
Abstract
Background:
Clinical research has demonstrated that brain reserve (BR) could exert positive effects on cognition for patients with Alzheimer’s disease (AD) and mild cognitive impairment (MCI). However, the effects of BR on cognition in individuals with subjective cognitive decline (SCD) are not clear.
Objective:
To examine cross-sectional effects of BR on cognition in SCD populations.
Methods:
One hundred forty-nine subjects were studied from the Sino Longitudinal Study on Cognitive Decline (SILCODE) study. Head circumference was used as a proxy of BR. Cognition was assessed across four domains (memory, executive, language, and general cognitive functions). Multiple linear regression models were conducted to examine effects of BR on cognitive scores. Furthermore, we addressed the question that whether the degree of self-perception of cognitive decline modified the effect of BR on cognitive performance in SCD subjects.
Results:
We found a positive effect of BR on language cognition in subjects with SCD. Furthermore, the positive effect of BR on language cognition survived in SCD participants with a low degree of self-perception of cognitive decline while disappeared in SCD participants with a high degree of self-perception of cognitive decline.
Conclusion:
This study suggests that BR has the potential to delay or slow down cognitive decline in SCD individuals, especially for mild SCD.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is the most common cause of dementia [1]. It is generally considered that amyloid-β plaques and neurofibrillary tangles are the two hallmarks of neuropathologic changes for AD [2]. A hypothetical model of AD and current studies both have indicated that a preclinical phase of 15 to 20 years may precede the onset of dementia in which individuals have AD pathological changes in the absence of clinical symptoms and would ultimately progress to mild cognitive impairment (MCI) and dementia with the increase of pathological changes [3 –6].
Increasingly, studies based on cerebrospinal fluid, positron emission tomography, or postmortem examination have demonstrated that approximately 30% cognitively normal elderly persons have AD neuropathologic changes, and some subjects meet neuropathologic criteria for AD without signs or symptoms at the time of death [7 –10]. The concept of brain reserve (BR) was put forward to explain the phenomenon of disjunction between the degree of AD pathology and the severity of clinical symptoms [11]. BR, a hypothetical construct, commonly refers to neurobiological capital including numbers of neurons and synapse count [11]. In practice, BR has rarely been evaluated directly by measuring the number of neurons or synapses, and can be assessed with several proxies like head circumference (HC), intracranial volume (ICV), gray matter volume, cortical surface area, and cortical thickness [12]. Longitudinal studies have showed that smaller HC is an independent risk factor for AD, and the estimated hazard ratios for AD of small HC (<21.4 inches) were 2.3 [13, 14]. A recent study performed multiple linear regression models found a positive effect of ICV on multi-cognitive function in AD and MCI patients with AD biomarker [15]. Previous studies implied that the BR seems to be a moderator which can attenuated the negative effect of cerebral atrophy and apolipoprotein E (ApoE) ɛ4 allele on cognitive performance in AD and MCI [16 –18].
Subjective cognitive decline (SCD), defined by having self-perception of cognitive decline among cognitively normal elderly individuals, has received increasing attention as a risk factor for MCI and AD [19 –21]. However, effects of BR on cognition in SCD are not clear. Here, we aimed to investigate whether there are positive effects of BR on cognition in SCD subjects by measuring HC, especially for which cognitive function. And if so, we wonder whether this positive effect is affected by the degree of self-perception of cognitive decline.
METHODS
Ethics statement
Our study protocol was approved by the medical ethics committee of Xuanwu Hospital of Capital Medical University, Beijing, China, and all participants gave their written informed consent before any study procedures began.
