
Abstract
Background:
Previous studies have indicated that B vitamin deficiencies are an essential cause of neurological pathology. There is a need to provide evidence of the benefit of B vitamins for the prevention of cognitive decline in community-dwelling older adults.
Objective:
To examine the association between intake and plasma levels of vitamins B12, B6, and folate and cognitive function in older populations through a systematic review and meta-analysis.
Methods:
Medline (PubMed), EMBASE, and Cochrane databases were used to search the literature though August 8, 2019. We included observational population-based studies evaluating the association between concentrations or intake levels of vitamins B6, B12, or folate and cognition in older adults aged ≥45 years. The quality of all studies was assessed by the modified Newcastle-Ottawa Scale. Odds ratios (ORs) and hazard ratios (HRs) were analyzed by the random-effects model. Sensitivity analyses were conducted by excluding the studies with significant heterogeneity.
Results:
Twenty-one observational studies with sample sizes ranging from 155–7030 were included in the meta-analysis. Higher levels of vitamin B12 (OR = 0.77, 95% CI = 0.61–0.97) and folate concentration (OR = 0.68, 95% CI = 0.51–0.90) were associated with better cognition in cross-sectional studies, but not in sensitivity analyses or prospective studies. High vitamin B6 concentrations showed no significant benefit on cognition and dementia risk. Prospective studies did not provide substantial evidence for the relationship.
Conclusion:
The results from our meta-analysis suggest that vitamins B12, B6, and folate may not be modifiable risk factors for slowing cognitive decline among community-dwelling older individuals.
INTRODUCTION
Cognitive decline, as observed in mild cognitive impairment (MCI), Alzheimer’s disease (AD), and other dementias, has been one of the most common and costly chronic conditions contributing to decreases in the quality of life [1–6]. According to the National Center of Health Statistics (NCHS) and World Alzheimer Report 2015, the number of dementia patients worldwide will triple to 135.5 million by 2050 [7]. Dementia has become the sixth leading cause of death in all populations [7]. However, due to the unclear pathogeny, no effective strategies are available for preventing or treating this neurological disorder in late life.
Clinical practice guidelines have indicated that some malnourished conditions, such as deficiency of vitamin B12 or folate, are causes of dementia [8], and vitamin B12 supplements may reduce the risk of cognitive decline [9]. However, the current studies on vitamin status in the community population have not concluded consistently. Most observational studies conflated vitamin deficiencies with sub-optimal vitamin status, but they focused on sub-optimal vitamin status actually. Given the high prevalence of dementia and cognitive impairment in older adults and its significant consequences, it is critical to explore the role of B vitamin as a modifiable risk factor associated with indirect pathogenetic disease processes. Over the past few years, studies exploring the relationship between B vitamins, e.g., vitamin B12, folate, and vitamin B6, and cognitive impairment in community-dwelling older adults have been published. A few meta-analysis have also summarized the relationship between B vitamins and the risk of dementia, but with inconsistent conclusions [10–12]. The reasons may be because of the considerable heterogeneity in the studies they recruited, especially where the general concept of B vitamins included combinations of vitamin B12, folate, and vitamin B6 as the exposure measurement.
This study aims to assess the relationship between individual B vitamins, including vitamin B12, folate, and vitamin B6, and cognitive decline in older adults, through a systematic review and meta-analysis of published population-based studies with cross-sectional and prospective designs.
METHODS
This meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA-2009) [13] and Meta-Analysis for Observational Studies in Epidemiology (MOOSE) guidelines [14].
Search strategy
Studies were selected based on the following inclusion criteria: 1) community-based samples (N≥100); 2) aged human participants (>45 years); 3) observational (prospective or cross-sectional) design; 4) incorporated outcomes on incidence and prevalence of dementia or cognitive decline (e.g., decrease in Mini-Mental State Examination (MMSE) scores); 5) individual B vitamin exposure (vitamin B12, folate, or vitamin B6), blood concentrations, or intake levels; 6) reported effect estimates appropriate for the pooled analysis of effect sizes, such as odds ratios (ORs), hazard ratios (HRs), or other types of estimates, such as correlation or regression coefficients, that could be converted to the above indexes; and 7) results adjusted for covariates (at least by age, and sex).
We searched the PubMed, Cochrane library, and EMBASE databases from the inception date to August 8, 2019, with the search terms in Supplementary Table 1.
Modified Newcastle-Ottawa Scale (NOS) for quality assessment of observational studies
*0 = definitely no (high risk of bias); 1 = mostly no; 2 = mostly yes; 3 = definitely yes (low risk of bias).
