
Abstract
Background:
We previously reported the enhanced effects of physical exercise when combined with music (ExM) on cognitive function in community-dwelling normal elderly people compared to exercise alone. Following that study, participants voluntarily continued the ExM classes for 5 years.
Objective:
To identify the effects of a 5-year ExM intervention on cognitive function in normal elderly people.
Methods:
Fifty-four subjects continued the ExM classes once a week for 5 years (ExM group). Thirty-three subjects retired from the ExM class during the 5 years (Retired group). Twenty-one subjects never participated in any intervention over the 5 years (No-exercise group). Cognitive function and ADLs were assessed using neuropsychological batteries and the functional independence measure (FIM), respectively. The voxel-based specific regional analysis system for Alzheimer’s disease (VSRAD) was used to investigate medial temporal lobe atrophy.
Results:
Analyses of the raw scores after the 5-year intervention showed significant differences between the ExM and No-exercise groups in their MMSE scores, Raven’s colored progressive matrices (RCPM) time, logical memory (LM)-I, as well as the total and physical exercise sub-scores of the FIM. Analysis of subjects aged 70– 79 years at the beginning of this project showed significantly quicker performance on the RCPM in the ExM compared to No-exercise groups. The correlation coefficients between the total number of ExM sessions attended and the degree of changes in physical, neuropsychological, and VSRAD scores were significant for RCPM performance time and LM-I scores.
Conclusion:
Long-term ExM intervention reinforces multifaceted cognitive function in normal elderly people, and is especially beneficial for psychomotor speed.
Keywords
INTRODUCTION
The number of people with dementia is rising rapidly with the increase in longevity. Approximately 46.8 million people worldwide are estimated to be living with dementia, and 9.9 million new cases of dementia are diagnosed every year [1]. According to Alzheimer’s Disease International [2], these numbers will nearly double every 20 years to an estimated 74.7 million in 2030, and 131.5 million in 2050, with a large population occupying in Asia. Currently, there are no disease-modifying therapies against most dementia-related diseases. Thus, there is a need of multifaceted efforts including non-pharmacological interventions to prevent the occurrence and progression of dementia.
The positive effects of aerobic physical exercise on primary [3–10] and secondary [11–15] prevention of dementia have been well established. Several studies have reported that the combination of physical exercise and cognitive training is superior in enhancing cognitive function than individual exercise/training in both cognitively normal subjects [16–18] and elderly subjects with age-related declines [19–21]. Since 2010, we have carried out a dementia prevention/progress suppression program using physical exercise combined with music (the Mihama-Kiho Project). In our first report of non-pharmacological intervention in community-dwelling normal elderly people, we showed that musical accompaniment increased the positive effects of physical exercise on cognitive function [22]. In that study, the first group (ExM) performed physical exercise (once a week for one hour) with musical accompaniment, the second group (Ex) performed the same exercise without music, and the third group (Cont) received no intervention as the control. Before and after the year-long intervention, each subject was assessed using neuropsychological batteries. Results showed that physical exercise combined with music produced more positive effects on cognitive function than exercise alone, especially in visuospatial function (Mihama-Kiho Project Part 1). Neuroanatomical analysis using voxel-based morphometry (VBM) revealed that the grey matter volume of the frontal lobe was better preserved/larger in the ExM group compared to the Ex group, and the volume was decreased in the Cont group due to aging (Mihama-Kiho Scan Project Part 1) [23]. Although the research study concluded within a year, the participants wanted to continue the ExM class, so they started to manage the ExM class voluntarily and independently. Even now after 5 years from the end of the original study, the class continues to take place with many active participants.
Long-term intervention is necessary for a successful prevention of dementia. However, most studies on the “long-term” effects of physical exercise for dementia prevention were carried out for only several months (see the following reviews: [24–28]), with a few extending up to one year [29–36]. The longest non-pharmacological intervention for elderly people was reported by Oswald [17]. In that study, 375 community residents aged 75– 93 performed weekly cognitive, physical, and psychoeducational training, or a combination of physical training with cognitive or psychoeducational training for 5 years. The cognitive training and psychoeducational training consisted of 90 minute-long and the physical training 45 minute-long per session. In the combined training, each session consisted of 90 minutes of either cognitive or psychoeducational training followed by a 45 minutes physical training. Results showed that, compared to a no-treatment control group, there were significant training effects on cognitive function in the group exposed to the combined cognitive and physical training. While this study was well-designed and its results compelling, unfortunately, the number of subjects analyzed in the training group was small (n = 17), and no neuroimaging data were obtained. Two-year multi-domain intervention to prevent cognitive decline was reported from Finland (the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability; FINGER) [37–40]. Multi-domain lifestyle intervention was performed to subjects 60∼77 years old. The intervention included dietary counselling, exercise, cognitive training, and risk management of cerebrovascular disease. Compared to control group with general health advice, the report suggested that multi-domain intervention improves or maintains cognitive function of at-risk elderly people [37]. The report also explained that well-targeted dietary counselling may prevent age-related decline in diet quality and help to prevent cognitive decline [38]. Sociodemographics (sex, age, and education), socioeconomic status (income), cognition (Mini-Mental State Examination), cardiovascular factors (body mass index, blood pressure, cholesterol, fasting, glucose, and overall cardiovascular risk), and cardiovascular comorbidity did not modify response to intervention [39]. These series of studies are excellent as they assessed multifaceted influences of subjects’ characteristics to cognitive decline for 2 years, and is continuing even now to clarify the influences of long-term intervention.
