
Abstract
Background:
Recent studies showed that type 2 diabetes mellitus (T2DM) may increase the risk of cognitive impairment, but there are few biomarkers to diagnostically discriminate T2DM-associated cognitive impairment and cognitive impairment alone. In this study, we assessed certain cytokines involved in inflammation and vascular diseases and identified special panel of cytokines that could differentiate between T2DM and cognitive impairment.
Objective:
To investigate associations and differences between T2DM and cognitive impairment by cytokines analysis.
Methods:
A total of 264 participants were recruited, their blood samples were collected, and plasma and serum were separated and stored at – 80°C until the assessment of amyloid-β (Aβ)42, Aβ40 and 8 kinds of cytokines by Luminex multiplex assays.
Results:
Plasma Aβ40 is higher whereas Aβ42/40 ratio is lower in cognitive impairment and T2DM-associated cognitive impairment compared to other groups. As compared to health control, YKL-40 level was upregulated in cognitive impairment, PRGN was downregulated in T2DM associated cognitive impairment, OPN was substantially decreased in T2DM, and IL-6 was elevated in cognitive impairment and T2DM-associated cognitive impairment. Interestingly, VEGF and S100B were induced in T2DM when compared with cognitive impairment, and NSE level in T2DM-associated cognitive impairment is significantly lower than in T2DM or cognitive impairment.
Conclusion:
Aβ42, Aβ40, and Aβ42/40 ratio cannot distinguish T2DM-associated cognitive impairment from cognitive impairment. Certain cytokines (YKL-40, NSE, and VEGF) have good performance in distinguishing T2DM-associated cognitive impairment from simple cognitive impairment. Taken together, this may improve the accuracy of the diagnosis and establishment of individualized therapy.
INTRODUCTION
Dementia, including Alzheimer’s disease (AD), mixed dementia (MD), and vascular dementia (VaD) and so many other kinds of dementia, is an age-related disease and affects more than 35 million people worldwide [1]. The number of cases of type 2 diabetes mellitus (T2DM) is also increasing. Cognitive impairment is characterized by memory decline and impaired cognitive function, assessed by the Mini-Mental State Examination (MMSE) and other cognition scales. Cognitive impairment is a transitional state between normal cognitive and AD, and now recognized as a risk factor of AD [2]. The number of people suffering from dementia is increasing and is estimated to reach 135.5 million around the world by the year 2050, while the economic cost due to dementia has exceeded 1 trillion [3].
T2DM is a chronic and heterogeneous disease, marked by hyperglycemia, obesity, and insulin resistance. T2DM is widely spread around the world, likely due to the largest population of old and obese in history, and is still expected to increase over the next few decades [4]. Globally, there are 425 million patients estimated to have T2DM, and by 2040, it is expected that this figure will rise to 642 million [5]. There are plenty of works indicating that T2DM is a risk factor for cognitive decline and dementia [6–8]. A recent meta-analysis of 9,359,005 individuals in 122 studies demonstrated that T2DM is associated with mild cognitive impairment (risk ratio (RR) = 1.49), all-cause dementia (RR = 1.43), AD (RR = 1.43), and VaD (RR = 1.91) [9]. However, the mechanism for this is still unclear. Obesity, inflammation, vascular impairment, aging, insulin resistance, and oxidative stress maybe the major factors linking T2DM and cognitive impairment. Some studies suggest that the metabolic syndrome caused by obesity may destroy the homeostasis system in the brain, leading to brain insulin resistance and resulting in neuron toxicity and neuroinflammation [10]. Additionally, there are studies that found that hyperglycemia could induce blood–brain barrier permeabilization, which contributes to neuronal dysfunction, synaptic loss, and finally cognitive impairment [11].
Studies have shown that many cytokines especially those involved in inflammation or vascular injury show obviously differences in T2DM or cognitive impairment [12, 13]. This may indicate that we could screen several specific cytokine panels and combine them to distinguish T2DM, cognitive impairment, and T2DM-associated cognitive impairment (T2DM & cognitive impairment). Hence in this study, we conducted a cross-sectional study to detect cytokines that are involved in inflammation, neurodegeneration, and vascular injury, to estimate the associations and differences between T2DM and cognitive impairment.
