
Abstract
Background:
Postoperative delirium is associated with adverse postoperative outcomes. However, whether intravenous and inhalation anesthetics are associated with different risks of postoperative delirium remains unknown.
Objective:
We set up to determine the incidence and duration of postoperative delirium in older patients who had surgery under the intravenous anesthetic propofol or the inhalational anesthetic sevoflurane.
Methods:
Participants were patients who had total hip/knee replacements and were randomized to propofol (N = 106) or sevoflurane (N = 103) anesthesia group. The Confusion Assessment Method was employed by investigators who were blinded to the anesthesia regimen to assess the incidence and duration (days of postoperative delirium per person) of postoperative delirium on postoperative days 1, 2, and 3.
Results:
A total of 209 participants (71.2±6.7 years old, 29.2% male) were included in the final data analysis. The incidence of postoperative delirium was 33.0% with propofol anesthesia and 23.3% with sevoflurane anesthesia (p = 0.119, Chi-square test), and we estimated that we would need 316 participants in each arm to detect a potential statistically significant difference. Days of postoperative delirium per person were higher in the propofol (0.5±0.8) anesthesia group compared to the sevoflurane anesthesia group (0.3±0.5, p = 0.049, Student’s t-test).
Conclusion:
This pilot study established a system to compare effects of different anesthetics and generated a hypothesis that propofol trended to have a higher incidence and had longer duration of postoperative delirium than sevoflurane. Additional studies with a larger sample size are needed to test this hypothesis.
INTRODUCTION
Postoperative delirium, one of the most common complications after surgery in older patients [1, 2], has been associated with significantly prolonged hospitalizations [3–5], cognitive impairment [1, 7], functional decline [8, 9], development of Alzheimer’s disease and related dementia [7, 10–12], and increased mortality [1, 14]. Specifically, patients with underlying dementia are 2.5–4.7 times more likely to develop delirium, and patients with delirium face a 12.5-fold increased incidence of newly diagnosed Alzheimer’s disease and related dementias [10–13]. However, the causes and neuropathogenesis of postoperative delirium remain largely to be determined.
Importantly, evidence indicates that the same surgery under different anesthetics may have different incidences of postoperative neurocognitive disorder [15–18]. Specifically, patients who had surgery to treat cancer under sevoflurane anesthesia had a higher risk of developing delayed neurocognitive recovery than those under propofol anesthesia [17]. Additionally, patients who had radical rectal resection surgery under sevoflurane anesthesia had greater severity of postoperative cognitive dysfunction (POCD) than patients who had the same surgery under propofol anesthesia [18]. Patients carrying the ApoE ɛ4 alleles were more likely to develop early postoperative cognitive dysfunction after surgery under isoflurane anesthesia [19]. However, the effect of anesthetic type (e.g., inhalation versus intravenous anesthetic) on the incidence, duration, and severity of postoperative delirium in patients remains largely unknown.
A randomized study showed that laparoscopic surgery under epidural plus sevoflurane anesthesia was associated with a lower delirium rating scale (DRS) score than under epidural plus propofol anesthesia [20]. Previous studies also showed that the incidence of postoperative delirium in patients who had a gastrectomy, colectomy, or rectectomy under epidural plus propofol anesthesia or sevoflurane anesthesia was 6.9% and 26.7%, respectively [21].
Nevertheless, the potential differences in incidence, duration, and severity of postoperative delirium in patients who have surgery under general anesthesia with sevoflurane or propofol remain to be determined. We therefore set up this randomized clinical trial to determine the incidence, duration, and severity of postoperative delirium in older patients who had a total hip replacement (THR) or total knee replacement (TKR) under general anesthesia with sevoflurane or propofol. Notably, there are more than 1 million TKR/THR each year in United States [22]. It is estimated that there will be a significant increase in TKR/THR over the next 15 years, which will bring a heavy economic burden [23, 24]. The long-term objective of our study was to identify the anesthetic(s) associated with shorter duration, lower incidence, and less severity of postoperative delirium in patients. We hypothesized that the patients who had surgery under sevoflurane or propofol anesthesia would demonstrate different incidence duration, and severity of postoperative delirium.