Study participants
Data of 149 SCD with HC information were obtained from a cohort in China: Sino Longitudinal Study on Cognitive Decline (SILCODE) (Fig. 1). The protocol and design of the SILCODE study (NCT03370744) have been published previously in detail [22, 23]. Briefly, SILCODE was a longitudinal study carried out by Xuanwu Hospital of Capital Medical University, Beijing, China, and also it was the first project committed to promoting SCD research in Asia. The main purpose of this project is to collect longitudinal data from the SCD population and then study the dynamic changes in brain networks to explore the progressive mechanisms of AD in the brain and to construct a high-precision multimodal model for the ultra-early diagnosis of AD. Baseline recruitment started in 2017 and follow up is ongoing. At the baseline visit, a standardized diagnostic evaluation was performed for every participant including a medical history interview, physical and neurological examinations, laboratory tests, brain magnetic resonance imaging (MRI) scanning, and neuropsychological tests. The same examinations will be completed during the 15-month follow-up. Laboratory tests include blood glucose, blood lipids, homocysteine, folic acid, vitamin B12, thyroid hormone, hemoglobin, blood coagulation, syphilis-free status, and APOE ɛ4 status. The neuropsychological tests incorporates subjective cognitive decline questionnaire (SCD-Q9) [24], Hamilton Depression Rating Scale [25], Hamilton Anxiety Scale [26], Auditory Verbal Learning Test-Huashan version (AVLT-H) [27], Shape Trailing Test A (STT-A) and Shape Trailing Test B (STT-B) [28], animal fluency test (AFT) [29], Boston Naming Test (BNT) [30], and Montreal Cognitive Assessment-Basic (MoCA-B) [31]. Subjects were labeled as having SCD if they reported a decline in memory subjectively and failure to meet the criteria for MCI defined by Jak and Bondi [32], dementia due to AD established by the National Institute on Aging Alzheimer’s Association workgroups (NIA-AA) [33], and any other diseases that can cause cognitive impairment. All subjects with SCD aged between 60 and 80 years old were Mandarin-speaking, had at least 6 years of education, and were right-handed.
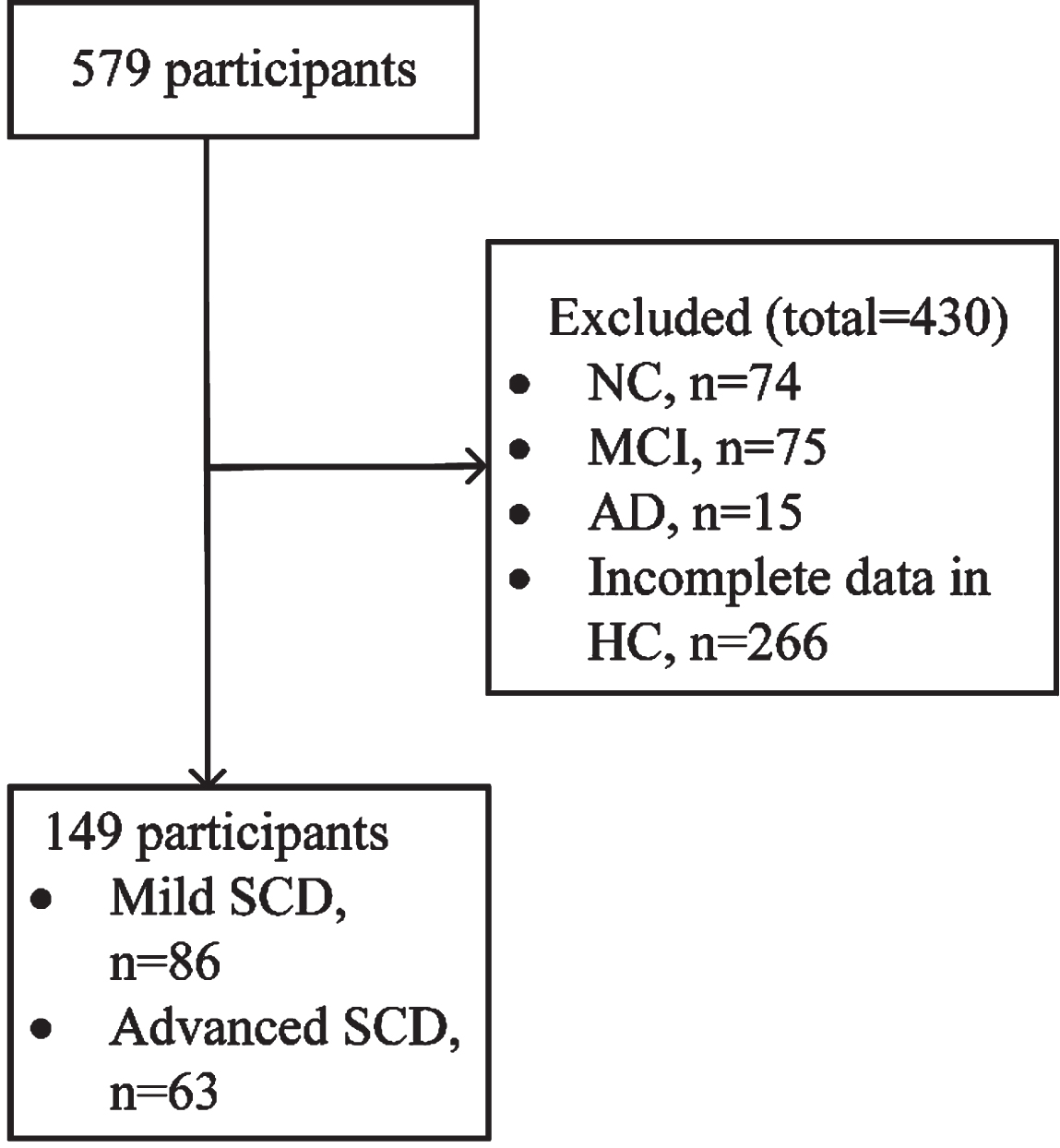
The flow chart of this study. NC, normal controls; MCI, mild cognitive decline; AD, Alzheimer’s disease; HC, head circumference; Mild SCD, subjective cognitive decline with low degree of self-perception of cognitive decline; Advanced SCD, subjective cognitive decline with high degree of self-perception of cognitive decline.
Head circumference
Subjects with SCD kept a sitting position and HC was measured by placing a measuring tape over the eyebrows and passing it around the head to fit over the most posterior protuberance of the occiput.
Defining of SCD and the degree of self-perception for cognitive decline