In our recent study, we investigated the long-term effects of ExM by evaluating cognitive function and grey matter volume in the participants of the Mihama-Kiho Project Part 1 [22]. We compared the results from neuropsychological tests between subjects who continued to participate in the ExM classes for 5 years and those who did not participate in any ExM or Ex classes. We also semi-quantitatively assessed the degree of atrophy in the parahippocampal gyrus using a voxel-based specific regional analysis system for Alzheimer’s disease (VSRAD) [41]. This is the second study to assess the long-term effects of a 5-year intervention of physical exercise, and also the first study to show changes in the volume of parahippocampal gyrus using MRI.
METHODS
Subjects
This study was carried out as one of the public welfare projects of Mihama and Kiho town. The subjects consisted of community-dwelling normal elderly people who participated in the Mihama-Kiho Project Part 1 from 2011 to 2013. In the original study, paper fliers were distributed by public servants to the inhabitants of Mihama and Kiho; as a result, 163 people applied to participate in the one-year physical exercise class (Fig. 1). The inclusion criteria were as follows: applicants are (a) over 65 years old, (b) physically and psychologically healthy, (c) with good eyesight, (d) able to hear instructions clearly, and (e) independent in life. As for the physical and psychological condition, public health nurses of each town met participants and interviewed their families about the applicants’ physical and psychological activities in their daily lives. The applicants were not adopted if they met any of the following exclusion criteria: (a) apparent history of cerebrovascular attack, (b) presence of chronic exhausting disease such as malignancy and infection, (c) presence of severe cardiac, respiratory, and/or orthopedic disabilities, (d) use of drugs that might adversely affect cognition (antidepressants and antipsychotics), and (e) a previous diagnosis of dementia [22]. Adopted applicants were randomly divided into two groups: the ExM (n = 83) and Ex (n = 80) groups. As a Cont group, we recruited another 39 subjects using the same method as the ExM and Ex groups. The subjects of the ExM and Ex groups participated in the physical exercise program for one hour once a week for one year. Before and after the intervention period, neuropsychological assessments and brain MRI were performed. The subjects of the Cont group were examined two times with an interval of one year using the same neuropsychological batteries and imaging used for the ExM and Ex group (Fig. 1, upper half). For additional details, please see our previous paper [22].
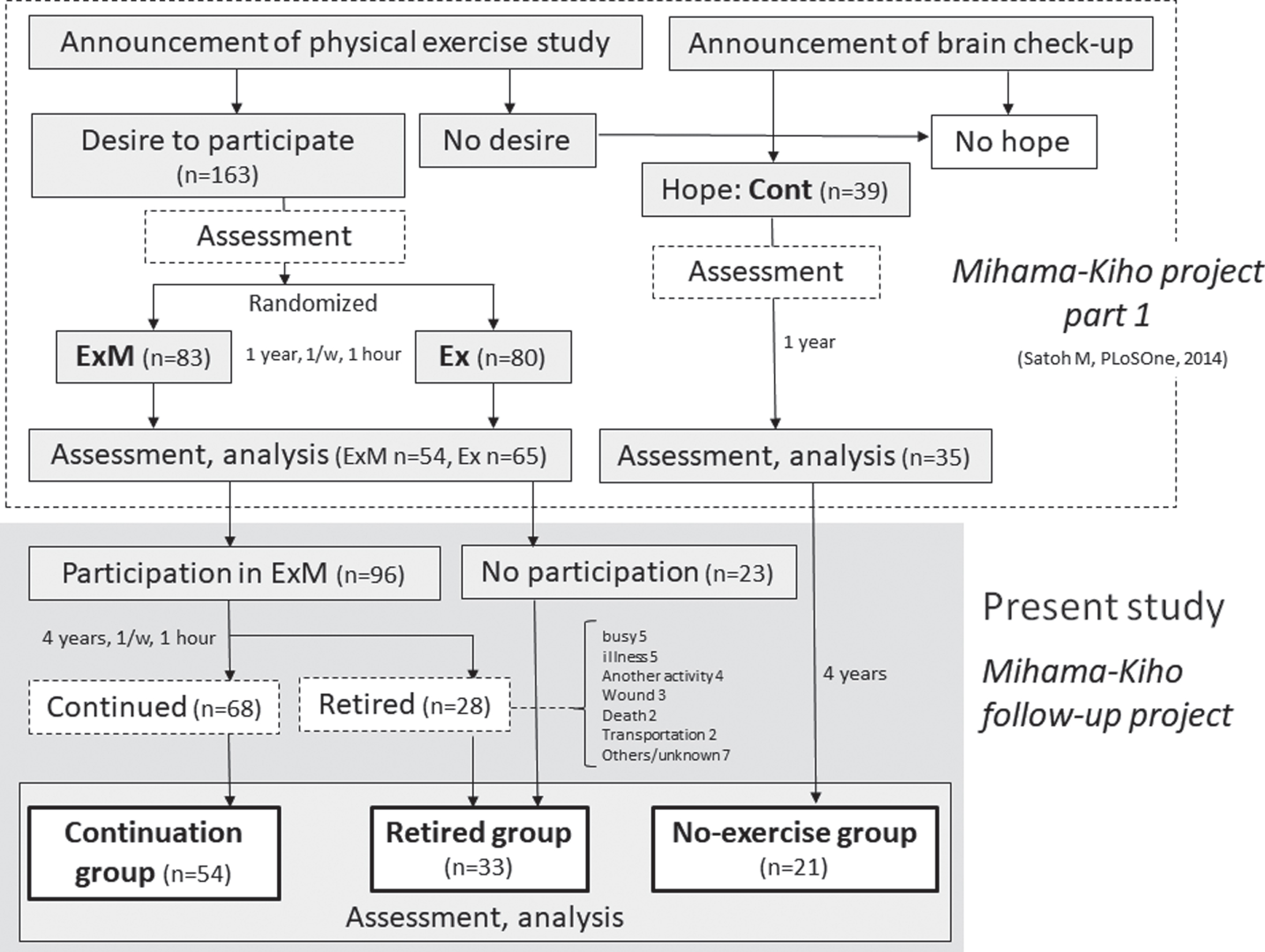
Flow diagram of this study.
