
Abstract
Background:
Match or mismatch of objective physiological and subjectively perceived fall risk may have serious consequences in patients with dementia (PwD) while research is lacking.
Objective:
To analyze mismatch of objective and subjective fall risk and associated factors in PwD.
Method:
Cohort study in a geriatric rehabilitation center. Objective and subjective risk of falling were operationalized by Tinetti’s Performance Oriented Mobility Assessment and the Falls Efficacy Scale-International. Four sub-groups according to objective and subjective fall risk were classified. Subgroups were compared for differences in clinical, cognitive, psychological, and behavioral variables.
Results:
In geriatric rehab patients with mild to moderate dementia (n = 173), two-thirds showed a mismatch of subjective versus objective risk of falling, independently associated with previous falls. Underestimation of objective fall risk (37.6%) was determined by lower activity avoidance (OR 0.39), less concerns about falling due to previous falls (OR 0.25), and higher quality of life (OR 1.10), while overestimation (28.9%) was determined by higher rate of support seeking strategies (OR 50.3), activity avoidance (OR 15.2), better executive (OR 21.0) and memory functions (OR 21.5), and lower quality of life (OR.75) in multivariate logistic regression.
Conclusion:
The majority of patients showed a mismatch between objective and subjective falls risk. Underestimation as well as overestimation of fall risk was associated with specific profiles based on cognitive- and psychological status, falls and fall-related behavioral consequences which should be included in the comprehensive assessment of fall risk, and planning of individualized fall prevention programs for this population.
INTRODUCTION
Multi-morbid patients with dementia (PwD) have a doubled risk for falls and serious injuries as compared to their cognitively intact peers [1, 2]. Given the significant personal, economic, and social costs, fall risk-identification and effective fall prevention therefore have high priority in this patient group and is considered as a relevant public health issue [3]. Several studies identified not only environmental but also a number of individual factors including impaired physical functioning, history of falls [3], and psychological factors such as elevated fear of falling (FOF) as important risk factors for falls in older adults. It could be shown that individuals who developed one of these outcomes are at risk for developing the other [4], with a resulting spiraling risk of falls, FOF, functional decline [5–8], and behavioral as well as psychological consequences [9, 10]. Approximately half the adults over the age of 65 years report fear of, or concerns about falling, with varying prevalence rates of 20% up to 85%, depending on sample characteristics and assessment methodology [11]. It is also a frequent phenomenon and high impact predictor [12] for rehabilitation outcomes in older adults in geriatric rehabilitation often emerging as a result of a psychological trauma of a previous fall [13], but also commonly found among persons who had not yet experienced a fall [4].
While it is plausible that appropriate concerns about falling might be a healthy response and can positively motivate persons with a high physiological fall risk to take precautions against falls by stability increasing gait adaptations, support seeking strategies, or a reduction in risky activities, disparities between objective physiological and subjectively perceived fall risk might lead to maladaptive behavioral and psychological changes. An underestimation of an objectively high fall risk for example could increase the chance of falling through risk-taking behavior [14] or lead to low compliance to prevention strategies [15]. In contrast, elevated fear of falling associated to lack of self-confidence to avoid falls, may increase fall risk through inappropriate maladaptive restriction of activities that he/she remains capable of performing [8, 16–19], leading to a loss of independence, muscle strength, and postural control [20], decreased quality of life, and increased rates of depression, and anxiety [9, 22].
Hence, in recent years, FOF has been clearly identified as one of the most important and potentially modifiable risk factors for falls in older adults [6, 23]. But while there is an increasing interest in identifying dementia specific factors for falls, little is currently known about etiology, covariates, and potential effects on physical and psychological functions of FOF and the relationship between the subjective and objective fall risk in patients with dementia, despite their high clinical relevance. Recent studies suggest less fear of falling in persons with cognitive impairment, identifying not only global but also specific aspects of cognition such as level of impairment or cognitive subdomains to be associated to prevalence of FOF [24–26].
The lower incidence of fear of falling may be part of a larger picture as patients with neurodegenerative diseases often present with poor self-awareness in other domains such as functional limitations that may exacerbate their already jeopardized decision-making and behavior. Impaired self-awareness has been documented across different functional, cognitive, emotional, and social domains in subgroups for neurodegenerative diseases and linked to anatomical correlates [27, 28]. With respect to risk of falling and functional capacities, deficits in specific cognitive sub-performances such as executive function/working memory showed significant discriminative validity for fallers versus non-fallers and documented restricted judgment in own motor planning [29], while executive function also influenced overestimation of own functional abilities among fallers [30] suggesting a potential mechanism for falling already in persons without cognitive impairment.
Previous research also documented an association between cognitive status and FOF, with higher levels of FOF [31] even when motor performance was less impaired, indicating disparities between subjective risk evaluation and objective risk assessment, e.g., by functional status. Besides attention-related or motor deficits, which partly may interact [31–33], the decreased ability to comprehend complex situations and react adequately in patients with dementia (PwD) may lead to mismatch of objective versus subjective risk, as an adjusted behavior in risk-associated situations will request a correct analysis of the complex challenges and simultaneous comparison to own capabilities or deficits.
Patients in hospital settings stand out for different reasons. Despite a high objective risk [34, 35], in many patients perceptions of falls neither match their clinical risk nor their actual likelihood of falling [36, 37]. The unfamiliar hospital setting with an unknown environment and processes or adverse medical conditions could further promote a mismatch between subjective and objective falls risk [34, 37]. Such misperceptions may have detrimental consequences as in-hospital patients with an underestimation of fall risk lack motivation to engage in behaviors to prevent falls and have greater confidence in performing high-risk tasks independently [14], while overestimation of risk may come along with overprotective, maladaptive activity avoidance, and lack of independence as in non-hospitalized persons [8, 16–19].
