
Abstract
Background:
Comprehensive clinicopathological studies of neuropsychiatric symptoms (NPS) in dementia are lacking.
Objective:
To describe the pathological correlations of NPS in a sample of institutionalized people with dementia.
Methods:
We studied 59 people who were consecutively admitted to a nursing home and donated their brain. Correlations between pathological variables and NPS upon admission (n = 59) and at one-year follow-up assessment (n = 46) were explored and confirmed using bivariate and multivariate statistical methods.
Results:
Mean (SD) age at admission was 83.2 (6.4) years and mean (SD) age at demise was 85.4 (6.6); 73% of the subjects were female and 98% presented advanced dementia. The most frequent etiological diagnosis was Alzheimer’s disease (AD; 74.6% clinical diagnosis, 67.8% pathological diagnosis). The pathological diagnosis of AD was associated with aggression (β est 0.31), depression (β est 0.31), anxiety (β est 0.38), and irritability (β est 0.28). Tau stage correlated with aggressive symptoms (β est 0.32) and anxiety (βest 0.33). Coexistence of AD and Lewy body pathology was associated with depression (β est 0.32), while argyrophilic grains were associated with eating symptoms (β est 0.29). Predictive models were achieved for apathy, including cognitive performance, basal ganglia ischemic lesions, and sex as predictors (R2 0.38) and for sleep disorders, including pathological diagnosis of AD and age at demise (R2 0.18) (all p-values <0.05, unadjusted).
Conclusion:
AD was the main pathological substrate of NPS in our sample of very elderly people with advanced dementia. However, correlations were mild, supporting a model of focal/asymmetric rather than diffuse brain damage, along with relevance of environmental and other personal factors, in the genesis of those symptoms.
INTRODUCTION
Dementia is usually accompanied by affective and behavioral symptoms which worsen the clinical prognosis and aggravate the suffering of the patients and their caregivers [1]. Also termed as neuropsychiatric symptoms (NPS), these manifestations arise from specific dysfunction of brain systems that are, in some cases, independent of cognitive impairment [2]. While the clinical expression of cognitive impairment is quite predictable, depending on the underlying brain pathology, affective and behavioral symptoms display large inter-individual variability, in response to the influence of psychological and environmental factors [3, 4].
The current classifications of dementia are largely based on the identification of abnormal protein aggregates in the brain which perturb molecular processes, cellular functions, and, ultimately, cell survival, with ensuing disruption of large-scale neural networks serving cognitive, behavioral, and sensorimotor functions [5]. In addition, vascular pathology, often asso{-}ciated with neurodegenerative processes, may contribute significantly to the clinical manifestations of dementia [6].
Studies addressing the neuropathological correlates of dementia in the very elderly suggest that, although those people show high prevalence of neuropathological findings, the effect of the different neurodegenerative and vascular markers on cognitive impairment is usually mild or absent [7], maybe due to the high frequency of concomitant pathology [8]. However, as already mentioned, cognitive and neuropsychiatric symptoms do not run in parallel [3, 4] and therefore the biological models of explanation could be different [2].
Previous investigations of clinical-pathological correlations of NPS in dementia were focused on specific pathologies, mainly Alzheimer’s disease (AD) and Lewy body disease, or symptoms, mostly aggression, apathy, visual hallucinations, and depression [9–14]. The results consistently pointed to tau, rather than amyloid, pathology as the main responsible for NPS in AD [9–11, 14], while neocortical Lewy body was the principal pathological substrate of visual hallucinations in unselected donors [12]. Recent in vivo studies reported associations between amyloid deposits and more severe NPS in the initial stages of AD, but the effect of tau-pathology was not controlled [15].
In addition to the symptom/pathology limited focus, most previous studies were based on hospital series of brain donators, in which very elderly patients and patients with advanced dementia are usually underrepresented [9–11, 14]. Moreover, little attention was paid to combination or sum of pathologies, and the effect of emerging entities, such as hippocampal sclerosis, argyrophilic grains, and TDP-43 related pathologies, has barely been investigated [13, 17].
We carried out a comprehensive clinical-patho{-}logical study of NPS in elderly people with advanced dementia that included the most frequent markers, as well as combination and sum of pathologies, to better understand the genesis of these burdensome symptoms and to glimpse possible therapeutic windows.