METHOD
Study design
A total of 264 participants were recruited in this study, and all underwent MMSE to definite cognition. The cohort contained 57 controls, 56 with T2DM, 69 with cognitive impairment (MMSE≤26), and 82 with T2DM & cognitive impairment. T2DM was diagnosed according to the 1999 WHO diagnostic criteria: 1) having typical “three more and one less (polydipsia, polyuria, excessive food and weight loss)” symptoms, and having a random plasma glucose level ≥11.1 mmol/L (200 mg/dl); 2) fasting plasma glucose level ≥7.0 mmol/L (126 mg/dl) (fasting for at least 8 h at the time of measurement); 3) plasma glucose concentration ≥11.1 mmol/L (200 mg/dl) 2 h after oral glucose tolerance test. If the patient met one of the above diagnostic criteria in two consecutive days, he/she was diagnosed with diabetes. Clinical characteristics showed there were no differences in gender or age among all groups. All demographic information was collected in the First Affiliated Hospital of University of Science and Technology of China. Blood was collected and centrifuged for 30 min at 4000 rpm. Plasma and serum were isolated and stored at – 80°C until assessed.
This study was approved by the ethics committee of Anhui provincial hospital medical research (approval #89). A written informed consent was obtained from each subject before participating in the study.
Cytokine detection
All cytokines YKL-40, NSE, IL-6, OPN, PRGN, S100B, ICAM-1, VEGF, Aβ40, and Aβ42 were detected by Luminex multiplex assay followed the kit instruction. Briefly, serum/plasma, standards, and control were diluted 1 : 2 by sample diluent provided in the R&D LXSAHM-08 kit or Fujirebio INNO-BIA plasma Aβ forms kit (#REF 81578) then added into wells; diluted beads are also added and incubated for 2 h. Then biotinylated secondary antibodies were added and incubated for 1 h, followed by incubation with streptavidin/R-phycoerythrin for 30 min. The wells were washed 3 times between each step. After removing streptavidin/R-phycoerythrin, the beads were read on the Luminex 200 (Luminex Corporation, TX, USA).
Statistical analysis
Concentrations of cytokines were calculated using GradPad Prism 8.0.1 (GradPad, La Jolla, CA, USA). All the data were presented as Mean±SEM; extreme values were deleted in each group. The distributions of all data sets were evaluated, and these data sets were not normally distributed according to the Kolmogorov-Smirnov test. Mann-Whitney test was used for compare the different data sets and calculate p values. Correlations between different cytokines were performed with Spearman’s coefficient.
RESULTS
Plasma Aβ levels are elevated in two cognitive impairment groups, but cannot discriminate T2DM metabolic syndrome
We recruited 264 individuals and separated them into four groups. The demographic information is shown in Table 1. The cognitive impairment and T2DM & cognitive impairment groups showed lower MMSE scores and years of education year than the others, and there are no significant differences in ages. To distinguish cognitive impairment and T2DM & cognitive impairment, we assessed a panel of cytokines involved in relevant pathologies (Table 2).
Demographic information of all groups
Values are presented as Mean±standard deviation or number (%). T2DM, type 2 diabetes mellitus; MMSE, Mini-Mental State Examination.
Cytokines information
The Amyloid Cascade Hypothesis is the most popular theory, in which amyloid-β protein precursor (AβPP) is cleaved by β-secretase and γ-secretase to produce Aβ40–42 that deposits and form neurotoxic plaques in the brain. Recently, plasma Aβ level was proved to have strong correlations with amyloid-β positron-emission tomography (PET) [14, 15], suggesting it could serve as a potential noninvasive biomarker for AD diagnosis. In this study, we found that plasma Aβ40 level was increased (160.9±5.396 pg/ml, n = 131 versus 144.2±4.475 pg/ml, n = 112; p = 0.04, Fig. 1a), whereas the Aβ42/40 ratio was decreased (0.192±0.004, n = 129 versus 0.206±0.004, n = 107; p = 0.006, Fig. 1c) in the cognitive impairment group compared with the non-cognitive impairment group. But the concentrations of Aβ42 did not show differences among any groups (28.1±1.12 pg/ml, 29.29±1.02 pg/ml, 28.41±0.85 pg/ml, and 29.98±1.27 pg/ml, Fig. 1b), which is consist with previous studies [12]. The results indicated that the Aβ40 levels or the Aβ42/40 ratio only show differences between cognitive impairment or not, but cannot distinguish T2DM & cognitive impairment patients from cognitive impairment cohorts.