Only a few studies examined prevalence and determinants of such disparities between physiological and perceived fall risk [14, 38–40]. These studies found different rates of disparities, dependent on the study sample, assessment methodology, and setting. While Delbaere et al. in a study sample of healthy community dwelling older adults found a relative low disparity between subjective and objective fall risk [38], other studies reported higher rates of disparities among persons with multiple sclerosis [40] and in hospitalized older adults [14, 39]. In the most comprehensive study using a wide variety of potential influencing factors, cognitive measures together with psychological measures stood out to determine mismatch especially so for overestimation of fall risk [38]. Interestingly in this sample without cognitive impairment, underestimation was not determined by cognitive status. However, it may not be valid to generalize these results to PwD in geriatric rehabilitation as these patients were not included in the abovementioned studies. Additionally, disparities between subjective and objective risk were classified inhomogenously and cognitive sub-performances, potentially relevant for a mismatch between subjective and objective risk of falling and relevant behavioral strategies, were also not or only selectively addressed in these studies. A documentation of effects of falls trauma or psychological status with potentially high impact on subjective risk of falling were also lacking in studies including functionally impaired study samples such as older hospitalized persons [14, 39] or multiple sclerosis patients [40]. However, this knowledge is essential to understand the complexity of falls including the objective physiological and subjectively perceived fall risk in PWD.
The aim of this study therefore was to document and analyze subjective versus objective risk of falling in patients with mild to moderate stage dementia, a high-risk population for falls prone to incorrect perception of risk. A wide range of socio-demographic, psychological, and physical factors and detailed measures of cognitive performances were used to interpret differences between patients with and without mismatch of subjective and objective risk of falling. We hypothesized that subjective overestimation and underestimation of falls differ with respect to different domains of associated variables. While we expected an underestimation to be mainly associated to impaired cognitive status in the present study sample with dementia, we expected overestimation to be mainly associated to psychological factors such as anxiety, based on results of a study with similar design in older persons without cognitive impairment [38].
METHODS
We present a cohort study of geriatric inpatients with dementia consecutively recruited during ward-based rehabilitation with data collection starting within 48 h after admission. The study was part of the project “Geriatric Rehabilitation for Demented Patients Study” conducted at the AGAPLESION Bethanien Hospital/Geriatric Center, University of Heidelberg, Germany [41] and was approved by the Ethics Committee of the Medical Faculty at the University of Heidelberg in accordance with the Helsinki Declaration.
The main inclusion was based on the diagnosis of mild to moderate dementia as a secondary admission diagnosis. Screening for cognitive impairment was performed using the Mini-Mental State Examination (MMSE) [42]. In patients with mild to moderate cognitive impairment (MMSE scores 17–26), a dementia diagnosis was confirmed or rejected by a geriatrician according to core criteria for all-cause dementia based on a standardized approach, including history-taking from the patient and a knowledgeable informant, physical and neurological examination, neuroimaging, laboratory tests, and neuropsychological testing [43]. This diagnostic approach was also applied in patients with preexisting dementia diagnosis to allow a standardized diagnostic proceeding across the whole study sample. The diagnosis of dementia was not given when there was evidence for a concurrent medical comorbidity or use of medication or drug that could concurrently explain the dementia syndrome. Exclusion criteria were acute confusion, severe visual or auditory impairment, psychiatric disorders, functional-motor deficits, or medical conditions and inadequate language level, or lack of written informed consent by participants or their legal representatives.
Measurements
Measures were assessed by trained research assistants and comprised well-established assessments, validated in older persons and in cognitively impaired patients with additional standardized questions regarding fall related behavioral strategies.
Clinical characteristics
The clinical characteristics of the study participants included cognitive status (MMSE) [42], age, gender, living arrangement before admission (community dwelling versus institutionalized), number of medications, indication for geriatric rehabilitation by diagnostic groups as documented in patient charts, ADL/functional status (nurse-administered Barthel Index) [44, 45], frailty status (Canadian Study of Health and Ageing Clinical Frailty Scale) [46], and number of falls in the previous year. In addition, fallers were defined as people who had at least one injurious fall or at least two non-injurious falls during the last 12 months [47, 48] using a conservative classification more likely to document a disabling impact of falls on person’s life.
Objective versus subjective fall risks
Participants’ subjectively perceived fall risk (in the following classified as subjective risk) was measured using the Short Falls Efficacy Scale - International (Short FES-I), validated for use in older adults with cognitive impairment [49], which allows categories of low (score 7–8), moderate (score 9–13), and high concern (score 14–28) [50]. Tinetti’s Performance Oriented Mobility Assessment (POMA) [51] (maximum score 28) was used to assess patient’s physiological fall risk (in the following classified as objective risk). Both measures were used for stratifying patients for high versus low objective and subjective fall risk.
Psychological and fall related behavioral strategies
Besides fall-related self-efficacy, psychological status was assessed for depressive symptoms (Geriatric Depression Scale, GDS) [52], health–related quality of life (12-Item Short Form Health Survey; physical (SF-12 PCS) and mental (SF-12 MCS) component summary scales) [53], and trait anxiety (State-Trait Anxiety Inventory, STAI) [54].