MATERIALS AND METHODS
Ethics approval
This randomized clinical trial was performed exclusively in the Shanghai Tenth People’s Hospital affiliated with Tongji University, Shanghai, China. The hospital has about 3 million outpatients and more than 40,000 surgeries under anesthesia every year. The study protocol was approved by the Human Research Ethics Committee of Shanghai Tenth People’s Hospital, P. R. China (SHSY-IEC-3.0/15-78/01). Written informed consent was obtained from all participants before their enrollment in the study. This manuscript was written according to the applicable CONSORT guidelines.
Patient population
A total of 606 patients scheduled to have an elective THR/TKR under general anesthesia at Shanghai Tenth People’s Hospital were screened from June 2016 to November 2019 for potential participation in the study. Participant inclusion criteria were: 1) age of at least 60 years; 2) scheduled for surgery under general anesthesia; 3) American Society of Anesthesiologists (ASA) class I to III; 4) normal cognitive function at the time of enrollment evidenced by a Mini-Mental State Examination (MMSE) score of more than 24 of 30; 5) Chinese Mandarin as the native language, and 6) having verbal communication capability and writing skills and thus being able to provide informed consent. After reviewing the medical records of the screened patients, individuals excluded from participation were those identified as having: 1) pre-existing delirium assessed according to the Confusion Assessment Method (CAM); 2) prior diagnoses of neurologic diseases (e.g., stroke and Parkinson’s disease) diagnosed by the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10); 3) history of mental disorders (e.g., acute episode of major depressive disorder, schizophrenia, and mental retardation) diagnosed using the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV); 4) impaired vision or auditory function which may affect the assessments, and 5) unwillingness to participate in the study.
After obtaining the signed consent form, all participants were assigned to surgery under either sevoflurane anesthesia or propofol anesthesia by randomization using computer-generated lists. A total of 240 participants were enrolled in the study from June 2016 to November 2019. Among them, 31 participants were further excluded from the study, bringing the total number of participants to 209 (Fig. 1), with 103 participants in the sevoflurane anesthesia group and 106 participants in propofol anesthesia group. There have been no significant changes in surgery or anesthesia practices since the start of the present study.
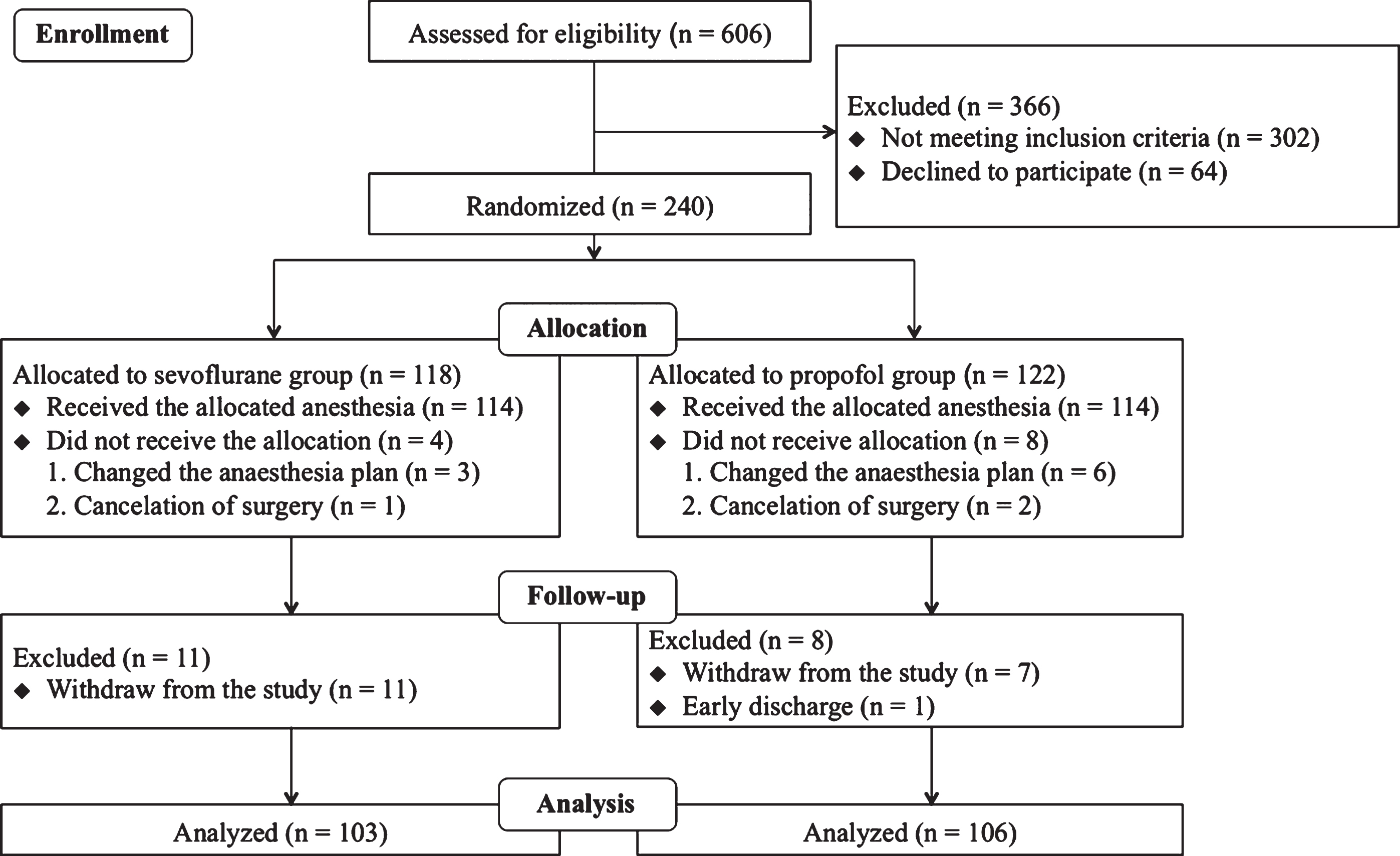
Flow diagram. The flow diagram shows that 606 participants 60 years old and older were screened for the study. A total of 240 participants were enrolled and randomized into the sevoflurane anesthesia group or propofol anesthesia group. Thirty-one participants were further excluded, resulting in 209 participants for the final data analysis.
Randomization
