diagnosis, PwD have to make many decisions, e.g., about their current and future living situation, therapy, level of care and support needed, and they need to define cornerstones for their patient decree for the time when they become unable to make decisions due to increasing cognitive impairment [12, 13]. All these fundamental decisions should be made in good consideration and with adequate support [14].
For optimum management of the dementia disease and to initiate individual, tailored, and patient-centered treatment, care, and support, a patient’s preferences for all affected domains and all stages of the disease must be known. However, there are considerable methodological challenges in validly eliciting the preferences of PwD. It is unclear how to best define preferences. Qualitative preference studies, such as interviews, are the most common method used to detect patient priorities [15]. In these studies, the quality of care, contact with relatives, person-centered caregiving, emphasizing dignity and respect were indicated as important for PwD [8]. However, decisions between alternatives that have different attributes or characteristics have not to be made, missing the opportunity to generate a numeric ranking of preferences, including a description of quantitative differences between various preferences and patient groups that were based on standardized methods. Within a complex healthcare system with scarce resources, it is important to know which aspects (attributes) of a treatment and which outcomes are most and least important from a patient’s perspective. Addressing the most preferred attributes could increase adherence to treatments and therapies, improve and individualize interventions, and finally improve patient-related outcomes [16]. Avoiding the least preferred attributes could save already scarce healthcare resources and preserve patients from low-value interventions, which, in turn, could improve patient-related outcomes. Those methods are grounded in microeconomy and pertain to the stated preference techniques, such as discrete-choice experiments, best-worst scaling, analytic hierarchy process and other types of survey questions using ranking and rating techniques [17, 18].
Therefore, the objective of this systematic review was to summarize the stated preferences of cognitively impaired people and PwD, considering all domains that could be affected by cognitive decline, such as the clinical status, symptoms, functioning, living situation, medical treatment, care, support, and patient-related outcomes.
MATERIALS AND METHODS
To identify and demonstrate patients’ stated preferences in cognitive impairment or dementia, a systematic review of quantitative studies was conducted.
Search strategy
The literature search was performed in PubMed, Science Direct, and Cochrane Library using a non-MeSH (medical subject headings) and MeSH search. The non-MeSH search used the key phrases “dementia” or “Alzheimer” or “Alzheimer’s disease” in combination with “preference*” or “priorit*” or “rank*”. MeSH terms were additionally used to find all studies that were linked to the terms in the PubMed database “mild cognitive impairment” or “dementia” in combination with the MeSH heading “patient preference”. Both search terms (non-MeSH and MesH) were combined using the OR operator. The systematic literature search included studies published between 1985 and April 12, 2019. The search strategy is presented in the Supplementary Material.
Data extraction
Studies were included if 1) the articles were written in English or German language, 2) the patients had cognitive impairment or dementia, Alzheimer’s disease, or cognitively healthy participants from the general population who were asked hypothetically to imagine having dementia; and 3) the preferences had been elicited based on stated quantitative preference methods, such as discrete choice experiment, analytic hierarchy process, best-worst scaling, or other quantitative rating methods, enabling a ranking of stated preferences of PwD to elicit the most and least important preferences. Studies using a qualitative approach, such as interviews or open question surveys, were excluded. Additionally, we excluded systematic reviews and study protocols.
Overall, the search strategy yielded 578 articles. After removing 34 duplicates, 544 studies were retrieved for title and abstract screening. Two independent reviewers screened the titles and abstracts (SL, HW). In cases where the reviewers could not make a decision, a third reviewer was involved (AR, BM). Overall, 440 studies (see Flowchart) were excluded after title and abstract screening, and 93 were excluded after full text screening, resulting in the inclusion of eleven studies. The flow chart of the screening procedure is demonstrated in Fig. 1.