Among the subjects of the ExM and Ex groups who received the neuropsychological and neuroimaging assessments after the one-year intervention, 96 subjects wanted to continue the ExM classes, and 23 subjects did not. Among the continuing participants in the ExM group, 28 subjects retired from the program within 4 years. In total, 68 subjects continued to participate in the ExM classes for a full 5 years, and among them, 54 subjects received the neuropsychological and neuroimaging assessments (Continuation group; Fig. 1, lower half). Subjects who did not choose to continue the ExM classes after the one-year intervention (n = 23) and those who ceased participating in ExM classes at some point over the subsequent 4 years (n = 28) constituted the Retired group. In total, 33 subjects of the Retired group received the neuropsychological and neuroimaging assessments. Among the Control group of the Mihama-Kiho Project Part 1, 21 subjects consented to the neuropsychological assessments and brain MRI over the 5 years following the first assessments (No-exercise group). The present study was named the Mihama-Kiho Follow-up Project. This study was carried out as official services by towns, and approved by each town council and mayor. This study received approval from the Kinan Hospital Research Ethics Committee, and was conducted in accordance with the Helsinki Declaration of 1975. All patients provided written informed consent. This study was registered to UMIN-CTR (UMIN000012148) on 28 October, 2013.
Physical exercise with music (ExM)
The ExM regimen is explained in detail in our previous paper [22]. The exercise program was established under collaboration of the Japan Fitness Association, experts in sports medicine, and the Yamaha Music Foundation. The program consists of 9 stages such as warmup, rhythmic walking, muscle training, cool down, and etc. (Table 1). With appropriate musical accompaniment, participants performed the exercises easily and enjoyably. The music was newly composed by Yamaha Music Foundation, and it belongs to so-called easy-listening like music by Paul Mauriat. One year after the start of the project, the impression of musical accompaniment was interviewed to subjects. All of them answered “good” or “not bad”, and no one answered “bad”. Thus, we may say that musical accompaniment was appropriate to the subjects, from the point of preference, comfortableness, and degree of difficulty. The exercise trainers were professional musicians who also held private licenses as physical trainers with the Yamaha Music Foundation. The intensity of the exercise gradually increased with the participants’ level. The ExM classes were held for one hour per week, and almost 200 classes in total were held over the 5 years.
Contents of the exercise
*Calculated based on the guideline of National Institute of Health and Nutrition. min, minutes.
Assessment of neuropsychological parameters and activities of daily living (ADLs)
The tests were nearly identical to those used at baseline in the Mihama-Kiho Project Part 1, and were performed 5 years after the beginning of the intervention. To quantify intellectual function, the Mini-Mental State Examination (MMSE) and the Japanese Raven’s Colored Progressive Matrices (RCPM) [42] were administered. RCPM measures not only the score but also the performance time, which reflects the psychomotor speed of the subject. Memory was evaluated using logical memory I and II (LM-I/-II) of the Rivermead Behavioral Memory Test (RBMT) [43], which consists of immediate and delayed recall of a short story. The assessment of constructional ability was based on the method described by Strub & Black [44]. A cube was shown to the examinees and they were asked to draw it. Their drawing was scored by assigning one of 4 possible grades (0: poor, 1: fair, 2: good, and 3: excellent). After the 5-year intervention, the Mie Constructional Apraxia Scale (MCAS) was also used to assess constructional visuospatial ability [45]. The MCAS is designed to assess constructional disabilities by evaluating not only the shape of a drawn Necker-cube but also the drawing process. A higher score is indicative of worse symptoms. For additional details, please see our previous paper [45].
For the assessment of ADLs, the functional independence measure (FIM) was used. The total possible FIM score was 126, and its assessment was divided into two main components: motor function (91 points) and cognitive function (35 points). The assessment of motor function was assessed by thirteen items including the act of eating, dressing, evacuation, urination, and walking. Cognitive function was assessed by five items including understanding, expression, and memory. A higher score is indicative of better motor or cognitive function. Additional details can be found in our previous papers [22, 46].
