
Abstract
Background:
Growing evidence has shown the association between ophthalmic disorders and the risk of cognitive decline, but the conclusions were inconsistent.
Objective:
This study aimed to verify the hypothesis that glaucoma or cataract or their combination is associated with incident dementia in Chinese older adults.
Methods:
We followed up 1,659 non-demented community residents aged ≥60 years for an average of 5.2 years in the Shanghai Aging Study. Histories of glaucoma and cataract were collected based on self-report and medical record confirmation. Consensus diagnoses of incident dementia and Alzheimer’s disease (AD) were made based on neurological and neuropsychological assessments.
Results:
During the follow-up, 168 cases (10.1%) of incident dementia and 124 cases (7.5%) of incident AD were identified. Participants with glaucoma at baseline had a significant risk of incident dementia (hazard ratio [HR] = 2.38, 95% confidence interval [CI] 1.08–5.23) and incident AD (HR = 2.77, 95% CI 1.17–6.56) after adjusting for confounders. There was no association between cataract and incident dementia (HR = 1.23, 95% CI 0.85–1.79) or AD (HR = 1.14, 95% CI 0.73–1.77). Those who had both glaucoma and cataract were more likely to develop dementia (HR = 3.08, 95% CI 1.29–7.37) and AD (HR = 3.72, 95% CI 1.52–9.14), compared to those without ophthalmic conditions.
Conclusion:
Glaucoma is an independent risk factor of incident dementia and AD. The comorbidity of glaucoma and cataract may significantly increase the risk of dementia and AD.
INTRODUCTION
According to the Global Burden of Diseases, Injuries, and Risk Factors (GBD) Study 2016, 43.8 million people are living with dementia worldwide [1]. With the acceleration of aging, the number of people living with dementia is estimated to increase to more than 131 million by 2050 [2]. Without the commitment of effective treatment and preventive intervention, dementia is still bringing an enormous burden on the patients, families, and health-care systems around the world. Identification of risk factors and further mechanistic studies are imperative to dementia research.
Glaucoma is a heterogeneous disease characterized by optic nerve head cupping with retinal ganglion cells (RGC) death and visual-field damage [3, 4]. Cataract, featured by the loss of lens transparency, is the leading cause of blindness in low- and middle-income countries [5]. These two ophthalmic diseases are both commonly prevalent in the older population. The prevalence of glaucoma is 3.5% in people aged 40–80 years [3]. For cataracts, the prevalence rate varies from 3.9% in people aged 55–64 years to 92.6% in people aged ≥80 years [5]. There is evidence that patients with Alzheimer’s disease (AD) exhibit optic nerve degeneration and RGC loss and have a significantly increased risk of glaucoma occurrence [6]. It was also reported that more equatorial supranuclear cataracts were found in AD patients than controls [7]. A few population-based studies have investigated the association between glaucoma, cataract, and cognitive decline, but with inconsistent conclusions due to the different study design, sample size, disease definition, and outcome measures [8–18].
The Shanghai Aging Study (SAS) is a longitudinal cohort study with the target population of older adults residing in an urban community [19]. In this study, we intended to verify our hypothesis that glaucoma or cataract or their combination is associated with incident dementia by analyzing the data from the baseline and prospective phase of SAS.
METHODS
Study participants
Based on the government maintained ‘residents list’ at the end of 2009, 3,141 registered residents were recruited from a community in downtown Shanghai, China. The study participants had to meet the following criteria: 1) registered community residents, not live in a nursing home or other institutions; 2) aged 60 years or older; 3) without schizophrenia or mental retardation based on their medical records; and 4) able to communicate and accept physical and cognitive examinations. The detailed information of the study design and the recruitment procedure of SAS has been published elsewhere [19].
This study was approved by the Medical Ethics Committee of Huashan Hospital, Fudan University, Shanghai, China (No. 2009-195). Written informed consent was obtained from all the participants and/or their legal proxy.
