
Abstract
Background:
Synaptopathy is critical in pathophysiology of Parkinson’s disease (PD). Cerebrospinal fluid (CSF) levels of neurogranin (NG) and amyloid-β42 (Aβ42) are considered markers of synaptic dysfunction in neurodegenerative diseases.
Objective:
To evaluate the CSF synaptopathy-related biomarkers, especially the novel Aβ42/NG ratio, in PD, establishing possible associations with cognitive level and other clinical parameters.
Methods:
Levels of NG, Aβ42, amyloid-β40, total and phosphorylated tau, and Aβ42/NG ratio were measured in 30 PD patients and 30 controls and correlated with cognitive and motor parameters. The accuracy in distinguishing the cognitive status was determined.
Results:
NG and Aβ42 were significantly reduced in PD, with higher NG levels in patients with worse cognition. The Aβ42/NG ratio showed a direct correlation with Mini-Mental State Examination, independently from age and sex, and differentiated cognitively impaired patients with 92% sensitivity and 71.4% specificity, accuracy higher than NG alone. No correlations resulted with motor disturbances or therapy.
Conclusions:
The novel Aβ42/NG ratio couples either presynaptic or postsynaptic markers of synaptic dysfunction, representing a potential global index of synaptopathy, useful to track cognitive functions in PD.
INTRODUCTION
Parkinson’s disease (PD) is a common neurodegenerative disorder, characterized by progressive motor and non-motor disturbances, due to the loss of dopaminergic cells in the substantia nigrapars compacta and the accumulation of α-synuclein (α-syn) positive Lewy bodies [1–3].
Both clinical and animal model studies demonstrated that synaptopathy has a critical role in the pathogenesis of PD and other neurodegenerative disorders (as Alzheimer’s disease, AD), underlying either the early preclinical phases or the successive overt manifestations [4–7]. Therefore, markers of synaptic activity could be important tools to investigate in vivo the pathophysiological events of neurodegenerative diseases, to monitor clinical progression of patients, especially in terms of cognitive decline, and to develop effective disease-modifying treatments [8, 9].
Neurogranin (NG) is a postsynaptic protein, localized in the dendritic spines, involved in signaling pathways through the regulation of the calcium-binding protein calmodulin. Recent evidence disclosed a role of NG in the pathogenic mechanisms of different neurodegenerative diseases, and accordingly, the cerebrospinal fluid (CSF) levels of NG have been considered a reliable marker of synaptic degeneration. Specifically, higher levels have been found in patients with AD and mild cognitive impairment compared to healthy individuals, with an increase proportional to the progression of cognitive decline [10–12]. In PD, instead, studies on NG are scarce and controversial yet [13–15].
Amyloid-β42 (Aβ42)is an amyloid-β derived peptide, deeply involved in the pathogenesis of AD and PD-dementia, whose CSF levels inversely reflect brain burden of amyloid plaques and loss of synapses [16–19]. In fact, while physiological amyloid-β is of importance in normal synaptic function, the soluble Aβ42aggregates exert neurotoxic effects operating at presynaptic level [20, 21]. Differently from NG, data on Aβ42 in PD are more abundant and solid, indicating that its reduction identifies those patients with worse cognition and risk of cognitive decline [19, 23].
Aβ42 and NG thus represent two different biochemical markers of synaptopathy strictly related with cognitive functions. Their assessment in combination as Aβ42/NG ratio has never been tested before, whereas it may constitute a global index of synaptic dysfunction, which couples both presynaptic and postsynaptic markers, with potential relevance in PD.
In this study we thus evaluated the level of NG, Aβ42, and the Aβ42/NG ratio, together with other CSF biomarkers, including amyloid-β40 (Aβ40), total and phosphorylated tau (t-tau and p-tau),in PD patients and controls (CTL), exploring possible correlations with cognitive level and other clinical parameters, in order to disclose the clinical significance of the synaptopathy-related biomarkers.
METHODS
Subjects
The study was performed at Tor Vergata University Hospital (Rome, Italy) and involved 30 PD patients and 30 controls (CTLs). PD was diagnosed by the 2015 Criteria [24]. CTLs included age/sex-matched subjects, with non-neurodegenerative conditions (psychogenic disorders—mostly paraesthesia, not psychogenic parkinsonism [25], headache, peripheral nervous system conditions) and no signs of motor/cognitive impairment.