A biostatistician (ZH) who was blinded to the purpose of the study was responsible for randomization of the participants in the study. Specifically, each participant was randomly assigned to the sevoflurane or propofol anesthesia group according to an allocated randomization number (in an established Excel table with a 1:1 ratio and block of 2). The randomized numbers were sealed in sequentially numbered envelopes and stored at the study site. The researcher (XMa) opened the sealed envelope containing the allocation and randomization number one day before assessment of the participants. Preoperative and postoperative interviews were performed by researchers (XM and HLZ) who were blinded to the participants’ anesthesia group assignments.
Preoperative interview
Participants were admitted two to three days before their scheduled surgery. Preoperative assessments were performed one day before the surgery. The assessments included demographic characteristics (e.g., age, gender, height, weight, and years of education) and clinical features [e.g., diagnosis, past medical history, Charlson Comorbidity Index (CCI) scores, type of surgery, anesthesia and surgery duration, Bispectral Index (BIS) values and others]. Preoperative cognitive function was assessed using the MMSE (Chinese version), which has 19 items, and the maximum score is 30 points. The CAM algorithm was performed preoperatively to exclude pre-existing delirium. The Visual Analogue Scale (VAS; ranging from 0 to 10) was used to assess subjective pain before the surgery.
Anesthesia and surgery
All patients received 1–2 mg midazolam preoperatively as part of standard anesthesia care. Propofol 2 mg/kg, sufentanil 0.5–1 μg/kg, and cisatracurium 0.5 mg/kg were used for amnesia, analgesia, and muscle relaxation, respectively. Methylprednisolone (40–80 mg) was administered to every patient to prevent a potential allergic reaction due to the placement of bone cement. Finally, atropine (0.25–1 mg) was given to every patient to reduce airway secretion. Anesthesia was maintained with sevoflurane or propofol and we used the BIS monitor to measure the anesthesia depth. The participants in the sevoflurane anesthesia group received 1% –4% sevoflurane from an anesthesia machine through the endotracheal tube. The participants in the propofol anesthesia group received propofol (629.8±255.0 mg) by target-controlled infusion. Standard anesthesia care was applied, including routine monitoring of the patient’s electrocardiogram (EKG), blood pressure, and oxygen saturation.
All patients had standardized postoperative care. There was no significant difference in the numbers of patient-controlled analgesia (PCA, including sufentanil 100μg and butorphanol tartrate 10 mg dissolved in 100 mL normal saline) pumps used between the participants in the sevoflurane and propofol anesthesia groups. There were no major complications (e.g., heavy bleeding, severe infection, and death) among the participants during the immediate postoperative period (e.g., up to three days after surgery).
