
Abstract
Because of their roles as potential risk factors, we evaluated whether obstructive sleep apnea (OSA) severity interacts with interleukin-6 (IL-6) in predicting incident dementia of the Alzheimer’s type (DAT). In 269 dementia-free participants, IL-6 and the apnea-hypopnea index (AHI) were measured at baseline and incident DAT was surveilled for up to 22.8 years. Cox models revealed a significant interaction: In the lowest IL-6 quartile only, a higher AHI was associated with an elevated risk of DAT. The association between OSA severity and incident DAT might be especially apparent in the absence of inflammation or absence of potential benefits from IL-6.
Keywords
INTRODUCTION
Obstructive sleep apnea (OSA) has been associated with a higher risk of incident dementia, especially dementia of the Alzheimer’s type (DAT) [1]. In fact, OSA may contribute to amyloid-β and tau pathology [1, 2]. However, only a subsample of the OSA population might be at risk for dementia, with varying risk depending on age, sex, and OSA severity [1]. Further, it is postulated that the association between OSA and incident DAT might vary according to underlying levels of inflammatory biomarkers, such as cytokines. Interleukin-6 (IL-6) is a regulatory cytokine involved in multiple brain functions, including promoting the inflammatory response, neurotrophic changes, and microglial activation [3]. IL-6 is thought to play an important role in the pathology of DAT via its response to amyloid-β deposition and its role in neuroinflammation [3, 4].
Given the increasing prevalence of OSA [5], a greater understanding of a potential effect modifying role of inflammation on the association between OSA and incident DAT is key in order to better risk-stratify individuals for disease and identify opportunities for intervention. In this study, we aimed to evaluate whether serum IL-6 levels interact with OSA severity when predicting clinical DAT in the prospective community-based Framingham Heart Study.
MATERIALS AND METHODS
Sample
This study was performed within the Framingham Heart Study Offspring cohort, which has included nine examinations approximately one every four years [6]. Dementia-free participants with a polysomnographic recording (baseline, subset of the Sleep Heart Health Study, 1995–1998), serum IL-6 assessment (baseline, 1995–1998), and continuous surveillance for incident DAT and all-cause dementia (until 2017) were included in the present study. Participant selection is presented in Fig. 1. All participants gave their written informed consent before the study. The institutional review board at Boston University Medical Center’s approved the study.