Characteristics of the included studies for vitamin B12, folate, and vitamin B6
MMSE, Mini-Mental State Examination; SMMSE, Standardized Mini-Mental State Examination; 3MSE, Modified Mini-Mental State Examination.
Data extraction
Data extraction involved retrieval of the study design, population characteristics (including sample size and age), years of follow-up, exposure to B vitamins, and outcome indicators (Table 2).
To reduce the heterogeneity of outcome indicators among different studies, we focused on two indicators of cognitive decline assessment: MMSE as the assessment of global cognitive function and a diagnosis of dementia by particular criteria. If an article from the same cohort reported both cross-sectional and longitudinal results, we included each of these results separately.
Statistical analysis
The quality of articles was assessed by using the modified Newcastle-Ottawa scale for observational studies (Table 1). Four domains (selection bias, performance bias, detection bias, and information bias) were rated by this scale.
Categorized exposure or continuous exposure was analyzed as subgroup analysis. The effect measurement of lowest versus highest B vitamin categories was adopted. The definitions of ‘lowest’ and ‘highest’ B vitamin categories were based either on threshold values defined a priori or on population-based percentile so that these may vary across studies.
The combined effect size was estimated by a random effects model [15]. Heterogeneity was assessed using the I2 statistic with percentage cut-offs of 25%, 50%, and 75% corresponding to low, moderate, and high heterogeneity, respectively. Sensitivity analyses were conducted by excluding the studies that introduced significant heterogeneity. Egger’s regression test was used to assess publication bias. If a sufficient number of publications were available (n = 10), publication bias was assessed via funnel plots (visually) [16].
Statistical significance is p < 0.05 (two-tailed). Statistical analyses were performed using STATA 15.1.
RESULTS
Literature search and study characteristics
We identified a total of 642 articles, including 359 articles from PubMed, 281 from EMBASE, and 2 from COCHRANE. Two hundred six articles were excluded because they were duplicates. After reviewing 436 articles’ titles and abstracts, we selected 55 articles for further evaluation. After applying the inclusion and exclusion criteria and excluding studies with insufficient data for the meta-analysis, our analysis included 21 studies. The studies are outlined in Table 2, including 6 cross-sectional, and 15 longitudinal studies. Four prospective studies of the 15 longitudinal studies also reported cross-sectional results. Sample sizes ranged from 155 to 7030. The follow-up duration ranged from 2 years to 13 years. Six prospective studies included cognitively impaired participants at baseline [17–22].
Most studies included two genders, and one study included only women [23]. Five studies reported exposure to B vitamins as a continuous variable [21, 24–27], and 16 studies reported it as a categorical variable. Three studies used tertiles [19, 28–30], 2 studies used binary indicators [31], 8 studies used quartiles [17, 32–35], and 3 used quintiles [20, 37].
Sixteen studies reported cognitive function as continuous scores [17–21, 32–34], and 6 studies classified cognitive function dichotomously [22, 35–37]. Among the 23 studies that used neuropsychological tests, 14 studies measured global cognition using the Mini-Mental State Examination (MMSE, SMMSE, or 3MSE (n = 11)), and 6 studies used a diagnosis of dementia or AD based on the DSM criteria.
Methodological quality
Overall, studies were deemed good quality (low to moderate levels of bias). The most common source of bias was a lack of a power analysis. Most studies did not report how they handled missing data; however, participant characteristics of the lost participants were well documented. All studies performed multivariate adjustments. Commonly adjusted covariates included age, gender, education, season of blood collection, physical inactivity, smoking, alcohol, APOE, and depression.