Voxel-based specific regional analysis system for Alzheimer’s disease (VSRAD)
The VSRAD was developed in the early 2000s [41]. It aims to semi-quantitatively assess the degree of atrophy in the parahippocampal gyrus for the purpose of diagnosing Alzheimer’s disease (AD), and is based on statistical parametric mapping (SPM, Wellcome Trust Center for Imaging, London, UK; http://www.fil.ion.ucl.ac.uk/spm). Performing the VSRAD assessment is very easy and the analysis can be completed with a few clicks of a computer mouse. In general, a patient with a VSRAD score over 2 is considered to possibly have AD, while a value under 1 is thought to be normal. It is important to note that the VSRAD is just one biomarker of AD, and a diagnosis of AD should be based on the combined results from neurological, neuropsychological, biological, and neuroimaging findings.
Statistical analysis
We analyzed the neuropsychological, VSRAD, and ADL scores at the end of the 5-year intervention and determined the degree of change in these scores over the 5 years. We focused particularly on the differences between the Continuation and No-exercise groups which were presumed to show the most characteristic findings. For the analysis of the demographic, neuropsychological, and VSRAD data between the Continuation, Retired, and No-exercise groups, ANOVAs were used if there was a normal distribution (Shapiro-Wilk test), and a Kruskal-Wallis test was used if there was not. The inter-group analyses between the Continuation and No-exercise groups were carried out as follows: the Shapiro-Wilk test was used to test for normality. If the result was parametric, a two-sample t-test or Welch test was used based on results from the test for homogeneity of variance (Levene test). If the result was non-parametric, the Mann-Whitney U test was used. In order to calculate correlation coefficients between the number of exercise sessions attended over 5 years and the neuropsychological, physical, and ADL data, Spearman’s rank correlation coefficient was used. We regarded the results as significant if the p-value was under 0.05. All statistical analyses were performed using IBM SPSS Statistics 23 software.
RESULTS
There were significant differences in several characteristics of the three groups at the start of the project: age, MMSE scores, LM-II, construction, and VSRAD (Table 2). The multiple comparisons identified significant differences between the Continuation and two other groups (age: Continuation versus No-exercise, p=0.020 and Continuation versus Retired, p = 0.045; LM-II: Continuation versus No-exercise, p = 0.009). Exercise habits in daily life of the participants was measured using the grade for activities of daily life (ADL-grade) which was established by the Ministry of Health, Labor and Welfare [22]. The scores for exercise habits in the Continuation, Retired, and No-exercise groups were almost the same, therefore, we can conclude that the subjects who participated in the ExM classes did so not because of the lack of physical movement in their daily lives. The physical, neuropsychological, VSRAD, and ADL scores of the Continuation and No-exercise group at the end of the 5-year follow-up are shown in Table 3. Compared with the No-exercise group, the MMSE score (p = 0.026), RCPM performance time (p = 0.015), LM-I score (p = 0.020), total FIM score (p = 0.030), and FIM exercise sub-score (p = 0.024) were significantly better in the Continuation group (Fig. 2a-e). In regard to the degree of change that occurred over the 5 years, the reduction in the LM-I score was significantly less in the Continuation group than in the No-exercise group (p = 0.008; Fig. 2f, Table 4). In relation to the total number of exercise sessions attended during the 5 years and the physical, neuropsychological, VSRAD, and ADL scores at the end of the 5-year follow-up, significant correlations were observed in the MMSE scores (r = 0.33, p < 0.001), the score (r = 0.20, p = 0.039) and time (r = – 0.23, p = 0.020) of the RCPM, the LM-I (r = 0.35, p < 0.001) and -II (r = 0.30, p = 0.001) scores, and the FIM cognition sub-score (r = 0.31, p = 0.001; Fig. 3, Table 5). The correlation coefficients between the total number of exercise sessions attended and the degree of changes in the physical, neuropsychological, and VSRAD scores were significant for RCPM performance time (r-=0.22, p = 0.020) and the LM-I score (r = 0.20, p = 0.036; Fig. 4 and Table 6).
Subjet’ characteristics of those ultimately belonging to the Continuation, Retired, and No-exercise group at the start of the Mihama-Kiho project
BMI, body mass index; Ex, exercise; LM, logical memory; MMSE, Mini-Mental State Examination; RCPM Raven’s Coloured Progressive Matrices; S&B, Strub and Black; S.D, standard deviation; VSRAD, Voxel-based Specific Regional analysis system for Alzheimer's Disease.
Differences in cognitive, physical, and ADLs between the Continuation and No-exercise groups at the end of the 5-year follow-up
ADLs, activities of daily livings; BMI, body mass index; Ex, exercise; FIM, Functional Independence Measure; LM, logical memory; MCAS, Mie Constructive Apraxia Scale, MMSE, Mini-Mental State Examination; RCPM Raven’s Coloured Progressive Matrices; S&B, Strub and Black; S.D, standard deviation; VSRAD, Voxel-based Specific Regional analysis system for Alzheimer's Disease.
