
Abstract
White matter hyperintensities (WMH) is mainly caused by cerebrovascular injury and may also increase the possibilities of progression to Alzheimer’s disease. The present study aims to determine whether plasma neurofilament light (NFL) protein levels could predict the progression of WMH volume in elderly persons without dementia. The present study enrolled 1029 non-dementia participants from the Alzheimer’s Disease Neuroimaging Initiative in which all had measurements of plasma NFL and WMH at baseline and 589 had longitudinal measurements during follow-up. Spearman correlation analyses and regression models were used to assess cross-sectional and longitudinal associations between plasma NFL and WMH. Plasma NFL concentration had a moderately strong correlation with WMH at baseline (r = 0.17, p < 0.001). Longitudinal analyses showed that higher baseline plasma NFL concentration was associated with accelerated progression of WMH (β=0.015, p = 0.007). Furthermore, higher change rates of plasma NFL could predict faster progression of WMH in the future (β=0.581, p = 0.002). The results of the study suggest that plasma NFL level might be used as a noninvasive biomarker to track variation trend in WMH in elderly persons without dementia.
Keywords
INTRODUCTION
White matter hyperintensities (WMH) are regions of increased signal on T2-weighted and fluid-attenuated inversion recovery (FLAIR) MRI sequences in the brain. WMH volume is highly associated with aging, vascular risk factors, early mortality, frailty, and depression [1, 2], and it may also increase the possibilities of progression to Alzheimer’s disease (AD) [3, 4]. High-resolution neuroimaging techniques visualize the structural and functional changes in the aging brain and also provide evidence to define the disease state [5]. WMH on magnetic resonance imaging (MRI) reflect regionally distributed small vessel cerebrovascular lesions. Independent of two recognized AD biomarkers, tau [6] protein and hippocampal atrophy [7], WMH may contribute to susceptibility to AD via an additional degenerative mechanism. Previous studies have proposed a hypothesis that the mechanism underlying the role of small vessel cerebrovascular lesion in the progression of neurodegeneration may be its interaction with the published AD marker—medial temporal lobe atrophy [8]. Though the mechanisms are still unclear, what is clear is that WMH contribute to rapid progression in the early stage of neurodegeneration. Risk factors for WMH have been established and they are controllable through lifestyle or pharmacological intervention [8]. Therefore, an available and reliable marker is warranted to monitor the further status of WMH, which might lead to an increased risk of adverse outcomes.
Plasma neurofilament light protein (NFL) is known as a potential and sensible blood-based neuronal injury marker, which increases with cerebrospinal fluid NFL [9]. Previous studies have aliso reported that symptoms of most neurodegenerative diseases manifest as NFL accumulation, indicating a potential prognostic role of neurodegenerative diseases [10]. Estimation of plasma NFL levels can be achieved through ultrasensitive single-molecule array in laboratory [11] which is relatively more accessible and inexpensive compared with other cerebrospinal fluid and neuroimaging biomarkers, especially if serial measurement is needed. At present, the association between plasma NFL and WMH has been investigated scarcely and also there is a lack of strong evidence. The purposes of the present study are to determine whether plasma NFL is a reliable predictor of WMH, to validate the hypothesis that longitudinal plasma NFL affects the change in WMH volume in non-dementia elders, and to explore monitorable avenues for prevention or treatment of rapid-progressing course.
METHODS
ADNI study design
Data were obtained from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (http://adni.loni.usc.edu). The ADNI began in 2003 under the leadership of Dr. Michael W. Weiner, MD. The ADNI participants have been recruited from more than 50 sites across the United States and Canada. For the present study, the data we used were collected from December 16, 2005, to May 2, 2019. Regional ethical committees of all institutions approved the ADNI study. All study participants gave written informed consent.
Participants
The present cohort consisted of all cognitively normal (CN) individuals and mild cognitive impairment (MCI) patients with baseline or longitudinal plasma NFL samples and more than one WMH follow-up spcan. Inclusion and exclusion criteria have been described previously [12]. All ADNI participants were aged 55 to 90 years, had completed at least 6 years of education, were fluent in Spanish or English, and had no significant neurologic disease other than AD. The CN participants had a Mini-Mental State Examination (MMSE) score of 24 or higher and a Clinical Dementia Rating (CDR) score of 0. The MCI group reported an MMSE score of 24 or higher, objective memory loss tested by delayed recall of the Wechsler Memory Scale (WMS) logical memory II, a CDR score of 0.5, preserved activities of daily living, and absence of dementia. Patients with AD dementia who fulfilled the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer Diseases and Related Disorders Association criteria for probable AD [13], reported MMSE scores of 20 to 26, and had CDR scores of 0.5 to 1.0 were excluded in the present study. Therefore, the main analyses were conducted in non-dementia individuals.