Demographics, Mini-Mental State Examination (MMSE) score adjusted for age and educational level, and the Charlson Comorbidity Index (CCI), a score measuring the presence of comorbidities [26], were recorded for each subject. PD patients were further assessed through Unified Parkinson Disease Rating Scale part 3 (UPDRS III), Hoehn and Yahr scale (H&Y), and calculation of the personal levodopa equivalent daily dose (LEDD) according to conventional formulas [27]. Assessment was performed under the effect of habitual antiparkinsonian medication (“ON state”) at the same time of CSF sampling. Lumbar puncture and CSF analysis were performed according to standard procedures, as previously described [28–30].
The study was conducted in agreement with Helsinki declaration principles, with the approval of local ethical committee (0026092/2017). Every subject signed an informed consent.
Biomarkers assay
Aβ42 and t-tau were measured by the automated system and the corresponding chemiluminescent immunoassay (CLIA) (Lumipulse, Fujirebio). Aβ40 and p-tau were analyzed by the corresponding enzyme-linked immunosorbent assay (ELISA) test, following standard procedures. NG was determined by an ELISA kit for the quantitative determination of Neurogranin truncated at P75 (EUROIMMUN); all samples were analyzed in duplicate.
To avoid differences due to pre-analytical handling, all measurements were assessed on the same frozen sample from each patient. All assays were performed in blind. The Aβ42/NG ratio has been calculated for each subject. In addition, Aβ42/Aβ40, t-tau/NG, and p-tau/NG ratios have been preliminarily calculated.
Statistical analysis
Variables’ distribution was evaluated with the Shapiro-Wilk test. Clinical-demographic data were compared with parametric or non-parametric tests, as appropriate. To allow statistical calculations, non-normally distributed variables were Log10-transformed.
Group differences in biomarkers were tested by one-way ANCOVA, using sex and age as covariates. Relationships among all clinical and biochemical variables were preliminarily explored by Spearman’s test, separately in each group. Associations between cognitive level or other relevant clinical parameters and biomarkers were then specifically tested by linear regression, either as a simple model or using age and sex as covariates. ROC (receiver operating curve) analysis and cut-off points calculation were performed to estimate sensitivity (Se) and specificity (Sp) values of biomarkers in distinguishing the cognitive status (“normal”=adjusted MMSE > 25 versus“impaired”=adjusted MMSE≤25 [31]). A p value <0.05 was considered significant. Analysis was conducted in blind, by IBM-SPSS-22.
RESULTS
Differences between PD and controls
Table 1 summarizes demographic, clinical, and biochemical data of the groups. No differences resulted in age, sex, CCI, and MMSE.
Summary of demographic, clinical and biochemical data of the groups. NA, not applicable; NS, not significant. Other abbreviations are spelled out in the text
The one-way ANCOVA model showed that in PD were significantly reduced: NG (215.07± 90.37 pg/ml versus 336.53±193.40; F(1,41) = 4.29, p < 0.05); t-tau (178.5±115.74 pg/ml versus 231.13 ±72.17; F(1,38) = 3.12, p < 0.05); p-tau (32.71 ±12.43 pg/ml versus 40.14±16.63; F(1,36) = 0.44, p < 0.05); Aβ42 (810.67±389.89 pg/ml versus 1125.5±548; F(1,41) = 4.02, p < 0.05). Aβ40 and Aβ42/NG did not differ significantly. Neither Aβ42/Aβ40 (PD versus CTL: 0.12±0.05 versus 0.14±0.5), t-tau/NG (0.8± 0.4 versus 0.9±0.8) nor p-tau/NG ratios (0.17±0.1 versus 0.14±0.1)significantly differed.
Clinical-biochemical associations
Figure 1A and B reports results of Spearman correlation. In PD, both NG and Aβ42/NG correlated with MMSE (respectively, R = –0.644, p = 0.01 and R = 0.597, p < 0.05), while no significant associations resulted between the remaining biomarkers, the combined ratios and other clinical parameters.