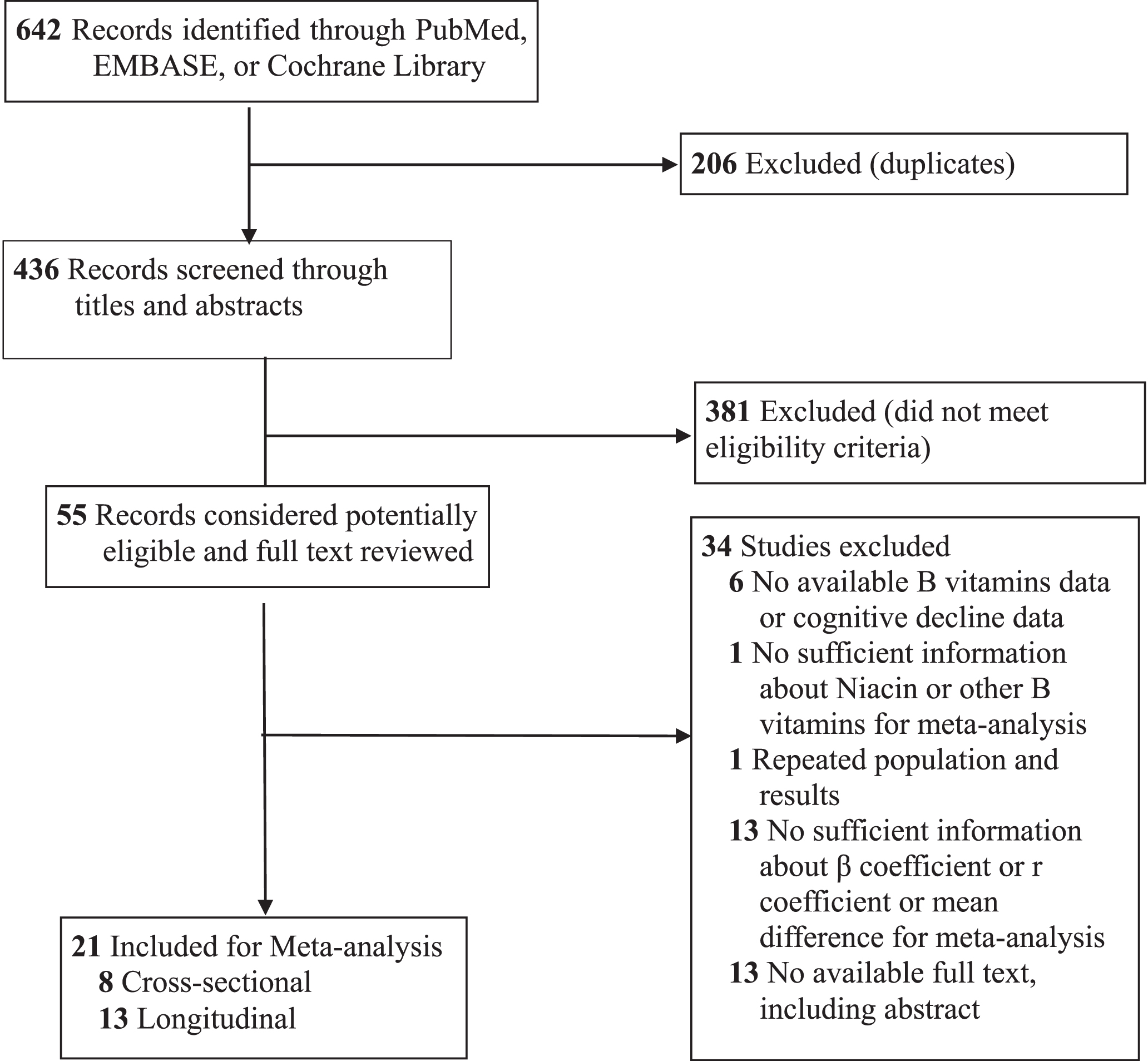
Literature Search and Screening Process.
Association between vitamin B12 and cognition
Individuals with high vitamin B12 blood concentrations had a lower risk of dementia compared to those with low vitamin B12 concentrations (OR = 0.77, 95% CI = 0.61–0.97) in cross-sectional studies (Fig. 2A). The heterogeneity among the studies was high (I2 = 76.9%) and disease bias was present (p < 0.05). The results of the stratified analysis showed that studies with vitamin B12 blood concentrations grouped in quartiles or quintiles had lower heterogeneity (I2 = 21.3%) and no publication bias; in these studies, there was no correlation between vitamin B12 and the risk of dementia (OR = 0.77, 95% CI = 0.57–1.04). Studies that were grouped by binary or tertile categories had higher heterogeneity and publication bias but also showed that the correlation between vitamin B12 and the risk of dementia was not statistically significant. Sensitivity analysis did not present a significant association after excluding four studies [26, 34] that contributed to the high level of heterogeneity (OR = 0.92; 95% CI = 0.68–1.23). No significant association was found in prospective studies that assessed either vitamin B12 blood concentrations (OR = 1.27; 95% CI = 0.97–1.67) or vitamin B12 intake (OR = 1.00, 95% CI = 0.81–1.23; HR = 1.10, 95% CI = 0.85–1.42) (Fig. 2B–D).