Cognitive functions were comprehensively assessed by subtests of the Consortium to Establish a Registry for Alzheimer’s Disease Neuropsychological Assessment Battery (CERAD-NAB) [55] and the Nuremberg Geronto-psychological Inventory [56], which included aspects of 6 different cognitive domains: executive functioning (phonemic verbal fluency), language semantic memory (modified version of the Boston Naming Test); episodic memory encoding and delayed recall (Word List-Learning and Word List-delayed recall); visuo-spatial abilities (Constructional Praxis–figures copying); speed of information processing (Modified Trail Making Test-connecting numbers). Z-values were adjusted for age, education, and gender. For global cognition the demographically corrected total score (TS) for the CERAD-NAB developed by Chandler was calculated [57]. The CERAD TS (maximum score 100) provides an effective global measure of cognitive functioning which is regarded as being superior to simplified tests such as the MMSE [58].
Single standardized questions were used to document fall-related coping strategies or relevant psychological parameters derived from methodologies in previously published studies [14, 60]. Single focus questions instead of comprehensive test protocols in these cases were used to reduce test burden of participants: Activity avoidance: “Do you avoid activities due to concerns about falling?” Answer categories (AC): (0) never/ (1) almost never/ (2) sometimes/ (3) often/ (4) very often. Support seeking strategies (participants’ intention to ask for help when performing high-risk behaviors) “Do you try to get external support (assistive devices or persons) for activities during which you are afraid of falling?” ACs: (0) never/ (1) almost never/ (2) sometimes/ (3) often/ (4) very often. Concerns about falling due to previous falls: “Did previous falls increase your concerns about falling?” ACs: (0) No/ (1) little/ (2) some/ (3) a lot.
Functional and motor assessment
Besides the POMA measurement, motor performance was documented by the Timed up and go test [61], lower extremity strength was documented by the One Repetition Maximum achieved at a leg-press training machine for maximal dynamic strength in hip- and knee- extensors (in kg) (Kaphingst, Lahntal, Germany), and physical activity during ward rehabilitation was assessed by the Physical Activity in Inpatient Rehabilitation Assessment [62]. The Hierarchical Assessment of Balance and Mobility was used to assess balance, transfers, and mobility [46]. Balance performance (sway area) was assessed by a body-fixed sensor (DynaPort® Hybrid, McRoberts, The Hague, The Netherlands) inserted in an elastic belt and positioned on the patients’ lower back at the height of the second lumbar vertebra. Balance was assessed during quiet standing with feet close together for a 30 s period while data analysis was executed automatically using on-line software (http://www.mcroberts.nl/analysis).
Statistical analyses
Socio-demographic and clinical baseline characteristics of participants were documented as frequencies (%), means with standard deviations or medians with interquartile ranges as appropriate for the distribution of the variables.
Associations between subjective and objective risk of falling and history of falls
Bivariate correlations were calculated to explore the correlation of objective (POMA) and subjective fall risk (Short FES-I) for fallers and non-fallers. Multivariate logistic regression analysis was performed to calculate odds ratios for the associations between the independent variables of objective (POMA) and subjective fall risk (Short FES-I) with the dependent variable of previous falls. Influence of the interaction term of objective and subjective fall risk was investigated. Analysis was performed without adjustment for covariates as well as adjusted for age, gender, and clinical frailty scale.
Subgroup classification and differences between subgroups by match versus mismatch
For sub-classification of study participants according to a match or mismatch between objective and subjective fall risk a χ² automatic interaction detection method (CHAID) was used based on results of the POMA (for objective risk) and Short FES-I (for subjective risk). CHAID is a tree-based segmentation technique that successively splits continuous variables into several intervals and afterwards summarizes these intervals appropriately to identify subgroups. Thereby, it splits the sample into smaller and smaller subgroups [63]. The algorithm was stopped after two steps resulting in four groups based on their subjective and objective fall risk. Additionally, we performed a non-parametric classification and regression tree (CART) analysis to ensure that no subgroups were missed. Unpaired t-tests, Mann-Whitney-U tests, and Chi-square tests as appropriate were used for comparison of patient characteristics between patient subgroups from the CHAID analyses followed by univariate logistic regression analysis factors to predict a mismatch of objective and subjective fall risk for variables found statistically different between subgroups. A two-sided p-value ≤0.05 indicated statistical significance. No covariates were included, as no confounding factors were known.
Factors associated with a mismatch
Variables from univariate regression analysis were subsequently included in a forward selection step-wise multivariate logistic regression analyses to explore the best set of independent correlates with a mismatch of objective and subjective fall risk for patients. Effects were quantified by adjusted odds ratios (OR) with corresponding 95% confidence intervals (95% CI). The step-wise method was selected to mitigate potential multicollinearity in variables considered in the multivariate analysis [64]. Analysis was performed separately in the high and low objective risk group as we hypothesize different correlates for mismatch in patients with high or low objective fall risk. In the logistic regression analyses the variables “activity avoidance”, “concerns about falling due to previous falls”, and “support seeking strategies” were considered to be on an interval scale to increase statistical power. Sensitivity analyses were performed considering these variables as nominal scaled (dichotomization 0 versus other categories). In the multivariate analysis, isolated missing data (less than 10% missing for a specific variable) was replaced by the expectation maximization algorithm based on the other variables [65]. All statistical analyses were performed using SPSS 25.0 for Windows.
RESULTS
Out of 673 patients admitted to rehabilitation, 173 were included in the study according to predefined inclusion criteria (for flow of participant recruitment, see Fig. 1). The study sample included high-aged (83.60±6.16 years) multi-morbid (number of medications: 9.3±3.2) persons with cognitive- (MMSE score 21.83±2.75) and functional impairment (median ADL Barthel score 60; IQR 45–70), and a high objective fall risk (mean POMA score 14.75±9.60) (Table 1).