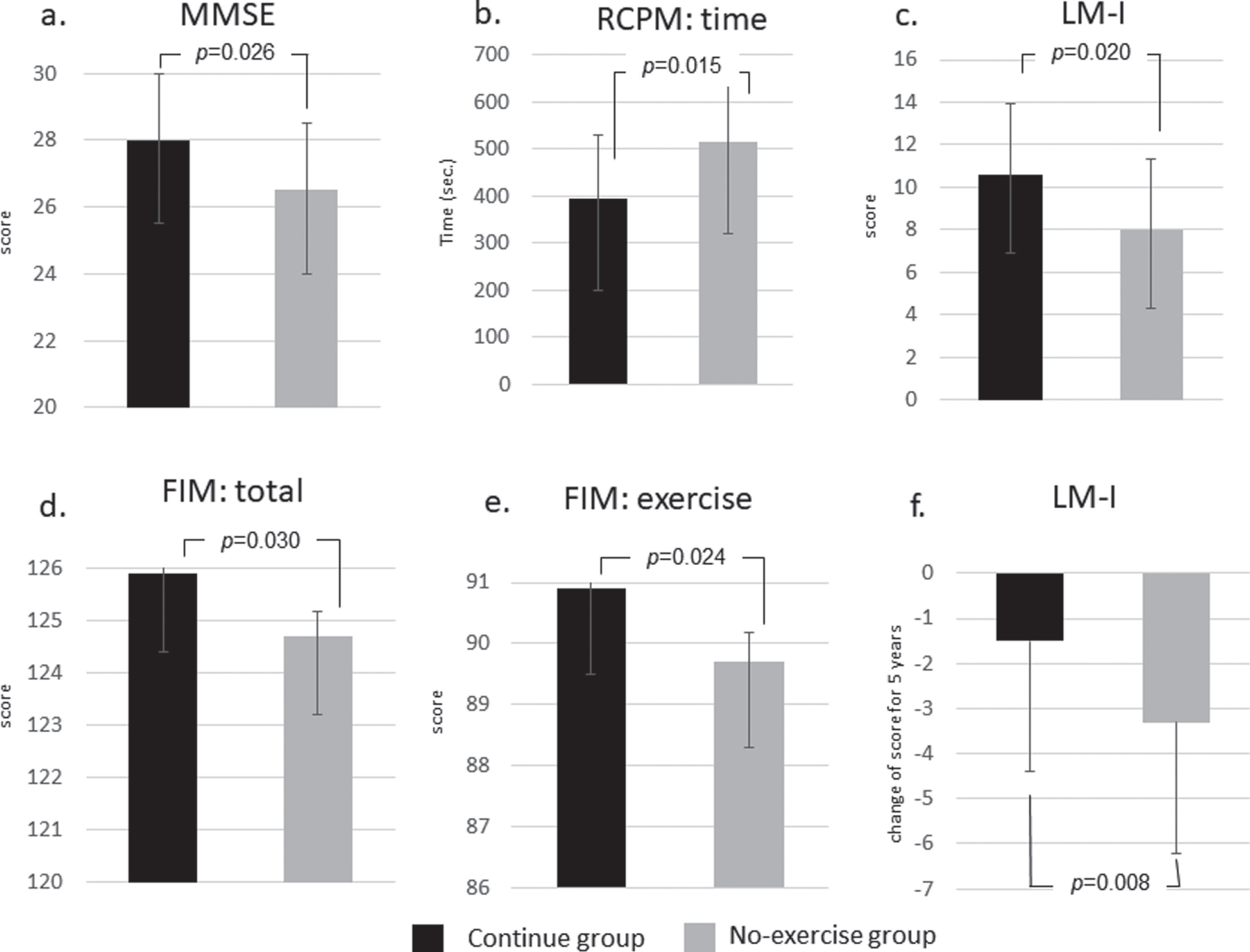
Significant results between the Continuation and No-exercise groups. Figure a-e show the raw data after 5 years. Figure f shows the significant changes over 5 years. For the abbreviations, see Table 3.
Differences in the degree of changes over 5 years between the Continuation and No-exercise groups
For the abbreviations, see Table 3.

Significance of results based on the correlation coefficients between the total number of exercise sessions attended over 5 years and cognitive, physical, and ADLs at the end of the 5-year follow-up. For the abbreviations, see Table 3.
Correlation coefficients between the total number of exercise sessions attended over 5 years and cognitive, physical, and ADLs at the end of the 5-year follow-up
Spearman’s rank correlation coefficient. For the abbreviations, see Table 3.

Significance of results based on the correlation coefficients between the total number of exercise sessions attended and the degree of changes in cognitive states over 5 years. For the abbreviations, see Table 2.
Correlation coefficients between the total number of exercise sessions attended and the degree of changes in cognitive, physical, and ADLs over 5 years
Spearman’s rank correlation coefficient. For the abbreviations, see Table 3.