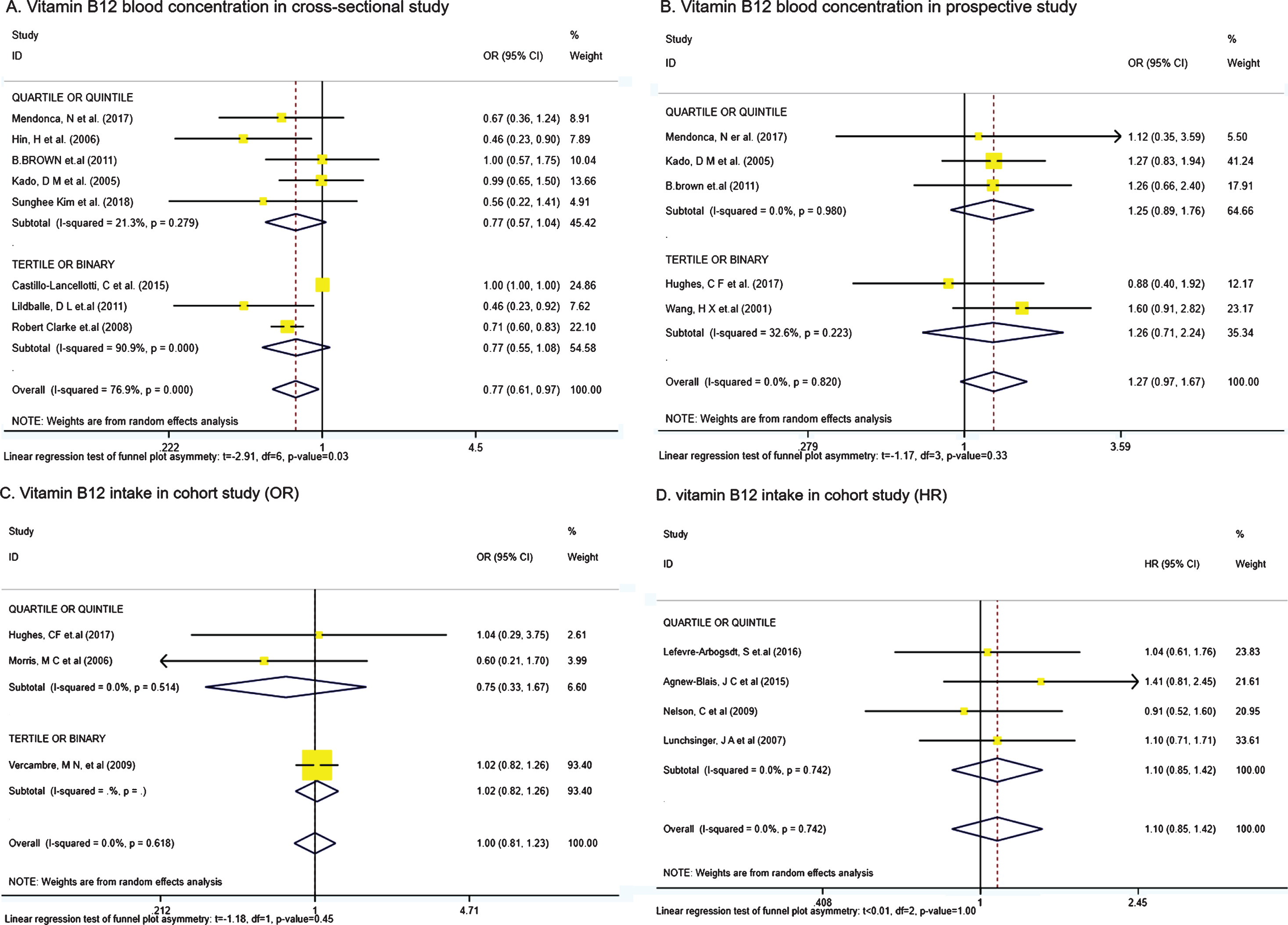
Forest plot of effect sizes for vitamin B12 on cognition. Note: Odds ratios or hazard ratios and 95% CIs were calculated using the Mantel-Haenszel method, with a random-effects model used to pool data. Risk ratio or hazard ratio data are rounded to 2 decimal places.
Association between folate and cognition
Compared with a low folate level, a high folate level was associated with a 32% lower risk of cognitive decline in cross-sectional studies (OR = 0.68, 95% CI = 0.51–0.90) (Fig. 3A). No significant association was found in prospective studies that measured folate blood concentrations (OR = 0.89, 95% CI = 0.79–1.00) and folate intake (OR = 0.84, 95% CI = 0.52–1.36; HR = 0.64, 95% CI = 0.41–1.00) (Fig. 3B–D). Sensitivity analysis showed no significance of the association (OR = 0.96; 95% CI = 0.90–1.01) after excluding four studies [18, 31] due to the moderate heterogeneity among the studies assessing folate blood concentrations.