Flowchart for patient inclusion. Presented are results of patient recruitment/exclusion specified for separate criteria.
Participant’s Characteristics (N = 173)
Presented are baseline values for the total study sample. MMSE, Mini-Mental State Examination; ADL, Barthel Activity of Daily Living Index; CFS, Clinical Frailty Scale; GDS, Geriatric Depression Scale, short version; Short FES-I, Short Falls Efficacy Scale - International; POMA, Performance Oriented Mobility Assessment; actual n was indicated for variables with incomplete data. 1fallers were defined as persons with >2 falls or at least 1 injurious fall during last year.
Associations between subjective and objective risk of falling and history of falls
Both variables were significantly correlated in the group of fallers (r = –0.359, p < 0.001) but not in patients without a history of falls (r = –0.184, p > 0.1). As shown in Table 2, the multivariate logistic regression analysis identified both the objective fall risk (POMA: OR: 0.97 (CI: 0.940–0.990), p = 0.007) as well as subjective risk (Short FES-I: OR: 1.08, CI: 1.039–1.121, p < 0.001) as independent risk factors for history of falls. There was no interaction between objective and subjective fall risk (full model, OR for interaction: 1.00, CI: 0.994–1.005, p = 0.881) detectable. This suggests that there is no synergy between these two risk factors and motivated a more thorough investigation of these two risk factors. Point estimates remained almost unchanged after adjustment for the known risk factors of age, gender, and clinical frailty scale, suggesting that the influence of other known covariates is minimal in our sample.
Logistic regression output for the model relating odds of experiencing ≥1 injurious fall or ≥2 non-injurious falls in the previous year based on their objective and subjective risk of falling
Results are presented for the logistic regression model using POMA and Short FES-I as independent variables and their association with multiple or injurious falls in the previous year. Given are odds ratios (OR), 95% confidence interval (95% CI) with p-value, and Nagelkerke R2 indicating the proportion of the variance in the dependent variable that is predictable from the independent variables. POMA, Tinetti’s Performance Oriented Mobility Assessment; Short FES-I, Short Falls Efficacy Scale-International.
Subgroup classification
The CHAID analysis was used to split the sample into four groups based on their objective versus subjective fall risk (Fig. 2) allowing sample specific cut-points. The POMA cut-point for low objective (LO) or high objective (HO) fall risk identified in the model was 19 with scores >19 indicating a low objective fall risk. Cut-points for subjective fall risk differed between the two groups as defined by objective fall risk with a Short FES-I cut point of >8 in the group with a low objective fall risk and >14 in the high objective fall risk group. Concerns about falling were significantly higher in the group with a high objective fall risk (mean Short FES-I score 13.67±5.72) as compared to the low objective fall risk (10.96±4.17; p= 0.001).
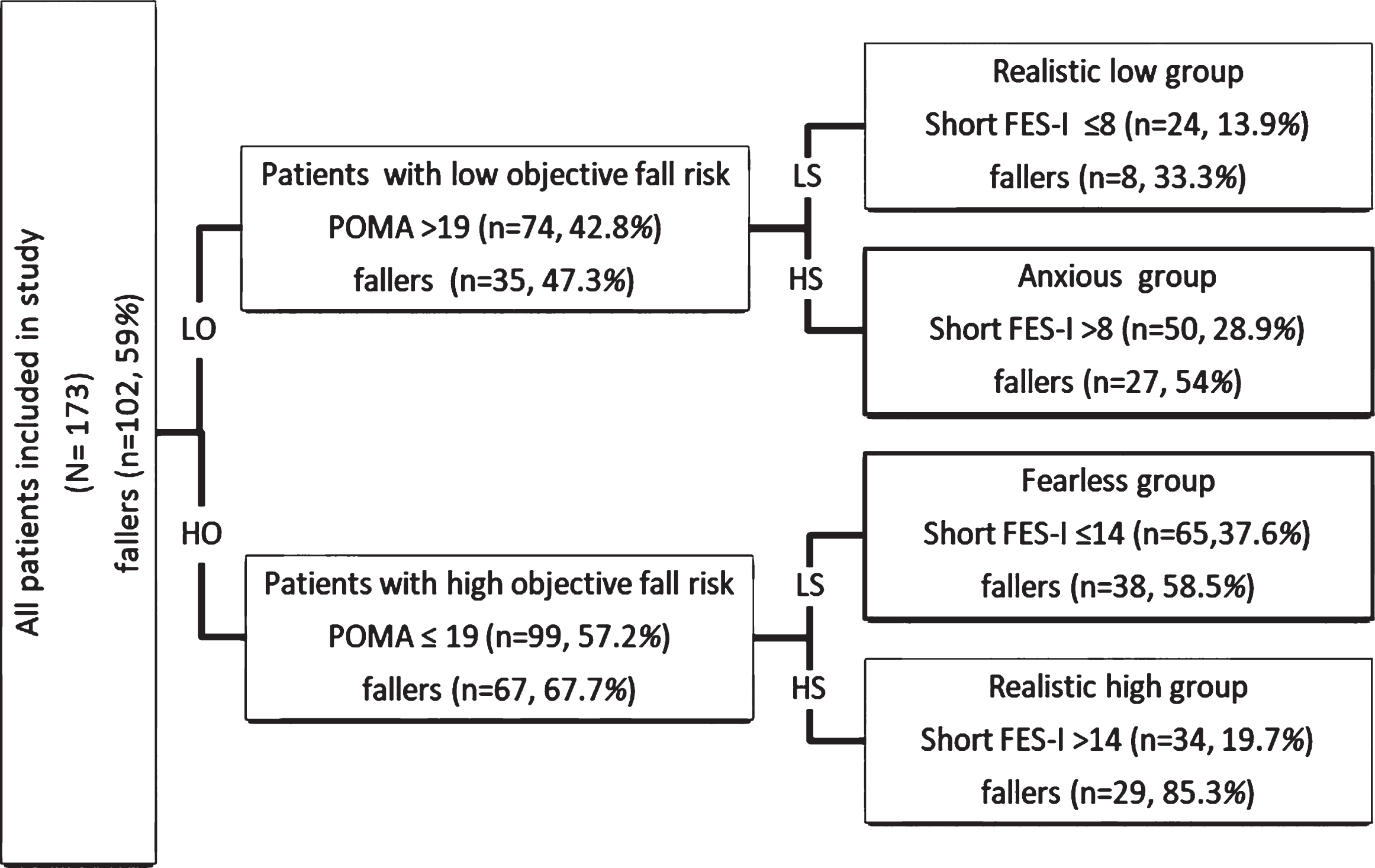
Classification of participants according to CHAID Analysis. Presented are results of a CHAID (χ² Automatic Interaction Detection Method) Analysis including fall incidence for total- and subgroups. POMA (Tinetti’s Performance Oriented Mobility Assessment) cut-off value for low objective (LO) versus high objective fall risk (HO). Short FES-I (Falls Efficacy Scale - International) cut-off value for low (LS) subjective versus high subjective (HS) fall risk. Fallers were defined as persons with >2 falls or at least 1 injurious fall during last year.