Plasma Aβ40 is increased while the Aβ42/40 ratio is decreased in cognitive impairment and T2DM & cognitive impairment groups. a–c) Aβ40 and Aβ42 are detected by Luminex multiplex assay. p values are calculated by Mann-Whitney test performed by GradPad Prism 8.
Inflammation and vascular damage related cytokines differentiated T2DM and cognitive impairment
To screen out factors that could discriminate cognitive impairment and T2DM & cognitive impairment, we analyzed the risk factors related to inflammation, vascular damage, neuroinflammation, and neurodegeneration. Interleukin-6 (IL-6) and osteopontin (OPN) are cytokines involved in many inflammatory processes, and previous studies showed conflicting results of circulating IL-6 levels in patients with AD [16–18]. OPN is reported to have a strong positive correlation with cognition, which may be considered as a biomarker for cognitive impairment or AD [19, 20]. The levels of IL-6 were elevated in the cognitive impairment and T2DM & cognitive impairment groups as expected (3.561±0.647 pg/ml versus 1.945±0.422 pg/ml; 2.880±0.385 pg/ml versus 1.945±0.422 pg/ml; p = 0.04; Fig. 2a). OPN levels were significantly lower in the T2DM patients (12046±1279 pg/ml versus 16245±1625 pg/ml; p = 0.03; Fig. 2b).
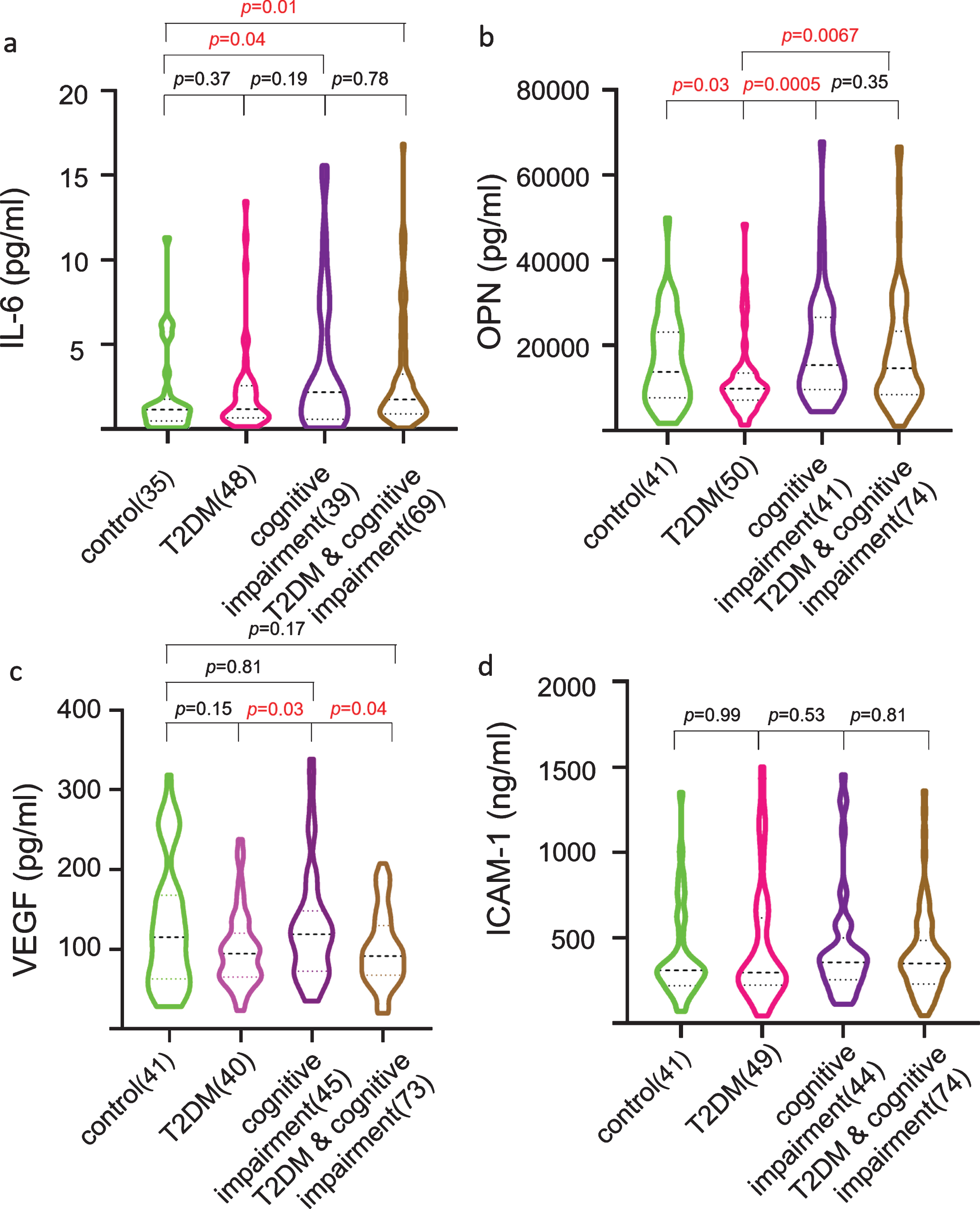
Plasma IL-6 levels are elevated in the cognitive impairment and T2DM & cognitive impairment groups, OPN levels are significantly lower in the T2DM group, VEGF levels are induced in the T2DM patients, while ICAM-1 does not show considerable results among all groups. a–d) Cytokines are detected by Luminex multiplex assay. p values are calculated by Mann-Whitney test performed by GradPad Prism 8.