As described above (Table 2), the subjects of the Continuation group were significantly younger than those in the No-exercise group. This means we cannot exclude the possibility of influences deriving from the difference of age to physical, neuropsychological, and VSRAD scores. Thus, we selected only the subjects that ranged in age from 70 to 79 years at the start of the intervention, and conducted the same series of analysis (Tables 7–9). In this analysis, among the subject characteristics of the 70 to 79-year-olds in the Continuation and No-exercise groups, only the LM-II scores significantly differed at the start of the Mihama-Kiho Project Part 1 (Continuation 11.8±3.4, No-exercise 9.3±2.6; p = 0.043; Table 7). Analysis at the end of the 5-year follow-up showed significant trends in RCPM performance time (p = 0.064) and LM-I scores (p = 0.066; Table 8). When evaluating the differences in the degree of change over the 5 years between the 70 to 79-year-olds in the Continuation and No-exercise groups, RCPM performance time in the Continuation group was significantly better than the No-exercise group (p = 0.005; Table 9).
Subject’ characteristics of the 70– 79 year-olds in the Continuation and No-exercise groups at the start of the Mihama-Kiho project
For the abbreviations, see Table 3.
Differences in cognitive, physical, and ADLs between the Continuation and No-exercise groups at the end of the 5-year follow-up
BMI, body mass index; Ex, exercise; LM, logical memory; MCAS, Mie Constructive Apraxia Scale, MMSE, Mini-Mental State Examination; RCPM Raven’s Coloured Progressive Matrices; S&B, Strub and Blood; S.D, standard deviation; VSRAD, Voxel-based Specific Regional analysis system for Alzheimer's Disease.
Differences in the degree of changes over 5 years between the Continuation and No-exercise groups in the 70 to 79 year-olds
For the abbreviations, see Table 3.
DISCUSSION
The results of the present study can be summarized as follows. I) Comparing the raw scores at the end of the 5-year follow-up, the Continuation group showed significantly better general intellectual function, psychomotor speed, and immediate memory, with better ADLs. II) Analyzing the differences in the degree of change over 5 years, immediate memory was significantly better preserved in the Continuation group than the No-exercise group. III) There was a significant difference between three study groups in age, scores of MMSE, delayed recall, visuospatial ability, and the degree of hippocampal atrophy. IV) Comparing subjects of the same age in the degree of change over 5 years, the Continuation group had significantly better psychomotor speed. V) Finally, the more ExM sessions the subjects participated in, the better their psychomotor speed and immediate memory was. From these results, we can conclude that long-term continuation of ExM contributes to better cognitive function in elderly people.
It is noteworthy that psychomotor speed was faster in the Continuation group compared to the No-exercise group in both the analysis of the degree of change over 5 years as well as the correlation with the total number of ExM sessions attended. This result is congruent with those of our previous studies which investigated the effects of singing in patients with dementia [47], participation in ExM by community-dwelling normal elderly people [22], and administration of ExM to patients with mild-to-moderate dementia (the Mihama-Kiho Project Part 2) [46]. The mechanism by which ExM improves psychomotor speed has been discussed previously [22]. In short, subjects listened to music, perceived the rhythm and the tempo of that music, judged whether their body movements and music were synchronous or not, and controlled their movements accordingly. The important factor is that these processes were performed simultaneously and continuously. This suggests that ExM consists of multifaceted tasks, and, by continuing such complex tasks over an extended period of time, the psychomotor speed of the Continuation group improved.
Although its physiological mechanisms remain unclear, the effectiveness of physical exercise in preventing the onset and progress of dementia has been well established [10]. It is generally thought that many neuroplastic and neuroprotective factors are related to the effects of physical exercise on cognitive function (Fig. 5) [25, 48– 54]. It was reported that listening to music activates a widespread neural network related to attention, semantic processing, memory, motor function, and emotional processing [22, 55– 66]. Music accompaniment might reinforce these mechanisms by having the subjects perform complex mental tasks such as analyzing music, monitoring physical movements, and judging their consonance.