According to the CHAID classification a large number of patients (n = 115; 66.5%) had a mismatch between subjective and objective fall risk: n = 65 (37.6%) had a high objective fall risk but low subjective concerns about falling (HO-LS) and were classified as the “fearless group”, while n = 50 (28.9%) had a low objective fall risk but high subjective concerns (LO-HS) and were classified as the “anxious group”. About one third of the patients showed a match between subjective and objective fall risk: n = 24 (13.9%) had a low objective and low subjective fall risk (LO-LS), classified as “realistic low group” and n = 34 (19.7%) had a high objective and high subjective fall risk (HO-HS), classified as the “realistic high group”. CART analyses identified the same four groups with comparable cutoff values demonstrating robustness of our results to the chosen statistical method.
Fall risk defined as percentage of multiple or injurious fallers were associated to the classification criteria POMA/Short FES-I. While in the subsample of persons with low objective fall risk as defined by the POMA score >19 around half of the participants were classified as fallers (47.3%), 2/3 of the participants (67.7%) were classified for the sub-group with objective high risk confirming the objective risk stratification by POMA.
Differences between subgroups by match versus mismatch
Table 3 presents the characteristics and differences between the low and high subjective subgroups within the low objective and high objective fall risk groups. By definition subgroups differed with respect to objective risk, representing the objective classification criteria (POMA), as well as subjective concerns about falling representing the subjective classification criteria (FESI). In each subgroup with respect to low versus high objective risk, persons with high subjective risk had a higher incidence of falls than those with less subjective risk with the group defined as both high objective as well as subjective risk scoring highest (85% fallers). Results thereby confirm data from the CHAID-analysis and suggest a synergistic effect of subjective and objective risks on frequency of falls.
Characteristics and differences between subgroups with high and low subjective fall risk for patients with a low or high objective risk
Summary statistics for the four groups according to the CHAID classification based on objective and subjective fall risk. Actual n was indicated for variables with incomplete data. Differences were compared using 1 = Unpaired t-tests, 2 = Mann-Whitney-U tests, and 3 = Chi-square tests as appropriate. POMA, Tinetti’s Performance Oriented Mobility Assessment; Short FES-I, Short Falls Efficacy Scale-International; 1fallers were defined as persons with >2 falls or at least 1 injurious fall during last year; CFS, Clinical frailty scale; ADL, Barthel Activity of Daily Living Index; SF-12 health–related quality of life, 12-Item Short Form Health Survey; PCS, physical component summary scale; MCS, mental component summary scale; STAI, State-Trait Anxiety Inventory, Trait score; GDS, Geriatric Depression Scale; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease Neuropsychological Assessment Battery; TMT, Trail Making Test; 1RM, Maximal Strength leg press; TUG, Timed up and go test; HABAM, Hierarchical Assessment of Balance and Mobility; PAIR, Physical Activity in Inpatient Rehabilitation Assessment; *higher scores indicate impaired performance or poorer status; a(0) never, (1) almost never, (2) sometimes, (3) often, (4) very often; b(0) no, (1) little, (2) some, (3) a lot.
In the low objective (LO) risk group, for clinical and motor parameters such as age, medication, functional- and frailty status, or motor performance (with the exception of sway area, p < 0.05), no significant between-group differences were documented for subgroups according to subjective risk. In contrast, the psychological and behavioral parameters showed significant differences. The “anxious” LO-HS mismatch subgroup, which rated its fall risk inappropriately high, showed a more affected status in most psychological variables documented (quality of life, anxiety and trend for depression) compared with the group with a congruent perception of their low objective fall risk (LO-LS). This anxious group also showed a trend for higher fall rates in the previous year (mean 1, IQR 0–2 versus median 0, IQR 0–1) and these fallers reported more concerns about falling due to previous falls than fallers in the realistic low group, which seemed unaffected by previous falls (median 1, IQR 0–2 versus median 0, IQR 0–0). Differences also showed up for behavioral/coping strategies with higher activity avoidance or and more frequent support seeking strategies in the anxious group. Surprisingly, this subgroup revealed significantly better performances in global cognitive status (CERAD Total) and the two cognitive domains executive function (phonemic verbal fluency) and episodic memory (word list learning).