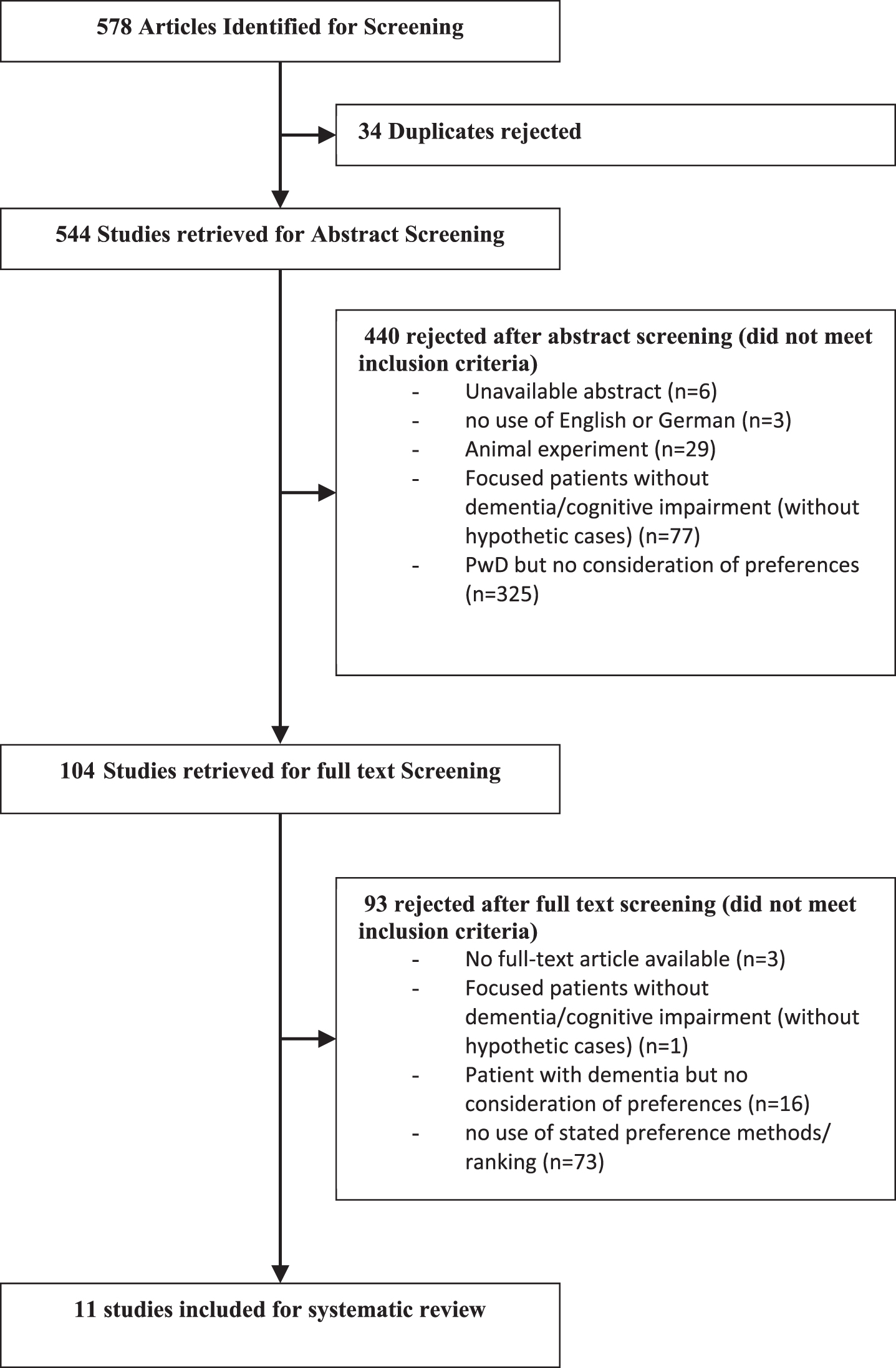
Study Flow Chart (CONSORT).
Data description
We extracted basic information describing the studies, including year of publication, author, country, aim of the study, and the sample size. We furthermore extracted the quantitative method used to elicit stated preferences. The coefficients of demonstrated preferences were used to derive the relative importance of each attribute, generating the ranking of stated preferences, which was the main result of this review. In some cases, the ranking of attributes was demonstrated for different subgroups, such as patients, caregivers and dyads. In these cases, each ranking of each subgroup was elicited and presented.