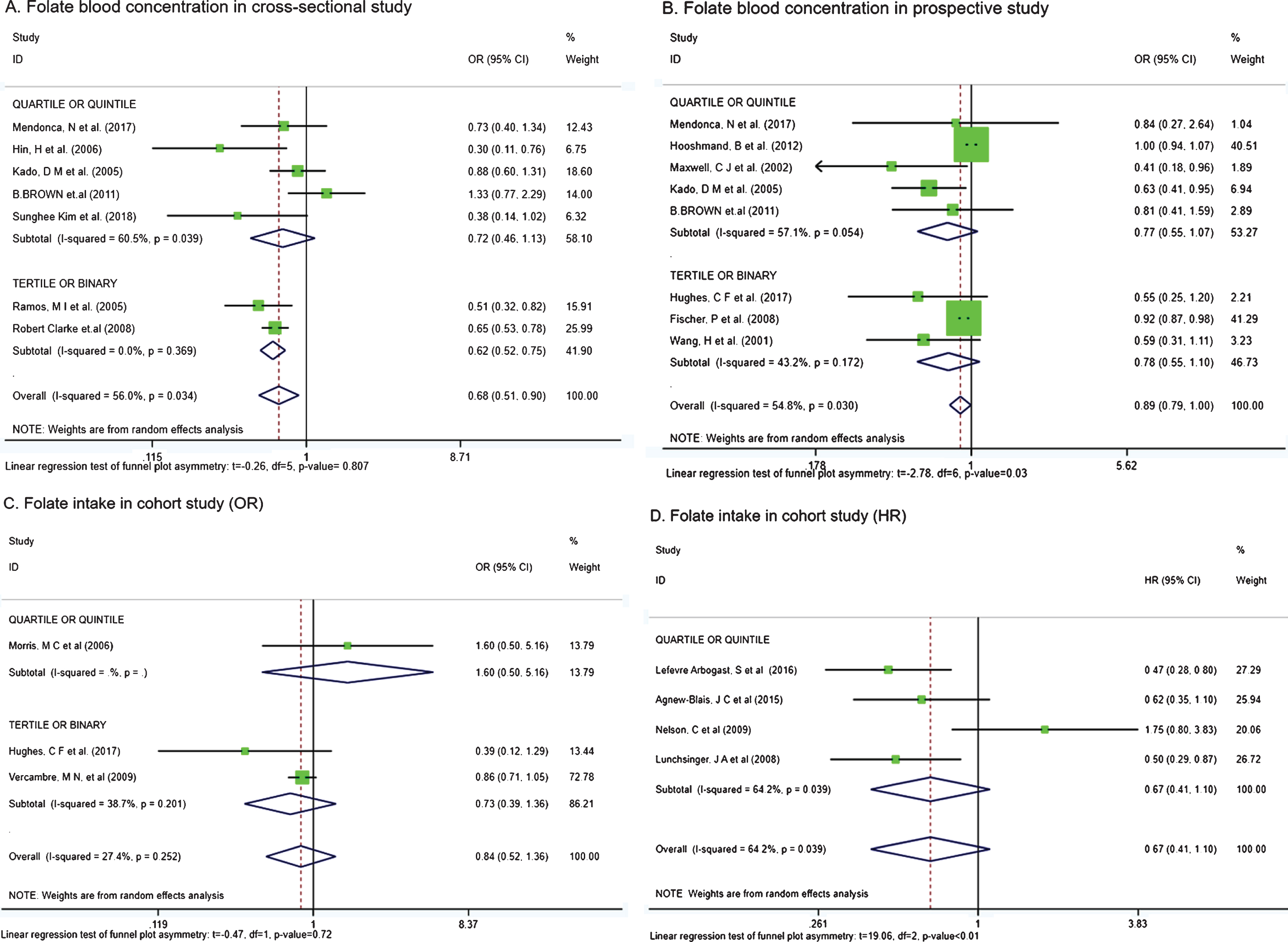
Forest plot of effect sizes for folate and cognition. Note: Odds ratios or hazard ratios and 95% CIs were calculated using the Mantel-Haenszel method, with a random-effects model used to pool data. Risk ratio or hazard ratio data are rounded to 2 decimal places.