Demographic and lifestyle characteristics
At the baseline interview, research nurses collected the demographic and lifestyle information of each participant through an interviewer-administered questionnaire. Demographic characteristics consisted of birthdate, sex, and education years. Cigarette smoking was defined as smoking daily within the past month, and alcohol consumption was recognized if the participant had at least one serving of alcohol weekly during the past year [20]. Height and weight were measured by anthropometry in order to calculate body mass index (BMI). Depression was defined as present if the scores of the Center for Epidemiologic Studies Depression Scale (CESD) ≥16 [21].
Blood or saliva samples were collected from the participants to assess APOE genotype by using the Taqman SNP method [22]. The presence of at least one ɛ4 allele was considered as APOE ɛ4 positive.
Ophthalmic diseases and other medical histories
At baseline interview, ophthalmic diseases of each participant were asked based on a self-report questionnaire with questions as ‘do you have glaucoma or cataract in the past? If so, how long has it been since it was diagnosed?’ Participants were also asked for their medical history, including hypertension, type II diabetes mellitus, and heart diseases (coronary heart disease, valvular heart disease, cardiomyopathy, heart failure, heart rhythm problems). All the medical histories were confirmed by the medical records maintained with the participants [19].
Neurological and neuropsychological assessments and dementia diagnosis
Neurologists conducted the neurological examination to each participant, and the Clinical Dementia Rating (CDR) scale to the guardians to elicit memory complaints of the participants [23].
Neuropsychological tests were administered by the certified study psychometrists. The battery of tests covers the domains of global cognition, executive function, spatial construction function, memory, language, and attention, including 1) the Mini-Mental State Examination (MMSE); 2) the Conflicting Instructions Task (Go/No Go Task); 3) the Stick Test; 4) the Modified Common Objects Sorting Test; 5) the Auditory Verbal Learning Test; 6) the Modified Fuld Object Memory Evaluation; 7) the Trail-making tests A and B; and 8) the Renminbi (Chinese currency) Test. Tests 1 to 4, 6, and 8 were conducted in participants with <6 years of education, and tests 1 to 5 and 7 were conducted in participants with ≥6 years of education. The detailed description and normative data of these tests have been reported elsewhere [24].
Study neurologists and neuropsychologists reviewed the results of all examinations and reached a consensus diagnosis of the cognitive function of each participant [19]. Dementia was diagnosed based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) [25], and AD was diagnosed additionally based on the NINCDS-ADRDA criteria [26].
Follow-up procedure
Dementia-free participants at baseline were scheduled to follow-up from April 1, 2014 to December 31, 2016. Individuals who had one of the following conditions were ineligible to the follow-up interview: 1) deceased; 2) moved away from the original resident place; or 3) having severe mental disorders, vision impairment, hearing or speaking problems and unable to complete the interview and the neuropsychological tests [27]. A face-to-face neurological and neuropsychological evaluation was conducted using the same procedure as the baseline. New-onset dementia and AD cases were determined by the consensus diagnosis with the same method and criteria at the baseline.
Statistical analysis
The mean and standard deviation (SD) were used to describe continuous variables, while numbers and frequencies (%) were used to describe categorical variables. The one-way Analysis of Variance (ANOVA) and Kruskal-Wallis test were used for comparing continuous variables, and the Pearson Chi-square test and Fisher exact test were used for comparing the differences of categorical variables among subgroups.
The incidence of dementia/AD incidence was calculated as the number of new-onset dementia/AD cases divided by the total person-years of follow-up. Proportional-hazards assumption tests (phtest) based on Schoenfeld residuals were conducted before analyzing Cox regression. Cumulative incidence plots of dementia and AD were presented to show the incidence trends in participants with non-disease (non-glaucoma and non-cataract), single disease (glaucoma or cataract), and double diseases (glaucoma and cataract). Cox proportional hazards regression models were used to estimate the adjusted hazard ratios (HRs) for the association of 1) glaucoma with incident dementia/AD; 2) cataract with incident dementia/AD; 3) single disease (glaucoma or cataract) and double diseases (glaucoma and cataract) with incident dementia/AD. The time at risk was estimated as the time from the baseline until the date of follow-up interview when dementia was diagnosed or administrative censoring at the last follow-up interview. Confounders adjusted in the multivariate Cox regression models were age, sex, years of education, APOE ɛ4, baseline MMSE, cigarette smoking, alcohol consumption, hypertension, diabetes mellitus, BMI, depression, heart disease, and glaucoma or cataract accordingly.