Quality assessment of included studies
To assess the methodological quality of the included studies, the PREFS checklist (Purpose, Explanation, Findings, Significance) was used [19]. This checklist addresses the preference (Purpose), the possible selection bias (Respondents), the description of the used method (Explanation), the possible reporting bias (Findings), and the use of significance testing (Significance). We excluded the Respondents assessment because preference studies do not calculate how much respondents stopped or did not answer. According to this checklist, studies were ranked between zero, indicating a weak quality, and four, indicating the highest methodological quality (for details see Table 1) [19]. Two reviewers checked and judged the quality of the studies separately (SL, AR). If there was no consensus, a third reviewer became involved (BM).
Valuation of the PREFS checklist for the selected studies
Scale: 0 = poor, 1 = fair, 2 = good, 3 = very good, 4 = excellent.
RESULTS
Characteristics of the included studies
All eleven studies were published between 2010 and 2018. These studies considered a wide range of different attributes regarding the diagnostic procedure [20, 21], treatment preferences [22], leisure activities [23, 24], patient-reported outcomes [25, 26], care services [27, 28], and end-of-life care [8, 29]. One study was conducted in Canada, five were conducted in the United Kingdom (UK), one was conducted in Germany, three were conducted in the Netherlands, and two were conducted in the United States of America. The sample sizes of the included patients ranged between eight and 1,301. A description of the quality grading and characteristics of the studies is shown in Table 1 and Table 2, respectively.
Preference studies of people with cognitive impairment and dementia
AD, Alzheimer’s disease; ADL, Activities of Daily Living; DCE, discrete choice experiment; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; PET, positron emission tomography; PwD, people with dementia; QoL, quality of life; SPECT, single photon emission computed tomography
Diagnostic procedure
Based on a card sorting exercise, Bamford et al. [20] revealed preferences for diagnosing dementia using positron emission tomography (PET) or single photon emission computed tomography (SPECT) in the UK in 2016. Patients over 60 years (n = 68) with mild or moderate dementia (Mini-Mental State Examination > 12) ranked accuracy (rank 1), helpful staff (rank 2), and comfort during scans as most important (rank 3). The accuracy of the diagnostic procedure was perceived as more important than the circumstances of the scan, such as radiation dose (rank 5), space in the scanner (rank 6), duration of the scanning procedure (rank 7), or noise (rank 10). Most elicited attributes were similarly preferred between patients, caregivers, and healthy controls. However, compared to healthy controls, the presence of a companion, such as a caregiver, was very important for PwD and caregivers but not for healthy controls (rank 4 versus rank 8).
Mühlbacher et al. [21] elicited similar preferences for the general population older than 60 image having dementia in the UK and Germany (n = 1,301). Based on a discrete choice experiment (DCE), the authors investigated preferences for dementia test technologies. The preferences did not differ significantly between the two countries. The respondents reported that a test imprecision of 5% (Coeff: 10.0) and a test without a radioactive marker (Coeff: 9.0946) were most important, followed by test imprecisions of 15% (Coeff: 6.0402) and the cost for the test (Coeff: 5.3259). The absence of the test (Coeff: 1.9769), a spinal tap (Coeff: 1.7451), and a test imprecision of 30% (Coeff: 0.0) were least important.
Treatment
Janus et al. [22] elicited preferences for pharmacological or nonpharmacological treatments for caregivers (n = 81) and proxies (n = 59) of PwD using best-worst scaling techniques. Considering pharmacological treatment, caregivers reported that the fastest results (standard score: 0.36), recommendations by physicians and pharmacists (standard score: 0.33) and the most effective treatment (standard score: 0.29) were most important, but treatments with the lowest costs (standard score: –0.43) and the least amount of effort for themselves (standard score: –0.51) were less important. For the proxies, the most effective treatment (standard score: 0.58), the fastest result (standard score: 0.53), and the least negative effect (standard score: 0.36) are most important, whereas the treatment with the lowest cost (standard score: –0.75) was the least important. Concerning the preferences for nonpharmacological treatments, caregivers reported that minimally burdensome treatments for the patient (standard score: 0.35), the most appropriate treatment for the complaints (standard score: 0.27) and the patient’s preferences (standard score: 0.26) were most important, but the most feasible treatment (standard score: –0.36) and the most widely used treatment (standard score: –0.48) were least important. For the nonpharmacological treatment, the proxies of PwD reported that the least negative effect (standard score: 0.67) and the most effective treatment (standard score: 0.45) were most important, whereas the lowest cost (standard score: –0.57) and the treatment that required the least amount of effort (standard score: –0.67) were least important.