Plasma NFL
Plasma NFL wuas measured using an NFL kit (NF-Light, Uman Diagnostics) and transferred onto the single-molecule array platform (Quanterix Corp) through an in-house ultrasensitive digital immunosorbent assay [14]. The assay uses a combination of monoclonal antibodies, and purified bovine NFL as a calibrator. All samples were measured in duplicate. Analytical sensitivity was <1.0 pg/ml. The lower limit of quantification was 6.7 ng/L, and the upper limit of quantification was 1620.0 ng/L. All samples were measured within the range spanned by the limits of quantification. For the low concentration quality control sample of 5.20 ng/L, the intra-assay coefficient of variation was 6.2% and the inter-assay coefficient of variation was 9.0%, and for the high-concentration quality control sample of 185.4 ng/L, the intra-assay coefficient of variation was 4.9% and the inter-assay coefficient of variation was 7.2%. The measurements were performed from January 1 through April 1, 2018, by a board-certified laboratory technician using a single batch of reagents.
WMH quantification
Previous essays have described the quantification of WMH in detail [15, 16]. Structural brain images were acquired using 1.5-Tor 3-T MRI scanners with T1-, T2- weighted MRI scans using a sagittal volumetric magnetization-prepared rapid gradient echo sequence [9] and were coregistered and skull-stripped [17]. Volume of WMH was quantified in minimum deformation template space according to every voxel (based on corresponding proton density, T1 and T2 intensities), prior probabilities of WMH and the conditional probabilities of WMH based on the presence of WMH at adjacent voxels [8]. The total WMH volumes were products of labeled voxels and voxel dimensions and were quantified at baseline and 6, 12, 24, 36, 48, 60, 72, 84, and 96 months.
Statistical analysis
Before analyses, outliers located±3 standard deviation (SD) were excluded according to baseline NFL levels. Wilcoxon test was used to assess the differences in continuous variables between the MCI and CN groups. We tested the cross-sectional associations between baseline WMH volume and baseline plasma NFL concentration using the Spearman rank correlation. The correlation between longitudinal plasma NFL concentration and longitudinal WMH volume was evaluated by computing the Spearman rank correlation between individual-specific random slopes from linear mixed-effects (LME) models of NFL concentration and random slopes from LME of WMH volume. We tested LME models with longitudinal WMH level as the outcome variable. The model includes random intercepts and slopes for time and an unstructured covariance matrix for the random effects and regards the interaction between time and NFL, as well as interaction between time and change in NFL as predictors, other confounding variables including diagnosis, ApoE4 genotypes, and demographic factors. We stratified patients by baseline NFL concentration into quartiles and repeated the LME models for associations between WMH and NFL quartiles. LME models were carried out for different diagnostic groups separately. We used marginal R2 to present the linear mixed-effect models which could explain the proportion of the variance in the fixed effects. In addition, we draw mediation models to further investigate the role of NFL level in WMH progression and cognitive decline in all participants. The ADNI memory composite score (ADNI-Mem), the ADNI executive function score (ADNI-EF), MMSE, and CDR scales were used in the analysis.
Statistical significance was set at p < 0.05. All regression analyses were adjusted for age, sex, education, ApoE4 genotypes, and intracranial volume. And the analysis for the overall population was also adjusted for diagnosis. Time was treated as a continuous variable. All statistical analyses were performed using the R programming language, version 3.6.0 (R Foundation), with LME analysis performed specifically using the lme4 package, version 3.1.
Demographic characteristics of study participants at baselines
Baselinea: 1029 participants measured only baseline plasma NFL; Baseline & longitudinalb: 589 participants measured both baseline and longitudinal plasma NFL. NFL, neurofilament light protein; WMH, white matter hyperintensity; ApoE, apolipoprotein E.