All p values and 95% confidence interval (CI) were estimated in a two-tailed fashion. Differences were statistically significant at p < 0.05. Data were analyzed using Stata 15.1 (StataCorp LLC, College Station, USA).
RESULTS
Table 1 shows the baseline demographics, lifestyle, and medical histories of 1,659 participants who were successfully followed up for averagely 5.2 years. At baseline, the prevalence rates of glaucoma and cataract were 2.5% and 37.7%, respectively. Compared to participants with glaucoma or cataract, and non-glaucoma and non-cataract, participants with both glaucoma and cataract at baseline were the oldest (mean = 77.0 years), and had the largest proportion of women (75.9%), hypertension (65.5%), diabetes mellitus (20.7%), and depression (27.6%) (p < 0.05). At follow-up, the MMSE scores were 27.1 (SD = 3.7), 26.0 (SD = 4.7), and 25.8 (SD = 4.8) (p < 0.001) in participants with two ophthalmic diseases (glaucoma and cataract), single ophthalmic disease (glaucoma or cataract), and without glaucoma and cataract, respectively. Totally, 168 cases (10.1%) of incident dementia and 124 cases (7.5%) of incident AD were identified. Significant difference of the cumulative incidence of dementia and AD was found among the three groups (Fig. 1).
Demographics, lifestyle, and medical histories of study participants at baseline and follow-up
*Comparison among the three groups.
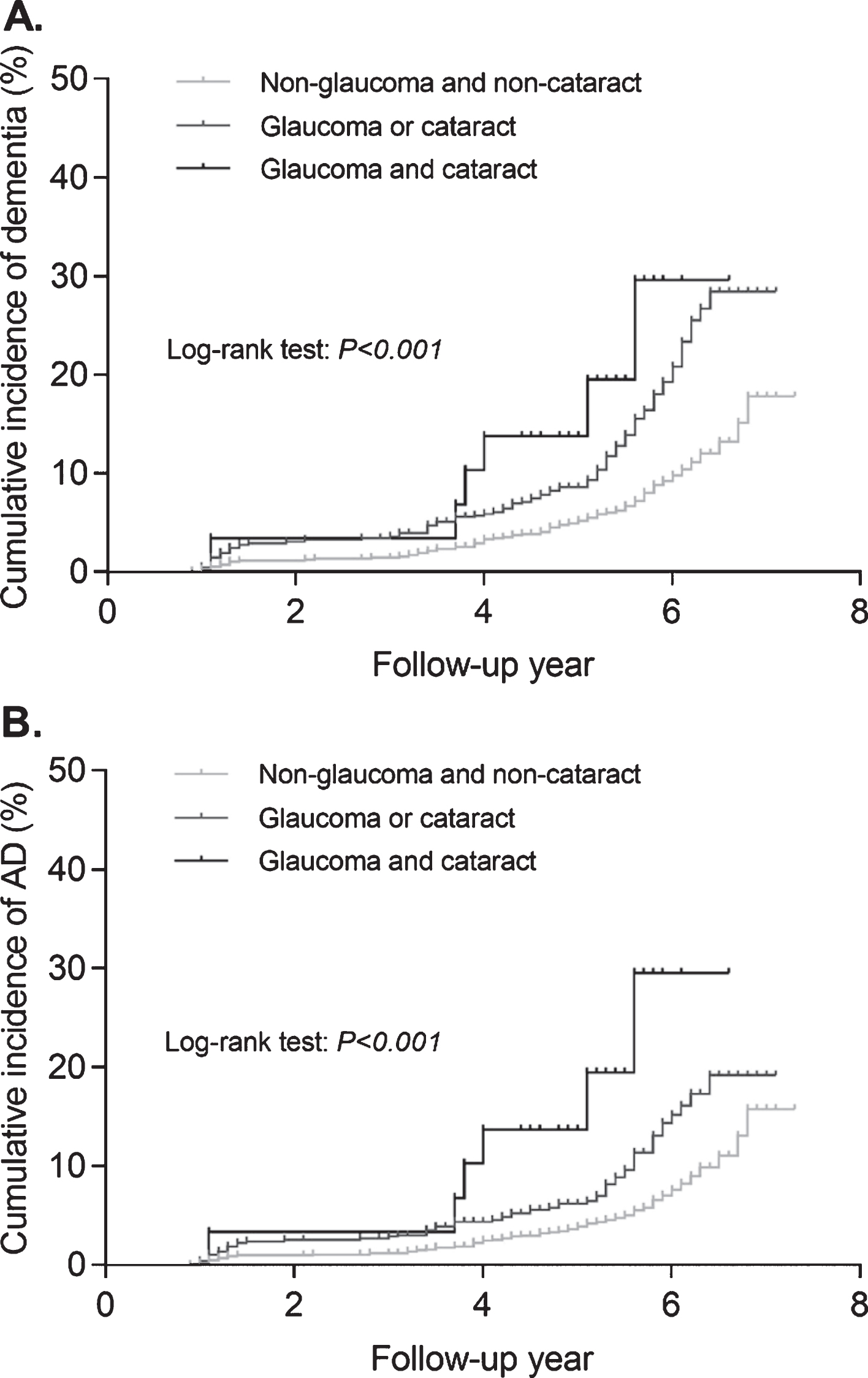
Cumulative incidence plots of dementia (A) and AD (B) in participants with non-glaucoma and non-cataract, glaucoma or cataract, and glaucoma and cataract.
As shown in Table 2, the incidence rates of dementia and AD in participants with glaucoma were 3.4 (95% CI 0.9–6.0)/100 person-years and 2.9 (95% CI 0.6–5.3)/100 person-years, respectively. The incidence rates of dementia and AD in participants with cataract were 2.9 (95% CI 2.4–3.5)/100 person-years and 2.1 (95% CI 1.6–2.6)/100 person-years, respectively. Glaucoma was significantly associated with a higher risk of incident dementia (HR = 2.38, 95% CI 1.08–5.23, p = 0.031) and AD (HR = 2.77, 95% CI 1.17–6.56, p = 