Patient's and caregiver’s outcomes
Barrios et al. [25] investigated the preferences for behavioral outcomes of seven patients with mild cognitive impairment (MCI) and their caregivers with a ranking task in the United States in 2016. Participants were recruited from a memory training program that includes cognitive rehabilitation and cognitive stimulation training and were asked for their preferences before and after the training program [30]. Before starting the training program, PwD ranked their own quality of life (QoL) (rank 1) and self-efficiency (rank 2) as most important, followed by caregiver QoL (rank 3) and depression of the caregiver (rank 4). Whereas PwD and caregivers equally preferred patients’ QoL and self-efficacy as most important, all other preferences significantly differed between both groups. For caregivers, patients’ depression was the second most important, but this factor was rather unimportant for patients themselves (rank 11). Furthermore, patients rated caregivers’ QoL and anxiety as more important and the self-efficacy and depression of the caregiver as less important compared to the rating the caregivers made by themselves. Notably, the rankings slightly changed over time: caregivers’ outcomes were more important for PwD after the intervention than they were before. Patients ranked caregiver burden as most important after the intervention, whereas this attribute was ranked as the 5th most important before receiving the intervention. Furthermore, after the intervention, caregivers rated their own QoL as the second most important preference, but it was only moderately important before the intervention (rank 5).
Smith et al. [26] analyzed the preferences of people with MCI (n = 29) within the same memory training program of Barrios et al. but based on a different and larger sample using a ranking task. In this analysis, patient preferences significantly differ from the analysis of Barrios et al. [25], which could be due to bias and a given uncertainty in eliciting preferences using small sample sizes. However, patients’ QoL (rank 1), self-efficacy (rank 2). and depression (rank 3) were most important for people with MCI (n = 29). Whereas patients’ QoL and self-efficacy still represented the most important stated preference, PwD’s depression was much higher ranked (patients: rank 3) compared to the findings of Barrios et al. [25] (patients pre-intervention: rank 11). Caregiver outcomes were less important for people with MCI. The QoL of the caregiver was ranked as moderately important for the patients (rank 5) but least important for the caregivers (rank 8). Furthermore, there were significant differences concerning the actual memory capacity between the ranking solicited from the PwD and the ranking by the caregivers. Memory was more important for the couples (dyads, patients and their caregivers) and caregivers (rank 2 and rank 3) than it was for PwD themselves (rank 10). Another difference was observed in the preferences concerning depression. Both PwD and caregivers ranked this outcome as more important in the absence of their caregiver or PwD, respectively. When couples were interviewed, both jointly ranked these attributes lower. In contrast to Barrios et al. [25], Smith et al. [26] added the attribute “actual memory performance” to the decision model. However, this additional attribute appears to be not responsible for the different results of similar studies (Barrios and Smith) because differences were observed mainly in the ranking for caregivers’ QoL and mood.
Activities
The study of Cohen-Mansfield et al. [23] examined proxy-reported preferences concerning the leisure activities of n = 77 PwD given by staff and family members. They ranked the activities separately for the past and present preference of the PwD. Listening to music (rank 1) and reminiscing (rank 2) were ranked as the highest preference for the PwD rated by family members and staff. Participating in group activities (rank 4 for family members and rank 5 for staff) and exercising (rank 5 for family members and rank 8 for staff) were moderately attractive, and playing trivia/word games and cooking/baking were least preferred for PwD (rank 9). However, females ranked cooking/baking much higher than males, revealing gender-specific differences in such preferences. The ranking of preferred activities in the past does not differ from the present rating (correlation 0.97). Differences in the preference for exercising were observed between family (5th position) and staff (8th position).