RESULTS
We measured the baseline NFL of 1,029 non-dementia participants, including 675 MCI subjects (341 in late-MCI stage, 258 in early-MCI stage, and others were not divided) and 354 CN controls. And more than one follow-up data of WMH were incorporated in the study. There were 589 participants measured annually up to 10 years after the baseline NFL examination. The demographic and biomarker characteristics are shown in the Table 1. Every participant had more than one measurement of WMH. The longitudinal data of WMH in 1029 participants were recorded with a median 4.6-year follow-up (range, 0.5–9), and in the 589 participants data were collected with a median 5.6-year follow-up (range, 1–10). In the 1,029 participants, baseline plasma NFL (mean, 34.3 versus 30.8, p = 0.003) and WMH volume (mean, 2.41 versus 0.98, p < 0.001) were significantly increased in patients with MCI compared with CN individuals. In the 589 participants, WMH volume (mean, 3.33 versus 2.40, p < 0.001) and plasma NFL (mean, 32.2 versus 30.8, p = 0.262) were also elevated, though there is a lack of statistical significance in the NFL increase.
Baseline plasma concentration NFL and WMH
Baseline plasma NFL concentration had a moderately strong correlation with baseline WMH (r = 0.17, p < 0.001, Fig. 1A). At baseline, higher NFL and WMH both correlated with diagnosis (r = 0.198, p < 0.001 with WMH; r = 0.077, p = 0.003 with NFL concentration) and age (r = 0.120, p < 0.001 with WMH; r = 0.297, p < 0.001 with NFL concentration). Using multiple mixed-effects models, we tested associations between baseline NFL and the longitudinal changes of WMH after adjusting for age, gender, education level, ApoE4 genotypes, and intracranial volume (diagnosis was also adjusted in all participants). Table 2 summarized the associations between baseline variables and longitudinal change of WMH. The analysis demonstrated that higher plasma NFL concentration was correlated with the longitudinal deterioration of WMH in all participants (β=0.015, p = 0.007) and in CN group (β=0.019, p = 0.034), rather than the MCI group (β=0.010, p = 0.141). Supplementary Table 1 showed that the correlation was also not significant in the early-MCI group (β<0.001, p = 0.060) and the late-MCI group (β=0.002, p = 0.716).
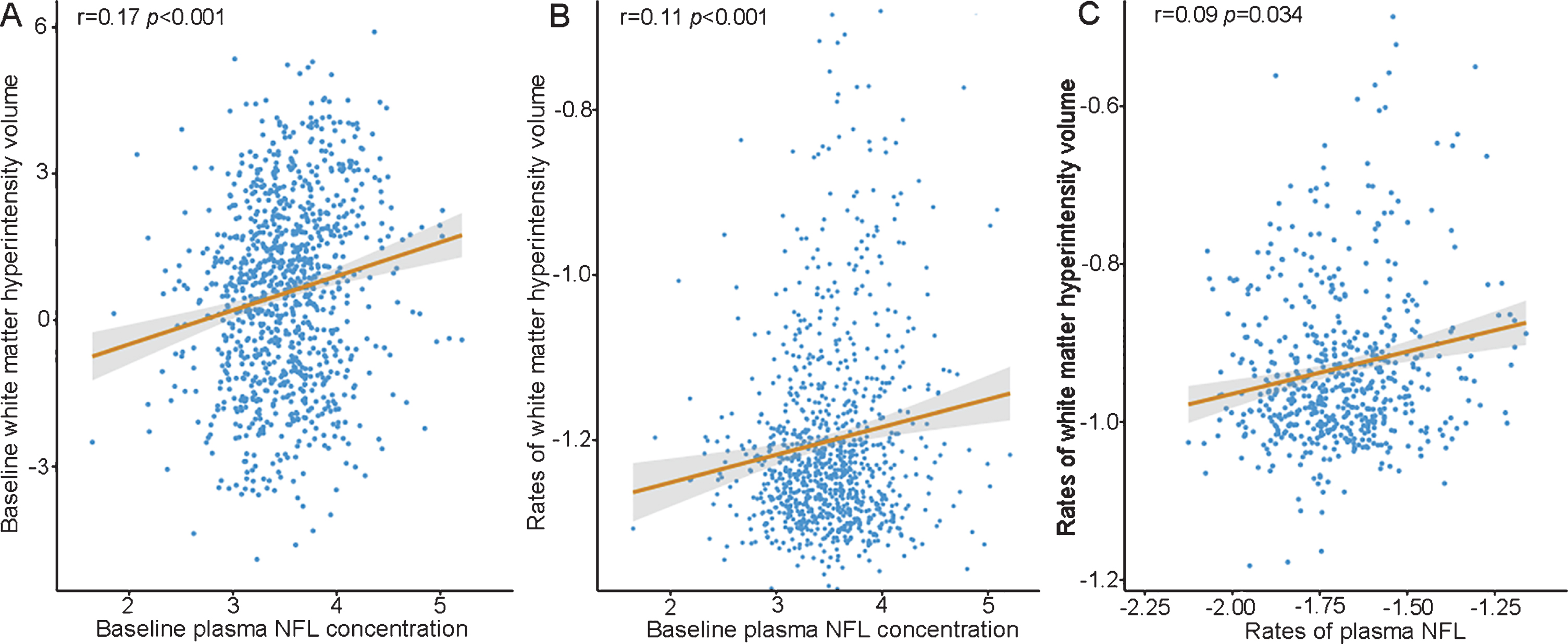