0.021) after adjusting potential confounders. However, no significant association was found between cataract and incident dementia and AD. Besides, the incidence rates of dementia and AD in participants with both glaucoma and cataract were 4.2 (95% CI 0.8–7.6)/100 person-years and 4.2 (95% CI 0.8–7.6)/100 person-years, respectively. A higher risk for incident dementia (HR = 3.08, 95% CI 1.29–7.37, p = 0.011) and incident AD (HR = 3.72, 95% CI 1.52–9.14, p = 0.004) was found in participants with both two ophthalmic diseases, but not in those with single ophthalmic disease (glaucoma or cataract) in two multivariate models.
Adjusted hazard ratios of incident dementia and incident AD in participants with different ophthalmic disease condition
Model 1 *adjusted for age, sex, education year, APOE ɛ4, baseline MMSE, and cataract; **adjusted for age, sex, education year, APOE ɛ4, baseline MMSE, and glaucoma; †adjusted for age, sex, education year, APOE ɛ4, and baseline MMSE; Model 2 additionally adjusted for cigarette smoking, alcohol consumption, hypertension, diabetes mellitus, BMI, depression, and heart disease.
DISCUSSION
In this study, we found that participants with glaucoma had a higher risk of all-cause dementia and AD in a 5-year follow-up period after controlling for potential confounders. There was no significant association between cataract and incident dementia/AD. Participants with both glaucoma and cataract were at a higher risk for incident dementia and AD comparing to those without these two ophthalmic diseases. To our knowledge, this is one of a few prospective community-based studies exploring the relationship between ophthalmic disorders and the risk of incident dementia and AD in the non-western population. Consensus diagnoses of dementia and AD were reached by a panel of professionals based on neuropsychological results and detailed clinical data to make the outcome measure more reliable. Furthermore, variables of demographic and lifestyle characteristics and medical histories collected at the baseline can be used to adjust potential confounders in multivariate models.