Details on the definition of SCD in this study published previously [22, 23]. In brief, a semi-structured interview was used to evaluate SCD before cognitive testing. This interview included information about the presence and onset of concerns, comparisons with other and a history of visiting a physician, related not only to memory but also other cognitive domains. Subjects who had memory complaints without measurable cognitive impairment and any other diseases that can cause cognitive impairment were classified as SCD. SCD were further divided into two groups: SCD with low degree of self-perception for cognitive decline (mild SCD), total score was less than or equal to median of 5.0 and SCD with high degree of self-perception for cognitive decline (advanced SCD), total score was greater than median of 5.0 according to SCD-Q9.
Statistical analyses
Data were analyzed using SPSS (version 25.0 for Window). All p values shown are subject to a significant level of 5%. A Shapiro-Wilk test, Q-Q plot, and p-p plot were used to confirm normality. All normally distributed continuous variables were reported as the mean±standard deviation and non-normally distributed continuous variables were described with the median and interquartile ranges. First, linear correlation analyses (Spearman) were used to explore associations between HC and score of neuropsychological tests including SCD-Q9, AVLT-H, STT-A, STT-B, AFT, BNT, and MoCA-B. Second, the predictive effects of HC on cognition were examined via a multiple linear regression analysis with the neuropsychological tests that had a significant correlation with HC as the dependent variable and HC as the independent variable (unadjusted), followed by a model including age, gender, education, body mass index (BMI, kg/m2), and APOE ɛ4 allele (model 1), and a model including age, gender, education, BMI, APOE ɛ4 allele, the presence of hypertension, diabetes mellitus, and dyslipidemia (model 2). Next, we examined whether the effects of HC on cognition differed according to the degree of self-perception of cognitive decline, by performing multiple linear regression analysis in mild SCD participants and in advanced SCD participants. For each regression model, we plotted and checked residuals. Residuals were normally distributed, heteroscedasticity was in conformance with test assumptions, and Durbin-Watson test statistics indicated independence of observations (results not shown). Furthermore, in order to increase the credibility of results, we conducted the same analyses with available ICV data in 79 subjects.
RESULTS
Demographic characteristics
Demographic and clinical characteristics of the total sample and subgroup are presented in Table 1. Of the 149 participants with SCD, 86 (57.7%) were SCD with a low degree of self-perception for cognitive decline and 63 (42.3%) were SCD with a high degree of self-perception for cognitive decline. The mean age was 65 (63–68) years old, 68.5% of subjects were female, and the mean years of education were 12 (11–15) in this study. There were no differences between mild SCD and advanced SCD participants in demographic and clinical characteristics except for SCD-Q9. As expected, participants with mild SCD had a lower score of SCD-Q9 (p = 0.000). The proportion of APOE ɛ4 allele carriers in this sample was 23.49%, with 23.3% mild SCD, and 23.8% advanced SCD.