Postoperative interview
Each participant was assessed with CAM and the CAM-based scoring system for delirium severity (CAM-S) twice daily between 8:00 am and 10:00 am and then between 4:00 pm and 6:00 pm on postoperative days 1, 2, and 3. The CAM algorithm consists of four criteria: 1) acute onset and fluctuating course, 2) inattention, 3) disorganized thinking, and 4) altered level of consciousness. To diagnose delirium, both the first and second criteria have to be present, as well as either the third or fourth criterion [25]. The incidence (presence or absence) of postoperative delirium was determined by CAM as the appearance of postoperative delirium on any day of postoperative days 1, 2, or 3. The severity of delirium was evaluated by the Chinese version of CAM-S [26]. Specifically, the average CAM-S scores obtained from postoperative days 1, 2, and 3 indicated the severity of postoperative delirium. CAM and the Chinese CAM-S have demonstrated reliability and validity among the Chinese older population. The Chinese version of the MMSE was used on postoperative day 3 to assess postoperative cognitive function. Parts of the MMSE were performed together with CAM on postoperative days 1, 2, and 3. VAS was used for the assessment of subjective pain on postoperative days 1 to 3.
Statistical analysis
Sample size
An estimated sample size of 100 per arm would lead to >80% power to detect a mean difference in the incidence of postoperative delirium between the two cohorts based on the previous studies [17, 21]. The power calculation was performed in the study design phase based on our primary hypothesis that there are differences in the incidence and severity of postoperative delirium between patients having surgery under sevoflurane anesthesia and propofol anesthesia. Our previous studies showed that the rate of drop-out during postoperative assessment was 8.5% [27]. We thus determined that we should enroll 240 participants into the study to have at least 100 participants per arm. Data from these participants would be used for the final data analysis.
Outcome analysis
The primary endpoint was incidence, duration, and severity of postoperative delirium. We compared these variables in the participants who had a THR/TKR under sevoflurane anesthesia and those who had a THR/TKR under propofol anesthesia. The one-sample Kolmogorov-Smirnov method was used to test the normality of all variables. They were generally divided into continuous parameters and categorical parameters. Continuous parameters, including age, body mass index (BMI), years of education, CCI scores, preoperative MMSE scores, postoperative MMSE scores, CAM-S scores, VAS scores, BIS values, blood loss, length of anesthesia, length of surgery and medications were presented as mean±standard deviation (SD). Categorical factors, such as gender, were presented as number and percentage of participants. Continuous variables were analyzed using the Student’s t-test. Categorical variables were analyzed using the Chi-square test or Fisher’s exact test. Outcome and safety data were analyzed in the intent-to-treat population. Specifically, the difference in postoperative delirium duration, incidence and severity between the participants in the sevoflurane and propofol anesthesia groups was analyzed by the Chi-square test and Student’s t-test. Days of postoperative delirium per person were calculated by the average of the days of postoperative delirium in the propofol and sevoflurane anesthesia groups. Two-tailed tests were performed whenever appropriate, and p-values<0.05 were considered statistically significant. Statistical analysis was conducted using GraphPad Prism software (version 6.0) and SAS version 9.4 (SAS Institute, Inc, Cary, NC).
RESULTS
Participant characteristics
A total of 606 participants aged at least 60 years were screened, and a total of 240 participants were initially enrolled. Thirty-one participants were excluded from the study due to changes in anesthesia from inhalational or intravenous anesthetic to the combination of inhalational and intravenous anesthetics (N = 9), surgery cancellation (N = 3), study withdrawal (N = 18), and early discharge (N = 1). In the end, 209 participants were included in the final data analysis (Fig. 1). Demographic variables, including gender, age, years of education, BMI and CCI, and perioperative variables, including ASA classification, blood loss, length of anesthesia, length of surgery, medications, the number of patients who preferred using a patient-controlled analgesia (PCA) pump, and MMSE scores were comparable between the participants in the sevoflurane and propofol anesthesia groups (Table 1).