MATERIALS AND METHODS
Setting
The Alzheimer’s Center Reina Sofía Foundation (ACRSF) was created as a multidisciplinary institution devoted to the integral research of AD and other neurodegenerative dementias [18]. The clinical protocol of the ACRSF has been described in detail elsewhere [19]. Briefly, patients and caregivers admitted to nursing home are invited to sign informed consent to participate in a research program that includes clinical assessments every six months, laboratory determinations, MRI study, and brain donation. The initial assessment is usually performed 2–4 weeks after nursing home admission, when the patient is adapted to the new environment. The informed consent forms for the ACRSF research program were previously approved by the ACRSF Ethics Committee.
Design
This was a single-center, prospective, observational study. All the residents who entered nursing home of the ACRSF since its inception in November 2007, for whom consent was obtained, which donated their brains, and had complete pathological and neuropsychiatric data at the time of database consultation (November 2014) were included in the study.
Demographic and clinical variables
The following variables were selected from the ACRSF protocol and analyzed for the study:
Sociodemographic variables. Age, sex, and education.
Clinical variables. Age of symptom onset, age of institutionalization, disease duration (i.e., from symptom inception to death), cognitive performance (measured by the Mini-Mental State Examination, MMSE) [20], and severity of dementia (measured by the Global Deterioration Scale, GDS) [21].
Neuropsychiatric symptoms were measured using the Neuropsychiatric Inventory (NPI) [22]. This instrument was administered by the study psychiatrists (JLA, LAO) through interview with the ward nurse assistant coordinator (usually the same informer was utilized for the same resident). The NPI assesses the frequency and severity of affective, perception/thought, and behavioral problems in people with dementia, across 12 different domains. A score between 0 and 12 is obtained for each type of symptom, with a total score between 0 and 144 (a higher score means greater severity). Neuropsychiatric symptoms were analyzed at nursing home admission and at one-year follow-up assessments. Two time point measurements were utilized because, as already mentioned, NPS are highly variable depending, not only on dementia severity, but also on medical, psychological, and environmental factors. Collecting the symptoms at two different time points could provide an estimation of the consistency of the obtained clinicopathological associations. In addition, a longitudinal view of symptoms could illustrate how the different pathologies manifest over time.
Psychotropic medications. Prescription of medications was coded as present or absent (either continuous or PRN prescriptions), at the assessment date. Medications potentially modifying neuropsychiatric symptoms were chosen and divided as follows: neuroleptics, antidepressants, anxiolytic/hypnotics, cholinesterase inhibitors, and memantine.
Pathological variables
The procedure for brain extraction was described elsewhere [18, 23]. In brief, rapid brain autopsy is performed after patient decease, with postmortem interval of 2–4 h. The fresh brain is immediately divided into two symmetrical halves and the left half is fixed in 4% phosphate-buffered formaldehyde for routine neuropathological assessment and diagnosis; the right half is cut in standard sections and rapidly frozen for long-term preservation. After fixation, a full neuropathological study is performed in the left half brain by obtaining 25 tissue blocks from cortical and subcortical brain regions. The neuropathological assessment is conducted according to the National Institute on Aging and Alzheimer’s Association (NIA-AA) guidelines [24].
The following primary antibodies were utilized in immunohistochemical staining for the assessment of common neurodegenerative conditions: AT100 anti-tau monoclonal antibody (Dako, USA), 6F/3D anti-amyloid beta monoclonal antibody (Dako, USA), NCL-L-ASYM anti-alpha-synuclein monoclonal antibody (Leica, Germany), and TARDBP 1078-2-AP anti-TDP-43 polyclonal antibody (ProteinTech Group). For visualization of the immunohistochemical signal, an ABC Vectastain Elite protocol was employed (Vector Laboratories).
These pathological variables were determined and utilized for the study:
Amyloid stage. An amyloid stage from 0 (no pathology) to 5 (widespread pathology) was obtained following the methods of Thal et al. [25].
Neuritic plaque score. Frequency of neuritic plaques was rated from 0 (none) to 3 (frequent), following the criteria of the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) [26].
Tau stage. Neurofibrillary tangles (NFT) were searched and stage of tau-related pathology was rated from 0 (no NFT) to 6 (widespread NFT), according to the descriptions of Braak et al. [27].
AD diagnosis. AD pathological diagnosis was established only in case of high probability of disease, i.e., frequent neuritic plaques (CERAD 3) and advanced NFT stage (Braak V-VI) [24].