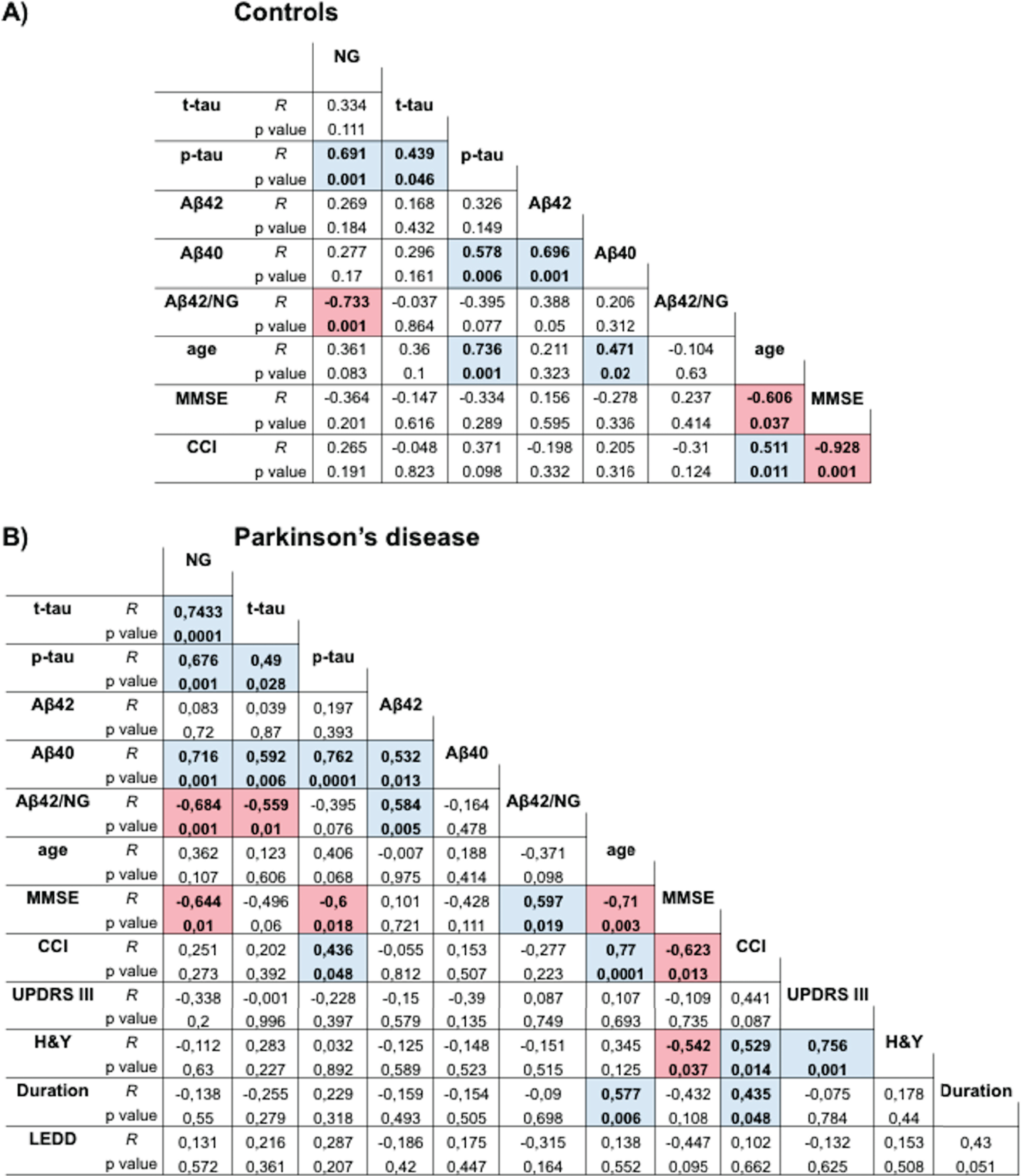
Spearman correlation graph for Control (A) and PD (B). Colored cells represent significant correlations, blue for direct and red for inverse.
The simple linear regression showed significant associations between NG or Aβ42/NG and MMSE (inverse with NG: F(1,13) = 7.03, R2 = 0.35, p < 0.05; T = –2.65, p < 0.05 – direct with Aβ42/NG: F(1,13) = 7.88, R2 = 0.38, p < 0.05; T = 2.8, p < 0.05 –tau proteins: not significant). The model adjusted for age and sex instead showed that only Aβ42/NG was independently related to MMSE (F(3,11) = 7.7, R2 = 0.65, p < 0.005; T = 2.3, p < 0.05) (Table 2).
Coefficients of adjusted linear regression models testing association between Aβ42/NG or NG and MMSE score
ROC analysis demonstrated for Aβ42/NG an area under the curve (AUC) = 0.88, p < 0.01; the cut-off value of 2.6 differentiated cognitive status with Se = 92% /Sp = 71.4%. Conversely, for NG, AUC = 0.8, p < 0.05; the cut-off value of 2.39 (Log10 transformed) differentiated cognitive status with Se = 67% /Sp = 71.4% (Fig. 2A, B).