Intercellular adhesion molecule 1 (ICAM-1) and vascular endothelial growth factor (VEGF) are both involved in vascular problems in AD patients. The level of ICAM-1 is also associated with plaques and neuroinflammation in AD [21, 22]. VEGF plays an important role in angiogenesis and has been suggested involved in vascular injury in both AD and T2DM [23]. We found that the VEGF concentration was significantly reduced in T2DM and T2DM & cognitive impairment groups when compared with the cognitive impairment group (99.25±6.72 pg/ml versus127.5±10.42 pg/ml; 99.91±5.48 pg/ml versus 127.5±10.42 pg/ml; p = 0.03/0.04, respectively; Fig. 2c). The reductive level of VEGF was also observed when compared with control group, but there is no significance. No were no differences among the four groups according to ICAM-1 levels (393836±40909 pg/ml, 449045±50416 pg/ml, 438272±46549 pg/ml, and 405233±29145 pg/ml; Fig. 2d). These results suggest that vascular damage may play an essential role in T2DM-induced cognitive impairment.
Neurodegeneration related biomarkers showed differences in cognitive impairment group with other groups
Progranulin (PRGN) and S100B are both known to play an essential role in neurodegeneration and neuroinflammation [24, 25]. S100B is suggested to be a potential marker of astrocytic damage/re-activation and may contribute to Aβ deposition [26]. PRGN is often regarded as a neurotrophic factor that participates in neuronal injury, studies have shown mutations in PRGN is considered as a cause of FTD, and reduced PGRN levels have been demonstrated to modify the risk of AD [27, 28]. In this work we found that the PRGN level was decreased in the T2DM & cognitive impairment group (34766±1072 pg/ml versus 40209±1711 pg/ml; p = 0.02) (Fig. 3a) compared to control. Meanwhile, S100B in patients with T2DM was lower in patients with cognitive impairment (64.24±6.07 pg/ml versus 95.96±9.85 pg/ml; p = 0.02; Fig. 3b). Interestingly, there was a strong positive correlation between S100B and OPN (r = 0.32, p < 0.0001; Fig. 3c), which implied that S100B may respond to the OPN-related inflammation pathway. These data further validate that the special panel of neurovascular cytokines can differentiate cognitive impairment from normal cognition individuals.