Vascular pathology. Vascular pathology was evaluated using the method of Deramecourt et al. The scores were obtained after evaluation of vascular lesions stage in the frontal lobe (range 0 to 6), the temporal lobe (range 0 to 6), the basal ganglia (range 0 to 4), and the hippocampus (range 0 to 4) [28].
Vascular diagnosis. Diagnosis of vascular disease was established if myelin loss or infarcts were present at least in one territory [28].
α-Synuclein stage. An α-synuclein stage was obtained between 0 (no pathology) and 6 (neocortical pathology) as described by Del Tredici and Braak [29].
Amygdala predominant Lewy bodies. Predominance of Lewy bodies in the amygdala was specifically searched and rated as present or absent, regardless of the α-synuclein stage.
Lewy body diagnosis. Diagnosis of Lewy body disease was made if α-synuclein stage was greater than zero [29] or amygdala Lewy bodies were present.
Argyrophilic grains. Argyrophilic grains were identified as round to oval, grain-like, tau-positive neuropilic inclusions in the anteriomedial portion of the temporal lobe [30]. Positive cases were graded from 0 (no grains) to 3 (grains beyond the temporal lobe [31].
Hippocampal sclerosis. Hippocampal sclerosis was defined as selective pyramidal cell loss and gliosis of CA1 region and subiculum [32]. This variable was rated as present or absent.
Limbic-predominant age-related TDP-43 ence-}phalopathy neuropathological change (LATE-NC). A simplified staging of TDP-43 inclusions from 0 (no inclusions) to 3 (inclusions in the middle frontal gyrus) was followed, according to Nelson et al. [33] (LATE-NC determination was not available at study inception, but it was incorporated during the paper review process).
Statistical analysis
Demographic, clinical, and pathological variables were presented using indexes of frequency, central tendency, and dispersion. Non-parametric statistics were utilized to compare the evolution of clinical variables in the initial and one-year follow-up assessments. Bivariate correlation analysis was conducted to explore the associations between pathological markers and NPS. Spearman’s rank correlation coefficient was utilized because the study variables were discrete and presented asymmetrical distribution. In addition, a possible effect of combination of pathological diagnoses on NPS was explored, using the following predefined combinations: 1) AD and vascular pathology, 2) AD and Lewy bodies, and 3) total number of diagnoses, including AD, vascular disease, Lewy bodies, argyrophilic grains, hippocampal sclerosis, and LATE-NC (possible score 0–6). As already mentioned, AD diagnosis was established in case of high probability of disease [24] and vascular diagnosis was accepted if myelin loss or infarcts were present [28]; for the rest of pathologies, any disease stage superior to zero was accepted. The Spearman’s r coefficient was interpreted as follows: negligible, <0.20; weak, 0.20–0.34; moderate, 0.35–0.50; strong, >0.50 [34].
Univariate regression analysis was carried out to explore the effect of neuropathological variables on neuropsychiatric symptoms. Those variables that presented a p-value <0.20 were selected for the multiple regression models. Age at demise, sex, cognitive performance (MMSE), pathological variables, and, when appropriate, psychotropic medications, were stepwise introduced or eliminated from the regression models (p-to-enter <0.05, p-to-leave >0.10). Since this was a primarily descriptive, exploratory study, multiple comparisons adjustments were not conducted [35]. The statistical analyses were performed using the Statistical Package for Social Sciences version 16.0 software (SPSS, Chicago, IL).
RESULTS
Brain autopsies were obtained from 63 patients, which approximately represented two thirds of the patients who participated in the ACRSF nursing home research program and died [36]. Pathological evaluation of two brains was not available at the time of data collection, adequate pathological assessment could not be performed in one brain due to the presence of cortical infarctions, and clinical data could not be obtained for one patient due to demise soon after nursing home admission. Hence, data will be presented from 59 patients and brains.
Mean (SD) age of patients at symptom onset was 76.0 (7.5), age at nursing home admission was 83.2 (6.4), and age at demise was 85.4 (6.6); 72.9% of the patients were female. The educational achievement of the subjects was as follows: illiterate 8.5%, able to read 3.4%, able to read and write 13.6%, primary education 67.8%, and superior education 6.8%. There was predominance of patients in the moderate to severe stages of dementia, which showed aggravation in the follow-up assessment (Table 1). The etiological diagnoses in life were as follows: AD (57.7%), AD and cerebrovascular disease (16.9%), Lewy body disease (15.3%), and other diagnosis (10.1%). All types of psychotropic medications were highly prescribed in the initial assessment and that was even increased one year later (Table 1).