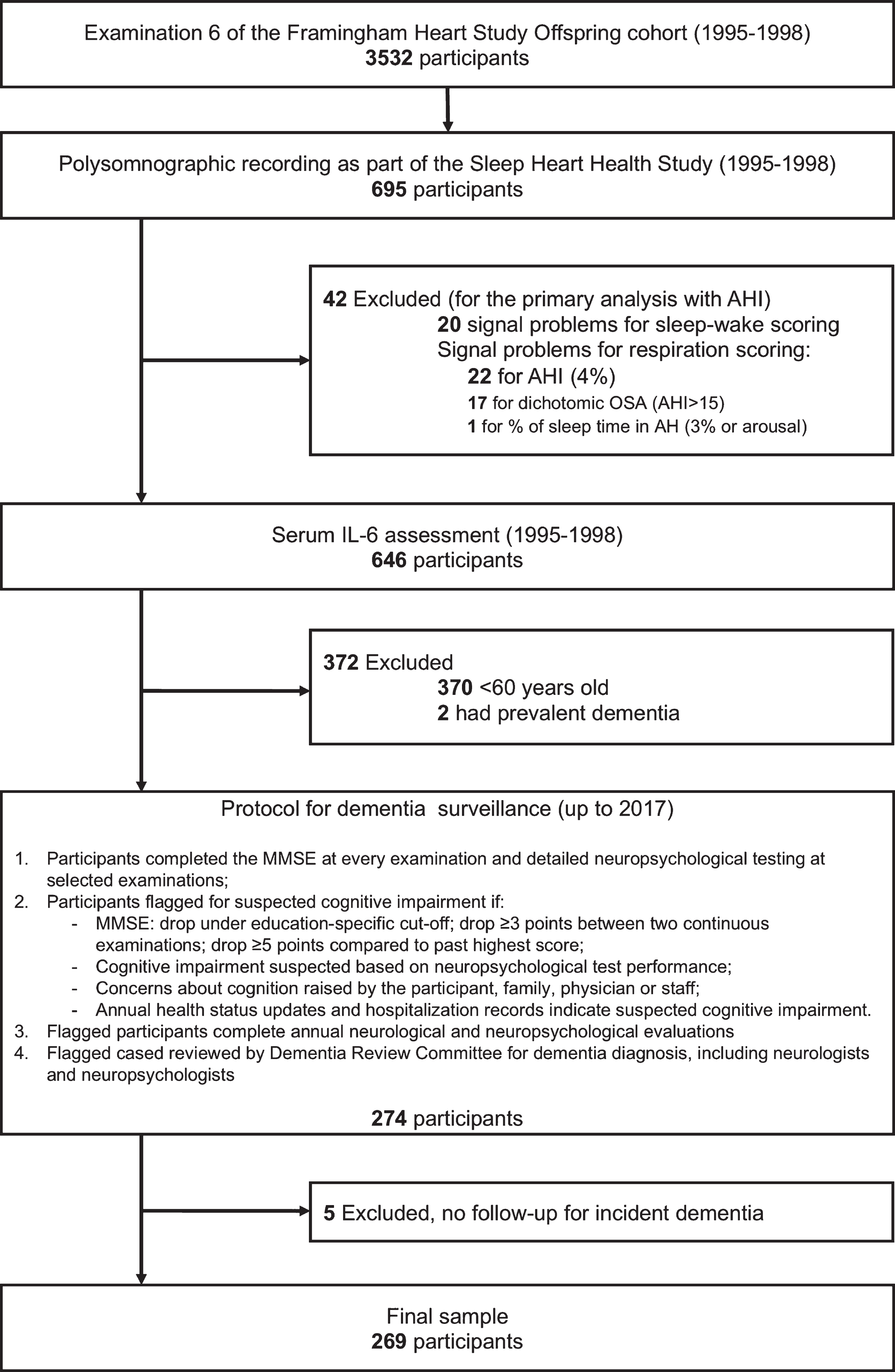
Selection of study participants and continuous surveillance for incident dementia. AHI, Apnea-Hypopnea Index; AH, Apneas and hypopneas; IL-6, Interleukin-6; MMSE, Folstein Mini-Mental State Examination.
Polysomnographic recording
The complete in-home overnight PSG recording included electroencephalograms, electrooculogram, chin electromyogram, oximetry, chest wall and abdomen inductance plethysomnography movements, and nasal/oral airflow (thermistry). The main exposure for this study was the apnea-hypopnea index (AHI) used continuously, corresponding to the number of apneas and hypopneas (accompanied by a ≥4%oxygen desaturation) per hour of sleep. Scoring criteria and the protocol were published previously [7]. In order to evaluate whether other variables defining OSA interacted similarly with IL-6 levels, we included as secondary exposures the presence of OSA defined by an AHI >15, also known as a moderate to severe OSA diagnosis, as well as the percentage of sleep time spent in apneas and hypopneas (accompanied by a ≥3%oxygen desaturation or an arousal), which represents OSA severity using different scoring criteria.
Serum IL-6 levels
After the blood draw at baseline, serum was frozen at –80°C. IL-6 was assessed at the second thaw by high-sensitivity quantitative ELISA using a commercially available assay (R&D systems; Human IL-6 Quantikine HS ELISA kit), which were run in duplicate (coefficient of variation intra-assay: 3.1±2.2).
Incident dementia
Methods for dementia surveillance are presented in Fig. 1. Dementia diagnosis was based on the Diagnostic and Statistical Manual of Mental Disorders IV-TR [8], and DAT was adjudicated based on the Alzheimer’s Disease and Related Disorders Association and the National Institute of Neurologic and Communicative Disorders and Stroke [9].
Statistical analyses
We included interaction terms in Cox proportional hazards models to examine interactions between IL-6 levels defined as quartiles and the AHI in their effects on incident dementia. In the presence of significant interactions, we stratified by IL-6 quartiles (as used previously when evaluating IL-6 and the incidence of cerebral events such as stroke [10]) and used Cox proportional hazards models to investigate IL-6 quartile-specific associations between AHI and incident dementia. Non-events were censored at death or at the date the participant was last known date to be dementia-free. The proportional hazards assumption was upheld. All models were adjusted for age, sex and body mass index. A natural log transformation was applied to the AHI and body mass index.