In the group with high objective fall risk, the “fearless” HO-LS mismatch group, which rated their risk inappropriately low, showed higher levels of quality of life in the motor component of the SF-12, less depressive symptoms, lower rates of activity avoidance, and support seeking strategies compared to the sub-group with a congruent perception of their high objective fall risk (HO-HS). The fearless also reported significantly less falls in the previous year (median 1, IQR 0–1 versus median 2, IQR 1–4) and these falls had significantly less effects on concerns about falling (median 0, IQR 0–1 versus median 3, IQR 2–3) than persons with realistic high concerns about falling. Subgroups also differed in reported risk of falling in all included variables (number of falls, number of fallers as defined by multiple/injurious falls) with lower fall risk in the fearless group. The subgroups did not differ significantly in the remaining clinical parameters, such as motor or cognitive performance.
Factors associated with a mismatch
Based on results of univariate logistic regression analyses (Supplementary Table 1), which included variables that were significantly different between subgroups of low and high objective fall risk, strength of associations between clinical, psychological and behavioral, cognitive and motor parameters, and mismatch were quantified by multivariate logistic regression analyses. A subjective overestimation of fall risk in patients with a low objective risk was determined by a higher rate of support seeking strategies (OR: 50.3; p = 0.010) and activity avoidance (OR: 15.2; p = 0.031), better executive (verbal fluency OR: 21.0; p = 0.035) and memory functions (word list learning OR: 21.5; p = 0.028), and lower quality of life (SF-12 MCS OR: 0.75; p = 0.035), while an underestimation of an objectively high risk was determined by a higher quality of live (SF-12 MCS OR 1.10; p = 0.028), less activity avoidance (OR: 0.39; p = 0.007), and less concerns about falling due to previous falls (OR: 0.25; p < 0.001) (see Table 4). Sensitivity analysis by logistic models with nominal recording of “activity avoidance”, “concerns about falling due to previous falls” and “support seeking strategies” qualitatively confirmed results without interference of results.
Multivariate logistic regression to identify independent variables for mismatch in subjects with low (model 1) or high objective risk (model 2)
Based on univariate logistic regression analyses the following variables were entered into the logistic regression: model 1, subjects with low objective fall risk (n = 66): number of falls in previous year, 12-Item Short Form Health Survey (SF-12) physical component summary (PCS) scale, mental component summary (MCS) scale, trait anxiety (STAI), activity avoidance, support seeking strategies, (CERAD) Consortium to Establish a Registry for Alzheimer’s Disease Neuropsychological Assessment Battery Total Score, Word list learning, phonemic verbal fluency, sway area; model 2, subjects with high objective fall risk (n = 86): model 2 (n = 86): number of falls in previous year, SF-12 PCS scale, MCS scale, activity avoidance, support seeking strategies, Geriatric Depression Scale (GDS), concerns about falling due to previous falls. Missing data were replaced for SF-12, STAI, GDS, and sway area in this analysis. OR, odds ratio; CI, confidence interval; **p < 0.05; **p < 0.01; ***p < 0.001.
DISCUSSION
The present study is the first to examine disparities between the perceived subjective and physiological objective risks of falling in a vulnerable group of multi-morbid, hospitalized geriatric patients with dementia with an extraordinary high risk of falling and of mismatch for risk classification. Two-thirds of study participants either underestimated (“fearless”) or overestimated (“anxious”) their fall risks while only one third had a realistic high or low subjective perception of their fall risks, which was congruent with their objective risk classification. Patients with mismatch perception had specific profiles based on cognitive, psychological, and health status expanding our knowledge about disparities between objective and subjective fall risk in patients with dementia. Cognitive impairment was associated with decreased subjective concerns in the subgroup with low objective risk (anxious group), while specific psychological and behavioral parameters, indicating affected psychological status were associated with increased concerns across both group classifications according to high and low objective risk. While disparities between objective and subjective risk seemed to effect risk of falling in this high-risk group for falling, study results also indicate a combined effect of both subjective and objective risk as used in the study for subgroup classification.
Sub-group classification
The CHAID analysis as used in the present study allowed a sub-classification of the total sample for subjective versus objective risk of falling by sample-specific cut-offs. These cut-offs were identical to those already suggested for the original assessments for risk of falling by the POMA to define moderate versus high risk of falling [66] and for staging levels of concerns about falling, which were identical to previously identified cut-off points in the validation of the FES-I- instrument [50]. The present cut-offs identified by CHAID analysis may therefore be stringent beyond the sample specificity of the present study and reliable as classification criteria for subjective versus objective risk of falling in various populations.
Subgroups of patients showed specific objective risks with high incidence of multiple or injurious falls retrospectively reported for the previous year, ranging from 59–83% in the high-risk group and between 33–55% in the low objective group. As shown in a previous study on accuracy of fall reporting in patients with dementia [67], such reports may represent lower estimation bounds of objective fall incidence and describe the study sample as vulnerable and at high to very high risk of falling also with respect to the very conservative definition of “fallers” classified by either injurious or multiple falls in this study. As could be expected, the subgroups with higher objective risk reported higher fall incidence compared to the low objective risk group, indicating a correct classification of high objective fall risk by POMA.