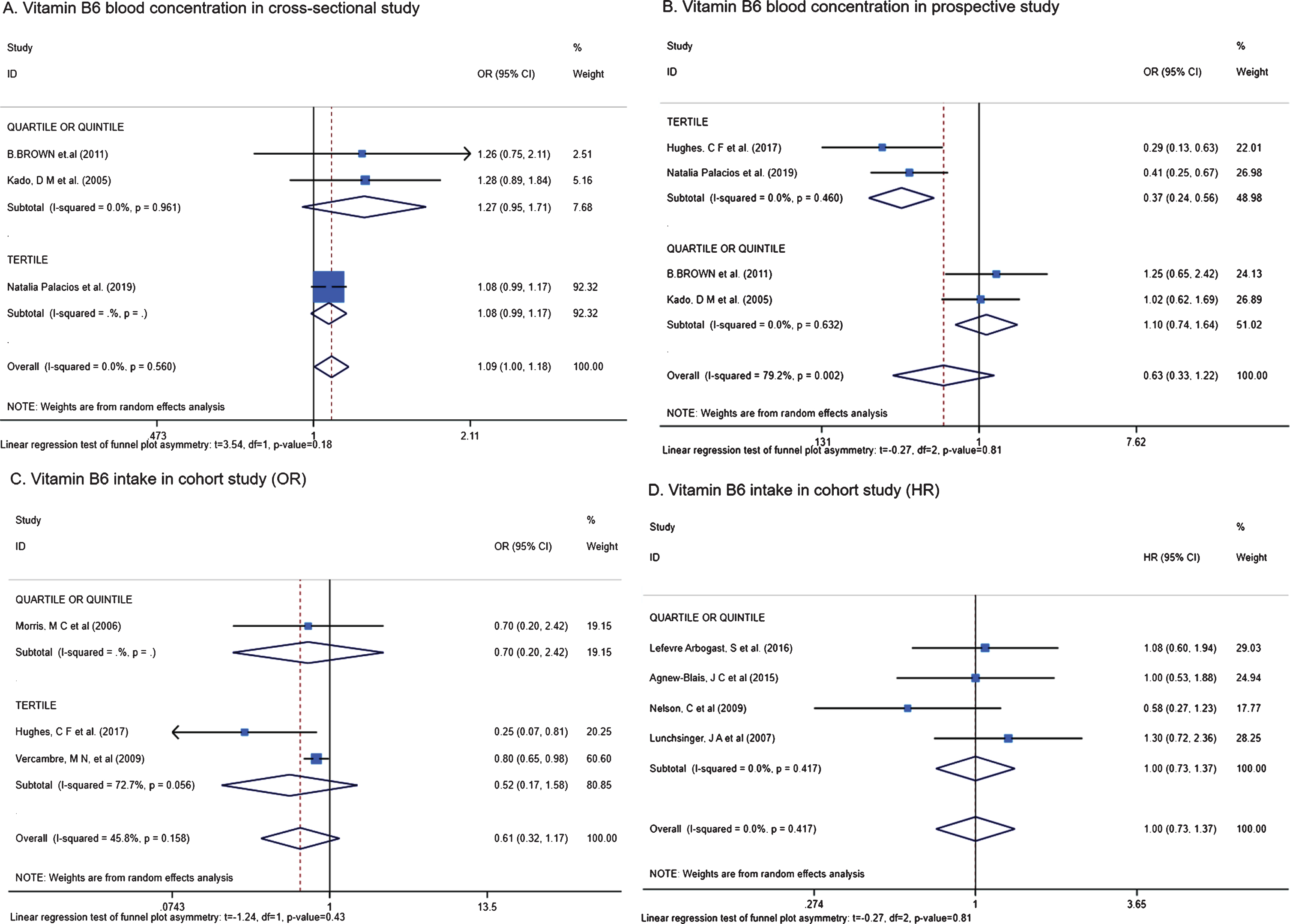
Forest plot of effect sizes for vitamin B6 and cognition. Note: Odds ratios or hazard ratios and 95% CIs were calculated using the Mantel-Haenszel method, with a random-effects model used to pool data. Risk ratio or hazard ratio data are rounded to 2 decimal places.
Association between vitamin B6 and cognition
No significant association was found between vitamin B6 and a higher risk of dementia or cognitive impairment in cross-sectional studies assessing blood concentrations (OR = 1.09, 95% CI = 1.00–1.18) and prospective studies assessing blood concentrations (HR = 0.63, 95% CI = 0.33–1.22) or intake (OR = 0.61, 95% CI = 0.32–1.17; HR = 1.00, 95% CI = 0.73–1.37) (Fig. 4A–D). The results of the meta-analysis were also nonsignificant, and the results remained similar in the sensitivity analysis (HR = 0.85, 95% CI = 0.72–1.01) after excluding one study [28] due to heterogeneity.