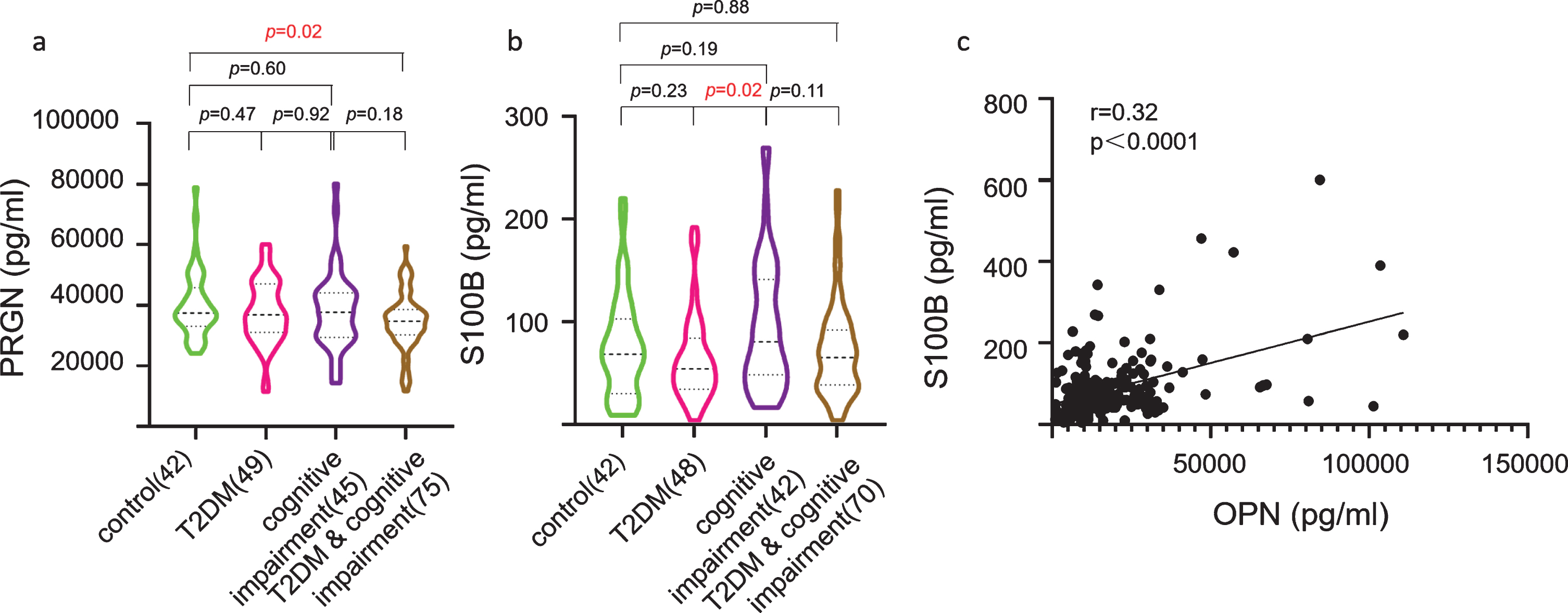
Plasma PRGN levels are significantly decreased in the T2DM & cognitive impairment group, S100B levels show different trends between the T2DM and cognitive impairment groups, and there are strong correlations between S100B and OPN. a, b) Cytokines are detected by Luminex multiplex assay. p values are calculated by Mann-Whitney test performed on GradPad Prism 8. c) Rho and p values are calculated by Spearman’s coefficient performed on GradPad Prism 8.
YKL-40 and NSE are biomarkers for nervous system damage [29], YKL-40 is demonstrated to have strong correlation with age and cognition [29], and studies have shown that NSE is increased as an outcome of neuron injury [30]. In our study, we found that YKL-40 was significantly elevated in cognitive impairment patients when compared with the control group (120133±12262 pg/ml versus 60583±8209 pg/ml; p = 0.0002; Fig. 4a). NSE levels were decreased in the T2DM & cognitive impairment group compared with T2DM or cognitive impairment groups (8345±328.3 pg/ml versus 9522±470.1 pg/ml, 8345±328.3 pg/ml versus 9470±500.3 pg/ml; p = 0.04; Fig. 4b). Meanwhile, strong correlations were observed between YKL-40 and IL-6 or PRGN (r = 0.500, p < 0.0001; r = 0.347, p < 0.0001; respectively), considering that IL-6 is a widely involved cytokine, PRGN may be a better biomarker for neuron damage in the brain. The data suggest that the cytokines involved in nervous system damage can discriminate the T2DM & cognitive impairment group from T2DM group.

Plasma YKL-40 levels are elevated in cognitive impairment group, while Enolase-2 levels show differences compared with the T2DM and cognitive impairment groups. Positive correlations are observed between IL-6 and YKL-40 and PRGN and YKL-40. a, b) Cytokines are detected by Luminex multiplex assay. p values are calculated by Mann-Whitney test performed on GradPad Prism 8. c, d) Rho and p values are calculated by Spearman’s coefficient performed on GradPad Prism 8.