Several population-based studies were conducted to examine the relationship between ophthalmic disorders and cognitive dysfunction, and the results were inconsistent. Two studies were conducted by the cross-sectional design. In the Beijing Eye Study, comprehensive ophthalmologic examinations were conducted in 3,127 older adults. They found that better cognition function was significantly associated with lower prevalence of primary angle-closure glaucoma (PACG) (β= –0.07) [15]. The Newcastle 85+ Cohort study from UK pointed out that glaucoma was associated with lower standardized MMSE (sMMSE) (odds ratio [OR] = 1.76), but not with MMSE-blind (OR = 1.17), suggesting that the association was driven by poor vision. They also found that treated cataract was related to better cognitive performance in both sMMSE and MMSE-blind [10]. In both studies, cognitive function was measured only based on MMSE scores rather than a clinical diagnosis based on neuropsychological and neurological assessments. Some prospective studies provided the association of ophthalmic disorders with the risk of incident AD and dementia. The Adult Change in Thought (ACT) cohort followed 3,877 participants with total 31,142 person-years. It demonstrated that people with ≤5 years glaucoma diagnosis had an increased risk of AD (HR = 1.46) and all-cause dementia, but not for participants with >5 years diagnosis [14]. However, the association was not found in the cataract diagnosis, which is consistent with our study. Another 3-year study prospectively followed 812 older adults found that participants with open angle glaucoma (OAG) were four times more likely to develop dementia (OR = 3.9). Although they used MMSE and other comprehensive domain-specific neuropsychological tests similar to ours, only suspected participants were assessed by a neurologist [9]. Studies using the Taiwan National Health Insurance Research Database found that the HR of dementia for glaucoma patients was 1.13 [16]; people with POAG had a significantly higher risk of AD (HR = 1.40) [17] and dementia (HR = 1.21) [16]; and people with normal tension glaucoma (NTG) had a higher risk of AD (HR = 1.52) [18]. However, Ou et al. analyzed the Medicare claims data (n = 63,235) and concluded that individuals with OAG had a decreased rate of AD or other dementia, comparing to those without OAG [8]. In addition, Curt Ekström et al. did not find an increased risk of AD in OAG patients during a 30-year follow-up [13]. In summary, previous studies did not obtain the consistent results of POAG/PACG/OAG with an increased risk of dementia/AD. Besides study design, genetic or cultural factors of the target population may also induce the diversity of results from different studies. Evidence of the association between ophthalmic disorders and the risk of incident cognitive impairment in the Chinese population has only been reported in Taiwan. Our study provided a unique opportunity to examine this longitudinal association in older community-dwellings living in mainland China.
Some studies demonstrated that vision impairment is a risk factor of dementia or cognitive impairment [28–34]. The Health ABC Study revealed that visual acuity, contrast sensitivity, and stereo acuity impairments were all associated with more annual score declining of the Modified MMSE for 9 years [28]. Zheng et al. found distant visual acuity was related to a declining MMSE score both cross-sectionally and longitudinally over time [29]. The 3C study concluded that moderate to severe near visual impairment was associated with an increased risk of dementia over 0–2 years (HR = 2.0) and 2–4 years (HR = 1.8), and self-reported distance visual function loss was associated with increased dementia risk beyond 4 years (HR = 1.5) [33]. Although glaucoma and cataract are all sight-threatening ophthalmic diseases, we only found a significant association of glaucoma, not cataract, with incident dementia. Our results provide evidence that vision impairment may not be regarded as a confounding factor for the development of dementia.