DISCUSSION
Our study demonstrated that the blood concentration or dietary intake levels of vitamin B12, folate, and vitamin B6, were not significantly associated with a lower risk of dementia in older adults in population-based prospective studies. However, these measures showed some extent of significant association in cross-sectional studies. To our knowledge, this is the first study to evaluate the association between individual B vitamins and middle-life (45–75 years old, only one study) and late-life (over 60 years old) cognition in a population. A previous meta-analysis only focused on compound B vitamins [11].
Vitamin B12 deficiency can cause many neurological diseases, such as myelopathy and neuropathy [38]. Cross-sectional studies showed significant associations between low blood vitamin B12 levels and lower scores on cognitive tests performed among elderly individuals [39–42]. On the other hand, the prospective study conducted by Clarke et al. [30] found that there was no association between cognitive decline (assessed with MMSE scores) and lower vitamin B12 levels. Previous studies have postulated that possessing the APOE ɛ4 allele in combination with other factors, such as level of education or B vitamin deficiencies, might increase the risk of dementia [43, 44]. APOE is an aggravating factor of the association between homocysteine and dementia [45]. Therefore, the differences in the results of those studies may be due to the interaction between vitamin B12 and the APOE ɛ4 allele.
Three prospective epidemiological studies have reported associations between a lower risk of cognitive decline and higher dietary folate [22, 46], but with inconsistent findings. Studies have shown that in participants with low vitamin B12 status, higher folate intake was not associated with cognitive function [20, 37], or that higher folic acid intake may have been related to a higher risk of cognitive impairment [47]. Additionally, findings have also been inconsistent in studies measuring blood concentrations. Kado et al. [25] found that individuals with serum folate in the bottom quartile were associated with a 7-year decline in cognitive function in adults 70 years or older. Some published studies [48] have reported neutral or harmful interactions between folate and vitamin B12 status and cognitive decline risk. Moreover, prevention trials have been inconclusive to date [49]. Durga et al. [50] found that folic acid supplementation for 3 years significantly improved domains of cognitive function that tend to decline with age. However, the participants they studied had high plasma total homocysteine concentrations and were vitamin B12-replete individuals and, thus, may not be representative of community-dwelling residents. A recent meta-analysis by Wald and colleagues [51] reviewed nine randomized clinical trials of folic acid supplementation and did not find any significant protective effect of the supplementation on cognitive decline.
Lefevre et al. [36] found that the intake of vitamin B6 was not associated with the risk of cognitive decline in community-dwelling individuals. In contrast, Hughes et al. [28] performed a prospective study that concluded that low vitamin B6 status and dietary intake might be associated with a reduced risk of cognitive decline in older adults. However, in Hughes’ study, some potential confounding factors such as alcohol and tobacco consumption, diabetes, history of cardiovascular diseases, and hypertension, were not adequately controlled for, and these confounders may have affected the conclusion. On the other hand, some articles have emphasized the potential positive effects of vitamin B6 from the perspective of metabolic mechanisms [52, 53]. Vitamin B6 has a crucial role in the synthesis of a variety of neurotransmitters, including dopamine and serotonin [54] and higher vitamin B6 intake has been associated with a greater volume of grey matter [53]. However, there is no evidence to support a beneficial effect of vitamin B6 on cognitive function in older adults with normal vitamin B6 blood levels [55].
A previous meta-analysis indicated that compound B vitamin tablet supplementation showed no obvious cognitive benefit in randomized controlled trials (RCTs) [10]. These trials vary greatly in the population sampled, study quality, and duration of treatment, thereby making it difficult to draw firm conclusions. There was an RCT [56] that included 168 adults (>70 years) with mild cognitive impairment who were either assigned to a placebo group or a treatment group (daily dose of 0.8 mg folic acid, 0.5 mg vitamin B12, and 20 mg vitamin B6) and followed for 2 years. This RCT reported that brain atrophy was 53% slower in the treatment group than in the placebo group, but only in the patients with tHcy concentrations >13 mmol/L at baseline, which is not representative of a community population. For healthy older adults, multivitamin supplements may increase their blood concentration of biomarkers, e.g., vitamin B12, which is relevant to white matter hyperintensities [57]. However, these biomarker changes were not accompanied by improved cognitive function [58]. A meta-analysis showed that there was no significant effect of taking B vitamins or antioxidant vitamins on global cognitive function in RCTs [12].