DISCUSSION
To our knowledge, this work is the first to show differences between cognitive impairment and T2DM & cognitive impairment, which has not been addressed before. We found that Aβ levels cannot distinguish the cognitive impairment and T2DM & cognitive impairment groups, whereas certain cytokines showed differences between the T2DM & cognitive impairment group and cognitive impairment group. For instance, YKL-40, NSE, and S100B in the T2DM & cognitive impairment group are even lower as compared to cognitive impairment. Meanwhile, some cytokines like VEGF and OPN are significantly lower in patients with T2DM. The results indicate that we can distinguish T2DM from T2DM & cognitive impairment via the cytokines strictly involved in neuronal or vascular injury but not inflammation. Great performance of cytokines to differentiate these diseases were observed when compared with Aβ, which do not show any differences between the cognitive impairment and T2DM & cognitive impairment groups (Fig. 1).
T2DM and cognitive impairment are both age-related diseases and have many associations between inflammation and vascular impairment which are the two major factors. Chronic inflammation primes macrophages, as well as microglia, to produce IL-1β, IL-6, IL-18, TNF-α and other cytokines and chemokines, which lead acute neuroinflammation in parenchyma, contributing to cognitive decline [31]. Meanwhile, evidence has shown that CSF levels of phosphorylated tau were elevated in T2DM and neuroinflammation is known to facilitate tau hyperphosphorylation [32]. On the other hand, there are many vascular pathologies in T2DM. In addition, T2DM increases the risk of VaD and the factor is higher than any other kinds of dementia [9], which implies that vascular damage maybe the primary cause. In the present study, we found that OPN and VEGF levels were decreased in the T2DM group compared with healthy controls, which confirmed the vascular damage and inflammation conditions in T2DM. Meanwhile, S100B, VEGF, and OPN levels showed differences between the cognitive impairment and T2DM & cognitive impairment groups, indicating that there are different pathological mechanisms underlying cognitive impairment patients with or without T2DM.
Although many previous studies examined T2DM and AD, there are still very few studies focused on the differences or associations between T2DM & cognitive impairment patients and simple disease based on a population study. As we mentioned before, Aβ is not a good biomarker to distinguish T2DM and cognitive impairment. Hence in this study, we detected cytokines involved in inflammation and vascular impairment which may discriminate cognitive impairment from T2DM & cognitive impairment. Our data partly demonstrate that there are strong associations between T2DM and cognitive impairment on some cytokines level. Levels of PRGN and IL-6 showed a similar trend in both diseases, and this may imply that the inflammation levels are similar in T2DM and cognitive impairment and is consist with studies which show that microglia cells are activated and release more cytokines in a female diabetic model [31]. But on the other hand, more differences are observed between cognitive impairment and T2DM & cognitive impairment; for instance, YKL-40, NSE, and VEGF are lower in T2DM & cognitive impairment when compared to cognitive impairment. Thus, our data showed that a specialized panel of certain cytokines may serve as potential biomarkers that help distinguish between different subtypes of cognitive impairment.
At last, there are some limitations must be declared in this study. Firstly, we are unable to accurately differentiate types of dementia or cognitive impairment only by the MMSE score. Secondly, we could not control various potential confounders which may have an association with cognitive impairment and T2DM, such as genetic polymorphism, life habits, education conditions, medication history, and other pathologies. Thirdly, some clinical data were not collected like body mass index, fasting plasma glucose, plasma insulin, blood pressure, and other cognitive tests. Finally, the small sample size and single district of the participants may interrupt the conclusion and limit the final accuracy of conclusion.
Conclusions
Our work indicates that there are close associations between T2DM and cognitive impairment. More importantly, many differences are also observed in cognitive impairment and T2DM & cognitive impairment which has not been examined previously. But traditional biomarkers such as Aβ are unable to discriminate these subgroups. In this work we found that some serum cytokines can serve as potential biomarkers for the discrimination of cognitive impairment and T2DM & cognitive impairment, and may help us to understand the mechanism of these two pathologies, and diagnose and treat patients more accurate. Furthermore, this study implies that cognitive impairment should be accurately differentiated from other pathologies; for example, T2DM may influence the diagnosis and therapy of the patients. It may be necessary for future studies to take this into account.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the National Key Plan for Scientific Research and Development of China (2016YFC1300501 and 2016YFC1300503), the Chinese Academy of Sciences (QYZDY-SSW-SMC012 and XDB39000000), the National Natural Sciences Foundation of China (31530089, 81701255, and 91849103), the Fundamental Research Funds for the Central Universities (YD2070002003), and the Foundation form National Synchrotron Radiation Laboratory.