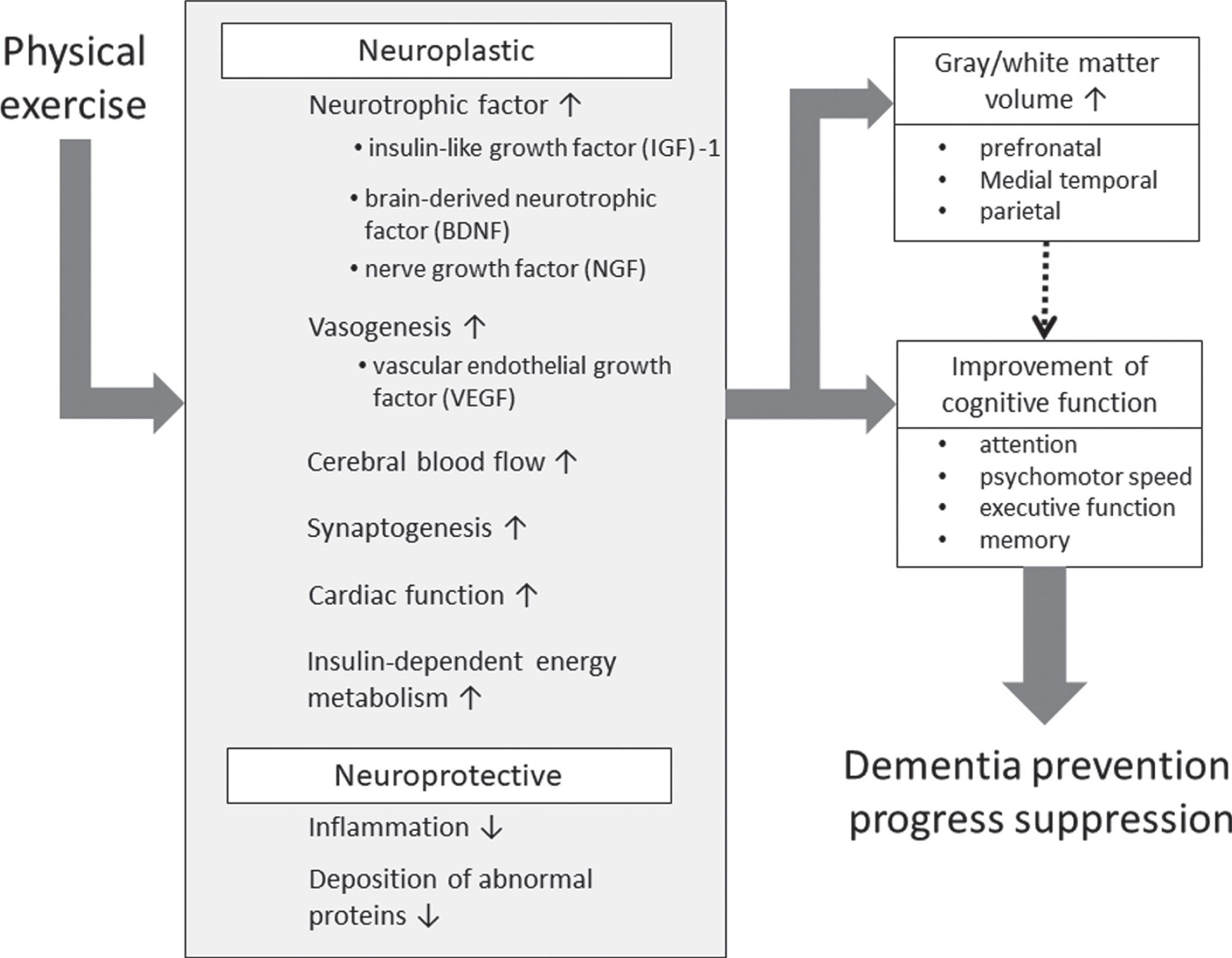
Hypothesized mechanism of dementia prevention by physical exercise.
We should not overlook the differences found at the baseline among three study groups in age, several cognitive abilities, and the degree of parahippocampal atrophy. It is well known that the cognitive function including the intellect and visuospatial ability and the volume of the brain decrease with age, even if they stayed within normal limits. At the start of the Mihama-Kiho Project Part 1, ages differed within the Continuation (72.4±5.0 years old), Retired (75.8±6.0 years old), and No-exercise (78.5±6.4 years old) groups. So, it is not impossible to hypothesize that the difference of cognitive function and hippocampal atrophy derived from the difference of age at the baseline.
In order to overcome the problem of significant difference of age at the baseline, we analyzed data from the subjects in the age range of 70 to 79 years inclusive, as shown in Tables 7–9. In these subcategorized analyses, the mean ages were almost the same between the Continuation and the No-exercise group, and the only significant difference was observed in LM-II, namely delayed recall, even though the results from the No-exercise group stayed within normal limits. There was a tendency for significance in the exercise habit, the score of MMSE and LM-I (immediate recall). The exercise habit was higher in No-exercise group, but their cognitive functions were relatively worse than the Continuation group. These facts leads to three possibilities: 1) the subjects in No-exercise group did not feel the necessity to participate in the exercise class, because they carried out enough physical movements in their daily lives, 2) the subjects in No-exercise group could not understand the importance of the physical exercise to dementia prevention, even if they accepted the same information from town office as the Continuation group, and 3) there were MCI or early dementia patients in the No-exercise group. As for the third possibility, the changes of cognitive function and hippocampal atrophy in 5 years were almost the same between two groups. If there was MCI or early dementia patients in No-exercise group, their cognitive function and hippocampal atrophy must have worsened in 5 years. As for the second possibility, the subjects of No-exercise group had normal cognitive function and have been spending daily family and social activities independently. The educational years did not differ between Continuation and No-exercise group. We suppose that it would not be correct to assume that the subjects of No-exercise group had lacked the ability to understand the information from town office introducing the physical exercise class. In summary, exercise habits in daily life might be a dominant factor determining whether or not to participate in physical exercise classes.
Even in the same age group of the Continuation and No-exercise group, time increase in the RCPM performance, namely worsening of the psychomotor speed, was smaller in the former group. This result suggests that physical exercise prevents the natural decline of psychomotor speed, and is congruent with the finding of our previous studies [22, 46]. Therefore, we can reasonably conclude that the long-term continuation of physical exercise brings positive effect to cognitive function of community-dwelling healthy elderly people, not only by the difference of ages at the baseline. We feel the need to announce the importance of physical exercise to dementia prevention, not only to subjects who spend physically inactive daily lives, but also to relatively active subjects such as No-exercise group in our experiment.