The study of O’Philbin [24] analyzed the preferences for digital life story work (LSW) service interventions of PwD and their caregivers in the UK. They were asked to be encouraged to perform digital LSW with the result of their own book. The PwD n = 17 completed an online survey with a DCE character, whereas the caregiver n = 67 joined a DCE to elicit their preferences. PwD in the UK most preferred a private setting (rank 1) and a session that focused on learning how to use the given app (rank 2). Presentation to friends and family seems to be the most common use of a digital LSW (rank 3); 53% of the respondents reported that they would pay for the service (rank 4), whereas 47% would not pay for the service (rank 5). Enjoying memories with the book, showing it to new people and having a service to get a book built (rank 10) were less preferred. The least preferred attribute was an instruction guide for the work (rank 11). In addition, for caregivers, the private setting is the most important attribute (Coeff: –0.802, willingness to pay (WTP): 41.45£), followed by a usability of the app (elementary Coeff: 0.180 WTP: –9.32£, advanced Coeff: –0.180) and follow-up assistance (Coeff: –0.150, WTP: 7.75£). A session focus (Coeff: –0.032) and a price for the intervention (Coeff: –0.019) were less preferred. In this study, the caregivers responded not to the patients but to themselves. The preferences of both groups did not differ significantly. PwD and caregivers paid special attention to ensure that the intervention takes place in a one-to-one setting.
Care services
Nieboer et al. [27] identified the preferences for long-term care services in a general Dutch elderly population (n = 1,082) wherein patients imagined having dementia using a DCE. Elicited preferences differed between patients living with a partner and those living alone. The most preferred attribute of patients living with a partner was a regular care provider (Coeff: –0.493, WTP: 88€), followed by transportation service (Coeff = –0.306, WTP: 55€), out-of-pocket spending for the care (Coeff: –0.280), coordinated care service (Coeff = –0.220, WTP: 39€), and short time on waiting list for all services (Coeff: –0.212, WTP: 38€). For patients without a partner, living near the caregiver was the most important attribute (Coeff: 0.498, WTP: 177€), followed by having a regular care provider (Coeff = –0.434, WTP: 154€), time on a waiting list (Coeff = –0.294, WTP: 154€), and transportation services (Coeff = –0.247, WTP: 88€). For people living alone, all services were found to be relatively more important than for those living not alone.
The attributes regular care provider and coordinated care service were ranked equally between both groups. Living in proximity of the caregiver was most important for patients living alone but was not important for patients with a partner. Furthermore, social activities were more important for those living alone (Coeff: 0.227 versus 0.144). Timeliness of the care provider (Coeff: –0.122), 4 hours of additional care per week (Coeff: 0.117) and individual preferences in care (Coeff: 0.068) were ranked as less important for the general elderly in the Netherlands.
Groenewoud et al. investigated preferences in patients’ health care decisions by using a DCE for a Dutch sample of n = 421 PwD in 2015. The representatives were divided into two subgroups: outcome-orientated and trust-orientated responders. The results of the groups differed only for a few preferences. However, a low travel distance (up to 5 km) to the health care provider was most preferred for both groups (Coeff: 1.035 outcome-orientated and 1.516 trust-orientated). For the outcome-oriented respondents, safety (Coeff: 0.923), 16 h extra care per week (Coeff: 0.779) and interprofessional treatment (Coeff: 0.709) were most preferred. Less preferred attributes for this subgroup were “Delivered care as agreed: sometimes” (Coeff: 0.131), “satisfied communication with staff 70% ” (Coeff: 0.084) and recommendations for a health care provider from family and friends (Coeff: 0.025). The trust-oriented subgroup most preferred a “travel distance to 20 km” (Coeff: 0.889) and “3 staff members per 15 residents” (Coeff: 0.769). In addition, the attribute “Waiting time 4 months” (Coeff: 0.699) was important. The least preferred attributes were “satisfied communication with staff 70% ” (Coeff: 0.250), waiting time of up to 8 months (Coeff: 0.201) and “delivered care as agreed: sometimes” (Coeff: 0.130).