Clinical variables and medications in the initial and follow-up assessments
Figures represent median (Q1, Q3), unless % is indicated; 1Wilcoxon or chi-square test (n = 42 [MMSE] and 35 [medications] pairs, due to missing data). GDS, Global Deterioration Scale; MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory.
The most frequent pathological diagnosis was AD (67.8%), followed by LATE-NC (53.5%), and vascular disease (50.8%). Lewy body disease was observed in 28.8% of the brains, of which 6 cases (10.2%) displayed amygdala predominance. Hippocampal sclerosis and argyrophilic grains were identified in, respectively, 24.1% and 8.9% of the brains (hippocampal sclerosis could not be assessed in one brain and argyrophilic grains could not be assessed in three brains) (Fig. 1). Different types of pathological changes coexisted in 74.6% of the brains, which therefore received more than one pathological diagnosis (15 [25.4% ] one diagnosis, 23 [39.0% ] two diagnoses, 21 [35.6% ] three or more diagnoses). The most frequent association was AD and LATE (39.3%), followed by AD and vascular disease (25.4%), LATE and Lewy body pathology (23.7%), and LATE and hippocampal sclerosis (21.1%) (all the other associations had a frequency of less than 20%, data not shown).
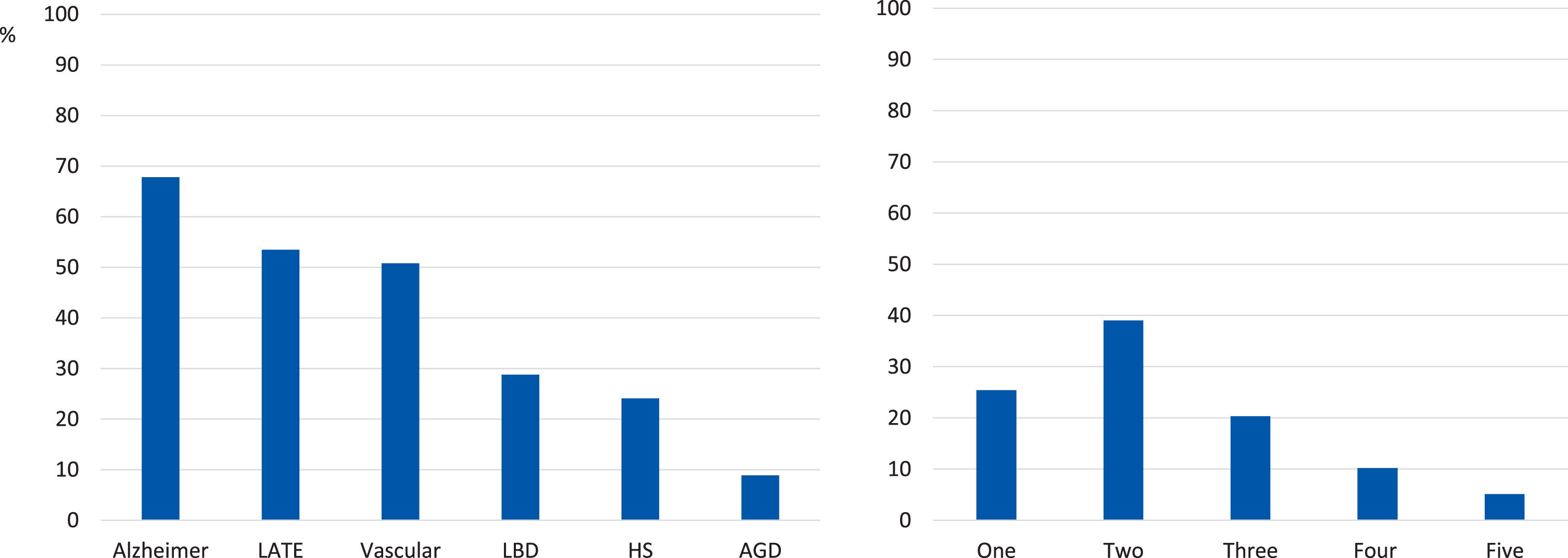
Disease distribution by specific pathologies (left) and number of pathologies (right), in the individual brains (n = 59). HS, hippocampal sclerosis; LATE, limbic-predominant age-related TDP-43 encephalopathy; LBD, Lewy body disease; AGD, argyrophilic grain disease.