Interestingly in both the high and low objective sub-groups, the group with the higher subjective concerns also had a higher risk of falling, suggesting that both the objective as well as the subjective measure is associated with fall incidence. This finding is also supported by results of regression analysis with both the measure for objective risk (POMA) as well as the subjective perception of risk (Short FES-I) determining the history of falls in the study sample. These results are in line with previous studies, where objective and subjective measures of fall risk were also found to be, at least partly, associated with previous [39, 40] or future falls [38] in cognitively-intact persons.
A main focus of this observational trial was to study mismatches of subjective and objective risk and potential factors related to the under- and overestimation of risk, which we discuss in the following as structured by overestimation versus underestimation of risk. We choose a separate analysis of both subgroups as similar trends with respect to match-mismatch may come along with very different potential causes or direction (positive versus negative) of consequences.
Underestimation of risks
A considerably large group of almost 40% of the total sample with high objective risk showed a comparatively low subjective level of concerns (fearless-group). We initially hypothesized that cognitive impairment may be associated with incorrectly few concerns as the cognitive task to adequately compare own abilities to everyday challenges associated with risk of falling will request complex and unimpaired cognitive resources, which are restricted in PwD. Contrary to this assumption, we did not find a significantly lower cognitive status in the fearless group as compared to the match group (realistic high concerns). As we focused in the present study on a cognitively-impaired sample, we established a wide variety of different cognitive tests documenting cognitive status in different cognitive domains. However, even when multiple domains with potentially different mechanisms to affect risk of falling or risk perception were analyzed, in none of these tests was a significant difference identified. Comparable studies either did not analyze cognitive status [39, 40] or found a comparable result, however, in community dwelling persons with intact cognition [38]. We therefore assume that cognitive status may not represent a relevant potential cause of match versus mismatch in the group with high objective fall risk at least in the range of cognitive status as documented for the present study sample.
The mismatch of low subjective and high objective risk may have consequences related to a potentially inadequate physical activity level and risk exposure (activity avoidance versus inadequately high activity) depending on adequate behavioral strategies. While comparable activity levels in an institutionalized setting such as geriatric ward rehab as documented in this study could be expected given the high external, institutional control of activities with an overwhelming effect on institutionalized persons’ mobility [68], it is the subjective report on activity avoidance which raises attention. Such a self-reported, less restricted activity behavior matches well with differences as documented for the psychological status with the mismatch group having less depressive symptoms, higher quality of life, more active support seeking strategies, and less concerns about falls, even when having experienced a fall as documented in the present study. Results confirm previous research in community dwelling persons without cognitive impairment [38] indicating an overarching subsample specification across different populations for such psychological outcomes. Between-group differences may indicate a rather less negative view on life perspectives and less reactivity to adverse events such as falls, allowing being more physically active but also to seek support and thus counterbalance objective risks. Results seem encouraging, as they translate mismatch classification (inadequate perception) into a positive direction, documenting unexpected remaining resources in a large subgroup of persons with moderate dementia.
In contrast to a previous study in higher functioning persons with intact cognition [38], being more active, or more correctly, having less perceived activity restriction, did not directly translate into a superior motor status in this fearless group with no significant differences in objectively measured motor/functional performances. Following the argumentation above, the higher self-reported Quality of Life associated with motor function may again have documented a subjective perception rather than an objective motor status, which was equal in both subgroups.
Relevant demographic and clinical variables such as medication, comorbidity, age, gender, and frailty status, all representing established risk factors for falls, did not differ between the fearless and realistic high-risk group, while risk of falling, which is directly related to concerns about falling, did. As already stated above, match (co-occurrence) of subjective and objective high-risk classification seemed to document accumulated risks. Unfortunately, a superior realistic risk perception was not associated with overall superior behavioral strategies and psychological status. As a reason for mismatch (low objective–high subjective), we assume that, despite the shown high association to risk of falling, the categorization of objective risk according to the POMA score, representing an external expert rating, may not cover all potential objective risk factors. Such risk factors may be highly specific for an individual’s subjective as well as objective risk and its’ perception. In addition, the sub-groups with additional higher concerns reported a higher incidence of falls, representing traumatic events with potential effect on subjective risk perception mirroring the interplay between falls, objective and subjective risk factors. The assumption is backed up by previous research documenting an association between fear of/concerns on falling and experience of own falls [11, 13]. While traumatic fall events are associated to fear of falling, the study findings indicate that a mismatch of subjective and objective risk seems not to be a relevant fall risk even in PwD, allowing fewer concerns to motivate such persons to take part in active prevention programs with increased risk exposure such as exercise programs.
Overestimation of risks
Similar to the objective high-risk group, in the low objective risk group, mismatch (the anxious group) also classified two-thirds of the total subgroup. Rates of misclassification differ substantially to cognitively intact, rather high functioning, community dwelling persons with only one-third classified as mismatch in a previous study [38], while less differences occurred to samples with a chronic medical status [39, 40].
Comparable to results in the high objective risk group, established risk factors for falls such as age, medication, or frailty were not different between the match (low realistic group) and mismatch group (anxious group). Study results are comparable to previous studies including patient samples [39, 40], while interestingly the study including comparatively high functioning community dwelling older persons showed a more pronounced effect of such factors between mismatch groups [38].
Also motor status, as documented in different motor-functional domains such as strength, balance control, complex functional performances, or habitual physical activity, with all of them also representing established independent risk factors for falls, did not significantly differ between subgroups with the exception of one variable (sway area), indicating no or a rather weak influence of motor domains on match/mismatch classification in the present study.