End-of-life care
Mulqueen et al. [29] examined PwDs’ preferences for end-of life care. The respondents were n = 6 patients living in residential care facilities and their n = 6 caregivers in Ireland in 2017, and they used the nominal group technique to elicit preferences. There were considerable differences between patients’ and caregivers’ preferences. Comfortable environment (quiet and no worries) (rank 1) and family involvement (rank 2) were most important for the patients, followed by family surrounding (rank 3), communication (rank 4), and familiar staff (rank 5). However, communication (rank 1) and pain management (rank 2) were most important for caregivers. Advance care planning (rank 3), family involvement (rank 4), and knowledge of care staff (rank 5) played a minor role for the caregivers.
Dening et al. [8] used the nominal group technique to analyze the preferences of PwD and their caregivers and the influence of the caregiver on the preferences of the PwD in 2012. The responding dyads attended a memory assessment service in the UK. Patient’s ranked family contact (rank 1), independence (rank 2), and safety (rank 3) as most important but comfortable environment as least important (rank 10). The preferences of the caregiver were elicited for themselves and depended on the experience the caregivers had made during the care process. Therefore, control (rank 1) and QoL (rank 2) were most important for the caregivers.
For patients and caregivers together, the place of care (rank 1) and not being a burden (rank 2) were ranked as most important, whereas legal preparations were unimportant for the dyads (rank 7).
DISCUSSION
An increasing number of patient preference studies have been published over the last two decades [31]. However, the number of published preference studies examining patients with dementia is still particularly rare. The studies analyzed herein covered a few domains of the entire treatment, care and support pathway as well as patient-related outcomes in dementia and differed mostly with regard to the methods used. In most cases, preferences were elicited using qualitative methods, such as interviews or focus group discussion, which precludes the calculation of coefficients or a numeric rank for attributes. Only a few studies used ranking methods. Some studies were based on hypothetical scenarios asking respondents to imagine having dementia and state the preferences that they thought they would have under this condition [21, 27]. Thus, only a few studies used stated preference methods, such as DCE, analytical hierarchy process or best-worst scaling, in patients actually suffering from dementia.
Elicited preferences regarding the diagnostic procedure revealed that accuracy, explanation by staff, comfort during the procedures, and being accompanied by a caregiver were most important for both PwD and caregivers. For patients alone, the accuracy is more important than the costs.
The most important patient-related outcomes were the QoL and self-efficiency of the PwD followed by the QoL and depression of the caregivers. However, there were significant differences in patient-reported outcomes between PwD and caregivers. Whereas depression was rather unimportant for PwD themselves, PwD rated caregiver’s QoL and anxiety as more important, and the self-efficacy and depression of the caregiver was less important compared to the rating the caregivers made themselves. Furthermore, preferences differ significantly between different studies, highlighting considerable uncertainty. This difference is highlighted by the studies of Barrios and Smith, reporting different rankings of attributes, although the list of attributes and methods were similar. Smith et al. elicited preferences of n = 88 PwD compared to n = 8 in Barrios et al. Therefore, the results of Smith may have a higher relevance and generalizability. However, both studies demonstrated that for PwD, their own QoL was most important. Although QoL is the most important and preferred outcome of PwD, less than 10% of intervention studies in dementia used this outcome as an indicator of a favorable intervention [26]. Most of the studies focused on clinical outcomes, such as cognition, mortality, morbidity or psychiatric behavior, and functional impairment. Hence, QoL should be considered in future studies. Some aspects that appear to be relevant for QoL are the preferred leisure activities. Participants mostly prefer activities that they practiced in their past lifetime [23]. Thus, caregivers report preferred activities independently of the presence of dementia. Furthermore, dementia-specific activities to improve PwD memory are least important. Perhaps PwD could feel exposed or ashamed while practicing those activities and therefore tend to avoid such activities. This possibility is highlighted by the study of O’Philibin [24]. Digital LSW is preferred in a one-to-one setting and would be used to show family and friends. In most cases, LSW could be used as a therapeutic aspect [32] but derived from their preferences; for PwD, it seems to be more active.