Total NPI score was 19.3 (SD 13.6, range 1–57) at nursing home admission and 22.7 (SD 16.3, range 1–59) at one-year follow-up assessment (13 patients could not be evaluated at follow-up due to death). Apathy was the most conspicuous neuropsychiatric symptom, with score of 5.2 (SD 4.0, range 0–12) in the initial assessment and significant increase to 7.0 (SD 3.9, range 0–12) at follow-up (p < 0.005). The rest of symptoms were usually of mild severity or, regarding hallucinations, euphoria, and disinhibition, virtually absent (Fig. 2). Symptom attenuation was observed for delusions (score of 0.6 [SD 1.7, range 0–8] in the initial assessment, 0.2 [SD 1.2, range 0–8] at follow-up, p < 0.05), without significant longitudinal changes for the rest of symptoms (all p values > 0.10, data not shown).

Neuropsychiatric symptoms in the initial and 1 year follow-up assessments. Bars represent mean value in the Neuropsychiatric Inventory; *p < 0.05; **p < 0.005 (Wilcoxon test).
Bivariate correlations of pathological markers and NPS are presented in Table 2. All the correlations were of mild intensity and mostly appeared in the initial assessment. Regression analyses confirmed associations between tau stage and total NPS (βest 0.37, p < 0.01), tau stage and aggressive symptoms (βest 0.32, p < 0.05), and tau stage and anxiety (βest 0.29, p < 0.05) in the initial assessment. The association between tau stage and anxiety remained when aggressive symptoms were included as covariate (βest 0.33, p < 0.05). There was also association between argyrophilic grains and eating alteration (βest 0.29, p < 0.05). Regarding apathy, a regression model was achieved which included vascular lesions in the basal ganglia, cognitive performance, and sex and explained 38% of the variance of that symptom (Table 3). As for the one-year follow-up assessment, only association between neuritic plaques and aggressive symptoms remained significant in the multivariate analysis (βest 0.34, p < 0.05).
A pathological diagnosis of AD was associated with total NPS in the initial assessment (βest 0.40, p < 0.005) and also with the following specific symptoms: aggression (βest 0.31, p < 0.05), depression (βest 0.31, p < 0.05), anxiety (βest 0.38, p < {}0.005), and irritability (βest 0.28, p < 0.05). In addition, a regression model was obtained for sleep disorder which included age at demise and explained 18% of variance of that symptom (Table 4). The combination of AD and Lewy body pathologies was associated with depressive symptoms in the initial assessment and that correlation persisted when the pathological diagnosis of AD was controlled (βest 0.32, p < 0.05). No other significant associations were obtained between single, combination, or total number of pathological diagnoses and NPS.
Bivariate correlations between pathological variables and neuropsychiatric symptoms
Spearman r is represented for the correlations between pathological variables and NPI score at nursing home admission (up, n = 59) and one-year follow-up assessment (down, n = 46) (<0.20 negligible, 0.20–0.34 weak, 0.35–0.50 moderate, >0.50 strong correlation; r values > 0.20 are highlighted); n: total number of coexisting diagnoses, considering the following: Alzheimer, vascular, Lewy body disease, hippocampal sclerosis, argyrophilic grains, and LATE-NC. LATE-NC, limbic-predominant age-related TDP-43 encephalopathy neuropathological change; NPI, Neuropsychiatric Inventory.
Regression model for the prediction of apathy at nursing home admission
The independent variables were stepwise forward introduced; cognitive performance was measured with the Mini-Mental State Examination and vascular pathology was measured using the method of Deramecourt et al. [28]; the following variables were excluded from the model: age at demise and psychotropic medications. βest, standardized regression coefficient.
Regression model for the prediction of sleep disorder at nursing home admission
The independent variables were stepwise forward introduced; the following variables were excluded from the model: sex and cognitive performance. βest, standardized regression coefficient.
DISCUSSION
We prospectively explored the neuropathological correlates of NPS in a sample of institutionalized people with dementia. A comprehensive approach that included the study of combination and sum of pathologies was deemed appropriate, given the variability of neuropsychiatric manifestations and the frequent coexistence of brain pathologies, particularly in the very elderly [5, 8].