Demographic and clinical characteristics of the study participants
All normally distributed continuous variables in the table were described as mean±standard and non-normally distributed continuous variables were described with the median (interquartile). Mild SCD, subjective cognitive decline with low degree of self-perception of cognitive decline; Advanced SCD, subjective cognitive decline with high degree of self-perception of cognitive decline; BMI, body mass index; HC, head circumference; SCD-Q9, subjective cognitive decline questionnaire; HAMD, Hamilton Depression Rating Scale; HAMA, Hamilton Anxiety Scale; AVLT-H-N5, Auditory Verbal Learning Test-Huashan version long-delayed free recall (20 min); AVLT-H-N7, Auditory Verbal Learning Test-Huashan version long-delayed recognition (20 min); STT-A, Shape Trail Test A; STT-B, Shape Trail Test B; AFT, Verbal Fluency Test (animal); BNT, Boston Naming Test; MES, Memory and Executive Screening; MoCA-B, Montreal Cognitive Assessment-Basic. aThe p value was calculated using Chi-square. bThe p value was calculated using Mann-Whitney U. cThe p value was calculated using independent samples t tests.
Effects of HC on neuropsychological tests
Spearman correlation analysis revealed a modest association between HC and AFT (one of the measures of language) in the total sample (r = 0.23, p = 0.006) but no significant correlation between HC and other cognitive measures (AVLT-H-N5: r = 0.052, AVLT-H-N5: r = 0.076, STT-A: r = –0.085, STT-B: r = –0.073, BNT: r = 0.081, and MoCA-B: r = 0.061, all p > 0.05). Furthermore, multiple linear regression analysis (unadjusted) revealed a positive effect of HC on AFT (β= 0.66, 95% CI = 0.233;1.087, p = 0.003; Fig. 2). With adjustment for age, gender, education, BMI, and APOE ɛ4 allele (model 1) and further combining the presence of hypertension, diabetes mellitus, and dyslipidemia (model 2), the positive effect survived (all p < 0.01; Fig. 2).
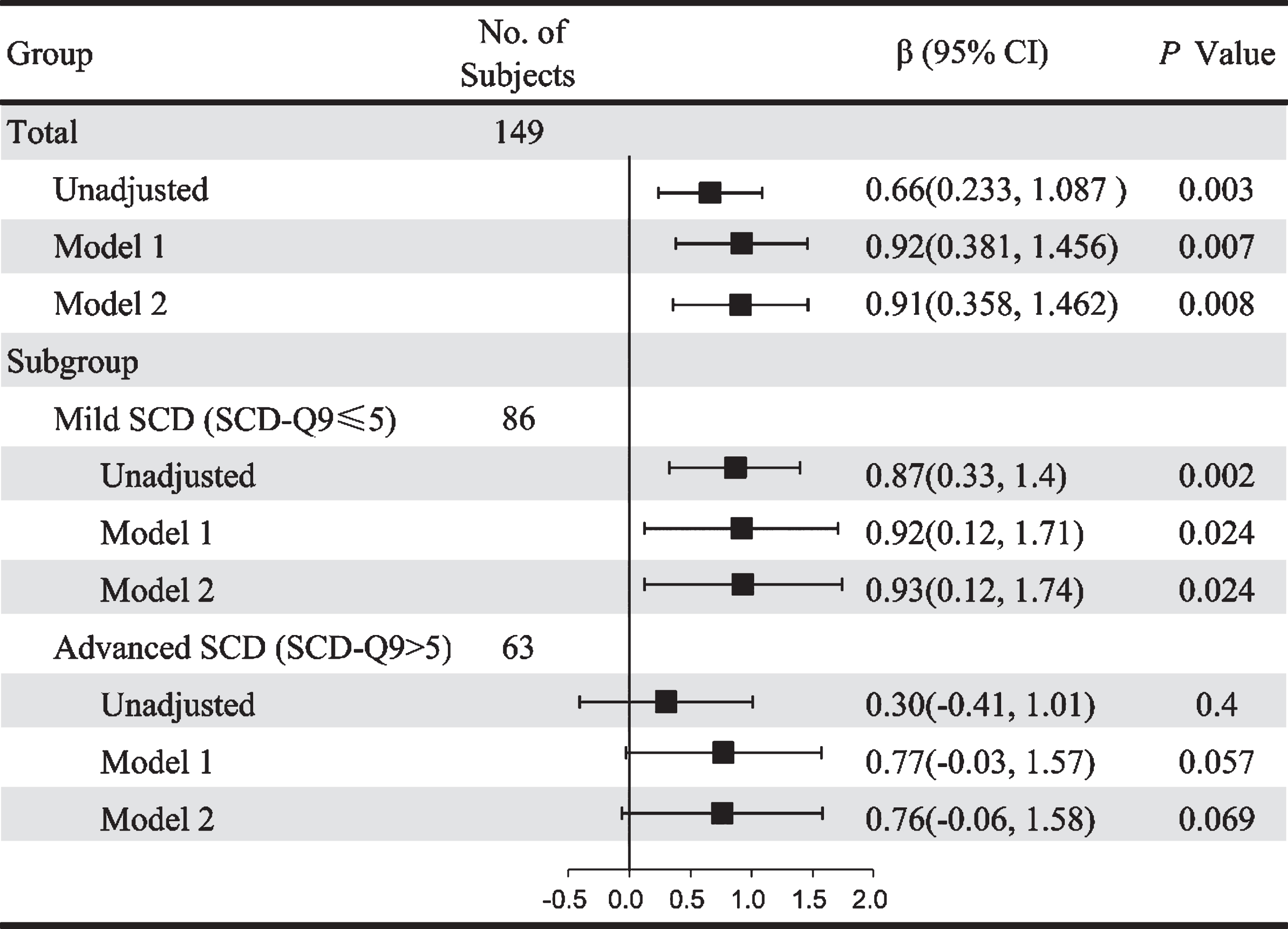