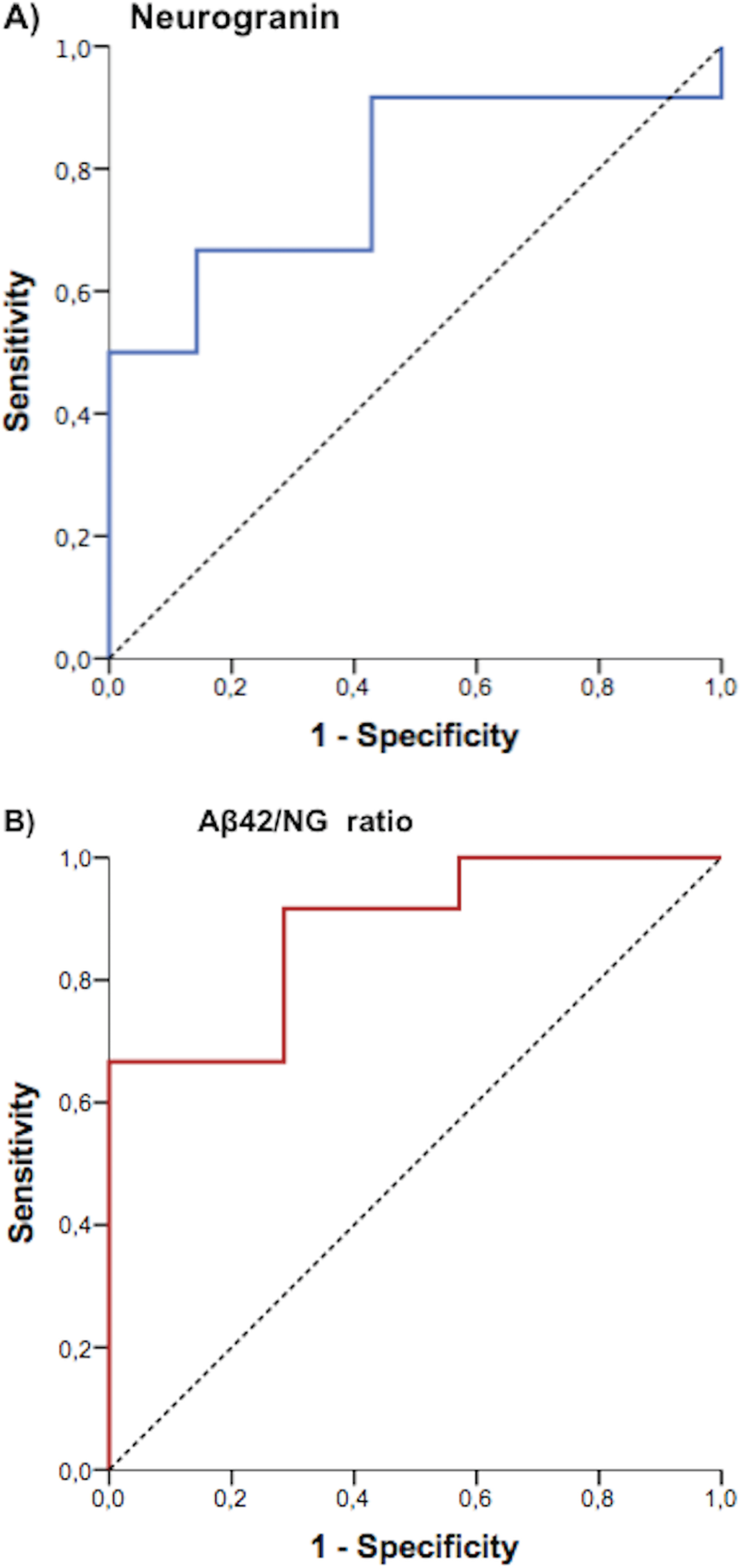
ROC curve analysis showing accuracy of (A) NG (AUC = 0.8, p < 0.05) and (B) Aβ42/NG ratio (AUC = 0.88, p < 0.01) to identify PD patients with cognitive impairment.
DISCUSSION
This study explored the clinical significance of synaptopathy-related CSF biomarkers NG, Aβ42 and, especially, the Aβ42/NG ratio, in PD. We found that, in PD patients, levels of NG and Aβ42 were reduced. Aβ42/NG and NG significantly correlated with MMSE, the first one independently from age and sex. Both markers effectively discriminated patients with cognitive impairment, although the ratio exhibiteda higher accuracy.