Overall, the observed symptom profile was consistent with previous studies, which showed low persistence of psychotic symptoms and reported apathy as the most prevalent and persistent NPS throughout the course of dementia [37]. In contrast with apathy, the severity of the rest of NPS was usually mild, also in agreement with previous investigations conducted in nursing homes [38] and severe dementia [37]. Likely, that was the effect of cognitive deterioration and apathy preventing verbal and motor expression of symptoms [39]. In our sample, use of neuroleptic and other psychotropic medications could also have contributed to symptom evolution, especially regarding delusion attenuation (Table 1).
Consistent correlations were found between NPS, particularly aggression, and AD pathological markers. Those findings are congruent with results from previous investigations showing associations be{-}tween NFT burden and aggression/agitation in AD [9], even in pre-cognitive stages [14]. In our study, tau stage was related to aggressive symptoms and anxiety in the initial assessment, while neuritic plaques were related to aggressive symptoms at one-year follow-up. That isolated neuritic plaque correlation should be taken very cautiously, since it is discordant with current knowledge of AD physiopathology (tau spreading after amyloid deposition plateaus) [40] and because of high patient attrition (22%).
Moderate correlation was found between ischemic vascular lesions in the basal ganglia and apathy (βest 0.46, Table 3). The importance of cerebrovascular burden in some NPS was assessed in several studies using magnetic resonance imaging (MRI). A study of 84 community-dwelling patients with AD demonstrated significant association between apathy and the presence of ischemic white matter lesions, which were also associated with disinhibition [41]. In contrast, we found an “inhibited behavior” profile in patients with cerebrovascular disease, particularly ischemic basal ganglia lesions, with trends of negative associations not only for disinhibition, but also for hallucinations, anxiety, euphoria, irritability, motor disturbance, and aggressive behavior (Table 2). These partially conflicting results could be due to the presence of high load of AD pathology in our sample, possibly preventing the outflow of disinhibited behavior in patients with frontal or subcortical vascular lesions. In fact, in a previous study of brain donors with dementia and pathological diagnosis of AD, the coexistence of vascular lesions was associated with less frequency of agitation [13].
In contrast with previous investigations, no correlation was found between AD markers and apathy. This unexpected result could be due to several reasons. Most previous descriptions of apathy in AD were conducted in vivo, without autopsy verification, so they could possibly be contaminated by other pathologies, such as Lewy body disease and vascular disease, which may increase the presence of that symptom [4, 38]. Previous clinicopathological studies showed associations of apathy and AD pathology [42], particularly NFT burden in the anterior cingulate [9, 10] but, again, the coexistence of vascular lesions was not specifically addressed. Besides, apathy may be influenced by cognitive deterioration and by other individual and environmental factors, not necessarily linked to AD. In our sample, the high use of psychotropic medications, particularly anxiolytic/hypnotics and neuroleptics, may have masked the relationship between AD pathology and apathy (Table 1), but that was not confirmed in the multivariate analysis (Table 3).
The coexistence of AD and Lewy body pathological diagnoses was linked to depressive symptoms (βest 0.32, p < 0.05). A previous investigation of 4,582 brain samples with AD demonstrated correlation between depression and NFT, but the effect size was very small (Cohen’s d = 0.16) and Lewy body pathology was not controlled [11]. Other study conducted in nondemented brain donors demonstrated association between late-onset depression and neuronal loss in hippocampus and some subcortical structures, together with subcortical Lewy bodies, but association between depression and AD pathology was not found [43]. Clearly, more studies are warranted to further investigate the relevance of depressive symptoms in the Lewy body variant of AD [44].
We also found association between argyrophilic grains and eating symptoms (βest 0.29, p < 0.05). Considered as the second most frequent neurodegenerative disorder, argyrophilic grain disease (AGD) is usually manifested as personality changes and memory failure, although there is important pathological and clinical overlap with AD and frontotemporal lobar degeneration [45]. In a multiethnic series of 983 unselected brain donors, the frequency of AGD was 15.2%, which was found to increase with age and low socioeconomic status [16]. The lower frequency of 8.9% observed in our study could be explained as random effect due to small sample size or, perhaps, as the consequence of differences in socioeconomic status. In the Brazilian study, appetite and eating changes were retrospectively reported in 40.8% of AGD samples, versus 30.0% of samples without AGD (p < 0.01); however, differences between pure (i.e., without co-pathology) AGD and pure AD were not found, possibly due to the confounding effect of cognitive deterioration and other NPS in the AD group [16]. To contrast those results, we analyzed post-hoc a possible confounding effect of AD pathology in the association between AGD and eating alteration; once AGD was introduced in the regression model, there was no effect of AD pathology (βest 0.00, p = 0.99). Since all our patients had loss of appetite and most of them (4/5) presented stages I-II of disease [31], disruption of connections between the amygdala nuclei and the lateral hypothalamic area could be the pathological substrate of the symptoms [46].