Effects of head circumference on animal fluency test in the total sample and according to the degree of self-perception of cognitive decline. Mild SCD, subjective cognitive decline with low degree of self-perception of cognitive decline; Advanced SCD, subjective cognitive decline with high degree of self-perception of cognitive decline; SCD-Q9, subjective cognitive decline questionnaire; β, partial regression coefficients; CI, confidence interval. Model 1: adjusted for age, gender, education, BMI, and APOE ɛ4 allele. Model 2: adjusted for age, gender, education, BMI, APOE ɛ4 allele, the presence of hypertension, diabetes mellitus, and dyslipidemia.
Effects of HC on neuropsychological tests according to degree of self-perception of cognitive decline
Next, we stratified the total sample according to the degree of self-perception of cognitive decline (mild SCD versus advanced SCD) and performed unadjusted, model 1 and 2 in both SCD subgroups. Multiple linear regression analysis with unadjusted showed a positive effect of HC on AFT (β= 0.87, 95% CI = 0.33;1.4, p = 0.002; Fig. 2), and model 1 found a positive effect of HC on AFT in mild SCD group (β= 0.92, 95% CI = 0.12;1.71, p = 0.024; Fig. 2). Furthermore, when combining the presence of hypertension, diabetes mellitus, and dyslipidemia (model 2), there was still positive effect in mild SCD group (β= 0.93, 95% CI = 0.12;1.74, p = 0.024; Fig. 2). However, all multiple linear regression analysis (with unadjusted, model 1 and model 2) indicated that there was no significant effect of HC on AFT in advanced SCD group (all p > 0.05; Fig. 2).
The validation results by available ICV data
Due to the lack of MRI data of 70 SCD subjects (unable to use or incomplete), analyses with available ICV data were performed in the remaining 79 subjects. Demographic and clinical characteristics of the 79 subjects and subgroup are presented in Supplementary Table 1. Similar to the results of HC, Pearson correlation analysis revealed a modest association between ICV and AFT in the total sample (r = 0.307, p = 0.006) but no significant correlation between ICV and other cognitive measures. Multiple linear regression analysis revealed a positive effect of ICV on language cognition in subjects with SCD and the positive effect of ICV on language cognition survived in SCD participants with low degree of self-perception of cognitive decline while disappeared in SCD participants with high degree of self-perception of cognitive decline (Supplementary Figure 1).