The mechanism of the relationship between B vitamins and cognitive function is unclear. One possible mechanism involves the role of vitamin B12, B6, and folate in the metabolism of total plasma homocysteine (tHcy). Hyperhomocysteinemia has been reported in many studies to be associated with an increased risk of cognitive impairment [59–61]. Supplementation with B vitamins can reliably decrease the plasma level of tHcy [62]. In the selected studies, the intake of B vitamins was measured by a specific food frequency questionnaire (FFQ) [23, 36]. Vitamin B6 blood concentrations were assessed by measuring PLP or pyridoxal-5-phosphate levels in the blood by high-performance liquid chromatography [28, 63]. Folate (vitamin B9) levels were preferentially determined through the measurement of folate in red blood cells [38, 64]. Serum vitamin B12 was assessed by transcobalamin saturation and holotranscobalamin concentrations [38, 66]. In a population with MCI, the accelerated rate of brain atrophy in the elderly individuals could be slowed by treatment with homocysteine-lowering B vitamins [56, 67]. However, evidence from a meta-analysis indicated that although elevated tHcy levels were associated with a higher risk of cognitive impairment and dementia, available evidence from randomized controlled trials showed no significant benefit for reducing the risk of dementia by using B vitamins to lower tHcy in community-dwelling older adults [10]. Additionally, both vitamin B6 and folate are involved in the synthesis of several key neurotransmitters, and folate deficiency has been related to oxidative stress and DNA damage in neurons [68, 69]. However, one study showed that a positive association with cortical folding was detectable in a population taking supplemental B vitamins, but cognitive function did not improve [55]. The uncertain mechanism by which B vitamins affect cognition may potentially explain the lack of association between the concentrations or intake of vitamin B12, folate, or vitamin B6 and cognition in the current meta-analysis.
Our study has several limitations. First, the included studies differed in neuropsychological tests and diversity in categorizing low (ranging from <150 to <308 pmol/L) and high (ranging from ≥150 to ≥522 pmol/L) vitamin B12 levels. Some studies also had marginally unequal sample sizes between low and high B vitamin categories. After excluding these studies that introduced heterogeneity in post hoc sensitivity analyses, the heterogeneity among the studies was lower, and B vitamins were not associated with a benefit for slowing cognitive decline. Therefore, it seems unlikely that this meta-analysis missed a potential beneficial association between B vitamins and any outcome analyzed due to inappropriate pooling of overly heterogeneous studies. Second, we only studied the relationship between B vitamins and global cognition or dementia incidence. However, B vitamins may have potential effects in specific domains of cognition. Due to the limitation of the number of articles, we did not analyze these associations. Third, we used both global cognition and dementia incidence simultaneously, which may have introduced bias, but the results remained similar after excluding eight studies measuring dementia incidence. Fourth, we did not consider the interactions among different B vitamins, because few studies reported such interactions. Fifth, we did not include RCTs because there are not enough intervention studies that met our inclusion criteria. Additionally, most intervention studies have focused on the effects of complex B vitamin supplements on the risk of dementia, and the content of B vitamins in each supplement was not consistent. Our study focuses on the independent effect of particular B vitamins on cognitive function. Sixth, the relationship between B vitamins and cognitive decline may be more evident in high-risk populations (such as older adults in the process of cognitive decline and those who have low B vitamin status). However, there were not enough studies that reported the relevant conclusions in these groups of people. Seventh, some studies have reported that other B vitamins, such as dietary vitamin B3 [70] and blood levels of vitamin B1 [55], may be related to AD and age-related cognitive decline. However, due to the limited evidence from observational studies, this study focused on the effects of B12, B6, and folic acid on cognitive decline. The role of other B vitamins needs further exploration before we can draw conclusions. Eighth, the research object of this study is the elderly population in the community. Few people have severe B vitamin deficiency, and most malnourished people are sub-optimal vitamin status. Therefore, the conclusion of this study may not be applicable to patients with severe B vitamin deficiency. Last, we did not exclude prospective studies with cognitive impaired participants or dementia at baseline, and the possibility that this had an influence cannot be disregarded.
Conclusion
Available evidence from observational population-based studies shows no significant association between vitamin B12, folate, or vitamin B6 and cognitive decline or dementia. Observational studies and RCTs with larger sample sizes and longer follow-up times are needed to provide solid evidence of the causal relationship, especially for other B vitamins.
Footnotes
ACKNOWLEDGMENTS
This work was supported by grants from National Natural Science Foundation of China (81773513), Shanghai Municipal Science and Technology Major Project (2018SHZDZX03), ZHANGJIANG LAB, Scientific Research Plan Project of Shanghai Science and Technology Committee (17411950701, 17411950106), and the National Project of Chronic Disease (2016YFC1306400).