Sensitivity analyses included the addition of the Revised Framingham Stroke Risk Profile score (single score representing stroke risk including age, smoking, cardiovascular diseases, atrial fibrillation, diabetes mellitus, hypertension) or the apolipoprotein E4 (APOE4) allele carrier status as a covariate (instead of body mass index, still adjusted for age and sex). Lastly, we performed a post-hoc analyses that included adjustments for all covariates (age, sex, body mass index, Revised Framingham Stroke Risk Profile score, and APOE4 allele carrier status).
Moreover, in order to explore whether findings remained across OSA definitions, secondary analyses were performed with moderate to severe OSA (AHI >15) and the percentage of sleep time in apneas and hypopneas with ≥3%oxygen desaturation or an arousal (instead of the continuous AHI, ≥4%desaturation) as exposures in separate statistical models, adjusted for sex, age, and body mass index.
Results were considered significant if p < 0.05, except for interactions, which were considered significant if p < 0.1. Statistical analyses were performed with SAS software V9.4 (SAS Institute Cary, NC).
RESULTS
Sample characteristics
The sample comprised 269 participants (mean age: 67.4±5.0 years, 50.2%men) followed on average for 14.3±5.7 years, up to 22.8 years. During follow-up, we observed 45 cases of all-cause dementia, 35 of which were consistent with DAT (Table 1). Body mass index as well as the proportion of participants treated for hypertension and who had prevalent cardiovascular diseases, were higher with increasing IL-6 quartiles. Approximately a quarter of the sample presented with OSA, characterized by an AHI >15 (median: 6.5, Q1:2.8, Q3:14.3). More specifically, 65 participants had an AHI >15, while 17 participants had an AHI >30. In the highest IL-6 quartile, 19 participants developed dementia (28.4%; 14 cases were DAT) whereas only 8 incident dementia cases were observed in the lowest quartile (12.3%, all were DAT).
Sample characteristics by IL-6 quartiles
Characteristics are presented as mean (standard deviation) or frequency (percent), except for variables marked with an (a) that are presented as median (lower quartile –upper quartile) as they were not normally distributed. Follow-up time for dementia was 14.3±5.7 years (min:1.9; max: 22.8). APOE4, apolipoprotein allele 4 carriers; FSRP, Framingham Stroke Risk Profile; HDL, high-density lipoprotein; IL-6, interleukin-6; AHI, apnea-hypopnea index; CES-D, Center for Epidemiologic Studies Depression Scale; DAT, dementia of the Alzheimer’s type.
Interaction between IL-6 and AHI on dementia risk
Significant interactions were observed between the AHI and IL-6 levels defined by quartiles when predicting incident DAT (p = 0.029) and all-cause dementia (p = 0.018) (Table 2). When stratified by IL-6 quartiles, greater OSA severity characterized by a higher AHI was associated with higher risk of DAT in the lowest IL-6 quartile only (see Table 2, HR per log unit increase in the AHI, 4.83; 95%CI, 1.48–15.76, p = 0.009). Results remained consistent and significant when statistical models were adjusted for the Revised Framingham Stroke Risk Profile score or the APOE4 allele carrier status. When using a fully adjusted model (age, sex, body mass index, Revised Framingham Stroke Risk Profile score, and APOE4 allele carrier status as covariates), we still observed a significant effect in the lowest IL-6 quartile (p = 0.027), where a higher AHI was associated with a higher DAT risk.
Interaction between OSA and IL-6 levels on the risk of incident DAT
All analyses are adjusted for age, sex, and BMI. OSA, obstructive sleep apnea; IL-6, interleukin-6; DAT, dementia of the Alzheimer’s type; HR, hazard ratio; AHI, apnea-hypopnea index; %AH, %of sleep time in apneas and hypopneas; BMI, body mass index.