The correlation between plasma NFL concentration and WMH volume. Baseline plasma NFL concentration is related with baseline WMH in 1,029 participants (1A); Baseline plasma NFL concentration is related with rate of WMH in 1,029 participants (1B); Rate of plasma NFL concentration is related with rate of WMH in 589 participants (1C); The Spearman r and p are for Spearman rank correlation in the whole cohort. Baseline and rates of plasma NFL and WMH volume were log-transformed.
Baseline and rate of plasma NFL associated with longitudinal WMH volumes in multiple linear mixed-effects models
NFL, neurofilament light protein; Rate, the change rate of NFL; WMH, white matter hyperintensity; ICV, were tested in multiple linear mixed-effects models adjusted for diagnosis in all participants.
All study participants were divided into four quartiles according to their baseline plasma NFL concentration. Comparing with the lowest quartile, the third (β=0.031, p = 0.039, 95% CI = 1.00–1.06) and the forth (β = 0.032, p = 0.041, 95% CI = 1.01–1.06) quartiles were both associated with increased WMH extent (Fig. 2A). The association was almost identical in CN group. Each Z score unit increase of plasma NFL in the highest quartile (β = 0.063, p = 0.024, 95% CI = 1.00–1.12) was associated with an increased severe result of WMH, compared to the lowest quartile (Fig. 2B). In contrast, no quartile of plasma NFL was associated with the progression of WMH in MCI group (Fig. 2C), compared to the lowest quartile (β = 0.021, p = 0.236, 95% CI = 0.98–1.05 for the second quartile; β = 0.018, p = 0.308, 95% CI = 0.98–1.06 for the third quartile; β = 0.024, p = 0.183, 95% CI = 0.99–1.06 for the forth quartile), but interestingly, there is no significant association between quartiles and WMH in late-MCI group (Supplementary Figure 1A), but the third (β = 0.538, p = 0.004) and the forth (β = 0.397, p = 0.035) quartiles in the early-MCI stage (Supplementary Figure 1B) were both significantly associated with WMH. The results also showed a positive correlation between baseline plasma NFL and the change rate of WMH volume (r = 0.111, p < 0.001, Fig. 1B). In the mediation models, WMH was mediator between NFL and the ADNI-EF scale (Proportion of mediation = 5.2%, p < 0.001) and the CDRs (Proportion of mediation = 3.1%, p = 0.04) in all participants, indicating that WMH may mediate the NFL-related cognitive decline. As for ADNI-Mem and CDR scales, the mediation models were not established.