Results on mismatch for effect of psychological status were comparable to frequency of mismatch in the underestimation group with high objective risk. However, mismatch between low objective and high subjective in this anxious subgroup of low objective fall risk had a completely different connotation. In contrast to the mismatch group in the high objective risk subgroup, overestimation of risk was associated with a lower psychological status as documented for almost all variables in this psychological domain including: both the physical (PCS) and mental sub-score (MCS) of Quality of life (SF-12), depressive symptoms (GDS, trend), trait anxiety (STAI), and concerns about falling, independent whether the participants experienced a previous fall or not. Although not documenting the same psychological constructs, result may indicate a rather “anxious” group, specifically documented in the low objective risk group by the STAI in this study, confirming previous results with anxiety representing the most frequent behavioral symptom in patients with less advanced cognitive impairment [69]. Such psychological symptoms may play an even larger role when no increased objective risk of falling is dominant, as in the high objective risk group of the present study, with less frequent traumatic fall events and reporting on concerns about falling independent from such an event. Study results are in accord with previous observational studies on the association of fear of falling with emotional status [13, 70] indicating that persons with high concerns about falling may tend to generally be more anxious with higher prevalence of neuroticism.
In the overestimation group psychological differences as stated above came along with behavioral consequences, which seemed to be more ambiguous as compared to the underestimation group with high objective risk. On one hand subjective reports on higher activity avoidance in the overestimation group may indicate a negative effect with respect to reduced fitness by lack of physical training/activity or decreased social participation, while a higher frequency of seeking support may help to compensate own deficits leading to a higher risk of falling on the other hand. Such a preventive strategy may be interpreted as an adopted SOC (Selection-Optimization-Compensation) behavior as suggested by Baltes [71] for successful aging to compensate individual deficits. Across all subgroups, the SOC model might be relevant and may lead to different intervention programs. While “selection” would be appropriate to choose adequate tasks perceived as within the range of individual abilities with relation to behavioral strategies and self- perception, “optimization” may refer to training of functions and thereby optimizing own resources, while “compensation” may refer to supportive strategies such as seeking help or using assistive devices when S-O strategies may no longer be feasible or effective. All of these strategies depend on a correct self-awareness and remaining ability to adequately select, optimize and compensate as a potential target for future interventions.
In the overestimation group with low subjective risk a result was documented for cognitive status, which remarkably deviated from the underestimation group. This overestimation group showed a higher cognitive performance in a number of single cognitive performances as well as the summary score of the well-established CERAD test battery, representing overall cognitive status. Similar results were documented in cross-sectional studies [24, 72]. Such an increased subjective risk perception in persons with less cognitive impairment as compared to persons with more advanced impairment may have contributed to an overestimation of subjective risk as in the present study. The finding also relates to the result mentioned above for anxiety as the leading behavioral symptom in persons with lower levels of cognitive impairment [69].
Apart from a direct comparison of potential single influencing factors for match versus mismatch groups, we also included regression models to find out which of the multiple comparisons, each with a distinguished potential effect and mechanism for disparities, would stand out in a comprehensive model. Two different regressions were run to acknowledge for potentially different interactions in the group of low objective risk (with a higher risk of overestimation of subjective risk, being anxious) and the group of high objective risk (with a higher risk of underestimation of subjective risk, being fearless). In summary, results of the single factor comparisons were confirmed and accounted for a surprisingly high percentage of variation (R2) given the complex nature of disparities, with a high impact of psychological factors in both sub-groups and a relevant, but rather unspecific influence of cognitive factors in the low objective subgroup.
Limitations
For group classification of high versus low objective risk, we used well-established, valid, and reliable measures associated with risk of falling. However, they represent—as in comparable studies—surrogate estimates for objective and subjective risk of falling. The study sample comprised patients of a large rehab center recruited according to defined inclusion criteria during 1 year, forming a large representative cohort for multi-morbid, geriatric rehab patients with diagnostically confirmed dementia. The focus on such a vulnerable sample may limit generalizability of results to other cohorts or settings to a certain extent. The study presents data on mismatch in a cognitively impaired study group prone for disparities for subjective and objective risk. As we included patients with low to moderate stage dementia only, available data did not allow reporting on potentially larger effects of cognitive status between more impaired or not impaired samples.
Conclusions
The study is the first to analyze the match/mismatch of subjective and objective fall risk in a vulnerable group of PwD with an extraordinary high risk for falling and for incorrect risk perception with two thirds of participants either underestimating or overestimating their risk of falls. The study findings show that high levels of perceived fall risk are likely to result in a higher fall incidence, independent of physiological risk, and that the disparity between physiological and perceived fall risk is associated mainly to psychological and behavioral pathways. Good news is that cognitive status per se does not have an impact on mismatch in the high-risk group, with a restricted, rather unspecific association in the low risk group despite diagnostically confirmed moderate stage dementia. Results of the larger fearless subgroup seem especially encouraging, as they translate a mismatch classification (inadequate perception) into a positive direction, documenting unexpected remaining resources with high potential for interventional strategies. Study results imply that measures of both physiological and perceived fall risk and other influencing factors should be included in comprehensive fall risk assessments so as to tailor interventions for preventing falls in a patient group with CI often excluded from adequate prevention- and therapeutic approaches [73].
Footnotes
ACKNOWLEDGMENTS
We thank Carolin Barz, Christian Bexten, Nils Bruemleve, and Andrea Fickelscherer for support in data collection and patient recruitment.
This study was supported by the Baden Württemberg Foundation and the Dietmar-Hopp Foundation. ID was supported by a doctoral research fellowship of the Ministry of Science, Research and the Arts Baden-Württemberg, Germany. The funding source had no role in the design and conduct of the study; collection, management, analyses and interpretation of the data; preparation, review or approval of the manuscript.