There are several possible reasons why the degree of cognitive changes over 5 years was less dramatic in the No-exercise group who spent relatively active daily lives compared to the Continuation group. First is the content of the physical activity. It is generally accepted that exercise using musical rhythm is more effective for improving the cognitive function of elderly people. Manual work seen in the No-exercise group, such as agriculture, fishery, and forestry do not always accompany rhythmic movements. Another factor may be the degree of lifestyle change. The overall exercise habit of the Continuation group increased more than the No-exercise group over the 5 years of investigation (p = 0.16, in Table 9), meaning lifestyle change itself has a stimulative effect. Finally, there may be a certain limit to the impact in which physical activity can bring to the cognitive function of elderly people. We cannot deny the possibility that the No-exercise group has already shown the maximum improvement brought by physical exercise. In order to further improve the cognition of the No-exercise group, another intervention such as cognitive training may be necessary.
We predict that the earlier the subjects participate in ExM classes, the larger the effects will be on cognitive function. The results of neuropsychological assessments at the end of the 5-year follow-up and the total number of physical exercise sessions attended were significantly correlated. The typical age at retirement in Japan is 65. Based on our studies, we recommend that elderly people start physical exercise as early as possible, at the latest by the time of their retirement. For much older people who hesitate to attend physical exercise classes, easy static technique such as Kirtan Kriya (KK) might be recommended [67–70]. The KK, which was assessed as the control group in Innes’s studies [69, 70], is based on the idea that music listening by itself is beneficial. The KK is an easy, cost effective meditation technique requiring only 12 minutes a day, and is known to improve stress, mood, well-being, sleep, and quality of life (QOL) of subjects with subjective cognitive decline and others [69].
Our present study has several limitations that should be noted. First, the number of subjects in the No-exercise group was relatively small as the number of participants recruited in the No-exercise group was half of that in the other two groups at the start of Mihama-Kiho Project Part 1. Second, various factors could influence cognitive function other than age, education, and exercise habits. When this project was initially started, we did not anticipate that we would re-assess the subjects 5 years later. Third, information on the subjects’ daily lives at home or in the community was not obtained from family members. Fourth, we did not consider the effect from lifestyle remodeling during the 5-year period. We do not have numeral objective data, but interviews to participants of physical exercise classes support the effects. For example, since the commencement of classes, several participants began to take the stairs instead of elevators, commute by bicycle or on foot instead of driving, stretch often and stand on tiptoes during cooking or doing the laundry. So, we allude that the direct and indirect effects of physical exercise enhanced the effectiveness found in the Continuation group. We will prepare another report focusing on the effects of lifestyle remodeling by participating in physical exercise classes. Fifth, the ExM intervention was carried out one hour a week. The standard recommendation of physical exercise for the dementia prevention is 120 [71] or 150 [72] minutes a week. As shown in our previous paper [22], the ExM is more effective than a single exercise. We speculate the effect would be much larger if the present intervention was done several times a week. Sixth and last, the anatomical changes in the brain were only assessed in the medial temporal areas using VSRAD, and did not include the entire brain. In the previous reports on the Mihama-Kiho projects, we had performed neuroimaging studies using the VBM (Mihama-Kiho Scan Project Part 1 and 2) [23, 73] based on publications regarding behavioral data (Mihama Kiho Project Part 1 and 2). In the FINGER trial for 2 years, no significant difference between the intervention and control group was observed in the changes of MRI measures [40]. As part of the present study, we also plan to report the changes in grey matter volume over these 5 years using VBM (Mihama-Kiho Follow-up Scan Project; Tabei et al., in preparation).
In spite of these limitations, the present study clearly identified the effectiveness of long-term ExM over years in elderly people. Japan is currently a rapid and remarkable aging society in which the world has never before experienced, while the public budget and labor power are limited. These ExM classes are managed by community residents themselves as a commercial activity by Yamaha. We expect similar activities to those described in our project will be useful for towns throughout Japan which suffer from depopulation, namely less people, and revenue shortfall
Summary
We investigated the effects of ExM over a 5-year period by following-up on participants of the Mihama-Kiho Project Part 1 [22]. Analysis of subjects ranging in age from 70 to 79 years old at the start of the project showed that psychomotor speed improved significantly in the ExM group that continued to participate in ExM classes over the 5 years. This finding is congruent with our previous studies which reported the positive effects of interventions including ExM or musical activities to healthy elderly people and to patients with dementia. Musical accompaniment may reinforce the multifaceted effects of physical exercise on cognitive function in elderly people. In our next paper, we will report the anatomical changes in the brain associated with long-term ExM in community-dwelling normal elderly people, using VBM of MRI data.
Footnotes
ACKNOWLEDGMENTS
We would like to thank the following persons for their kind contributions to this study: Shoko Fukuda in the speech therapy room, Isamu Nonomura in radiology, and Hideshi Kanai in the community cooperation room at Kinan Hospital; Tsutomu Nishi and Yoshimi Murotani (Shibano) at Mihama and Kyoko Higashi at the Kiho town offices, and Makoto Tayama at the Yamaha Music Foundation. This work was supported by a Scholarship grant from Daiichi-Sankyo Co., Ltd. 2018.