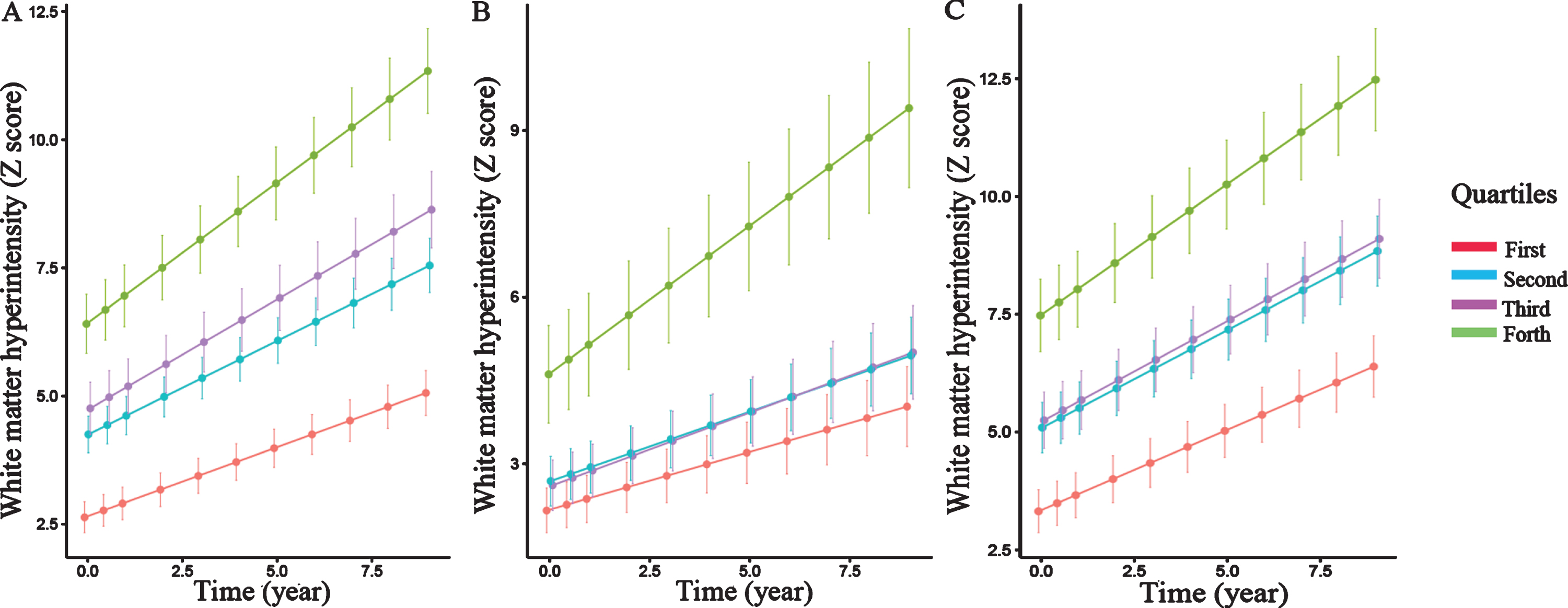
WMH volumes in quartiles of baseline plasma NFL level. Individuals with the highest quartile showed faster rate of WMH increases in all participants (A), CN participants (B), and MCI participants (C). Data from linear mixed-effect models adjusted for age, sex, educational level, ApoE4 genotype, intracranial volume, and diagnosis.
In additional analyses, we examined the interactions of plasma NFL concentration and age in all participants and MCI group, and the results (p for interaction = 0.281 for all participants; p for interaction = 0.932 for MCI group) showed that age was not an effect modifier for NFL. Adjusting for age also did not alter any of the results.
Longitudinal plasma NFL concentration and WMH
Patient-specific rates of NFL and WMH were calculated. In all the participants, greater rates of NFL were associated with accelerated deterioration of WMH (r = 0.089, p = 0.034). Figure 1C showed the correlation between change in NFL and change in WMH. The multiple mixed-effect models also demonstrated that higher rates of plasma NFL could predict a worse progression of WMH (β = 0.581, p = 0.002 for all participants, β = 1.183, p = 0.002 for CN group), but the relation were not established in the MCI group (β = 0.371, p = 0.105). The LME model had R2 value of 0.09 for the rates of plasma NFL. Age was also an independent risk factor for the change of WMH (95% CI 1.00–1.01, p = 0.018). After adjusting for interaction between NFL and ICV (p for interaction = 0.038 for all participants; p for interaction = 0.065 for MCI group), the results were almost identical as before (β = 0.577, p = 0.002 for all participants; β= 0.364, p = 0.111 for the MCI group).