Characteristics of the study population
Data are presented as mean±SD or number of participants (%). SD, standard deviation; y, year; kg, kilogram; m, meter; mL, milliliter; mg, milligram; μg, microgram; min, minute; CCI, Charlson Comorbidity Index; ASA, American Society of Anesthesiologists; BIS, Bispectral Index; PCA, patient-controlled analgesia; MMSE, Mini-mental State Examination; VAS, Visual Analogue Scale. aBMI was calculated by dividing the patient’s weight by the square of their height.
There was no significant difference in anesthesia depth, determined by BIS, in the participants who had surgery under sevoflurane anesthesia or propofol anesthesia (Table 1). Moreover, there was no significant difference in these variables between the included and excluded participants in the propofol and sevoflurane anesthesia groups (Table 2 and Supplementary Table 1).
Characteristics of the included participants and excluded participants
Data are presented as mean±SD or number of participants (%). SD, standard deviation; y, year; kg, kilogram; m, meter; CCI, Charlson Comorbidity Index; MMSE, Mini-Mental State Examination; VAS, Visual Analogue Scale. aBMI was calculated by dividing the patient’s weight by the square of their height.
Note there was a significant difference in the VAS score on postoperative day 1 between participants in the propofol (4.8±2.4) and sevoflurane anesthesia groups (5.5±2.3): p = 0.038, Student’s t-test, indicating that the participants in the sevoflurane anesthesia group may experience more pain than those in the propofol anesthesia group on postoperative day 1.
The incidence and severity of postoperative delirium in the sevoflurane and propofol anesthesia groups
The overall incidence of postoperative delirium among all participants in the current study was 28.2% (59 out of 209). The incidence of postoperative delirium in the propofol and sevoflurane anesthesia groups was 33.0% (35/106) and 23.3% (24/103), respectively (Table 3). Chi-square test indicated that there was no significant difference in the incidence of postoperative delirium: the relative risk (RR) for sevoflurane versus propofol was 0.706 with 95% CI 0.452 to 1.092, p = 0.119 (Table 3). We estimated that we would need 316 participants in each arm to detect the statistical differences.
Comparison of postoperative delirium incidence and severity in the propofol and sevoflurane anesthesia groups
Data are presented as mean±SD for continuous variables and number of participants (%) for categorical variables. ap-value was obtained using Chi-square test. bp-value was obtained using Student’s t-test. cp-value was obtained using the unpaired Student’s t-test with Welch’s correction.
There was no significant difference in the severity of postoperative delirium (determined by CAM-S) between the participants in the sevoflurane anesthesia group (2.3±1.2) and those in the propofol anesthesia group (2.5±1.2): the mean difference was –0.15 with a 95% CI of –0.373 to 0.175, p = 0.364, Student’s t-test (Table 3).
Duration of postoperative delirium in the propofol and sevoflurane anesthesia groups
However, there was a significant difference in the days of postoperative delirium per person between the participants in the propofol anesthesia group (0.5±0.8) and those in the sevoflurane anesthesia group (0.3±0.5): p = 0.049 (unpaired Student’s t-test with Welch’s correction) (Table 3).
DISCUSSION
There was a 9.7% difference in the incidence of postoperative delirium between the participants in the sevoflurane anesthesia group (23.3%) and those in the propofol anesthesia group (33.0%), although this difference did not reach statistical significance (Table 3). However, there was a significant difference in days of postoperative delirium incidence per person between the propofol and sevoflurane anesthesia groups (Table 3). Taken together, these findings suggest that the study outcomes would be underpowered [28] to demonstrate that patients having THR/TKR under propofol anesthesia have a higher risk of developing postoperative delirium than patients having THR/TKR under sevoflurane anesthesia. We estimate that 316 participants would be required in each group in future studies to detect a true difference in incidence.
These findings differ from those in a previous study [20]. Nishikawa et al. reported that sevoflurane anesthesia was a better choice than propofol anesthesia for the preservation of mental function during the early postoperative period. However, these studies had a longer duration (more than 3 hours) of laparoscopic surgery, used a combination of epidural anesthesia and general anesthesia, and the anesthesia depth between participants in the two groups was not specifically compared. In the current study, however, participants had THR/TKR with an average operation time of 1.5 hours, and had solo general anesthesia with a similar anesthesia depth.