Several explanations and potential mechanisms support the association between glaucoma and dementia, especially AD. First, some AD-related pathological proteins were found in glaucoma patients. Yoneda et al. reported that a notable decrease of Aβ42 level and a significant increase of tau level was found in vitreous samples of glaucoma patients [35]. Decreased normal tau protein and significantly increased abnormal hyperphosphorylated tau protein (AT8) were also found in the retina of glaucomatous eyes [36]. Second, the theory about cerebrospinal fluid (CSF) and intra cranial pressure (ICP) was raised to explain the relationship between glaucoma and AD. It was reported that both POAG and NTG patients had lower CSF pressure or ICP [37, 38]. Some AD patients also presented with low CSF pressure [39]. Considering low CSF pressure may lead to an abnormally high trans-lamina cribrosa pressure, which could induce glaucomatous optic nerve damage [37, 41], glaucoma may be a kind of ocular manifestation of AD. Third, a common mechanism based on glymphatic system was proposed recently [42]. Some evidence has shown that AD patients had a deficient clearance of Aβ due to the failure of the glymphatic system. Intriguingly, a similar glymphatic system is also present in the retina [43]. Increasing trans-lamina cribrosa pressure mentioned above may also suppress the glymphatic transport, leading to a deficient clearance of Aβ protein and subsequent glaucoma optic neuropathy [44]. Fourth, Helicobacter pylori (Hp) infection was raised as another hypothesis of the linkage between AD and glaucoma [45]. According to this theory, Hp may influence the pathophysiology of glaucoma and AD by promoting platelet and platelet-leucocyte aggregation [45]. Fifth, genetic studies indicated that OPTINEURIN (OPTN) gene was a contributory gene not only in adult-onset POAG, but also in neurofibrillary tangles and dystrophic neurites in AD [46]. The coding protein ‘optineurin’ may be a new common role involved in both glaucoma and AD. Finally, autophagy may play a crucial role in both AD and glaucoma. Jaeger et al. found that autophagy participated in the transport and metabolism of amyloid-β protein precursor (AβPP). The alteration of autophagy could result in AβPP and Aβ accumulation, which would lead to neuronal cell death [47]. It has also been confirmed that autophagy occurs constitutively in RGC, and an increase of intraocular pressure can disrupt the retinal autophagic mechanism through a low expression of two specific autophagy markers [48].
The controversial evidence had been presented for the association between cataract and AD in recent years [7, 49–51]. Goldstein et al. firstly found that Aβ would accumulate in lenses from AD patients. They also saw equatorial supranuclear cataracts in lenses from 9 AD individuals but not in 8 controls [7]. Moncaster et al. found protein aggregation, amyloid formation when synthetic Aβ was incubated with human lens protein [49]. However, Michael et al. draw the opposite conclusion. They did not find detectable Aβ deposition in the lens of AD patients, and concluded that cortical lens opacities have no relationship with the pathology of AD [50, 51]. From their point of view, cataract could not be a predictor of AD, which is consistent with our population-based result.
The current study has some limitations. We excluded individuals with severe vision impairment at the recruitment according to our exclusion criteria. Therefore, our study may have a selection bias because participants with severe glaucoma and cataract could not be recruited to our study. This selection bias could induce an underestimated intensity of the association of glaucoma and cataract to the risk of dementia. Additionally, we collected the history of ophthalmic diseases based on self-reports with confirmation from the medical records instead of ophthalmological examinations by ophthalmologists. Misdiagnoses of glaucoma/cataract was inevitable because mild symptoms of glaucoma/cataract may not be aware by some participants. Lacking ophthalmic examinations obstructed the classification of glaucoma and cataract subtypes, which may relate to different pathophysiological mechanisms. The self-report information may also induce a quite rough “exposure time” which was used for the time-to-event statistical model. Furthermore, in the statistical models, we have adjusted all the potential confounders collected in our study. However, we still might not exclude the possible influence of uncollected confounders, which could be the unique characteristics of participants with glaucoma or cataract, and could also affect cognitive function. Finally, our findings may not be generalized to other areas in China or other countries, since the participants in our study were all Han Chinese living in an urban community in a well-developed metropolis in China.
Conclusion
In conclusion, our study indicates that glaucoma is an independent risk factor of incident dementia and AD. Meanwhile, the comorbidity of glaucoma and cataract may significantly increase the risk of dementia and AD. More evidence is needed to illuminate the mechanisms of the linkage between the ophthalmic disorders and cognitive decline. Whether medication and surgery treatments to ophthalmic diseases have a benefit to cognition in older individuals should also be further studied.
Footnotes
ACKNOWLEDGMENTS
This work was supported by grants of Shanghai Municipal Science and Technology Major Project (2018SHZDZX01) and ZJLab, National Natural Science Foundation of China (81773513), Scientific Research Plan Project of Shanghai Science and Technology Committee (17411950701, 17411950106), and National Project of Chronic Disease (2016YFC1306402).