It could be argued that PwD living with a partner differ in their preferences compared with those living alone. The ranking of patients without a partner differed in cases of transportation service or in the living situation. PwD without a partner living close to the caregiver was ranked highest, verifying that PwD wanted to live as long as possible in their own homes [33]. However, there are also similarities between the groups, for example, the preference for receiving care by the same professional caregiver or nurse. There is some evidence that such approaches are safe, beneficial for improving patient and caregiver outcomes and cost-effective [34–36]. Additionally, a short time on a waiting list for a care institution is of mediocre importance for both PwD living alone and PwD living with a partner, underlining that patients and caregivers are sensitized to the fact that serious health events could tremendously change the living and care situation of PwD.
Some preferences deal with the financial situation of PwD. A negative WTP indicates that respondents living with their partner prefer to spend money for extra home care rather than spending money for institutionalization. For PwD, distance to the health care provider, safety, and staffing were more important than the quality of care. This outcome seems to indicate that PwD prefer very close and intensive support from care professionals. Preferences were similar for end-of-life care. Interpersonal relations such as family contact or involvement as well as comfort and independence were most important. Patients and caregivers mutually influence each other if preferences are jointly elicited. Place of care, i.e., at home was most important, but the recommendation of family plays a minor part. Furthermore, preferences differ across countries. Respondents from Ireland most preferred a comfortable environment in end-of-life care, whereas this factor was least preferred in the UK. The studies of Dening and Mulqueen differ in some aspects, which could be due to the different sample sizes used in these studies. Nevertheless, family contact or involvement was important for respondents in both studies.
In addition to the methodological limitations of the quantification of patients’ preferences, the dependence of the sample size and the setting where preferences were elicited, this review revealed that preferences were not stable over time, e.g., before and after a disease-specific intervention or adverse life event [37]. Yu et al. highlighted the tremendous heterogeneity in the revealed preferences across different studies, demonstrating that preferences depend on the eliciting methods used [38]. Therefore, further research is needed to assess patient preferences in dementia diseases capturing several domains of diagnostics, treatment, care, and support as well as patient- and caregiver-related outcomes. In addition, it is of vital importance to assess the association between sociodemographic and clinical factors and different patterns of preferences. Knowing these preferences would allow us to more easily individualize treatment, care, and support in routine care to increase adherence to such interventions by a simultaneous improvement of PwD quality of life. These factors should be evaluated in future studies using designs with a high methodological quality and an adequate sample size. In addition, further research is needed to evaluate whether innovative and simpler quantitative measures, such as analytical hierarchy process, are more suitable for eliciting stated preferences in cognitively impaired patients or PwD.
Implications
The results of this systematic review do not exactly portray clinical practice, treatment, and care decisions. However, they should be considered for the development of clinical guidelines to optimize the treatment and care of PwD. Treatment and care decisions should correspond to the demonstrated PwDs’ and their caregivers’ preferences, such as minimal burdensome treatments for the patients, proximity to the caregiver or exactness in diagnostic tests, to improve the outcomes of both groups. Measuring individual preferences should be implemented in all phases of the disease. Considering these preferences will help to integrate PwD in decision-making processes concerning their therapy and care at all stages of the dementia disease. Participation from patients and their caregivers in the decision-making process would improve the success of treatments and other interventions [39]. Thus, preferences reported by patients with MCI and PwD can inform and guide the development of new medicines and therapies. As in most other diseases, in MCI and dementia, the patient is the best expert regarding his or her own health and wellbeing and should be involved as an active partner in all decisions regarding treatment, care and living situation.
Limitations
We were not able to perform a formal meta-analysis of patient preferences because the literature search yielded only a few studies with heterogeneous objectives, measures, and populations, causing an inconsistent reporting of patient preferences. Recall bias of PwD is a further limitation. It is unclear how long PwDs are able to make informed treatment decisions due to their declining cognitive abilities [40]. Consequently, it is important to explore the preferences of PwD who are still capable of judging options and express treatment and care preferences to their physicians and caregivers.
The sample sizes of the studies retrieved were small, varying from eight to 1,301. These small sample sizes limit the generalizability of the reported results. For statistically robust conclusions, the sample size of preference studies should be much higher. For example, for a patient preference study based on a discrete choice experiment, a sample size of at least n = 300 is recommended [41, 42]. In addition, an exclusion criterion for our review was the use of languages other than German or English. Hence, our strategy may have excluded preference studies in other languages.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/19-1299r2).