To date, the Aβ42/NG ratio has never been tested before in PD or other neurodegenerative diseases. Our results highlight its value as a potential tool to identify PD patients with progressive cognitive decline. In fact, despite this ratio did not differ between PD and CTL (probably because both Aβ42 and NG were reduced in PD), its progressive reduction in patients but not in controls, due to the lowering of Aβ42 or to the increase of NG, disclosed the worsening of cognitive functions expressed as adjusted MMSE score. Specifically, at the cut-off value of 2.6, the Aβ42/NG ratio discriminated cognitively impaired patients with Se = 92% /Sp = 71.4%.
The Aβ42/NG ratio joined together either presynaptic (Aβ42) or postsynaptic (NG) markers of synaptopathy, providing a global index of synaptic dysfunction, whose clinical significance was higher than NG alone. Indeed, NG levels were reduced in PD, with higher values in those patients with poor cognitive performances. However, differently from the Aβ42/NG ratio, the inverse association between NG and MMSE was lost in the presence of main covariates (age and sex) and the diagnostic accuracy for patients with cognitive impairment was limited to Se = 67% /Sp = 71.4%.
NG has been scarcely explored in PD and the few available studies demonstrated a reduction of CSF levels, probably due to molecular interactions with α-syn [15]. The correlation with cognition has not been clarified yet: some authors observed an association [13, 14], whereas, more recently, Hall and colleagues did not [15]. Our data, thus, confirm the decrease of CSF NG levels in PD and support the existence of a link between their increase and the cognitive decline, especially in early phases of the disease [14]. Conversely, no significant associations were found with motor disturbances (evaluated in “ON state”) or therapy.
In our population, the Aβ42 was significantly lower in PD than in CTL group, although in a normal range [32, 33]. Moreover, levels of Aβ40 were similar, indicating a normal rate of production in amyloid-β [34]. The lowering of Aβ42 in our PD group could be thus essentially due to the presence of cognitively impaired patients or at risk for dementia [22, 35], although in the absence of associations with MMSE. However, when we combined the Aβ42 into the Aβ42/NG ratio, it was able to enhance the clinical significance of NG in tracking cognitive functions.
Finally, in agreement with previous studies, we measured low levels of both t-tau and p-tau, which probably reflect some molecular interaction between tau proteins and α-syn within the core pathology of PD [30, 33].
Altogether our findings may suggest that NG and Aβ42 are synergistically involved in precipitating synaptic transmission dysfunction; as well, the respective increase and reduction in CSF reflect such pathological events. Actually, in AD the hippocampal and amygdala load of amyloid plaques directly correlated with NG CSF levels [36], while, in cognitively intact subjects, they correlated with amyloid-tracer uptake in the precuneus [37]. In PD, a previous study demonstrated that CSF NG correlated with cognitive performances, amyloid-β-derived peptides and glucose metabolism in parietal, occipital and lateral frontal areas [14]. The Aβ42/NG ratio thus emerges as a reliable index to monitor synaptic dysfunction and its clinical correlates in term of cognition in PD. Otherwise, the absence of significance for tau proteins/NG ratios suggests the specificity of molecular events identified by the Aβ42/NG ratio.
We are aware that a number of limitations have to be taken into consideration. First, the sample size and the cross-sectional design that make our results absolutely preliminary. Then, the absence of a comprehensive cognitive evaluation, adjunctive CSF biomarkers (e.g., α-syn species), morphological and PET imaging, and neuropathology data that might have extended our findings. However, the homogeneity of the population, also due to the inclusion of CCI in the criteria to match PD and CTL, strengthen the reliability of the results.
Despite these limitations, our study demonstrated in another, independent PD population, the reduction of CSF NG levels, also showing a proportional increase in those patients with cognitive decline.
The novel Aβ42/NG thus emerged as a potential index of global synaptic dysfunction, useful to track cognitive impairment in PD patients. Although lumbar puncture’s invasiveness may complicate a massive subjects enrollment, further studies on larger and prospectively-observed cohorts are now necessary to validate these preliminary findings and reveal the usefulness of Aβ42/NG ratio as predictor of cognitive decline in newly-diagnosed PD patients. On the other hand, deciphering in vivo the contribution of synaptopathy to clinical burden of PD may promote the development of novel disease-modifying treatments counter acting synaptic dysfunction, as preclinical studies and other translational evidence suggest [5, 38].