DISCUSSION
The goal of this study was to examine the effects of BR on cognition in SCD subjects and whether these effects were modulated by the degree of self-perception of cognitive decline. The main findings of our study are 1) BR has a positive effect on language cognition in participants with SCD, and 2) the positive effect of BR on language functioning was survived for mild SCD participants while not in advanced SCD participants after subgroup analysis.
At present, although literature concerning the relationship between BR and SCD is relatively scarce, the protective effects of BR on cognition in this study align with a previous study [15]. They demonstrated that BR (as measured with ICV) has positive effects on all cognitive domains such as memory, attention, visuospatial, and executive functions in predementia (SCD + MCI) and AD dementia participants with positive AD biomarkers, except for the language. Furthermore, when the sample were stratified by disease stage (dementia versus predementia), they found that BR differentially impact on cognitive domains, as BR has positive effects on executive function in predementia (SCD + MCI) participants and attention, executive function, and visuospatial ability in AD dementia participants. On the contrary, the positive effect of BR on cognition was limited to language in our study. An explanation for the inconsistent results in the present study in comparison to the previous study could be relate to differences in study methodology, cohort characteristics, sample size, and in how well other confounding factors are accounted for in the analyses. In our study, we evaluated the objective cognition of SCD by Jak/Bondi criteria [34], measured BR by HC, did not include AD biomarker, and the sample size was relatively small. However, they evaluated the objective cognition of SCD by Petersen’s criteria [35], measured BR by ICV, included a sample covering the spectrum from SCD, MCI, to dementia with AD biomarker and the sample size was relatively large. In any case, our results extend to demonstrate that BR has a beneficial effect for cognition of SCD populations who have more hazards developing AD.
In the present study, we further addressed the question that whether the degree of self-perception of cognitive decline (as measured with SCD-Q9) modified the positive effect of BR on cognitive performance in SCD subjects and reported that higher degree of self-perception of cognitive decline (SCD-Q9 > 5) disappeared the positive effect of BR on cognitive performance. SCD-Q9 is a tool for SCD screening and contains nine questions which are characterized by different SCD domains, such as global memory functioning, temporal comparisons, and items querying the individual’s ability to complete daily or routine activities. Endorsement of these questions has been linked to smaller medial temporal lobe volumes or amyloid positivity [36, 37]. It was widely held that SCD changes dynamically in the course of AD, and SCD could become increasingly intense in preclinical AD with increased amyloid pathology [38]. Indeed, our previous studies have confirmed that SCD-Q9 can also be applied in Chinese SCD subjects and the scores of SCD-Q9 significantly increased across the spectrum of AD [23, 39]. Accordingly, we speculated that BR exerting beneficial effects on cognition is limited to mild SCD due to light neuropathologic burdens of AD. However, we did not employ AD biomarkers to reflect pathological changes in this study and this issue will be explored in our future studies.
The present study has its limitations. It was a relatively crude method that HC was employed to measure BR (numbers of neurons and synapse) as HC mainly reflect premorbid brain size and is broadly accepted as a surrogate for maximal adult brain size. Thus, HC may not really reflect the real size of the current brain volume. However, the findings of this study were consistent with the validation results by ICV data. Furthermore, the study had a relatively small sample size and this may affect the accuracy of results. Hence a larger sample is needed to verify the results of the study. Moreover, the present study was a cross-sectional study and longitudinal follow-up studies are needed to confirm whether BR provides a buffer against the progression of cognitive decline in SCD populations.
In conclusion, our results indicate that BR (as measured by HC) has the potential to delay or slow down cognitive decline in SCD individuals, especially for SCD individuals with low degree of self-perception of cognitive decline. Therefore, it is important that improvements of prenatal and early life conditions including nutrition, CNS infections and inflammations, and perinatal brain injury to promote optimal neural development and could increase BR in population, which in turn may help protect against the effects of AD.
Footnotes
ACKNOWLEDGMENTS
This article was supported by The National Key Research and Development Program of China (2016YFC1306300, 2018YFC1312001), National Natural Science Foundation of China (61633018, 81801052, 81601454), Beijing Municipal Commission of Health and Family Planning (PXM2020_026283_000002), and China Postdoctoral Science Foundation 2018M641414.