When analyzed dichotomously based on clinical cut-offs, the presence of moderate to severe OSA (AHI >15) also interacted with IL-6 quartiles to predict incident DAT, where the presence of OSA was associated with higher DAT risk in the lower IL-6 quartile only (see Table 2, HR, 7.37; 95%CI,1.10, 49.42; p = 0.04). The same finding was observed using the percentage of sleep spent in apneas or hypopneas (≥3%oxygen desaturation or arousal), where more sleeping time spent in apneas and hypopneas was associated with increased DAT risk in the lower IL-6 quartile only (see Table 2, HR, 5.06; 95%CI, 1.35, 18.99; p = 0.016).
DISCUSSION
In the community-based Framingham Heart Study, we observed that OSA severity was associated with incident DAT, but surprisingly, only in participants with low levels of IL-6. The estimated effect was large: For persons with very low inflammation, determined by IL-6 levels, each logarithmic unit increase of the AHI was associated with a 4.8-fold increase in DAT risk. Our findings suggest that the relationship between OSA and DAT is especially apparent in settings less confounded by other dementia risk factors, as indexed by levels of inflammation. A prior study showed that self-reported OSA was only associated with incident dementia risk in those without the APOE4 allele [11], suggesting that the contribution of OSA may not be evident when stronger risk factors are also present. Thus, the association between OSA and incident DAT may more clearly emerge in individuals with few competing dementia risk factors.
Another interpretation for our results could be related to an anti-inflammatory role of IL-6: although IL-6 has many pro-inflammatory functions, IL-6 promotes a negative feedback loop involved in tissue repair and suppressing the inflammatory response [12]. When comparing post-mortem brains of individuals with clinical DAT to cases with high Alzheimer’s disease pathology but without clinical symptoms, resilience to pathology was associated with elevated IL-6 levels, suggesting that IL-6 played a role in clearance and resolution of inflammation [4]. Therefore, very low levels of IL-6 may represent an environment where oxidative damage and Alzheimer’s disease pathology caused by OSA are not repaired properly, which then increase DAT risk.
Strengths of our study included the rigorous and continuous surveillance for incident dementia as well as the community-based sample, which increases the generalizability of our findings. Our main limitation was the small number of dementia cases, especially in the lowest IL-6 quartile. In future studies, investigators should aim to replicate our findings in larger samples, with statistical models that adjust for multiple sources of confounding. In addition, future studies should include a more comprehensive cytokines panel to evaluate their interaction with OSA when predicting dementia. Moreover, the overall OSA severity of our sample was low, with only 17 participants having severe OSA (AHI > 30). Thus, we were not able to examine severe OSA as an exposure, and it is therefore unclear whether our findings are generalizable to populations with severe OSA.
Because of the high prevalence of OSA and its association with dementia [1, 5], and the underlying heterogeneity of OSA, it is imperative to better identify OSA subpopulations at higher risk of developing dementia. Our results suggest that OSA is associated with DAT only in individuals with very low IL-6 levels, and the underlying mechanisms explaining this association need to be investigated in a larger sample. Given the preliminary and surprising nature of these findings, further studies are needed to confirm whether OSA is associated with DAT risk especially in individuals with very low IL-6 levels.
DATASET
The Framingham Heart Study makes phenotypic and genetic data available through the online repositories BioLINCC and dbGap, respectively. Sleep data are available via the National Sleep Research Resource.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank the staff and participants of the Framingham Heart Study and the Sleep Heart Health Study. The Framingham Heart study and Dr. Seshadri are funded by contracts from the National Health Institutes (N01-HC-25195, HHSN268201500001I, 75N92019D00031), grants from the National Institute on Aging (AG054076, AG008122). Dr. Baril is funded by the Fonds de la Recherche du Québec en Santé (#260192) and the Canadian Institutes of Health Research (#396130). Dr. Redline is partially supported by funds from the National Heart, Lung and Blood Institute (R35 135818). Dr. Pase is funded by a National Heart Foundation of Australia Future Leader Fellowship (ID 102052), the National Health and Medical Research Council (APP1158384), the Alzheimer’s Association (AARG-18-591358), and the Bethlehem Griffiths Research Foundation. Dr. Pase and Dr. Himali are also supported by a grant from the National Institute on Aging (AG062531).