Zhang and colleagues reported that patients who had surgery to treat cancer under sevoflurane anesthesia demonstrated a higher incidence of postoperative cognitive dysfunction at 7 days after the surgery than the patients who had the same surgery under propofol anesthesia [17]. However, their study participants were cancer patients and the endpoint were the incidence of POCD measured at 7 days after the surgery. In our study, the participants were patients with arthritis of the hip or knee, and we assessed the incidence and severity of postoperative delirium on postoperative days 1, 2, and 3.
There have been pre-clinical studies regarding the anesthesia neurotoxicity of sevoflurane and propofol as summarized in our previous review [29]. However, to our knowledge, there have been no animal studies to compare the delirium-like behavior in rodents between propofol and sevoflurane anesthesia. The current results that demonstrated the difference between sevoflurane and propofol anesthesia on postoperative delirium in patients will promote pre-clinical investigation to study the potential difference of sevoflurane and propofol on delirium-like behavior and the underlying mechanisms in rodents.
Previous study demonstrated that propofol might reduce emergence delirium and agitation associated with sevoflurane anesthesia for children having dental rehabilitation [30]. Costi and colleagues also reported that a short time administration of propofol at the end of sevoflurane anesthesia was able to reduce the emergence delirium in children undergoing MRI scans [31]. These results would suggest the beneficial effects of propofol on postoperative delirium. Different findings were obtained in the current study that propofol anesthesia was associated with potentially higher incidence and longer duration of postoperative delirium than sevoflurane anesthesia in the participants. The reason of such difference is not known at the present. However, we determined the incidence and duration of postoperative delirium in the current studies rather than the emergence delirium and agitation as determined in these previous studies [30, 31].
It is possible that the use of midazolam in the participants might contribute to the difference in the incidence and duration of postoperative delirium between the propofol anesthesia and sevoflurane anesthesia in the current study, owing to the different interaction between midazolam and propofol versus midazolam and sevoflurane. Specifically, Kim and colleagues reported that midazolam did not affect the postoperative delirium associated with propofol anesthesia [32] but decreased the incidence of severe emergence agitation among pediatric patients undergoing dental treatment under sevoflurane anesthesia [33]. Therefore, the use of midazolam could be a confounding factor in the current studies. The future research will test this hypothesis by systematically determining the role of midazolam in postoperative delirium.
Note that propofol may need longer time to be eliminated from body than the sevoflurane [34–38], therefore, propofol could have longer duration of residual effects of anesthesia than sevoflurane. We thus hypothesize that this difference in pharmacokinetics between propofol and sevoflurane may contribute, at least partially, to the observed difference of the incidence and duration of postoperative delirium between the participants in the propofol anesthesia group and the participants in the sevoflurane anesthesia group. The future studies to test this hypothesis are warranted.
Although many studies suggest postoperative delirium and POCD usually develop in same trend, a recent study showed different findings that postoperative delirium and POCD may not always overlap [39]. Therefore, postoperative delirium and POCD could be the different manifestations of perioperative neurocognitive deficits. Nevertheless, the difference in participants, time of assessment and types of surgery may also contribute to such different trend of postoperative delirium and POCD observed in current study and the previous study [17]. More research is needed to further determine the association of postoperative delirium and POCD in the future.
There are several limitations in the present study. First, the sample size was relatively small, which might cause the observation of no statistically significant difference in the incidence and severity of postoperative delirium between the participants in the propofol and sevoflurane anesthesia groups. Second, the participants only included patients who had THR or TKR surgery. Future studies may need to include patients who have different types of surgery (e.g., abdominal surgery). Third, we only enrolled participants with a baseline MMSE of more than 24 in the current study, which excluded participants with severe cognitive dysfunction, so the results would not be generalizable to those with cognitive impairment.
In conclusion, we have established a system to compare the effects of different anesthetics (e.g., propofol versus sevoflurane) on the incidence, duration, and severity of postoperative delirium in patients. The current findings suggest that we will need a larger-scale study to test the hypothesis that propofol anesthesia is associated with greater incidence and severity of postoperative delirium than sevoflurane anesthesia. The current study serves as a pilot study and raises novel concerns regarding the use of “bad” anesthesia in individuals who are susceptible to developing postoperative delirium.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank the surgeons and anesthesiologists in the Shanghai Tenth People’s Hospital for help in recruiting the research participants and providing their anesthesia care. This work was supported by funding from the National Natural Science Foundation of China (81720108012, 81571034) to Y.S. and a Henry K. Beecher Professorship from Harvard University to Z.X.