A trend of motor hyperactivity was observed in the follow-up assessment for patients with LATE-NC (r = 0.27), but that was not confirmed in the multivariate analysis. Similarly, no consistent affective or behavioral correlates were found for hippocampal sclerosis or amygdala predominant Lewy bodies (Table 2). While, to the authors’ knowledge, clinicopathological studies of NPS in hippocampal sclerosis or amygdala predominant Lewy bodies have not been published, our LATE-NC results are consistent with those from a previous study of 51 brain samples which displayed both AD (Braak stages IV-VI) and widespread TDP-43 pathology. In that study, behavioral disturbances, including disinhibition and stereotyped behavior, were retrospectively searched but not found [47].
Sum of pathologies was not associated with NPS. In fact, the opposite trend was observed, with almost null correlation between total NPS and total number of pathological diagnoses (r = 0.04 and r = –0.03, respectively, in the initial and the follow-up assessments) (Table 2). Those results support a model of asymmetrical or regional rather than diffuse brain pathology as a substrate for NPS [2], according to which an increase in the pathological burden would lead to a progressive reduction of all the behavioral and psychological manifestations of dementia, except apathy.
Our results may not seem consistent because virtually all the clinicopathological correlations were observed in the initial assessment but were not confirmed in the follow-up visit. We believe that was mainly due to patient attrition (22%) and consequent reduction in statistical power. In addition, the high use of psychotropic medications at follow-up (Table 1) may have contributed to the loss of individual clinicopathological correlations, even though the mean values of NPS did not change.
Our study has some other limitations to be noted. Firstly, our patients suffered from advanced dementia and reliable clinical information for the initial stages of disease was not available. In addition, some relevant pathologies were not represented-particularly frontotemporal lobar degeneration- and, except for apathy, the severity of NPS was usually mild. Thus, the obtained results cannot be generalizable to patients with mild dementia, frontotemporal dementia, or severe neuropsychiatric manifestations. However, given the proximity between clinical evaluation and death, our results should validly reflect the correlations between brain pathology and NPS in elderly people with advanced dementia. Second, the NPI, by conditioning the detailed evaluation of each symptom to a probe question, may not be adequate for the assessment of severe dementia, where symptom manifestations may become subtle or unclear, just conveyed, for instance, through facial expression [48]. Third, only the left half of the brain was studied, and, except for vascular lesions, the analyses were driven by disease stage, rather than specific locations. Correlations between AD markers and symptoms such as apathy, delusions, or hallucinations could have been missed for that reason. Fourth, since multiple comparison adjustments were not conducted, the probability of type I error was increased; hence, our novel results should wait for confirmation. Fifth, the small sample size did not permit adequate analysis of pathological combinations. And sixth, retrospective postmortem study may not be the best method to ascertain the pathological substrate of NPS, since the coexistence of symptoms and pathology is not ensured.
In conclusion, NPS were mainly associated with AD pathology in our sample of very elderly people with advanced dementia. The associations were consistent but only of mild to moderate strength, suggesting relevant role for other contributors (e.g., genetic, chemical, psychological, environmental, and social factors) [39]. Clearly, the pathological correlations of NPS deserve more investigation to better understand, and comprehensively treat, these burdensome and complex manifestations. Clinicopathological studies excluding donors with advanced dementia [49] and prospective studies started in life, incorporating chemical and neuroimaging markers, could be especially useful to clarify the pathological substrate of NPS. Since neurodegenerative conditions usually present with focal/asymmetrical patterns of cortical involvement [50], prominent and well-defined behavioral disturbances could be characterized as the result of damage to specific brain locations which, in turn, could be compensated with selective interventions. However, for people with advanced dementia, the treatment of NPS should remain global, mainly based on environmental modifications and personal interaction.
ACKNOWLEDGMENTS
The statistical analyses were reviewed by JM Rojo-Abuin, from the Council for Scientific Research, Madrid, Spain.
The authors are grateful to the ACRSF residents and their families, which generously participated in the clinical assessments and donated the brain. We are also grateful to all the ACRSF professionals for their continuous support.
The present investigation was fully financed by the Reina Sofía Foundation and the Carlos III Institute of Health.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/20-0600r3).