DISCUSSION
As previous study suggested, ischemic diseases cause severe outcomes as a consequence of neuronal loss [18]. NFL was regarded as a marker of neuroaxonal injury after ischemic diseases with a potential to monitor the subsequent progression [19]. The findings are consistent with the primary hypothesis that the baseline plasma NFL levels may have positive association with baseline WMH and the change in WMH. NFL could predict the gradual deterioration of WMH in non-demented elders. Generally, higher baseline NFL levels predict larger volume of WMH in the future. Stratifying subjects into quartiles by baseline NFL concentrations, NFL had greater value in prediction in higher quartiles. Another result also supported that changes in plasma NFL levels were positively associated with longitudinal changes in WMH. During the long-term follow-up, the greater changes in plasma NFL indicate more increases in the volume of WMH in the future. This finding suggests that plasma NFL is a dynamic biomarker for the progressive aggravation of WMH. The association differed by clinical stage. The primary hypothesis was established in cognitively normal participants, but the association was not significant in MCI participants, especially in the late-MCI participants. The crucial implication is to offer an available noninvasive blood-based method to track longitudinal WMH volume change. Especially in cognitively normal participants, the benefit was more visible. Previous studies have demonstrated that WMH was highly prevalent in cognitively normal older adults [1]. The present study also suggested that it could mediate the NFL-related partial cognitive decline. Therefore, plasma NFL is a convenient and available tool for cognitively normal individuals to understand the future trend of the change of WMH.
The novelty value of the present study was to demonstrate the association between plasma NFL and WMH from baseline and longitudinal aspects. Meanwhile, our study put forward a convincing way to track or predict the further change in WMH through following up plasma NFL. Estimation of plasma NFL levels can be achieved through ultrasensitive single-molecule array in laboratory [11], which is relatively more accessible and inexpensive compared with other cerebrospinal fluid and neuroimaging biomarkers, especially if serial measurement is needed. As the results indicated, the association between plasma NFL and WMH disappeared in MCI participants which maybe explained as follows. NFL in cerebrospinal fluid is a marker of subcortical large-caliber axonal degeneration and it is highly associated with NFL in plasma [20–22]. The growth rate of plasma NFL was faster in AD and MCI individuals compared with CN individuals [23]. A recent study showed that deficiency of white matter microstructural integrity was a good indicator of axonal injury [24]. According to previous community-based studies, WMH volume was elevated in MCI individuals [8] and AD patients compared with CN individuals. Actually, the differences in change rates of WMH between different clinical stages have not been investigated. A previous study showed that WMH, as one of vascular risk factors, did not influence the progression of AD in the symptomatic stage [25]. In MCI individuals, especially in late-MCI stage, as the two markers might increase at different rates, the ability of NFL for tracking the progression of WMH was weakened. In the present study, this ability of plasma NFL was more sensitive in the early-MCI stage compared with the late-MCI participants
As mentioned above, previous findings have also proven that WMH volume was an alternative marker to observe the progression of cognitive decline and could accelerate the progression of neurodegeneration [2, 23]. In addition, previous studies provided evidence that intracranial artery stenosis was associated with the volume of WMH [26] and also proposed that WMH could be a substitutive marker for cerebrovascular diseases. Therefore, predicting the further trend of WMH can help us identify cognitive state and the risk of cerebrovascular diseases [27]. Our study suggested that the predictive ability of plasma NFL for the further progression of WMH was greater. The existing dementia risk models were developed rapidly and more integrated and the selection of risk models should vary according to different populations [28]. Our study demonstrated the association between plasma NFL and extent of WMH, which were both candidate biomarkers for cognitive decline. Further studies could incorporate the combination of two variables into dementia risk models due to their interactions. The validity may be more acceptable in cognitively normal people.
Our study has some limitations. The first limitation is that the conversion from normal cognition to cognitive decline needs a long-term follow-up to testify whether the association differs by clinical stage. In addition, the role of plasma NFL level in cerebrovascular diseases and cognitive decline needs further investigated and their associations need further explanation. At last, only moderate to severe WMH is considered to be associated with cognitive impairment, so further studies should pay more attention to these participants.
In conclusion, the findings suggest that plasma NFL level can be used as a noninvasive biomarker to track variation trend in WMH among non-demented individuals, especially cognitively normal people. The dynamic changes of plasma NFL can be more accurate to predict the further status of WMH. Therefore, plasma NFL concentration may be considered as a candidate method to monitor effects on the progression of WMH.
Footnotes
ACKNOWLEDGMENTS
This study was supported by grants from the National Natural Science Foundation of China (91849126), the National Key R&D Program of China (2018YFC1314700), Shanghai Municipal Science and Technology Major Project (No.2018SHZDZX01) and ZHANGJIANG LAB, Tianqiao and Chrissy Chen Institute, and the State Key Laboratory of Neurobiology and Frontiers Center for Brain Science of Ministry of Education, Fudan University. Data collection and sharing for this project was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.